Back to Journals » Clinical Ophthalmology » Volume 17
Impact of a Swept Source-Optical Coherence Tomography Device on Efficiency in Cataract Evaluation and Surgery: A Time-and-Motion Study
Authors Multack S, Pan LC, Timmons SK ![]() , Datar M, Hsiao CW, Babu R, Pan SM, Woodard L
, Datar M, Hsiao CW, Babu R, Pan SM, Woodard L
Received 5 August 2022
Accepted for publication 5 December 2022
Published 5 January 2023 Volume 2023:17 Pages 1—13
DOI https://doi.org/10.2147/OPTH.S384545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Samuel Multack,1 Li-Chen Pan,2 Sean K Timmons,2 Manasi Datar,2 Chia-Wen Hsiao,3 Raiju Babu,3 Sun-Ming Pan,3 Lawrence Woodard4
1Multack Eye Care and Associates, Olympia Fields, IL, USA; 2Commercial Strategy and Market Access, Boston Healthcare Associates (a Veranex Company), Boston, MA, USA; 3Health Economics and Outcomes Research, Alcon, Fort Worth, TX, USA; 4Atlanta Eye Surgery Center, Atlanta, GA, USA
Correspondence: Samuel Multack, Multack Eye Care and Associates, 20303 Crawford Ave, Olympia Fields, IL, 60461, USA, Tel +1-708-898-1858, Email [email protected]
Purpose: This study aims to assess the time impact of ARGOS® (image-guided swept-source optical coherence tomography biometer integrated with operating room (OR) technologies (SS-OCT w/ORT)) compared to LENSTAR LS 900 (optical low-coherence reflectometry (OLCR)), IOLMaster 500 (partial coherence interferometry (PCI)), and IOLMaster 700 (SS-OCT) on efficiency in the cataract evaluation and surgery.
Patients and Methods: Data from 212 patients (two study sites) who underwent evaluation and/or cataract surgery were collected. The primary objective was to compare the performance of four biometers; statistical analyses were conducted to compare 1) biometer measurement times for all patients (ANOVA w/post-hoc Dunnett’s test) and stratified by cataract density (ANOVA) and 2) rate of biometer acquisition failure (Chi-square test w/post-hoc Bonferroni correction). Real-world observational data collected were then used to develop a practice-based time-efficiency model to demonstrate the combined effect that adopting an SS-OCT w/ORT has on a practice’s cataract workflow. Real-world data inputs included assessment of patient’s eyes’ cataract grade density, time taken for optical biometry, Manual A-scan (ultrasound biometer) when acquisition failed, and measurement times associated with other devices used in cataract evaluation and surgery.
Results: For 208 patients (56% non-dense, 44% dense), the SS-OCT w/ORT biometer had a 0% acquisition failure (SS-OCT: 3% (p = 0.05); OLCR: 5% (p = 0.004); PCI: 15% (p < 0.0001)) and an average time savings of 30 seconds/patient compared to the other biometers in this study (p < 0.05). When acquisition failed, ultrasound biometry resulted in an additional 2.5 minutes/patient. For a cohort of 1000 patients, an SS-OCT w/ORT and an image-guidance system adopted at a practice using an SS-OCT, femtosecond laser, and intraoperative aberrometer offer up to 58% efficiency gain across the cataract workflow.
Conclusion: Results from this study demonstrate an SS-OCT w/ORT’s efficiencies in cataract evaluation and surgery driven by faster measurement times, reducing the need for ultrasound biometry, and its integration benefits with other devices.
Keywords: cataract surgery, swept-source optical coherence tomography biometer, time-and-motion study, preoperative evaluation phase
Corrigendum for this paper has been published.
Introduction
Over the past few decades, the volume of cataract surgeries performed has steadily increased, with cataract surgery being one of the most common surgical procedures performed in the United States and worldwide.1 The World Health Organization expects the world’s population over 60 years to double between 2015 and 2050. With an aging population and increased life expectancy, the demand for cataract surgery is expected to expand worldwide.2 Although the rates and demand for cataract surgery are increasing, several studies have shown that the number of available ophthalmologists will fall short of demand. The Health Resources and Service Administration agency estimated that there will be a shortage of more than 6000 ophthalmologists by 2025.3 Given the projected volume of cataract procedures, identifying opportunities to improve efficiencies within the cataract procedure workflow may address the expected increasing demand for cataract procedures and decreasing supply of ophthalmologists.
As part of the ophthalmic evaluation for cataract surgery, a comprehensive examination of the patient’s ocular biometry is essential to achieve satisfactory refractive outcomes. For many years, measuring the anatomical characteristics of a patient’s eye involved the use of a contact ultrasound probe compressing the cornea (Manual A-scan).4 Optical biometry has since evolved to include non-invasive technologies that can measure anatomical characteristics of the eye by optical methods. Various optical methods exist, including optical low-coherence interferometry (OLCR), partial coherence interferometry (PCI), and swept source optical coherence tomography (SS-OCT). Several optical biometers on the market leverage these optical methods to accurately measure a patient’s ocular biometry: IOLMaster* 500 [Carl Zeiss Meditec, Inc., IOLMaster* 500, Dublin, CA, USA] utilizes PCI, LENSTAR* LS 900 [Haag-Streit USA, Inc., LENSTAR* LS 900, Mason, OH, USA] is based on OLCR, and both IOLMaster*. 700 [Carl Zeiss Meditec, Inc., IOLMaster* 700, Dublin, CA, USA] and ARGOS® [Alcon, ARGOS®, Fort Worth, TX, USA] leverage SS-OCT technology*.4 (*Trademarks are the property of their respective owners).
