Back to Journals » International Medical Case Reports Journal » Volume 19
Immune-Mediated IgA Nephropathy Induced by PD-1 Blockade in Extranodal NK/T-Cell Lymphoma
Authors Mohammadi N, Li F, Wang H, Mohammadi A, Wang L ![]() , Cong J
, Cong J ![]()
Received 26 January 2026
Accepted for publication 28 May 2026
Published 9 June 2026 Volume 2026:19 593548
DOI https://doi.org/10.2147/IMCRJ.S593548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Niloofar Mohammadi,1 Fuli Li,2 Henan Wang,2 Alireza Mohammadi,3 Liang Wang,2 Jia Cong2
1Department of Medicine, Capital Medical University, Beijing, People’s Republic of China; 2Department of Hematology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Medicine, Qeshem International Branch, Islamic Azad University of Medical Sciences, Hormozgan, Iran
Correspondence: Jia Cong, Department of Hematology, Beijing Tongren Hospital, Capital Medical University, No. 3 Xihuan South Road, Daxing District, Beijing, People’s Republic of China, Tel +8615810595387, Email [email protected]
Abstract: A man in his early fifties was diagnosed with extranodal natural killer/T-cell lymphoma involving the nasal cavity and cervical lymph nodes. At the time of diagnosis, renal function was entirely normal. He was started on first-line combination therapy consisting of a PD-1 monoclonal antibody, pegaspargase, the histone deacetylase inhibitor chidamide, and systemic corticosteroids, with an early and favorable clinical response of the lymphoma. However, prior to the second treatment cycle, routine laboratory evaluation revealed new-onset proteinuria accompanied by a rising serum creatinine level. Subsequent renal biopsy demonstrated IgA-dominant immune complex deposition with crescent formation, consistent with rapidly progressive IgA glomerulonephritis. The immune checkpoint inhibitor was promptly discontinued, and high-dose corticosteroid therapy was initiated, followed by cyclophosphamide. Renal function showed partial but meaningful improvement. Given the renal toxicity, systemic immunotherapy was withheld, and the lymphoma was subsequently managed successfully with radiotherapy alone. At twelve months of follow-up, the patient remained in complete oncologic remission, with markedly improved renal parameters. This case highlights a rare presentation of rapidly progressive IgA nephropathy associated with PD-1 blockade in extranodal NK/T-cell lymphoma, a relationship that remains insufficiently characterized in current literature. It emphasizes the importance of close and regular monitoring of renal function and urinalysis during immunotherapy. Early recognition of renal involvement, together with timely discontinuation of the immune checkpoint inhibitor and appropriate immunosuppressive treatment, may preserve kidney function while still allowing effective control of the underlying malignancy.
Keywords: extranodal NK/T-cell lymphoma, immune checkpoint inhibitor, IgA nephropathy, rapidly progressive glomerulonephritis, drug-induced nephrotoxicity
Introduction
Extranodal NK/T-cell lymphoma (ENKTL), nasal type, is a distinct and highly aggressive subtype of non-Hodgkin lymphoma, with a well-established etiological association with Epstein–Barr virus (EBV) infection.1–3 It accounts for fewer than 10% of non-Hodgkin lymphoma cases in endemic regions such as East Asia and Latin America and is far less prevalent in Western populations.4,5 Patients most commonly present with sinonasal involvement, characterized by nasal obstruction, epistaxis, and progressive midline destructive lesions.6,7
The treatment approach for ENKTL has evolved substantially over the past two decades. Traditional anthracycline-based regimens, such as CHOP, have demonstrated limited efficacy and have largely been replaced by L-asparaginase–based protocols, frequently administered in combination with radiotherapy.8,9
More recently, the emergence of immunotherapeutic and molecularly targeted approaches has further expanded the treatment landscape. Immune checkpoint inhibition targeting the PD-1/PD-L1 axis has shown encouraging clinical activity,10,11 while histone deacetylase inhibitors, such as chidamide, are increasingly being incorporated into salvage or combination treatment regimens.12–14
Despite these therapeutic advances, treatment-related toxicities remain a significant clinical concern. L-asparaginase has been associated with thrombotic microangiopathy and proteinuric nephropathy,15,16 while immune checkpoint inhibitors may precipitate immune-mediated glomerulonephritis,17 interstitial nephritis,18 or acute kidney injury.19 Histone deacetylase inhibitors have primarily been linked to hematologic and metabolic adverse effects, with uncommon renal toxicities.20,21
Despite increasing recognition of immune checkpoint inhibitor–related nephrotoxicity, reports describing IgA nephropathy specifically induced by PD-1 inhibitors in patients with ENKTL remain limited, with crescentic or rapidly progressive forms being particularly rare. PD-1 inhibitors have been associated with immune complex–mediated glomerulonephritis, whereas pegaspargase is more commonly linked to endothelial injury and thrombotic microangiopathy, and histone deacetylase inhibitors such as chidamide are typically associated with mild tubular or interstitial injury. This distinction supports the attribution of the present case primarily to PD-1 blockade. Therefore, among the agents used in this case, PD-1 inhibition represents the most plausible cause of immune complex–mediated glomerular injury, particularly IgA nephropathy.
