Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
Immune Response-Related Genes – STAT4, IL8RA and CCR7 Polymorphisms in Lung Cancer: A Case–Control Study in China
Authors Ma Y, Zhou Y, Zhang H, Su X
Received 14 July 2020
Accepted for publication 22 September 2020
Published 21 October 2020 Volume 2020:13 Pages 511—519
DOI https://doi.org/10.2147/PGPM.S271983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Yunfan Ma, Yinxi Zhou, Huixin Zhang, Xiaoan Su
Department of Thoracic Surgery, General Hospital of Ningxia Medical University, Yinchuan, Ningxia 750004, People’s Republic of China
Correspondence: Yunfan Ma
Department of Thoracic Surgery, General Hospital of Ningxia Medical University, #804 Shengli South Road, Xingqing Region, Yinchuan, Ningxia 750004, People’s Republic of China
Tel/Fax +86 951-6743244
Email [email protected]
Purpose: This study aimed to evaluate the associations between immune response-related genes – STAT4, IL8RA and CCR7 polymorphisms and risk of lung cancer.
Methods: Seven polymorphisms of STAT4, IL8RA and CCR7 were genotyped in 350 cases and 350 controls using a MassARRAY platform.
Results: The STAT4 rs1400656-G and rs7574865-T alleles may decrease the susceptibility to lung cancer (prs1400656= 0.020; prs7574865= 0.014); while IL8RA rs1008562-C and CCR7 rs3136685-T alleles may increase the risk of disease (prs1008562< 0.001; prs3136685= 0.018). The STAT4 rs1400656-GA and rs7574865-GT genotypes were determined as protective genotypes against lung cancer risk (prs1400656= 0.048; prs7574865= 0.042). However, IL8RA rs1008562-CG/GG and CCR7 rs3136685-TT genotypes were significantly associated with an elevated risk of disease (prs1008562< 0.0001; prs3136685= 0.020). Genetic model analysis revealed that STAT4 rs1400656 and rs7574865 were relate to a declining risk of disease under dominant and log-additive models (rs1400656: p dominant = 0.014, p log-additive= 0.016; rs7574865: p dominant = 0.013, p log-additive= 0.013). In contrast, IL8RA rs1008562 exhibited a strong correlation with an elevated risk of lung cancer under all three models (p dominant < 0.0001, p recessive = 0.011, p log-additive< 0.0001). Moreover, CCR7 rs3136685 was correlated with an increased risk of disease under recessive and log-additive models (p recessive = 0.007, p log-additive= 0.019); and CCR7 rs17708087 was also identified as a risk factor in the dominant model (p = 0.038).
Conclusion: These results widen the scope of knowledge about the association between STAT4, IL8RA and CCR7 polymorphisms and risk of lung cancer.
Keywords: lung cancer, signal transducers and activators of transcription 4, STAT4, interleukin 8-receptor alpha, IL8RA, Chemokine (C-C motif) receptor 7, CCR7, single nucleotide polymorphisms, SNPs
Introduction
Lung cancer is the most common diagnosed malignant tumor, with the fastest growing morbidity and mortality rates compared with other types of tumors.1 The 5-year survival rate for lung cancer patients depends on the stage when they were diagnosed: early detection and treatment can significantly improve the prognosis of patients.2 Lung cancer has obvious familial aggregation and genetic predisposition.3 Thus, identification of individuals with a high risk of lung cancer will help people focus on their body health; and a personalized and comprehensive response plan, including tobacco prevention, healthy diet, proper exercise, periodic physical examination and so on, will finally decrease the incidence of disease. With the awareness of genetic counseling, single nucleotide polymorphisms (SNPs) are extensively used to evaluate the susceptibility to cancer.4–6 However, it still needs a great effort to find more SNPs to draw the genetic map of lung cancer.
The Nobel Prize on tumor immunotherapy provided us clues that SNPs on immune response related genes may influence the genetic predisposition to lung cancer to a large extent.7 In this study, we focused on three immune response related genes: signal transducers and activators of transcription 4 (STAT4), interleukin 8-receptor alpha (IL8RA) and Chemokine (C-C motif) receptor 7 (CCR7). STAT4 can change the tumor microenvironment by influencing the level of growth factors and cytokines, which may have indirect effects on tumor cell growth and apoptosis.8 IL8RA may have associations with serum IgE levels, and IL8RA polymorphisms were associated with risk of bronchial asthma.9 CCR7 can induce cells to lymphoid organs, and its expression is associated with lymph node metastasis of cancer.10 However, to date, few studies focus on the STAT4, IL8RA and CCR7 polymorphisms in lung cancer.
Seven SNPs were chosen as candidate SNPs in this study: rs1400656, rs7574865, rs11685878 on STAT4; rs1008562 and rs3138060 on IL8RA; and rs3136685 and rs17708087 on CCR7. A case-control study in an Indian population reported that rs1400656 might affect genetic susceptibility to asthma.11 rs7574865 and rs11685878 have been investigated in the virus infection and clearance in a Chinese population.12 rs1008562 was correlated with an increased risk of colorectal cancer,13 and rs3138060 was related to bacterial infection in the urinary tract.14 The rs3136685 was selected because of its correlation with prostate cancer risk,15 and rs17708087 may exert an influence on myocardial infarction.16 In this study, we genotyped these genetic polymorphisms in lung cancer patients and healthy controls, and aimed at improving our understanding of genetic predisposition to lung cancer.