Precise optical measurements are essential for the selection of an appropriate optical intraocular lens (IOL) power, which contributes to achieving highly accurate refractive outcomes.5 For patients receiving an advanced-technology IOL (AT-IOL), intraoperative guidance systems are available to support an ophthalmologist, such as an image-guidance system for IOL alignment and an intra-operative aberrometer for IOL power refinement. Two such systems include the VERION® Image Guided System (image-guidance system) [Alcon, VERION® Image Guided System, Fort Worth, TX, USA] and the Optiwave Refractive Analysis (ORA) SYSTEM (intraoperative aberrometer system) [Alcon, ORA System, Fort Worth, TX, USA], both of which integrate with ARGOS® (SS-OCT w/ORT). The image-guidance system is comprised of three separate components: VERION® Reference unit (image-guidance reference unit) [Alcon, VERION® Reference unit, Fort Worth, TX, USA], VERION® Digital Marker LenSx (image-guided femtosecond laser) [Alcon, VERION® Digital Marker LenSx, Fort Worth, TX, USA], and VERION® Digital Marker Microscope (image-guided optical microscope) [Alcon, VERION® Digital Marker Microscope, Fort Worth, TX, USA]. The image-guidance reference unit is an in-office cataract refractive device that captures a high-resolution image of the eye, which can also be achieved using the SS-OCT w/ORT’s integrated image guidance software. The image-guided femtosecond laser and the image-guided optical microscope interface with a femtosecond laser, such as LenSx, as well as the surgical microscope in the operating room (OR). The intraoperative aberrometer provides real-time refraction measurements of the patient’s eye during surgery, assisting surgeons in achieving the desired refractive outcomes,6 and is powered by ORA AnalyzOR™ Technology (intra-operative aberrometer cloud-based database) [Alcon, ORA AnalyzOR™ Technology, Fort Worth, TX, USA] which validates a surgeon’s IOL calculation to provide more predictable outcomes and has been shown to significantly improve the rate of outcomes within 0.50 diopters.7
Previous research has established the accuracy, repeatability, and reproducibility of the four optical biometers.8,9 Although optical biometry devices have been shown to be more advantageous than ultrasound biometers, failing to acquire the measurement using an optical biometer requires the use of a contact ultrasound biometer as an alternative method to measure the eye. Furthermore, higher failure rates and use of contact ultrasound biometers instead may also be more prevalent in patients with denser cataracts.10 Separate studies have compared two optical biometers and reported the superior measurement time of the SS-OCT biometer compared to the PCI and OLCR biometer8,9 and the superior acquisition rate of the SS-OCT w/ORT biometer compared to the PCI, OLCR, and SS-OCT biometer.11–14 However, to our knowledge, there are no prospective real-world studies directly comparing the biometer measurement time and acquisition failure across four different biometers (SS-OCT w/ORT, SS-OCT, PCI, and OLCR) in both non-dense and dense cataract patients or the overall impact of the time saved by using an SS-OCT biometer on a practice’s workflow, from clinic to surgery employing time-and-motion techniques. Time-and-motion methodology enables the study of process improvement through the evaluation of efficiency of clinical activities. A time-and-motion study is a continuous, observational study where the observer records the time taken to accomplish a task and pin-point potential opportunities to increase the efficiency in care.
The objective of this study was to evaluate measurement times and acquisition failure rate for four optical biometers used in cataract evaluation and surgery. The primary objective aimed to quantify data from an observational real-world time-and-motion study at two study sites to compare the performance of four biometers, including biometer measurement times for all patients (stratified by cataract density) and the rate of biometer acquisition failure. The secondary objective was to create a practice-level time efficiency model to investigate the overall impact that an optical biometer would have on a practice’s cataract evaluation and surgery workflow for a hypothetical cohort of 1000 patients by leveraging workflow mapping, inputs from published literature, and real-world observational time measurements.
Methods
Study Design
A prospective, real-world, within-subjects, observational time-and-motion study of patients coming in for evaluation and/or cataract surgery was conducted at two study sites. This study was conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice. All study measures collected for this study were strictly observational. No protected health information (PHI) was collected. The study received a Non-Human Subjects Research Determination from Sterling Institutional Review Board (IRB) (Atlanta, GA) and informed consent was waived. At both study sites, patients underwent several diagnostic devices as per the study protocol, including multiple optical biometers and ultrasound biometry. To reduce potential bias, the order in which patients received each optical biometer was randomized using block randomization. Block randomization allowed for equal representation of each biometer by randomizing the order in which the participants received each device. The ultrasound biometry measurement was introduced as the last diagnostic device the patient received as it requires direct contact with the patient’s cornea and has the potential to fatigue the eye if used earlier.
Participants
The study included patients over the age of twenty-two years scheduled to undergo either cataract evaluation and/or cataract surgery. Additional inclusion criteria for both study sites included patients that did not have corneal or retinal pathology and patients that were not scheduled to undergo additional surgical procedures at the time of their scheduled cataract surgery. To ensure that the development of dry eye did not bias the study results, patients took a 90-second break in between measurements and were instructed to close their eyes and blink multiple times. Furthermore, to ensure consistency of data collected at study site 2, patients were excluded if the patient was unable to fixate, had nystagmus or other eye movement abnormalities, were wheelchair bound, or had a body mass index (BMI) >50.
Data Collection
Data collection at study site 1 was performed on a single day by a team of five trained research collaborators. Data collectors arrived one-day prior to the day of data collection to assess the layout of the practice and to shadow practice staff. Each researcher was assigned to collect data for a given set of procedures within one of the three locations within the practice (clinic, surgical laser room, and OR). Practice staff were instructed to continue working as they normally do, while data collectors observed and collected data. Owing to the coronavirus disease 2019 (COVID-19) pandemic, data at study site 2 was collected by clinical staff at the study site over a three-month period. The on-site researchers were trained prior to the start of the data collection process to maintain and ensure the quality and consistency of data collected using data collection forms. All data collection forms and processes were pre-determined, the start and end time for each measurement were pre-defined, and data collectors were trained in these measurements at both study sites.