Case Presentation
The patient, a man in his early fifties, initially presented in December 2023 with nasal congestion and hearing loss. The patient provided written informed consent for publication of clinical details and accompanying images. His symptoms progressed in April 2024, with the development of a foreign-body sensation in the pharynx. Histopathological examination of a biopsy specimen confirmed extranodal NK/T-cell lymphoma, with an immunophenotype positive for CD56 and CD3, negative for CD20, a Ki-67 proliferation index of approximately 40%, and Epstein–Barr virus–encoded RNA positivity.
Positron emission tomography/computed tomography (PET/CT) performed in June 2024 demonstrated a hypermetabolic mass in the nasopharynx with associated cervical lymphadenopathy. The disease was staged as Ann Arbor stage IIA,22 CA stage III,23,24 with an NRI24 classification and a PINK-E score of 2.25 Baseline renal function and routine urinalysis were within normal limits prior to treatment.
On June 6, 2024, the patient initiated the first cycle of combination therapy consisting of pegaspargase (3,750 IU on day 1), tislelizumab (200 mg on day 2), chidamide (30 mg twice weekly), and dexamethasone (20 mg on days 1–4). Following an initial clinical response, the chidamide dose was reduced to 20 mg twice weekly due to the development of severe vomiting and diarrhea.
Prior to initiation of the second chemotherapy cycle on July 3, 2024, routine laboratory evaluation identified new-onset proteinuria, with a 24-hour urinary protein excretion of 3.6 g, accompanied by an elevation in serum creatinine level, suggesting immune-mediated renal toxicity. Consequently, the PD-1 inhibitor was discontinued. The patient subsequently received a second cycle of combination therapy consisting of pegaspargase (3,750 IU on day 1), chidamide (20 mg twice weekly), and dexamethasone (15 mg on days 1–5). Despite these modifications, proteinuria progressed to 6.2 g/day, with further deterioration in renal function as evidenced by rising serum creatinine levels.
A nephrology consultation was obtained, and a renal biopsy performed on July 12, 2024, demonstrated IgA nephropathy with features consistent with rapidly progressive glomerulonephritis. The patient was subsequently treated with pulse-dose methylprednisolone (500 mg/day for 3 days), followed by oral prednisolone at 60 mg/day with gradual tapering. Additionally, cyclophosphamide was administered intravenously in two doses (600 mg initially and 400 mg one week later), resulting in partial recovery of renal function.
Renal biopsy revealed diffuse proliferative and necrotizing glomerulonephritis on light microscopy, with IgA-dominant immune complex deposition on immunofluorescence and mesangial proliferative changes on electron microscopy. According to the Oxford classification (MEST-C), the findings were consistent with M1, E1, S1, T0, C1, supporting a diagnosis of IgA nephropathy with features of rapidly progressive glomerulonephritis.
By September 2024, proteinuria had decreased to approximately 5 g/day, accompanied by improvement in renal function. The patient subsequently received radiotherapy for extranodal NK/T-cell lymphoma in October 2024 using 6-MV X-ray intensity-modulated radiotherapy with image-guided radiotherapy (IMRT/IGRT). The prescribed doses were 61.6 Gy delivered to 95% of the PGTV and PGTVnd in 28 fractions of 2.2 Gy, and 50.4 Gy delivered to 95% of the PTV in 28 fractions of 1.8 Gy.
Following completion of radiotherapy, no further antitumor treatment was administered, and glucocorticoids for renal disease were gradually tapered. At the 12-month follow-up in August 2025, the patient had achieved complete remission of lymphoma with near-complete resolution of nephropathy. Laboratory evaluation performed at an outside institution on August 12, 2025, demonstrated a serum creatinine level of 119 µmol/L (reference range: 57–97 µmol/L) and a 24-hour urinary protein excretion of 50.4 mg (reference range: 28–141 mg/24 h). The patient remained on low-dose maintenance prednisone at 2.5 mg orally. The patient’s clinical course, therapeutic interventions, and renal outcomes are summarized in Figure 1.
 |
Figure 1 Timeline of clinical course and treatment. Chronological summary of symptom onset, diagnosis of extranodal NK/T-cell lymphoma, initiation of combination therapy, development of proteinuria and renal dysfunction, renal biopsy confirming IgA nephropathy with rapidly progressive features, immunosuppressive treatment, and subsequent radiotherapy with clinical remission. |
Discussion
Renal involvement has increasingly been recognized as a clinically meaningful immune-related adverse event associated with immune checkpoint inhibitors (ICIs).26 In this case, the close temporal relationship between the initiation of tislelizumab, a programmed cell death-1 (PD-1) inhibitor, and the subsequent development of heavy proteinuria, hypoalbuminemia, and rising serum creatinine strongly supports the diagnosis of ICI-related nephropathy,19 rather than direct renal toxicity from pegaspargase or chidamide.19,26,27 This attribution is further supported by the known association between PD-1 inhibitors and immune complex–mediated glomerular diseases.