Subjects and Methods
Subjects
A total of 350 lung cancer cases and 350 healthy controls were collected at the General Hospital of Ningxia Medical University. The diagnosis of lung cancer was established by histopathological examination of biopsy or resected tissue specimens. All the cases were more than 18 years old and had no history of any malignancy. The patients who had received chemo or radiotherapy were excluded. The controls were recruited at the physical examination center of our hospital, with no history of any malignant disorder or serious disease. Controls who were under 18 years old were excluded.
The sample size was calculated using Sampsize online tool (http://sampsize.sourceforge.net/iface/s3.html), and followed by the conditions: α=0.05, power=0.90, and expected OR=1.8. The calculated sample size was 318 in both the case and control groups. The sample size was therefore sufficient.
The basic characteristics of the participants are described in Table 1. The cases include 180 males and 170 females, 187 smokers and 163 nonsmokers, with a mean age of 56.9 years; and the control group contains 175 males and 175 females, 180 smokers and 170 nonsmokers, with a mean age of 58.1 years. No significant difference was observed in the distribution of sex, age, or smoking status between the two groups (p > 0.05).
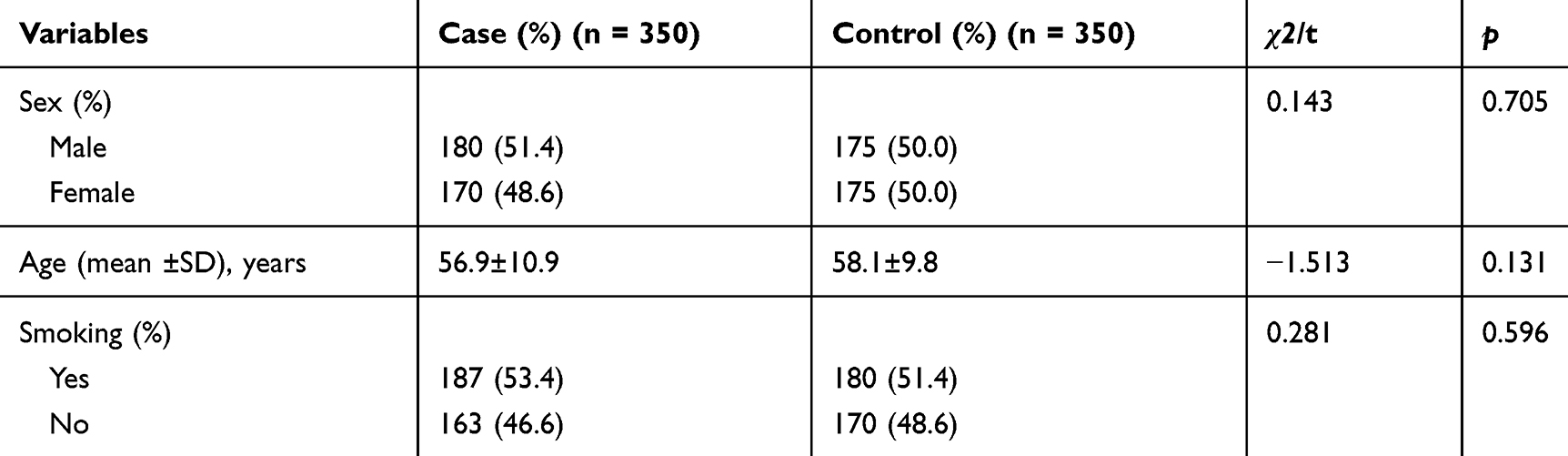 |
Table 1 The Basic Characteristics of the Participants |
Two milliliters of whole blood was collected from each subject into tubes containing ethylenediaminetetraacetic acid. After centrifugation, the samples were stored at −80 °C until further use.
We obtained written informed consent from each subject, and the study was approved by the Ethics Department of General Hospital of Ningxia Medical University and carried out in accordance with the World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects.
SNP Selection and Genotyping
Seven tag SNPs in immune response genes STAT4, IL8RA and CCR7 were selected based on previous association studies on cancers and pulmonary disease. All of the SNPs are with minor allele frequency (MAF) > 5% in Asian populations of the NCBI database. Tag SNPs were selected with linkage disequilibrium (LD) greater than 0.8 using HaploView.
DNA was extracted using a PureLink™ Pro 96 Genomic DNA Purification Kit (Invitrogen, Carlsbad, CA). Primers were designed using Sequenom MassARRAY Assay Design 3.0 software and listed in Table 2. Genotyping was performed on Mass ARRAY iPLEX (Sequenom, San Diego, CA, USA) platform using a matrix-assisted laser desorption ionization time of flight (MALDI-TOF) mass spectrometer. The results were output by Sequenom TYPER 4.0 software.17
 |
Table 2 The Primers Used in This Study |
Statistical Analysis
Statistical analysis was performed with SPSS package version 20.0 (SPSS, Chicago, IL, USA). Minor allele frequencies (MAFs) of each SNP were checked for divergence from Hardy–Weinberg equilibrium (HWE). HaploReg v4.1 (https://pubs.broadinstitute.org/mammals/haploreg/haploreg.php) was used to predict the potential functions of the SNPs. Allele and genotype frequencies in the cases and controls were evaluated using Chi-square tests. The association between SNPs and lung cancer risk were evaluated using SNPstats (https://www.snpstats.net/start.htm) and expressed by odds ratios (ORs) and 95% confidence intervals (CIs). Statistical significance was established when p < 0.05.