Sample Size Calculation
An a priori sample size calculation was conducted to assess the primary objective comparing the average measurement times by dense and non-dense cataract patients across all four biometers. Based on a medium effect size and a 95% statistical power, a desired sample size of 176 patients in total or 88 patients per group (dense and non-dense cataract patients) was determined.
Study Measures
The dataset comprised real-world data from two separate study sites which contributed different measurements to the study. Key differences between the measurements collected at the two study sites were a result of the available in-house devices. For both dense and non-dense cataract patients, biometry measurement data were collected for an SS-OCT w/ORT and an OLCR at study site 1 and for all four biometers (SS-OCT w/ORT, OLCR, PCI, and SS-OCT) at study site 2. Ultrasound biometry was collected at both study sites; at study site 1, ultrasound biometry time measurement data was collected for patients regardless of biometry acquisition failure, whereas, at study site 2, ultrasound biometry time measurement data was collected only for patients that failed to acquire a biometry measurement using one of the four biometers. In addition to the optical biometry measurements, measurement times for additional devices used in the clinic (image-guided reference unit), surgical laser room (image-guided femtosecond laser), and the OR (image-guided optical microscope and intraoperative aberrometer) were collected at study site 1. Measurements collected at each study site and their respective definitions are summarized in Table 1. For measurement purposes, the number of scans completed per eye for each biometer was set at 5 scans per eye. Dense cataract patients were defined as those with Nuclear Sclerosis (NS) level greater than three and/or the patient was diagnosed with mature cataract or Lens Opacity Classification System III (LOCS III) grade greater than four.
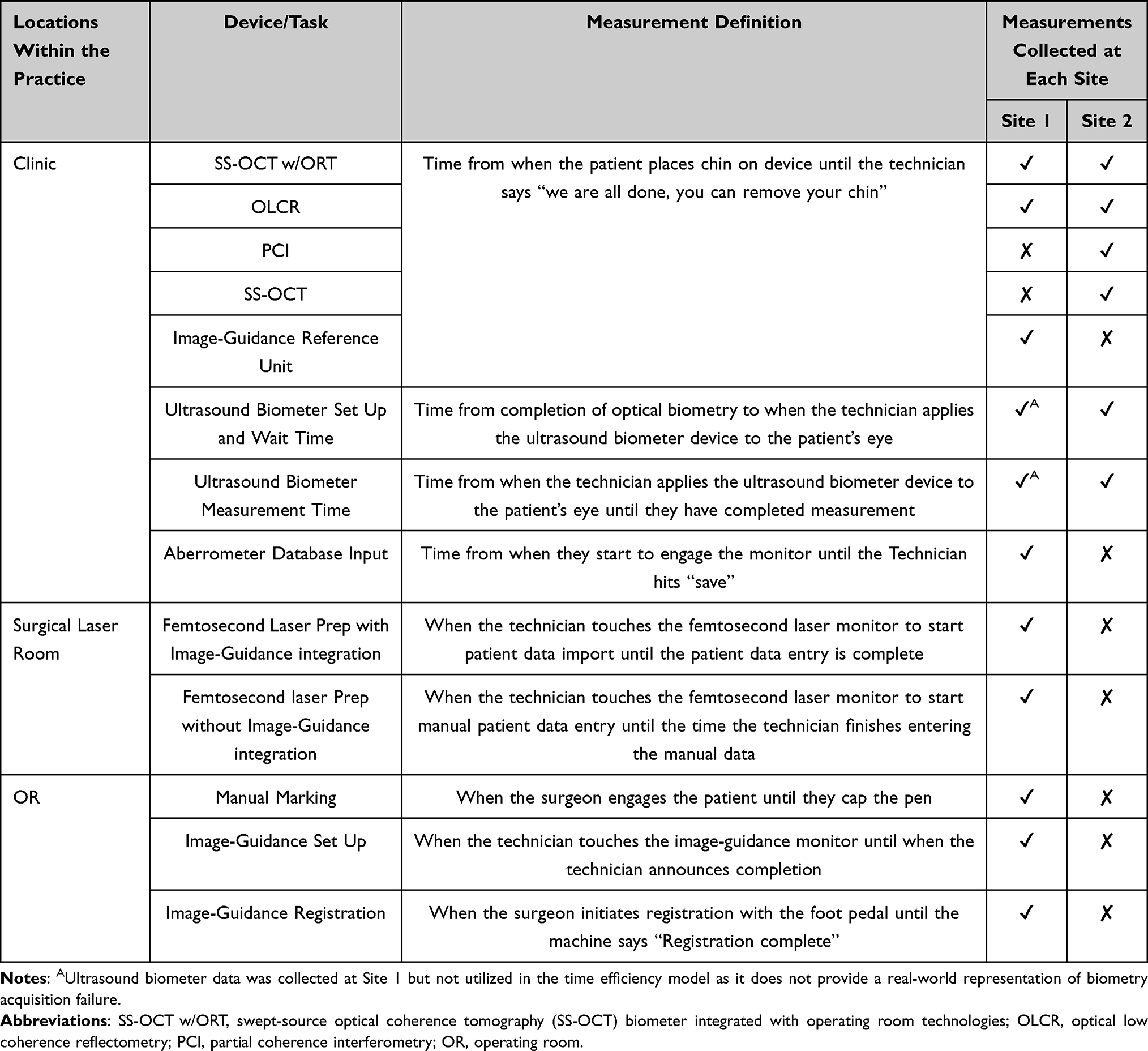 |
Table 1 Measurements Collected at Each Study Site with Pre-Defined Start and End Times |
Data Analysis
Outliers were assessed using the Tukey Method. For both dense and non-dense cataract patients, lower (Q1), middle (Q2 or interquartile range (IQR)), and upper (Q3) quartiles were identified for each biometer. Lower limits were established by subtracting 1.5 from Q1 values and then multiplying by the IQR. Upper limits were instituted by adding 1.5 to Q3 values and then multiplying by the IQR (Supplementary Table 1).15 Biometer measurement times below the lower limit and greater than the upper limit were classified as outliers. If a patient was an outlier for three out of the four biometers from study site 2, their data was removed from the dataset. Although ultrasound biometry measurement time was collected at both study sites, only the measurements collected at study site 2 were summarized and reported as it reflects a real-world representation of its use.