Although renal abnormalities have been reported with all three agents, the overall clinical course and kidney biopsy findings—IgA nephropathy with crescent formation consistent with rapidly progressive glomerulonephritis—are most consistent with glomerular diseases previously described in association with PD-1/PD-L1 inhibition.17,27,28 A summary of previously reported cases of therapy-related nephropathy in patients with lymphoma is provided in Table 1.
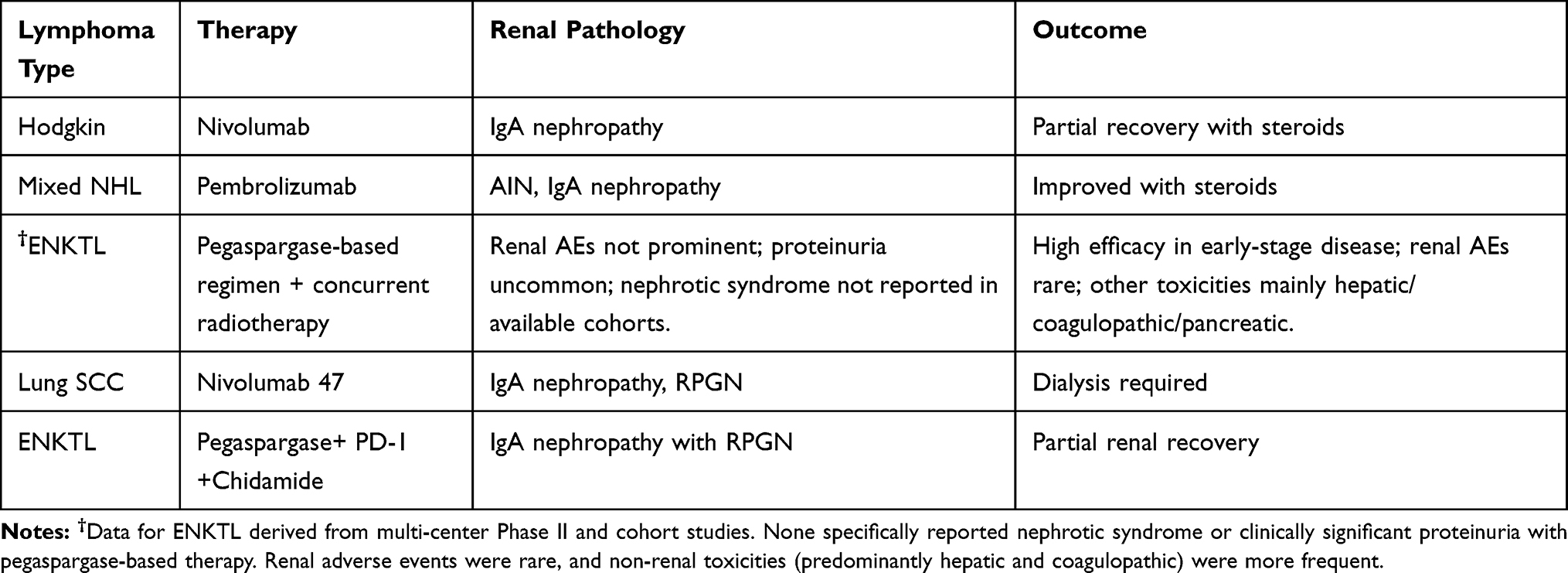 |
Table 1 Reported Cases of Drug-Induced Nephropathy in Lymphoma and Immune Checkpoint Inhibitor (ICI) Settings. Summary of Published Cases, Including Lymphoma Type, Treatment Regimen, Renal Pathology, and Clinical Outcomes |
The reported incidence of renal impairment related to immune checkpoint inhibitor therapy is approximately 2–5% in patients receiving monotherapy, rising to nearly 9–10% when combination regimens are used.19,26,29 Previous reports, including a series by Palamaris et al,30 support the association between PD-1 blockade and glomerular disease Compared with typical mild mesangial IgA nephropathy, the present case demonstrated aggressive crescentic features, suggesting a spectrum of disease severity.