Results
The position of candidate SNPs and predicted function are listed in Table 3. The predicted function according to the HaploReg database showed that the seven SNPs were involved in the changes of reference epigenomes (regulation of the promoter and/or enhancer histone), regulatory motifs, and expression quantitative trait loci (eQTL).
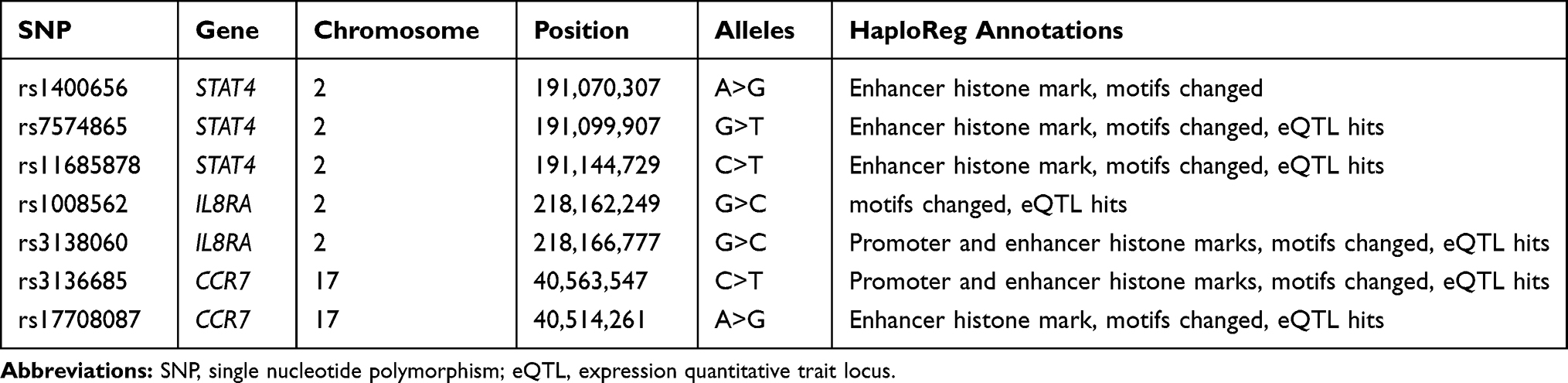 |
Table 3 Basic Information and Predicted Functions of Candidate SNPs |
The MAFs of SNPs in cases and controls are listed in Table 4. All SNPs were consistent with HWE (p > 0.05). Comparing the MAF of each SNP between cases and controls, we found that four SNPs had potential influence on lung cancer risk: rs1400656, rs7574865, rs1008562 and rs3136685. The minor alleles of rs1400656 and rs7574865 may decrease the susceptibility to lung cancer (rs1400656: OR = 0.694, 95% CI: 0.510–0.945, p = 0.020; rs7574865: OR = 0.735, 95% CI: 0.574–0.941, p = 0.014). However, the minor alleles of rs1008562 and rs3136685 may increase the risk of lung cancer (rs1008562: OR = 1.655, 95% CI: 1.332–2.057, p < 0.001; rs3136685: OR = 1.309, 95% CI: 1.048–1.634, p = 0.018).
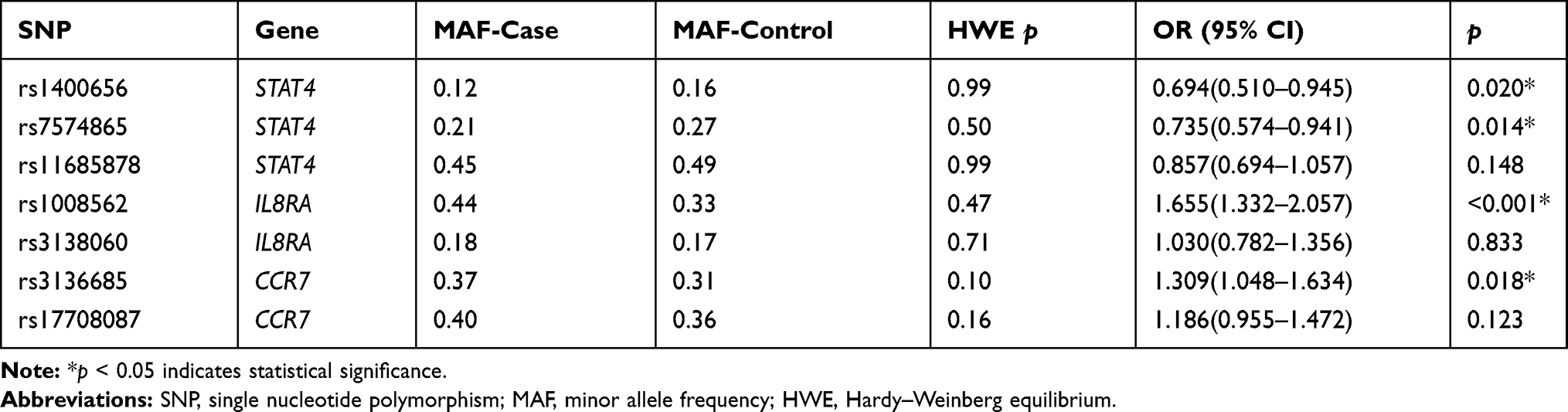 |
Table 4 Allele Frequency Distributions Among Lung Cancer Cases and Healthy Controls |
The genotype frequencies of SNPs among cases and controls are presented in Table 5. Compared with the AA genotype, the GA genotype frequency of rs1400656 was lower in cases than in controls, thus the GA of rs1400656 was considered as a protective genotype against lung cancer risk (OR = 0.66, 95% CI: 0.46–0.94, p = 0.048). Moreover, the GT genotype of rs7574865 was also correlated with a reduced risk of lung cancer (OR = 0.70, 95% CI: 0.51–0.96, p = 0.042). However, the CG and GG genotypes of rs1008562 were significantly associated with a 1.92-fold and 2.50-fold increased risk of disease, respectively (p < 0.0001). The TT genotype of rs3136685 was also correlated with a 2.09-fold elevated risk of disease (95% CI: 1.23–3.54, p = 0.020).