Descriptive statistics for continuous variables (the number of observations, mean and standard deviation (SD)) and for categorical variables (frequency and percentage of patients within each observation group) were summarized. The four groups (SS-OCT w/ORT, OLCR, PCI, and SS-OCT) were compared on mean time spent per patient to complete optical biometry using a one-way analysis of variance (ANOVA) followed by a post-hoc Dunnett’s multiple comparison test to assess differences between an SS-OCT w/ORT and other biometers. To further assess the differences in the average biometry measurement time, patients were stratified by cataract density (dense vs non-dense cataract patients) and compared by biometer as well as across biometers using a one-way ANOVA. A chi-square test with a post-hoc Bonferroni correction was conducted to compare the occurrence of acquisition failure using an SS-OCT w/ORT versus other biometers. All summary statistics and statistical analyses were performed using SAS©, Version 9.3 (SAS Institute, Cary, NC, USA). Outlier assessment was conducted using Microsoft® Office Excel®. The significance level was considered at p ≤ 0.05.
Model Development
Real-world observational data collected at the two study sites was used to develop a value-based efficiency model to demonstrate the combined impact that adopting an SS-OCT w/ORT has on a practice’s cataract evaluation and surgery workflow compared to a clinical workflow using a different biometer. In addition to data inputs from the time-and-motion study, parameters from peer-reviewed literature were leveraged, including the average age of a cataract patient (67.7 years old) and the average patient walking speed based on the 60–69 age group (1.02 m/s).16,17 Furthermore, the model included the following assumptions:
- Diagnostic devices (biometers, image-guided reference unit, ultrasound biometer) within the clinic are assumed to be 10 meters apart.
- Technicians will guide patients between each diagnostic device and will walk at the same speed as the patient (1.02 m/s).
- Technicians will clean each diagnostic device after each use (15 seconds).
- Ultrasound biometry is assumed to be available in-house.
- Within a practice, it is assumed that 50% of patients will receive a conventional IOL and 50% of patients will receive an AT-IOL.
- Only patients receiving an AT-IOL will undergo procedures using the femtosecond laser, image-guidance system (image-guided reference unit, image-guided femtosecond laser, and image-guided optical microscope) and the intraoperative aberrometer.
Two scenarios were utilized to evaluate the efficiency and integration impact of an SS-OCT w/ORT compared to the three other biometers. Each scenario depicts the time taken per 1000 cataract patients undergoing cataract surgery in both eyes. The time savings across the hypothetical cohorts of 1000 cataract patients aim to depict surrogate markers of improved clinical efficiency at the practice-level.
- Scenario 1: The impact of an SS-OCT w/ORT biometer on efficiency in the diagnostic workup (optical biometry measurement, including acquisition failure requiring the use of ultrasound biometry) of a cataract patient compared to an OLCR, a PCI, and an SS-OCT biometer (Figure 1).
- Scenario 2: The impact of an SS-OCT w/ORT biometer on efficiency and integration throughout the clinic evaluation and surgery workflow compared to an SS-OCT biometer – Demonstrating an SS-OCT w/ORT’s ability to integrate with an image-guided femtosecond laser obviating the need to manually enter patient data, an image-guided optical microscope (digital marking) obviating the need to manually mark the patient in the holding room, and automatic data transmission to the intraoperative aberrometer’s cloud-based database obviating the need for manual data entry (Figure 2).
 |
Figure 1 AUltrasound Biometer Wait + Set-Up + Measurement Time, when biometer acquisition failed. Abbreviations: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies; OLCR, optical low coherence reflectometry; PCI, partial coherence interferometry; OR, operating room. |
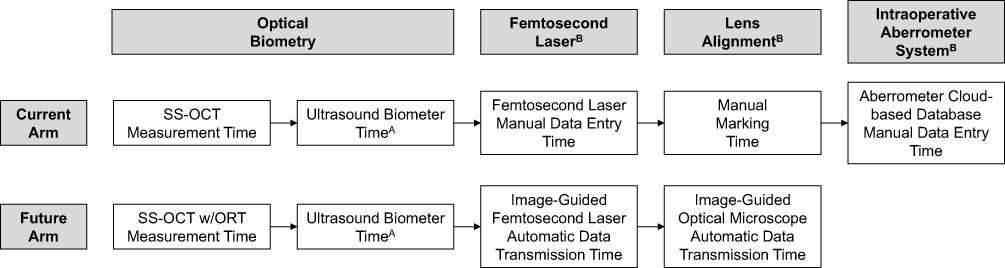 |
Figure 2 AUltrasound Biometer Wait + Set-Up + Measurement Time, when biometer acquisition failed, BTime measurements applied only to patients receiving an advanced technology intraocular lens (IOL), SS-OCT W/ORT replaces the need for the Image-Guided Reference Unit for clinic to OR integration. Abbreviation: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies. |
Results
Twenty-two patients from Site 1 and 190 patients from Site 2 who underwent evaluation for cataract surgery were included in the study. Data for a total of 208 patients (dense (44%) and non-dense cataracts (56%)) were included. Four patients were excluded from the study, a flow-chart of the recruitment and attrition shown in Figure 3. One patient from study site 1 was unable to fixate, one patient was too short to obtain biometer measurements, one patient from study site 2 was classified as monocular, and one patient from study site 2 was identified as an outlier (Tukey Method) for 3 out of the 4 biometer measurements.