The majority of renal immune-related adverse events present as acute interstitial nephritis, accounting for about 80–90% of reported cases.18,19,26 In contrast, glomerular involvement represents a smaller proportion, estimated at 10–15%, and includes entities such as membranous nephropathy, minimal change disease, lupus-like nephritis, and IgA nephropathy.17,26,31 Although nephrotic syndrome is relatively rare, with an incidence of roughly 0.4–1%, its clinical importance is substantial, as delayed recognition may result in irreversible renal damage.17,26,32
Histopathologically, ICI-associated IgA nephropathy is most commonly characterized by mesangial hypercellularity, mesangial deposition of IgA and C3 immune complexes, and the presence of occasional cellular crescents, typically corresponding to a mild-to-moderate proliferative pattern.27,33,34
As summarized in Table 2, each agent in the treatment regimen has been associated with a distinct pattern of renal involvement, including immune-mediated interstitial nephritis with PD-1 inhibitors, endothelial injury with asparaginase derivatives, and mild tubular or interstitial inflammation with histone deacetylase inhibitors, whereas dexamethasone may exert a protective anti-inflammatory effect. In the setting of combination therapy, differential diagnosis is essential. Pegaspargase is primarily associated with endothelial injury and thrombotic microangiopathy, whereas chidamide is more commonly linked to mild tubular or interstitial injury. Importantly, the temporal relationship between drug exposure and onset of renal injury, together with the absence of histopathological features typical of thrombotic microangiopathy or isolated tubular injury, argues against pegaspargase- or chidamide-induced nephrotoxicity. Collectively, these findings support PD-1 inhibitor–induced immune complex–mediated glomerulonephritis as the most plausible diagnosis in this case.
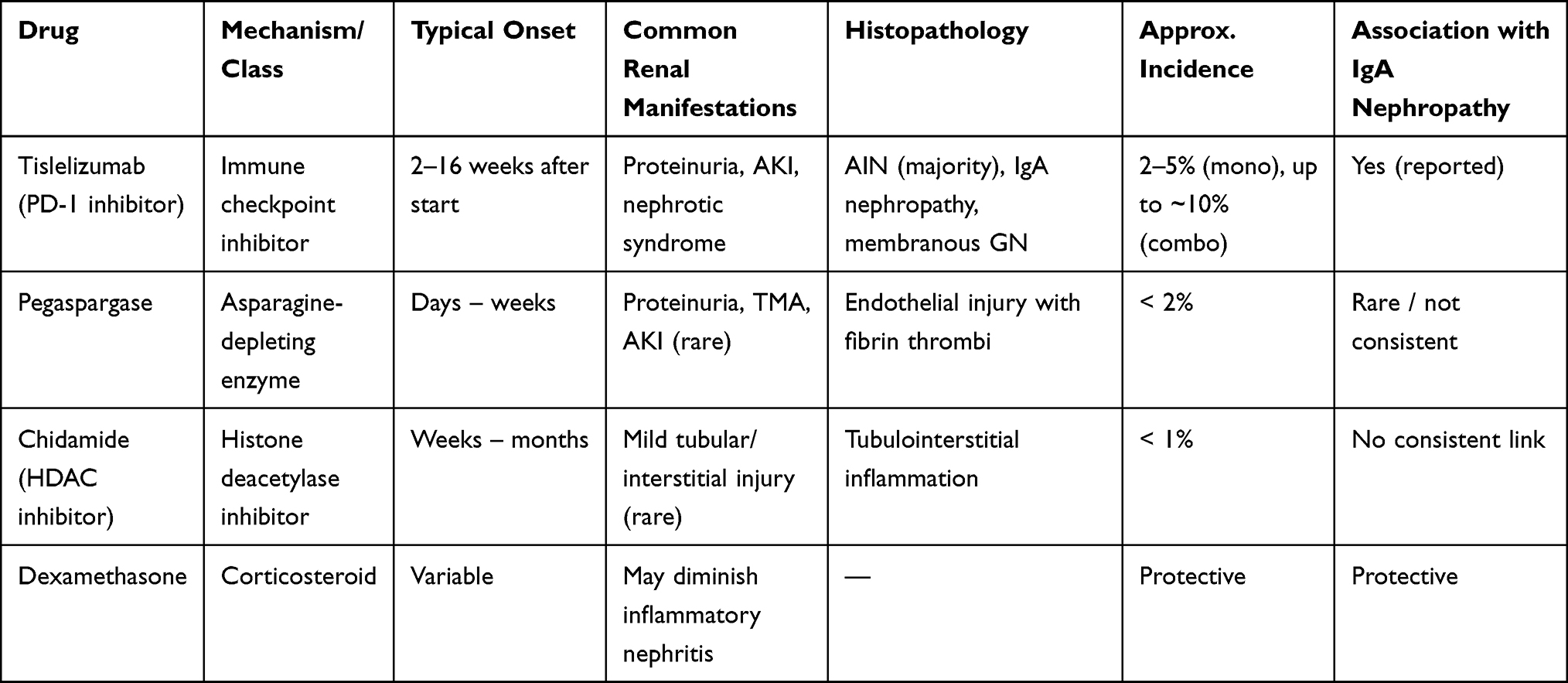 |
Table 2 Comparison of Renal Adverse Events Among the Administered Agents. Comparison of Mechanism, Onset, Clinical Manifestations, Histopathology, and Association with IgA Nephropathy for the Drugs Used in This Case |
In contrast, the present case demonstrated more aggressive pathological features, including diffuse endocapillary proliferation, segmental necrosis, and extensive crescent formation, consistent with a diffuse proliferative and necrotizing pattern of glomerulonephritis on light microscopy.