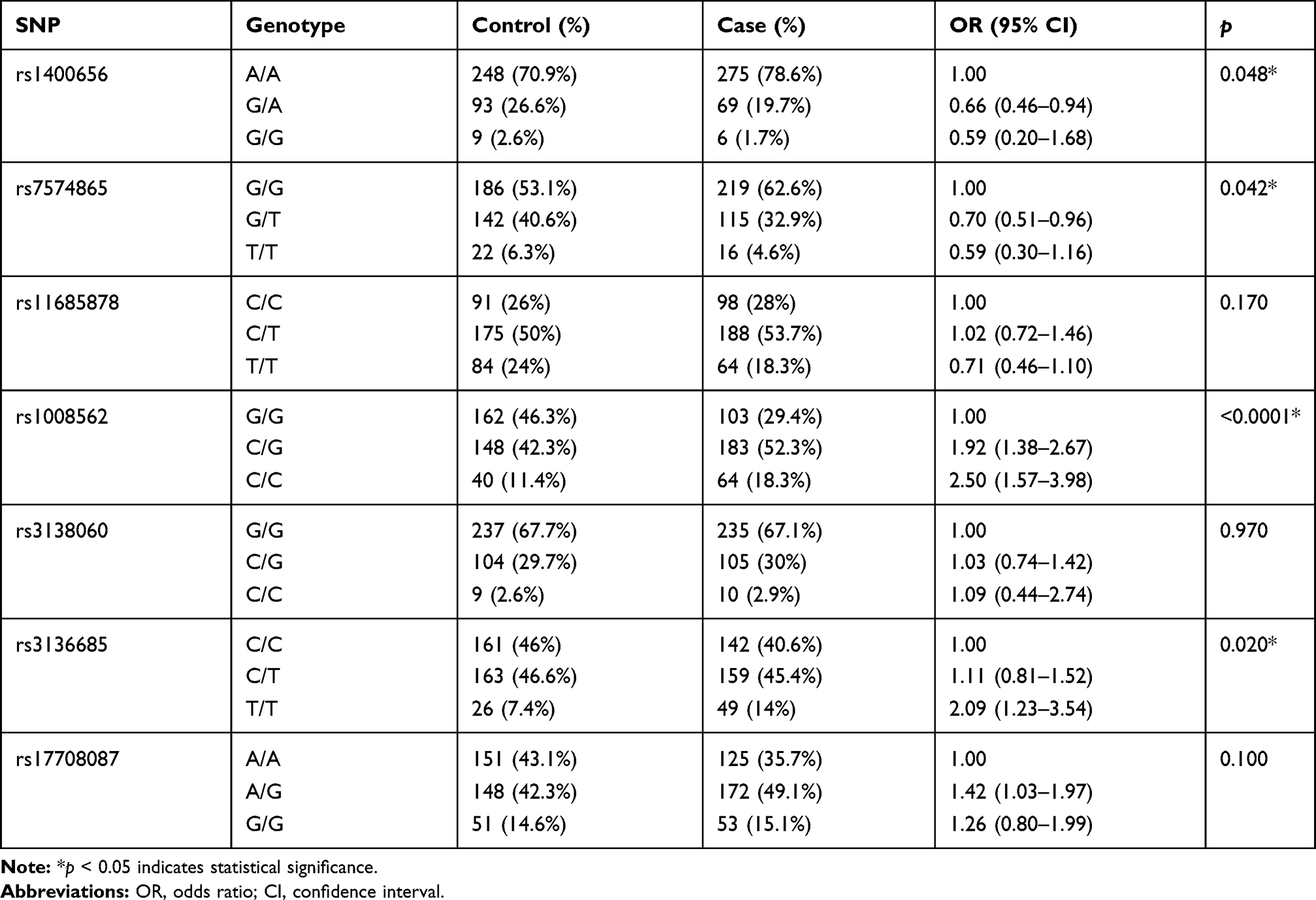 |
Table 5 Genotype Frequency Distributions Among Lung Cancer Cases and Healthy Controls |
The effects of candidate SNPs on the risk of lung cancer were further evaluated under genetic models (Table 6). The minor alleles of rs1400656 and rs7574865 were related to a declining risk of disease under dominant and log-additive models (rs1400656: p dominant = 0.014, p log-additive= 0.016; rs7574865: p dominant = 0.013, p log-additive= 0.013). In contrast, the allele C of rs1008562 exhibited a strong correlation with an elevated risk of lung cancer under all three models (p dominant < 0.0001, p recessive = 0.011, p log-additive< 0.0001). The allele T of rs3136685 was correlated with an elevated risk of disease under recessive and log-additive models (p recessive = 0.007, p log-additive= 0.019). In addition, the allele G of rs17708087 was also identified as a risk allele in the dominant model (p = 0.038).