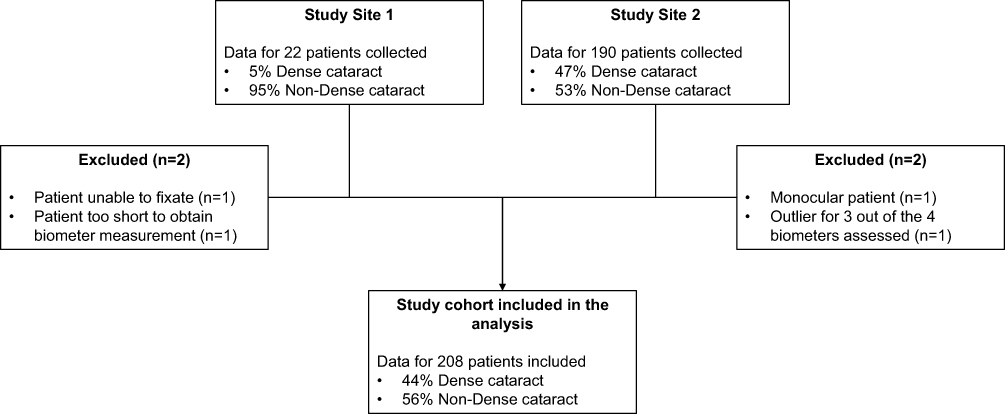 |
Figure 3 Patient enrollment and inclusion from both study sites. |
The average time required to obtain the measurements for the four biometers is shown in Table 2. Significant differences in measurement times were found when comparing all four biometers (p < 0.0001). Compared to the SS-OCT w/ORT biometer (mean: 1.01 minutes; SD: 0.29 minutes), the time required to obtain optical measurements using the OLCR (mean: 1.58 minutes; SD: 0.42 minutes), PCI (mean: 1.71 minutes; SD: 0.43 minutes) and SS-OCT (mean: 1.24 minutes; SD: 0.35 minutes) biometers were significantly higher (p < 0.05). When comparing the average time by density group, non-dense and dense cataracts, the average time taken across all biometers was found to be statistically significantly different (p < 0.0001). Among the patients with dense cataracts, the time required to obtain measurements using the SS-OCT w/ORT biometer was statistically significantly higher (p < 0.05) when compared to all other biometers. Similarly, among the patients with non-dense cataracts, the time required to obtain measurements using the SS-OCT w/ORT biometers was found to be statistically significantly higher (p < 0.05) when compared to all other biometers. When comparing the measurement times for each biometer, the SS-OCT w/ORT, OLCR, and SS-OCT biometer measurement times were significantly faster for the non-dense cataracts compared to the dense cataracts (p < 0.001), but there was no significant difference between the non-dense and dense group for the PCI biometer (p = 0.3776).
 |
Table 2 Average Acquisition Times by Biometer (SS-OCT w/ORT, OCLR, PCI, SS-OCT) for All Patients, and by Cataract Density [Study Site 1 and 2] |
Further assessments were conducted to evaluate the measurement acquisition failure rate among all biometers and by cataract density (Table 3). Among all 188 patients assessed, the acquisition failure rate was highest for the PCI biometer (14.9%) then the OLCR biometer (5.3%) then SS-OCT biometer (2.7%) and lowest for the SS-OCT w/ORT (0%) and were found to be statistically significantly different across all four biometers (p < 0.0001). When comparing the acquisition rate to an SS-OCT w/ORT using the Bonferroni correction, the acquisition failure rate for all three biometers (OLCR: p = 0.004, PCI: p < 0.0001, SS-OCT: p = 0.05) was statistically significantly higher. When assessing the acquisition rate by density, the SS-OCT w/ORT biometer (0%) has a superior acquisition failure rate for dense (0%) and non-dense (0%) cataract patients compared to an OLCR (dense: 10.0% and non-dense: 1.0%), a PCI (dense: 25.6% and non-dense: 5.1%), and an SS-OCT (dense: 5.6% and non-dense: 0%).