Immunofluorescence studies demonstrated dominant mesangial IgA deposition with accompanying C3 co-deposition, while electron microscopy revealed mesangial electron-dense deposits and widespread foot process effacement, findings that support an immune complex–mediated mechanism of injury.27,33 Although the histopathological features in this case overlap with those previously reported in ICI-associated IgA nephropathy, the degree of crescent formation and necrotizing change is more consistent with a rapidly progressive, RPGN-like phenotype. This observation suggests that ICI-related glomerulonephritis likely represents a pathological spectrum of IgA-dominant disease, ranging from classic mesangial proliferative patterns to severe crescentic and necrotizing forms.17,27,33 Collectively, these findings are indicative of immune dysregulation induced by checkpoint blockade, characterized by loss of immune tolerance, exaggerated effector responses, and subsequent autoantibody and immune complex formation.18,35,36 Immune checkpoint inhibition disrupts immune tolerance by enhancing T-cell activation and reducing regulatory T-cell function, thereby promoting autoimmune responses and immune complex formation.
In contrast, pegaspargase has been primarily associated with endothelial injury, proteinuria, and thrombotic microangiopathy, often in the setting of treatment-related hepatic dysfunction,15,16 whereas chidamide, a histone deacetylase (HDAC) inhibitor, is rarely linked to clinically significant nephrotoxicity beyond mild tubular or interstitial changes.20 Importantly, neither agent has been consistently associated with the development of de novo IgA nephropathy, supporting PD-1 inhibition as the most plausible driver of the glomerular pathology observed in this case.17,27,32
The management of ICI-related nephropathy primarily involves prompt discontinuation of the immune checkpoint inhibitor and initiation of high-dose corticosteroid therapy, typically prednisone or an equivalent at a dose of 1–2 mg/kg/day. With corticosteroid monotherapy, approximately 80% of affected patients experience partial or complete recovery of renal function. In cases of steroid-refractory disease, additional immunosuppressive agents such as cyclophosphamide or mycophenolate mofetil may be required.34,37,38 In the present case, the patient was treated with high-dose corticosteroids followed by cyclophosphamide, an approach commonly used in rapidly progressive glomerulonephritis. The observed partial recovery of renal function suggests a favorable response to immunosuppressive therapy, consistent with previously reported outcomes.
Rechallenge with immune checkpoint inhibitors following nephrotoxicity remains a matter of careful clinical judgment. Available evidence indicates that ICIs may be cautiously reintroduced in selected patients who have achieved complete renal recovery, with resolution of proteinuria and normalization of serum creatinine, provided that immunosuppressive therapy has been appropriately tapered and close renal monitoring is maintained.19,26,32 Nonetheless, recurrent renal injury has been reported in approximately 20–25% of rechallenged patients, underscoring the importance of individualized, multidisciplinary decision-making.19,32
This study has several limitations. First, as a single-patient case report, it does not allow for generalizable conclusions or definitive establishment of causality. Second, no detailed immunological or biomarker analyses were performed to directly investigate the underlying mechanisms of immune dysregulation. Therefore, the observed association between PD-1 inhibition and IgA nephropathy should be interpreted as suggestive rather than conclusive.