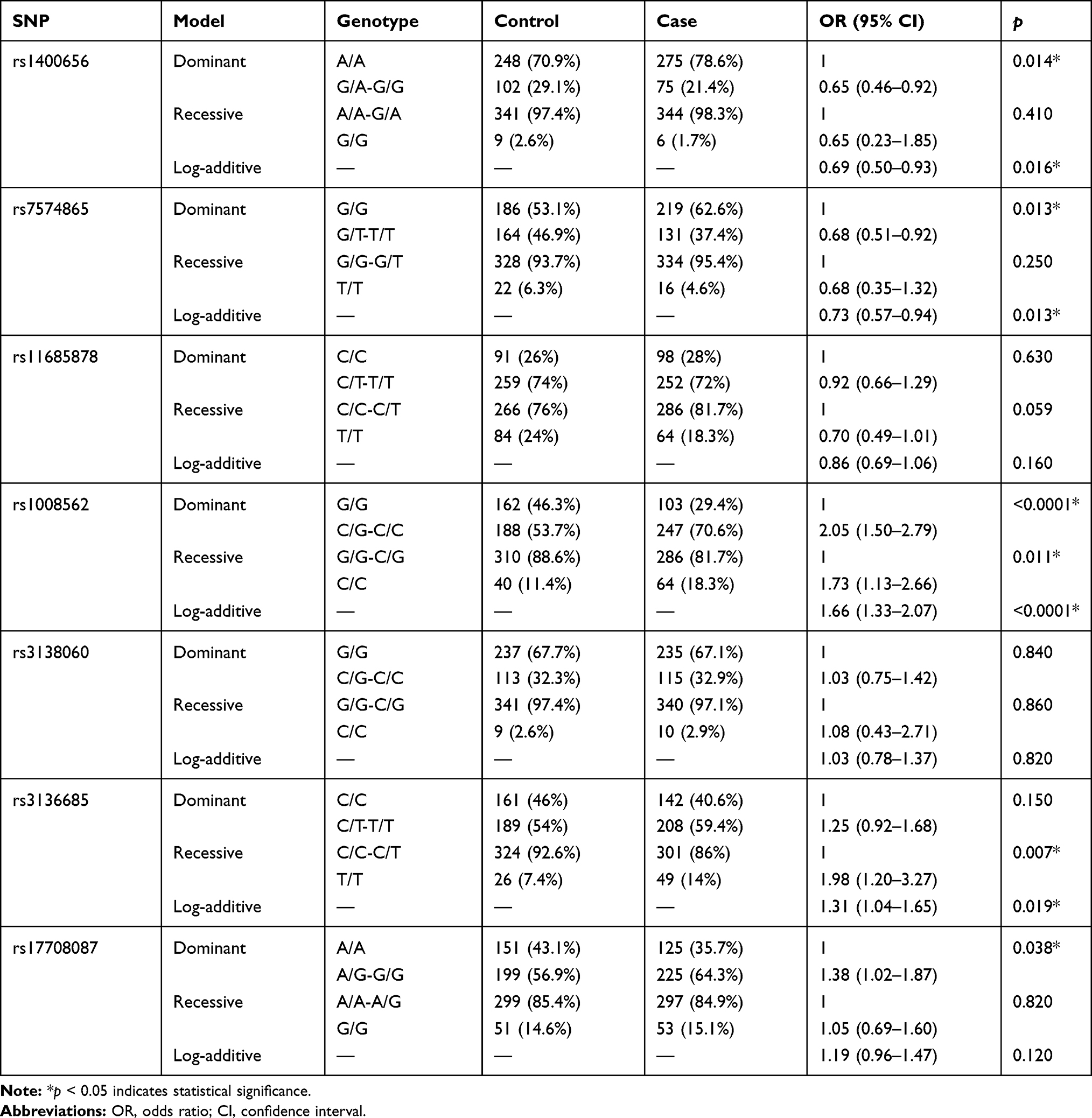 |
Table 6 Association Between Candidate SNPs and Risk of Lung Cancer in Three Genetic Models |
Smoking is an important risk factor for lung cancer. So a stratification analysis was conducted (Table 7). The rs1400656 polymorphism was correlated to a reduced risk of disease in smokers (p dominant = 0.019, p log-additive= 0.015), while rs7574865 exhibited a declining risk of disease in nonsmokers (p dominant = 0.046, p log-additive= 0.031). In contrast, rs1008562 polymorphism was associated with an elevated risk of disease in both subgroups (smokers: p dominant = 0.001, p log-additive= 0.003; nonsmokers: p dominant = 0.003, p log-additive= 0.001). In addition, rs3136685 has influence on lung cancer risk only in nonsmokers (p dominant = 0.033, p recessive = 0.027, p log-additive= 0.008).