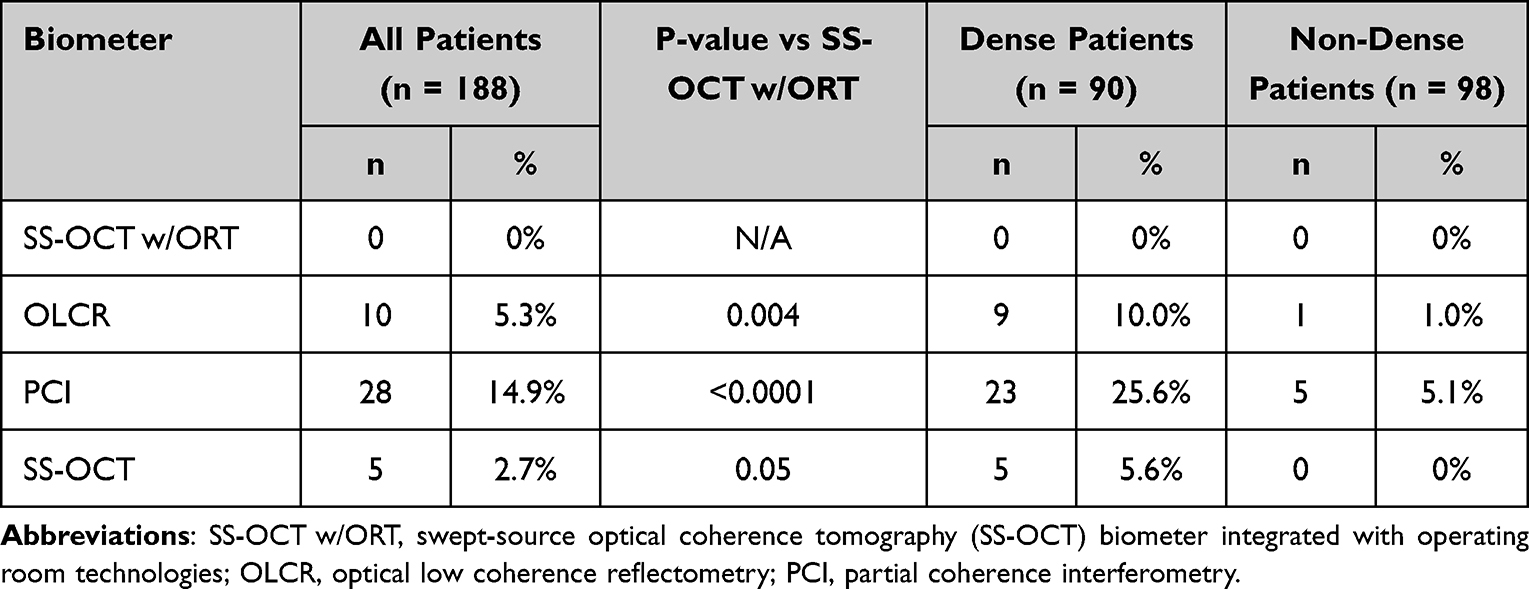 |
Table 3 Acquisition Failure Rate by Biometer for All Patients, and by Cataract Density [Study Site 2] |
The measurement times collected from sites were leveraged to develop the practice-based time efficiency model. In addition to the secondary endpoints from peer-reviewed literature (described in the methods section) and the average optical biometry measurement time and acquisition rate for each biometer’s successful and non-successful biometry acquisitions by cataract density (Supplementary Table 2), additional data points collected from the time-and-motion study were applied to the hypothetical cohort of 1000 patients. The additional data points leveraged in the model included the average surgeon walking speed (1.28 meters/second) used in conjunction with the additional time required for the surgeon to manually mark patients (mean: 0.77 minutes; SD: 0.12 minutes) prior to surgery, time measurements for manual data entry into femtosecond laser without image guidance (mean: 0.39 minutes; SD: 0.02 minutes) and aberrometer cloud-based database (mean: 2.32 minutes; SD: 0.63 minutes), and data transmission times using the femtosecond laser with image guidance (mean: 0.22 minutes; SD: 0.05 minutes) and image-guided optical microscope (digital marking) (mean: 0.42 minutes; SD: 0.15 minutes) (Supplementary Table 3).
Scenario 1 (Diagnostic Evaluation Efficiencies)
For a hypothetical cohort of 1000 patients, an SS-OCT w/ORT’s biometry measurement time is 16 hours and 54 minutes compared to the biometry measurement and ultrasound biometry time for OLCR (28 hours and 50 minutes), PCI (35 hours and 26 minutes), and SS-OCT (21 hours and 46 minutes). Due to faster biometry measurement time and the superior (lower) acquisition failure rate, an SS-OCT w/ORT results in 11 hours and 56 minutes (41% time efficiency), 18 hours and 32 minutes (52% time efficiency), and 4 hours and 52 minutes (22% time efficiency) time savings compared to an OLCR, a PCI, and an SS-OCT, respectively (Figures 4–6).
 |
Figure 4 Efficency Impact of an SS-OCT w/ORT in the Clinic Compared to OLCR per 1,000 Patients (Hours). AUltrasound Biometer Wait + Set-Up + Measurement Time was only collected when biometer acquisition failed. Abbreviations: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies; OLCR, optical low coherence reflectometry. |
 |
Figure 5 Efficency Impact of an SS-OCT w/ORT in the Clinic Compraed to PCI per 1,000 Patients (Hours). AUltrasound Biometer Wait + Set-Up + Measurement Time was only collected when biometer acquisition failed. Abbreviations: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies; PCI, partial coherence interferometry. |
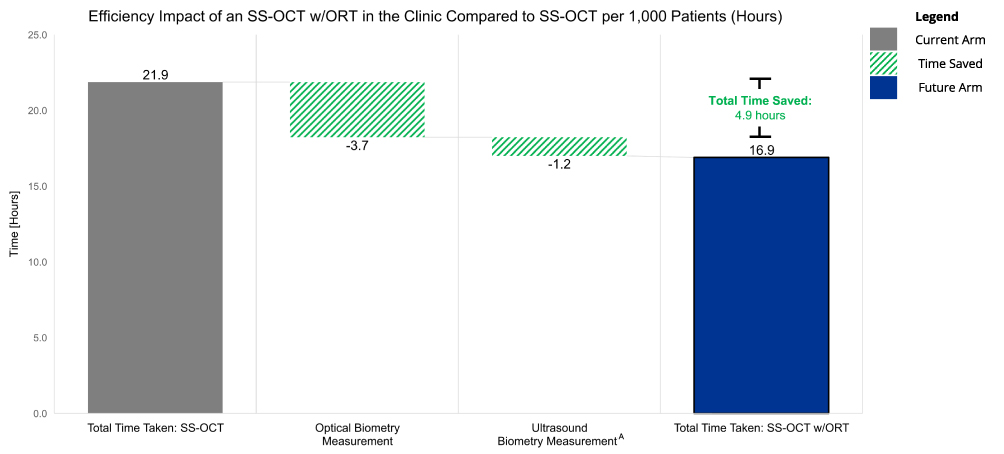 |
Figure 6 Efficieny Impact of an SS-OCT w/ORT in the Clinic Compared to SS-OCT per 1,000 Patients (Hours). AUltrasound Biometer Wait + Set-Up + Measurement Time was only collected when biometer acquisition failed. Abbreviation: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies. |
Scenario 2 (Integration Capabilities)
To further illustrate the impact associated with adopting an SS-OCT w/ORT biometer, Scenario 2 builds upon the base case assessing the diagnostic evaluation efficiencies compared to the SS-OCT biometer. In Scenario 2, the end-to-end impact of adopting an SS-OCT w/ORT and an image-guidance system were assessed for a practice with an SS-OCT, femtosecond laser and intraoperative aberrometer. For a hypothetical cohort of 1000 patients, results from this scenario show that the SS-OCT w/ORT biometer offers time savings within each section of the practice with a total time savings of 30 hours and 27 minutes (58% time efficiency). The SS-OCT w/ORT saves 25 hours and 16 minutes within the clinic (biometer measurement, ultrasound biometry measurement, aberrometry manual data entry time savings), 1 hour and 26 minutes in the surgical laser room (automatic data transmission compared to manual data entry) and 3 hours and 45 minutes in the OR (digital marking vs manual marking) (Figure 7).