As illustrated in Figure 2, patients with extranodal NK/T-cell lymphoma receiving combination therapy should undergo structured renal surveillance, including regular urinalysis, serum creatinine assessment, and quantification of proteinuria. Early referral to nephrology and timely kidney biopsy is recommended for patients who develop proteinuria or acute kidney injury. Once IgA nephropathy, with or without features of rapidly progressive glomerulonephritis, is confirmed, prompt initiation of immunosuppressive therapy and appropriate modification of the oncologic treatment regimen are warranted.26,39
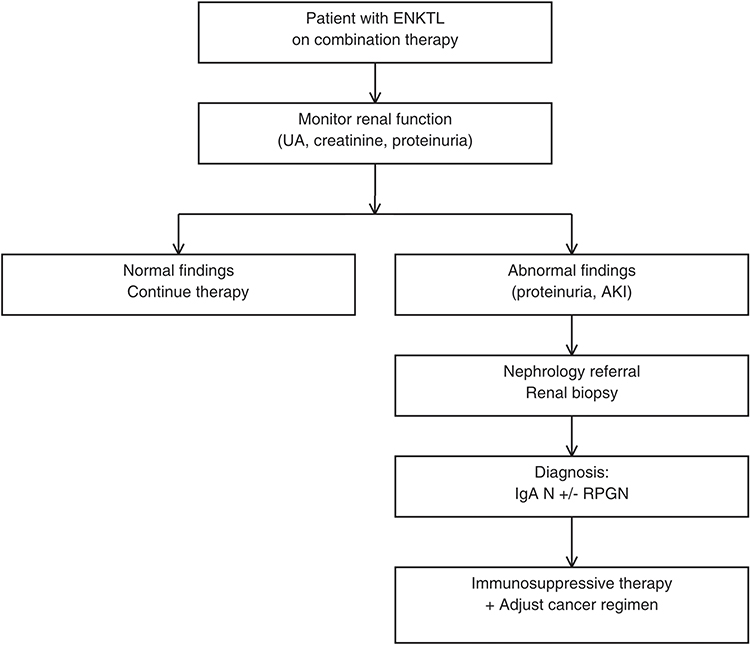 |
Figure 2 Clinical management algorithm for renal monitoring. Schematic approach to renal monitoring in patients receiving combination therapy. Abnormal findings prompt nephrology referral and renal biopsy. Confirmed IgA nephropathy is managed with discontinuation of the immune checkpoint inhibitor, immunosuppressive therapy, and adjustment of the oncologic regimen. |
Emerging biomarkers, including kidney injury molecule-1 (KIM-1) and cystatin C, may enable earlier detection of subclinical nephrotoxicity. KIM-1 serves as a marker of proximal tubular epithelial injury and may identify immune-mediated renal damage before elevations in serum creatinine become apparent.28,35 Cystatin C, a low-molecular-weight protein freely filtered by the glomeruli, provides a more sensitive assessment of changes in glomerular filtration rate compared with serum creatinine and may help differentiate true renal dysfunction from pseudo–acute kidney injury related to corticosteroid therapy or intravascular volume shifts.28,35 Collectively, these biomarkers represent promising tools for facilitating early intervention and potentially improving outcomes in ICI-associated nephropathy.
This case contributes to the limited but expanding body of evidence implicating PD-1 inhibitors, including tislelizumab, in the development of IgA nephropathy with crescentic transformation.17,27,33 It highlights the critical importance of early renal surveillance in patients treated with immune checkpoint inhibitors, particularly when administered in combination with targeted therapies. Prompt recognition of renal involvement and timely initiation of immunosuppressive treatment are essential to mitigate the risk of irreversible kidney injury and to allow continuation of effective oncologic therapy. In the present case, early intervention not only led to meaningful recovery of renal function but also enabled completion of lymphoma-directed treatment, ultimately resulting in complete remission of extranodal NK/T-cell lymphoma.10,11,40
Conclusion
Nephropathy induced by PD-1 monoclonal antibodies is an uncommon but clinically meaningful immune-related adverse event in the treatment of extranodal NK/T-cell lymphoma. This case underscores the importance of vigilant renal monitoring throughout immune checkpoint inhibitor therapy, particularly when such agents are used in combination with other potentially nephrotoxic treatments, including pegaspargase and histone deacetylase inhibitors. Routine assessment of serum creatinine, urinalysis, and proteinuria prior to each treatment cycle facilitates early recognition of renal injury. Timely multidisciplinary evaluation and appropriate immunosuppressive intervention are essential to minimize the risk of irreversible renal damage while preserving antitumor efficacy.
Ethics Statement
Written informed consent was obtained from the patient for publication of clinical details and accompanying images. Although institutional approval was not required for this case report in accordance with local regulations, the study was reviewed and approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University (Approval No. TREC2022-KY103).
Disclosure
The authors declare no competing interests in this work.
References
1. Montes-Mojarro IA, Fend F, Quintanilla-Martinez L. EBV and the pathogenesis of NK/T cell lymphoma. Cancers. 2021;13(6):1414. doi:10.3390/cancers13061414.
2. He X, Gao Y, Li Z, Huang H. Review on natural killer/T-cell lymphoma. Hematol Oncol. 2023;41(2):221–8. doi:10.1002/hon.2944.