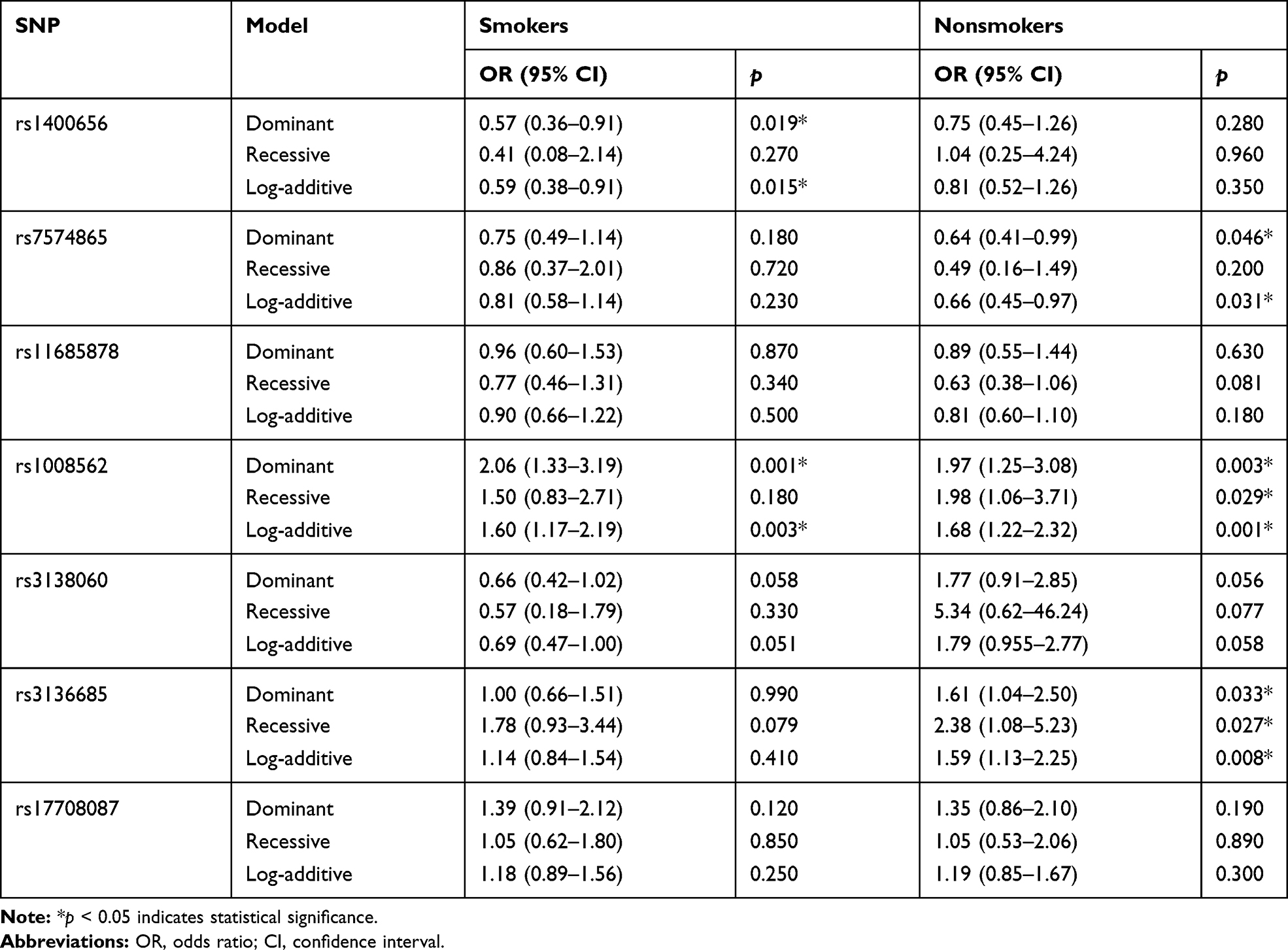 |
Table 7 Association of Candidate SNPs with the Risk of Lung Cancer in Smokers and Nonsmokers |
Discussion
Immune response has always been the research hotspot in the study of cancer prevention and treatment in the last few years.18 In this study, we took immune response genes STAT4, IL8RA and CCR7 as the starting point, and explored the association between seven SNPs on these genes and lung cancer risk. We identified that two SNPs (STAT4 rs1400656 and rs7574865) had a protective role against the risk of disease, and three SNPs (IL8RA rs1008562, CCR7 rs3136685 and rs17708087) may increase the risk of disease.
STAT4 is involved in a variety of immune response processes, including production of interferon-γ (IFN-γ), signal transduction of IL-12, -23, IFN and other cytokines in immune cells, differentiation and activation of immune cells, and so on.19 STAT4 polymorphisms have been extensively investigated in several kinds of immune regulation disorders, such as rheumatoid arthritis, polymyositis/dermatomyositis, intestinal Behcet’s disease, and systemic lupus erythematous.20–22 In recent years, the important role of STAT4 polymorphisms has been gradually found in the genesis and progression of liver cancer. A meta-analysis reported that rs7574865 G allele was correlated with an increased risk of HBV-induced liver cancer.23 We identified that minor allele T of rs7574865 might be a protective allele for the risk of lung cancer, suggesting that rs7574865 polymorphism may have a similar influence on the occurrence of cancer. In addition, we also determined rs1400656 G allele as a protective allele against the risk of disease. However, due to the limited literature, the protective effects of rs1400656 and rs7574865 on lung cancer need to be further verified.