 |
Figure 7 Integration Capabilities of an SS-OCT w/ORT in Clinic Evaluation and Surgery Workflow Compared to SS-OCT per 1,000 Patients (Hours). AUltrasound Biometer Wait + Set-Up + Measurement Time was only collected when biometer acquisition failed. Abbreviation: SS-OCT w/ORT, swept-source optical coherence tomography (SS-OCT) biometer integrated with operating room technologies. |
Discussion
This real-world, multi-site, time-and-motion study of cataract patients undergoing evaluation and surgery found that an SS-OCT w/ORT biometer significantly reduces the time required to collect the optical biometry measurements, due to its faster biometry time (~30-second savings on average) and superior acquisition failure rate (0%), compared to a PCI, OLCR, and SS-OCT biometer. Furthermore, statistically significant differences in the biometry measurement times for the SS-OCT w/ORT biometer were found for both dense cataract and non-dense cataract patients when compared to all other biometers assessed, implying an improved performance. As a result of the SS-OCT w/ORT’s integration capabilities, the SS-OCT w/ORT takes ~58% less time than all other biometers during the routine cataract evaluation and surgery workflow, which was interpreted as surrogate markers for improved clinical efficiency and increased patient throughput.
Several previously published studies have sought to assess the impact of optical biometers used in cataract evaluation; however, there have not been any previously published articles that have prospectively compared the performance of four commonly used biometers in cataract patients and assessed by cataract density. Although no previously published articles have assessed all four biometers, similar differences in the measurement times were found by Srivannaboon et al and Passi et al when comparing the SS-OCT biometer against other biometers, these two studies found that the biometry measurement times with the SS-OCT biometer were faster than the PCI and OLCR biometers.9,11 A key performance indicator of an optical biometer is its ability to acquire the biometry measurements essential for biometric formulas, although Srivanaboon et al and Passi et al did not assess the acquisition rates of the biometers, Shammas et al, An et al, Huang et al and Tamaoki et al have assessed the acquisition rate of various biometers on the market, including the SS-OCT w/ORT biometer.8,12–14 All four articles found that the SS-OCT w/ORT biometer has the lowest acquisition rate when compared to all biometers, except when compared to the use of a contact ultrasound biometer. Acquisition rates ranged from 0.6% to 4% for the SS-OCT w/ORT biometer, 3% to 7.4% for the SS-OCT biometer, 15% to 23% for the PCI biometer, and 3% to 21% for the OLCR biometer.8,12–14 Results from these previously published studies are consistent with our study’s findings in that an SS-OCT w/ORT biometer has a lower acquisition failure rate and reduces the need for ultrasound biometry, with this study identifying a 0% acquisition failure rate for all patients, including patients with denser cataracts, and is the first study to quantify the biometry measurement time for an SS-OCT w/ORT biometer in both dense and non-dense cataracts compared to three other biometers. Furthermore, this study is the first to assess the overall impact that an optical biometer has on a practice’s workflow, both within the clinic during cataract evaluation as well as in the surgical laser room and OR during cataract surgery. Owing to its measurement acquisition efficiencies and integration capabilities with devices in the clinic, surgical laser room, and OR, an SS-OCT w/ORT shows significant time savings throughout a cataract surgery practice’s workflow. Future studies should aim to evaluate and quantify whether an SS-OCT w/ORT biometer offers significantly better patient experience and cost-effectiveness compared to other biometers.
There were a few limitations of the study. First, given the COVID-19 pandemic, the research team that collected data at study site 1 differed from study site 2; however, clear measurement definitions with specific start-and-end times, consistent with data collected at study site 1, were pre-defined and on-site research coordinators were trained prior to data collection in an attempt to minimize biases. To further minimize potential bias, a within-subject study design was employed in which each patient observed in the evaluation phase underwent measurements using all biometers. Second, the assessment of cataract density is subjective, and ophthalmologists may employ different scales when assessing cataract density. Even though we standardized the measurement of cataract density grading across both practice sites, the results should be interpreted with caution. Lastly, this study employed several assumptions when building out the practice-based efficiency model, including the distance between devices, the proportion of patients receiving each lens type, and the layout of devices within the practice which may vary by practice. Although the assumptions were drawn from peer-reviewed literature, this limits the generalizability and caution should be exercised when applying these results to other practices.