3. Yamaguchi M, Suzuki R, Oguchi M. Advances in the treatment of extranodal NK/T-cell lymphoma, nasal type. Blood. 2018;131(23):2528–2540. doi:10.1182/blood-2017-12-791418.
4. Haverkos BM, Pan Z, Gru AA, et al. Extranodal NK/T cell lymphoma, nasal type (ENKTL-NT): an update on epidemiology, clinical presentation, and natural history in North American and European cases. Curr Hematol Malig Rep. 2016;11(6):514–527. doi:10.1007/s11899-016-0355-9
5. Bennani NN, Tun AM, Carson KR, et al. Characteristics and outcome of extranodal NK/T-cell lymphoma in North America: a retrospective multi-institutional experience. Clin Lymphoma Myeloma Leuk. 2022;22(5):e300–e309.
6. Yang H, Xun Y, Ke C, et al. Extranodal lymphoma: pathogenesis, diagnosis and treatment. Mol Biomed. 2023;4:29. doi:10.1186/s43556-023-00141-3;.
7. Borges A, Fink J, Villablanca P, et al. Midline destructive lesions of the sinonasal tract: simplified terminology based on histopathologic criteria. Am J Neuroradiol. 2000;21(2):331–336.
8. Reneau JC, Shindiapina P, Braunstein Z, et al. Extranodal natural killer/T-cell lymphomas: current approaches and future directions. J Clin Med. 2022;11(10):2699. doi:10.3390/jcm11102699
9. Huang L, Yuan B, Wu HX, et al. Comparative study of l-asparaginase-based LOP regimen over CHOP regimen before radiotherapy for stage IIE extranodal Nasal type NK/T cell lymphoma: a study of 2 centers. Clin Lymphoma Myeloma Leuk. 2017;17(3):152–158. doi:10.1016/j.clml.2016.12.003
10. Gao Y, He HX, Li XP, et al. Sintilimab (anti-PD-1 antibody) plus chidamide (histone deacetylase inhibitor) in relapsed or refractory extranodal natural killer T-cell lymphoma (SCENT): a phase Ib/II study. Signal Transduct Target Ther. 2024;9(1):121. doi:10.1038/s41392-024-01825-0
11. Du L, Zhang L, Li L, et al. Effective treatment with PD-1 antibody, chidamide, etoposide, and thalidomide (PCET) for relapsed/refractory natural killer/T-Cell lymphoma: a report of three cases. Onco Targets Ther. 2020;13:7189–7197. doi:10.2147/OTT.S262039;.
12. Liu WP, Zhao DL, Liu T, et al. A Multi-center, real-world study of chidamide for patients with relapsed or refractory peripheral T-Cell lymphomas in China. Front Oncol. 2021;11:750323. doi:10.3389/fonc.2021.750323;.
13. Wang JN, Su N, Fang Y, et al. Comparison of chemotherapy combined with chidamide versus chemotherapy in the frontline treatment for peripheral T-Cell lymphoma. Front Immunol. 2022;13:835103. doi:10.3389/fimmu.2022.835103;.
14. Shi YK, Jia B, Xu W, et al. Chidamide in relapsed or refractory peripheral T cell lymphoma: a multicenter real-world study in China. J Hematol Oncol. 2017;10(1):69. doi:10.1186/s13045-017-0439-6
15. Aldoss I, Forman SJ. How I treat adults with advanced acute lymphoblastic leukemia eligible for CD19-targeted immunotherapy. Blood. 2020;135(11):987–995. doi:10.1182/blood.2019002132.
16. Truelove E, Fielding AK, Hunt BJ. The coagulopathy and thrombotic risk associated with L-Asparaginase treatment in adults with acute lymphoblastic leukaemia. Leukemia. 2013;27(3):553–559. doi:10.1038/leu.2012.290.
17. Kitchlu A, Jhaveri KD, Wadhwani S, et al. A systematic review of immune checkpoint inhibitor–associated glomerular disease. Kidney Int Rep. 2021;6(1):66–77. doi:10.1016/j.ekir.2020.10.002
18. Herrmann SM, Perazella MA. Immune checkpoint inhibitors and immune-related adverse renal events. Kidney Int Rep. 2020;5(8):1139–1148. doi:10.1016/j.ekir.2020.04.018.
19. Cortazar FB, Kibbelaar ZA, Glezerman IG, et al. Clinical features and outcomes of immune checkpoint inhibitor–associated AKI: a multicenter study. J Am Soc Nephrol. 2020;31(2):435–446. doi:10.1681/ASN.2019070676
20. Subramanian S, Bates SE, Wright JJ, et al. Clinical toxicities of histone deacetylase inhibitors. Pharmaceuticals. 2010;3(9):2751–2767. doi:10.3390/ph3092751
21. Fraczek J, Vanhaecke T, Rogiers V. Toxicological and metabolic considerations for histone deacetylase inhibitors. Expert Opin Drug Metab Toxicol. 2013;9(4):441–457. doi:10.1517/17425255.2013.754011.
22. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–3068. doi:10.1200/JCO.2013.54.8800
23. Sun JB, Ke XY, Zhang MZ, et al. New prognostic models for extranodal natural killer T-cell lymphoma, nasal-type using Cox regression and machine learning. Transl Cancer Res. 2021;10(2):613–626. doi:10.21037/tcr-20-3017
24. Chen S-Y, Yang Y, Qi S-N, et al. Validation of nomogram-revised risk index and comparison with other models for extranodal nasal-type NK/T-cell lymphoma in the modern chemotherapy era: indication for prognostication and clinical decision-making. Leukemia. 2021;35(1):130–143. doi:10.1038/s41375-020-0791-3
25. Kim SJ, Yoon DH, Jaccard A, et al. A prognostic index for natural killer cell lymphoma after non-anthracycline-based treatment: a multicentre, retrospective analysis. Lancet Oncol. 2016;17(3):389–400. doi:10.1016/S1470-2045(15)00533-1
26. Sprangers B, Leaf DE, Porta C, et al. Diagnosis and management of immune checkpoint inhibitor-associated acute kidney injury. Nat Rev Nephrol. 2022;18(12):794–805. doi:10.1038/s41581-022-00630-8
27. He X, Liu F, Jin YY, et al. Glomerular diseases after immune checkpoint inhibitors use: what do we know so far? Ren Fail. 2022;44(1):2046–2055. doi:10.1080/0886022X.2022.2147439
28. Gupta S, Cortazar FB, Riella LV, et al. Immune checkpoint inhibitor nephrotoxicity: update 2020. Kidney360. 2020;1(2):130–140. doi:10.34067/KID.0000852019
29. Seethapathy H, Zhao S, Chute DF, et al. The incidence, causes, and risk factors of acute kidney injury in patients receiving immune checkpoint inhibitors. Clin J Am Soc Nephrol. 2019;14(12):1692–1700. doi:10.2215/CJN.00990119
30. Palamaris K, Alexandris D, Stylianou K, et al. Immune checkpoint inhibitors’ associated renal toxicity: a series of 12 cases. J Clin Med. 2022;11(16):4786. doi:10.3390/jcm11164786
31. Miao J, Sise ME, Herrmann SM. Immune checkpoint inhibitor related nephrotoxicity: advances in clinicopathologic features, noninvasive approaches, and therapeutic strategy and rechallenge. Front Nephrol. 2022;2:1017921. doi:10.3389/fneph.2022.1017921
32. Sise ME, Seethapathy H, Reynolds K. Diagnosis and management of immune checkpoint inhibitor-associated renal toxicity: illustrative case and review. Oncologist. 2019;24(6):735–742. doi:10.1634/theoncologist.2018-0764.
33. Chabannes M, Lisri Z, Lang S, et al. Immune checkpoint inhibitor therapy associated with IgA nephropathy: a case report and literature review. Front Immunol. 2024;15:1393901. doi:10.3389/fimmu.2024.1393901;.
34. Tota M, Baron V, Musial K, et al. Secondary IgA nephropathy and IgA-associated nephropathy: a systematic review of case reports. J Clin Med. 2023;12(7):2726. doi:10.3390/jcm12072726
35. Franzin R, Netti GS, Spadaccino F, et al. The use of immune checkpoint inhibitors in oncology and the occurrence of AKI: where do we stand? Front Immunol. 2020;11:574271. doi:10.3389/fimmu.2020.574271;.
36. Chen RU, Lin Q, Tang HY, et al. PD-1 immunology in the kidneys: a growing relationship. Front Immunol. 2024;15:1458209. doi:10.3389/fimmu.2024.1458209;.
37. Cassol C, Satoskar A, Lozanski G, et al. Anti−PD-1 immunotherapy may induce interstitial nephritis with increased tubular epithelial expression of PD-L1. Kidney Int Rep. 2019;4(8):1152–1160. doi:10.1016/j.ekir.2019.06.001
38. Kishi S, Minato M, Saijo A, et al. IgA nephropathy after nivolumab therapy for postoperative recurrence of lung squamous cell carcinoma. Intern Med. 2018;57(9):1259–1263. doi:10.2169/internalmedicine.9814-17
39. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073–4126. doi:10.1016/S1470-2045(15)00533-1
40. Diab R, Kamran S, Adcock B, et al. Extra-nodal nasal natural killer T-cell lymphoma treated with a checkpoint inhibitor: a case report of a sustained complete response. Cureus. 2021;13(4):e14654. doi:10.7759/cureus.14654
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.