IL8RA (also known as CXCR1) is one of the receptors of IL8 (also known as CXCL8). Their binding proteins take part in the initiation and progression of several kinds of cancers via PI3K and MAPK pathway.24 Stimulation of IL8 in lung cancer cells was mediated by IL8RA and EGFR to a large extent.25 Lee et al have reported that the interaction of IL8RA rs2234671 (C/G) and smoke exposure was substantially correlated with the lung cancer risk.26 Slattery et al demonstrated that IL8RA rs1008562 in the CHIEF pathway had significant associations with rectal cancer.27 In this study, we found that rs1008562 exhibited a strong relationship with the risk of lung cancer, suggesting that rs1008562 polymorphism may also exert an influence on the development of lung cancer via the network of the CHIEF pathway.
CCR7 has two ligands CCL19 and CCL21, which are mainly expressed in lymphatic organs. CCR7 can induce immune cells towards the lymphatic organs, which means it plays a crucial role in the migration of tumor cells.28 Wang et al has found that the up-regulation of HIF-1α and HIF-2α could improve the expression of CCR7 under hypoxia conditions, and led to the metastasis of lung cancer.29 In this study, we compared the CCR7 rs3136685 and rs17708087 polymorphisms between lung cancer patients and a heathy control, and found that both polymorphisms had a strong correlation with lung cancer risk, suggesting they might be used as biomarkers to identify the high-risk groups. Moreover, considering the specific role of CCR7 on metastasis, we will further investigate the association between its polymorphisms and prognosis of lung cancer patients in a future study.
The effects of genetic polymorphisms on lung cancer risk can be significantly different in smokers and nonsmokers,30 so we conduct a stratification analysis. The rs1008562 polymorphism was associated with risk of disease in both of subgroups, suggesting that rs1008562 polymorphism was a significant risk factor. While rs1400656, rs7574865 and rs3136685 were significant only in one subgroup, we speculated it may be due to the limited sample size.
Although the present study provided novel susceptible SNPs for lung cancer, it has some inevitable disadvantages. Firstly, we were unable to collect information about the pathological types and treatment regimens, and therefore, we cannot conduct the stratification analysis according to pathological type, and evaluate the effect of these polymorphisms on the response to treatment. Secondly, the current results are insufficient to explain the molecular pathogenesis of the disease. Thirdly, the sample size was modest, and the allele and genotype frequency of SNPs could be variable among different populations, thus the results identified here should be verified in a larger sample size and different populations.
In conclusion, we found that two SNPs (STAT4 rs1400656 and rs7574865) had a protective role against the risk of lung cancer, and three SNPs (IL8RA rs1008562, CCR7 rs3136685 and rs17708087) may increase the risk of disease. These results widen the scope of knowledge about the association between immune response genes, STAT4, IL8RA and CCR7 polymorphisms, and risk of the disease.
Acknowledgments
This work was supported by the Colleges and Universities Science Research Program of Ningxia [Grant number: NGY2016092].
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Hong QY, Wu G-M, Qian GS, et al. Prevention and management of lung cancer in China. Cancer. 2015;121(Suppl S17):3080–3088. doi:10.1002/cncr.29584
3. Wang J, Liu Q, Yuan S, et al. Genetic predisposition to lung cancer: comprehensive literature integration, meta-analysis, and multiple evidence assessment of candidate-gene association studies. Sci Rep. 2017;7(1):8371. doi:10.1038/s41598-017-07737-0
4. Thomas M, Sakoda LC, Hoffmeister M, et al. Genome-wide modeling of polygenic risk score in colorectal cancer risk. Am J Hum Genet. 2020;107(3):432–444. doi:10.1016/j.ajhg.2020.07.006
5. Kumaran M, Ghosh S, Joy AA, et al. Fine-mapping of a novel premenopausal breast cancer susceptibility locus at Chr4q31.22 in Caucasian women and validation in African and Chinese women. Int J Cancer. 2020;146(5):1219–1229. doi:10.1002/ijc.32407
6. Mokhtarian R, Tabatabaeian H, Saadatmand P, et al. CD44 gene rs8193 C allele is significantly enriched in gastric cancer patients. Cell J. 2020;21(4):451–458. doi:10.22074/cellj.2020.6389
7. Rotte A, D’Orazi G, Bhandaru M. Nobel committee honors tumor immunologists. J Exp Clin Cancer Res. 2018;37(1):1–3. doi:10.1186/s13046-018-0937-6
8. Li J, Liang L, Liu Y, et al. Clinicopathological significance of STAT4 in hepatocellular carcinoma and its effect on cell growth and apoptosis. Onco Targets Ther. 2016;9:1721–1734. doi:10.2147/OTT.S100040
9. Voron’ko OE, Dmitrieva-Zdorova EV, Gabaeva MV, et al. M31R and R335C polymorphic variants of the IL8RA gene in Russian and Buryat patients with atopic bronchial asthma. Genetika. 2011;47(9):1247–1253.