In conclusion, the results from this real-world observational study and value model demonstrate substantial and significant time efficiencies with an SS-OCT w/ORT biometer, owing to its faster measurement time, lower acquisition failure rate and end-to-end integration capabilities. This study confirms the effectiveness and impact of an SS-OCT w/ORT biometer in significantly reducing execution time, which may translate to improved practice and patient benefits. Greater efficiency may offer improved practice workflow and increased patient throughput at a practice, which may address the expected demand in cataract procedures. In addition to practice benefits, patients may benefit from a potential decrease in wait times as well as improved patient experience and comfort in reducing the use of a contact ultrasound.
Abbreviations
AT-IOL, advanced-technology intraocular lens; BMI, body mass index; IRB, Institutional Review Board; IQR, interquartile range; IOL, intraocular lens; LOCS, Lens Opacity Classification System III; M, meter; NS, Nuclear Sclerosis; OR, operating room; OLCR, optical low-coherence reflectometry; ORA, Optiwave Refractive Analysis; PCI, partial coherence interferometry; PHI, protected health information; S, second; SD, standard deviation; SS-OCT, swept-source optical coherence tomography biometer; SS-OCT w/ORT, swept-source optical coherence tomography biometer integrated with operating room technologies.
Funding
This study was funded by a research grant from Alcon.
Disclosure
Li-Chen Pan and Sean Timmons are employed by Boston Healthcare Associates (a Veranex Company), and at the time this research was performed Manasi Datar was employed by Boston Healthcare Associates. Dr Datar reports that under consulting agreements with RenalytixAI and Foundation Medicine, Veranex received funds to conduct research. Chia-Wen Hsiao, Sun-Ming Pan, and Raiju Babu are employees of Alcon. Dr. Multack and Dr. Woodard are consultants for Alcon. The authors report no other conflicts of interest in this work.
References
1. Lee CM, Afshari NA. The global state of cataract blindness. Curr Opin Ophthalmol. 2017;28(1):98–103. doi:10.1097/ICU.0000000000000340
2. World Health Organization. Ageing and health; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
3. US Dept Of Health and Human Services, Health Resources and Services Administration, Bureau of Health Workforce, National Center for Health Workforce Analysis. National and regional projections of supply and demand for surgical specialty practitioners: 2013–2025. 2016.
4. Turczynowska M, Koźlik-Nowakowska K, Gaca-Wysocka M, Grzybowski A. Effective ocular biometry and intraocular lens power calculation. Eur Ophthal Rev. 2016;10(2):94. doi:10.17925/eor.2016.10.02.94
5. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):P1–P126. doi:10.1016/j.ophtha.2021.10.006
6. Alcon. Alcon cataract refractive surgery diagnostics | MyAlcon professional. Available from: https://professional.myalcon.com/cataract-surgery/cataract-equipment/refractive-diagnostics/.
7. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one-month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/J.JCRS.2016.02.048
8. Shammas HJ, Ortiz S, Shammas MC, Kim SH, Chong C. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J Cataract Refract Surg. 2016;42(1):50–61. doi:10.1016/j.jcrs.2015.07.042
9. Srivannaboon S, Chirapapaisan C, Chonpimai P, Loket S. Clinical comparison of a new swept-source optical coherence tomography-based optical biometer and a time-domain optical coherence tomography-based optical biometer. J Cataract Refract Surg. 2015;41(10):2224–2232. doi:10.1016/j.jcrs.2015.03.019
10. Mylonas G, Sacu S, Buehl W, Ritter M, Georgopoulos M, Schmidt-Erfurth U. Performance of three biometry devices in patients with different grades of age-related cataract. Acta Ophthalmol. 2011;89(3):237–241. doi:10.1111/j.1755-3768.2010.02042.x
11. Passi SF, Thompson AC, Gupta PK. Comparison of agreement and efficiency of a swept source-optical coherence tomography device and an optical low-coherence reflectometry device for biometry measurements during cataract evaluation. Clin Ophthalmol. 2018;12:2245–2251. doi:10.2147/OPTH.S182898
12. An Y, Kang EK, Kim H, Kang MJ, Byun YS, Joo CK. Accuracy of swept-source optical coherence tomography based biometry for intraocular lens power calculation: a retrospective cross-sectional study. BMC Ophthalmol. 2019;19(1):1–7. doi:10.1186/s12886-019-1036-y
13. Huang J, Chen H, Li Y, et al. Comprehensive comparison of axial length measurement with three swept-source OCT-based biometers and partial coherence interferometry. J Refract Surg. 2019;35(2):115–120. doi:10.3928/1081597X-20190109-01
14. Tamaoki A, Kojima T, Hasegawa A, et al. Clinical evaluation of a new swept-source optical coherence biometer that uses individual refractive indices to measure axial length in cataract patients. Ophthalmic Res. 2019;62(1):11–23. doi:10.1159/000496690
15. Seo S, Gary M, Marsh PD. A review and comparison of methods for detecting outliers in univariate data sets. Department of Biostatistics, Graduate School of Public Health; 2006:1–53. Available from: http://d-scholarship.pitt.edu/7948/.
16. Kauh CY, Blachley TS, Lichter PR, Lee PP, Stein JD. Geographic variation in the rate and timing of cataract surgery among US communities. JAMA Ophthalmol. 2016;134(3):267–276. doi:10.1001/jamaophthalmol.2015.5322
17. Xie YJ, Liu EY, Anson ER, Agrawal Y. Age-related imbalance is associated with slower walking speed: an analysis from the national health and nutrition examination survey. J Geriatr Phys Ther. 2017;40(4):183–189. doi:10.1519/JPT.0000000000000093
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.