10. van den Bosch T, Koopmans AE, Vaarwater J, van den Berg M, de Klein A, Verdijk RM. Chemokine receptor CCR7 expression predicts poor outcome in uveal melanoma and relates to liver metastasis whereas expression of CXCR4 is not of clinical relevance. Invest Ophthalmol Vis Sci. 2013;54(12):7354–7361. doi:10.1167/iovs.13-12407
11. Kumar A, Das S, Agrawal A, Mukhopadhyay I, Ghosh B. Genetic association of key Th1/Th2 pathway candidate genes, IRF2, IL6, IFNGR2, STAT4 and IL4RA, with atopic asthma in the Indian population. J Hum Genet. 2015;60(8):443–448. doi:10.1038/jhg.2015.45
12. Jiang X, Su K, Tao J, et al. Association of STAT4 polymorphisms with hepatitis B virus infection and clearance in Chinese Han population. Amino Acids. 2016;48(11):2589–2598. doi:10.1007/s00726-016-2283-3
13. Bondurant KL, Lundgreen A, Herrick JS, Kadlubar S, Wolff RK, Slattery ML. Interleukin genes and associations with colon and rectal cancer risk and overall survival. Int J Cancer. 2013;132(4):905–915. doi:10.1002/ijc.27660
14. Han SS, Lu Y, Chen M, Xu YQ, Wang Y. Association between interleukin 8‐receptor gene (CXCR1 and CXCR2) polymorphisms and urinary tract infection: evidence from 4097 subjects. Nephrology (Carlton). 2019;24(4):464–471. doi:10.1111/nep.13260
15. Dubey B, Jackson MD, Zeigler-Johnson C, et al. Inflammation polymorphisms and prostate cancer risk in Jamaican men: role of obesity/body size. Gene. 2017;636:96–102. doi:10.1016/j.gene.2017.09.016
16. Wołkow P, Drabik L, Totoń‐Żurańska J, et al. Polymorphism in the chemokine receptor 7 gene (CCR 7) is associated with previous myocardial infarction in patients undergoing elective coronary angiography. Int J Immunogenet. 2016;43(4):218–225. doi:10.1111/iji.12270
17. Gabriel S, Ziaugra L, Tabbaa D. SNP genotyping using the sequenom massARRAY iPLEX platform. Curr Protoc Hum Genet. 2009. doi:10.1002/0471142905.hg0212s60
18. Medler TR, Cotechini T, Coussens LM. Immune response to cancer therapy: mounting an effective antitumor response and mechanisms of resistance. Trends Cancer. 2015;1(1):66–75. doi:10.1016/j.trecan.2015.07.008
19. Korman BD, Kastner DL, Gregersen PK, Remmers EF. STAT4: genetics, mechanisms, and implications for autoimmunity. Curr Allergy Asthma Rep. 2008;8(5):398–403. doi:10.1007/s11882-008-0077-8
20. Ji JD, Lee WJ, Kong KA, et al. Association of STAT4 polymorphism with rheumatoid arthritis and systemic lupus erythematosus: a meta-analysis. Mol Biol Rep. 2010;37(1):141–147. doi:10.1007/s11033-009-9553-z
21. Sugiura T, Kawaguchi Y, Goto K, et al. Positive association between STAT4 polymorphisms and polymyositis/dermatomyositis in a Japanese population. Ann Rheum Dis. 2012;71(10):1646–1650. doi:10.1136/annrheumdis-2011-200839
22. Kim ES, Kim SW, Moon CM, et al. Interactions between IL17A, IL23R, and STAT4 polymorphisms confer susceptibility to intestinal Behcet’s disease in Korean population. Life Sci. 2012;90(19–20):740–746. doi:10.1016/j.lfs.2012.03.017
23. Shi H, He H, Ojha SC, et al. Association of STAT3 and STAT4 polymorphisms with susceptibility to chronic hepatitis B virus infection and risk of hepatocellular carcinoma: a meta-analysis. Biosci Rep. 2019;39(6):BSR20190783. doi:10.1042/BSR20190783
24. Liu Q, Li A, Tian Y, et al. The CXCL8-CXCR1/2 pathways in cancer. Cytokine Growth Factor Rev. 2016;31:61–71. doi:10.1016/j.cytogfr.2016.08.002
25. Luppi F, Longo A, De Boer W, Rabe K, Hiemstra P. Interleukin-8 stimulates cell proliferation in non-small cell lung cancer through epidermal growth factor receptor transactivation. Lung Cancer. 2007;56(1):25–33. doi:10.1016/j.lungcan.2006.11.014
26. Lee K-M, Shen M, Chapman RS, et al. Polymorphisms in immunoregulatory genes, smoky coal exposure and lung cancer risk in Xuan Wei, China. Carcinogenesis. 2007;28(7):1437–1441. doi:10.1093/carcin/bgm030
27. Slattery ML, Lundgreen A. The influence of the CHIEF pathway on colorectal cancer-specific mortality. PLoS One. 2014;9(12):e116169. doi:10.1371/journal.pone.0116169
28. Legler DF, Uetz-von Allmen E, Hauser MA. CCR7: roles in cancer cell dissemination, migration and metastasis formation. Int J Biochem Cell Biol. 2014;54:78–82. doi:10.1016/j.biocel.2014.07.002
29. Li Y, Qiu X, Zhang S, Zhang Q, Wang E. Hypoxia-induced CCR7 expression via HIF-1α and HIF-2α correlates with migration and invasion in lung cancer cells. Cancer Biol Ther. 2009;8(4):322–330. doi:10.4161/cbt.8.4.7332
30. Sun S, Schiller JH, Gazdar AF. Lung cancer in never smokers—a different disease. Nat Rev Cancer. 2007;7(10):778–790. doi:10.1038/nrc2190
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.