Back to Journals » International Journal of Women's Health » Volume 17
Immune Checkpoint-Related Gene Polymorphisms and High Serum Concentration of PD-L1 and CTLA4 Contribute to the Resistance to Platinum-Based Chemotherapy in Cervical Cancer
Authors Yuan H, Wang X, Liu K, Zhang J, Wang P ![]()
Received 9 October 2025
Accepted for publication 18 December 2025
Published 30 December 2025 Volume 2025:17 Pages 5719—5731
DOI https://doi.org/10.2147/IJWH.S569408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Hongqin Yuan,* Xinfeng Wang,* Kaidong Liu, Jia Zhang, Pei Wang
Department of Radiotherapy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, Shanxi, 030013, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pei Wang, Department of Radiotherapy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, # 3, Zhigong New Street, Xinghualing District, Taiyuan, Shanxi, 030013, People’s Republic of China, Email [email protected]
Purpose: This study aims to evaluate the feasibility of using immune checkpoint-related gene polymorphisms and serum levels of PD-1, PD-L1 and CTLA4 in predicting chemotherapy resistance in patients with cervical cancer.
Methods: Seven candidate SNPs in PDCD1, CD274 and CTLA4 were genotyped in 1032 cervical cancer patients (537 non-responders and 495 responders based on their responses to chemotherapy), and the serum level of PD-1, PD-L1 and CTLA4 was detected by ELISA.
Results: The frequencies of minor allele A of PDCD1- rs2227982, CD274-rs2890658 and CTLA4-rs3087243 were significantly higher in non-responders than that in responders (p ≤ 0.0001). Moreover, the genotype AA of the three SNPs was associated with a 2.24, 3.78 and 2.71-fold increase in susceptibility to platinum resistance, respectively (p ≤ 0.0001). In addition, all of the three SNPs were associated with the risk of cisplatin resistance in both patients with squamous cell carcinoma and adenocarcinoma under different genetic models (p < 0.05). The serum concentrations of PD-L1 and CTLA4 in the non-responder group were significantly higher than those in the responder group (p < 0.0001). Moreover, the PD-L1 and CTLA4 levels of carriers with mutant genotypes of CD274-rs2890658 and CTLA4-rs3087243 were significantly higher than those of with wild-type, and the serum levels of homozygous mutant carriers were even higher (p < 0.0001).
Conclusion: The PDCD1- rs2227982, CD274-rs2890658 and CTLA4- rs3087243 polymorphisms and high serum levels of PD-L1 and CTLA4 may predict chemotherapy resistance in cervical cancer patients.
Keywords: platinum-based chemotherapy, chemotherapy resistance, cervical cancer, PD-L1, CTLA4
Introduction
Early-stage cervical cancer usually responds well to standardized treatments such as surgery and chemoradiotherapy.1 For patients with advanced distant metastases and recurrent cervical cancer, although no standardized treatment plan exists, chemotherapy, especially platinum-based chemotherapy, has become one of the preferred approaches.2 Cisplatin was the first platinum compound approved by the FDA for cancer treatment and is currently used for various solid tumors, including cervical cancer.3 However, a significant number of patients do not achieve good therapeutic effects due to chemotherapy resistance.4 Platinum-based drugs not only cause DNA cross-linking, block the cell cycle, and induce oxidative stress and apoptosis, but also induce immunogenic cell death.5 The mechanism of cisplatin resistance involves multiple genes and molecular signaling pathways. Known factors include reduced drug uptake or increased drug efflux, intracellular drug inactivation, abnormal DNA repair, alterations in apoptotic signaling pathways, and epigenetic influences, among others.6–9 However, relatively few studies have explored cisplatin resistance from the perspectives of the tumor microenvironment and immune response.
The efficacy of cisplatin partially depends on the activation of the anti-tumor immune response.10,11 Cisplatin can kill tumor cells, triggering the release of signaling molecules that recruit and activate dendritic cells, thereby initiating the T-cell-mediated anti-tumor immune response.12 Additionally, cisplatin-induced DNA damage may generate new mutations, thereby increasing tumor cell immunogenicity and enhancing their recognition by T cells. Moreover, cisplatin can modulate the tumor microenvironment by influencing the functions of various immune cells.13 However, immune checkpoints (such as PD-1, PD-L1, CTLA-4) act as brakes on the immune system. Their abnormal high expression creates an immunosuppressive tumor microenvironment, which may counteract the immune benefits of cisplatin.14 Previous studies have found that PD-L1 gene polymorphisms may lead to poorer prognosis for lung cancer patients after chemotherapy.15 However, although the rate of resistance to platinum-based chemotherapy is relatively high in cervical cancer, few studies have examined the correlation between immune checkpoint gene variations in cervical cancer patients and chemotherapy resistance.
If specific single nucleotide polymorphisms (SNPs) associated with chemotherapy resistance in cervical cancer patients can be identified, and if serum biomarkers can distinguish individuals prone to resistance, alternative or combined therapies could be considered earlier. This would aid clinical decision-making. In this study, we focused on three immune checkpoint-related genes, PDCD1, CD274 and CTLA4, and selected several common SNPs (minor allele frequency >5%) in the East Asian population. Among these, rs10204525, rs2227981 and rs2227982 in the PDCD1 gene have been associated with the risk and prognosis of esophageal cancer,16 colorectal cancer17 and breast cancer.18 The rs2890658 and rs4143815 in the CD274 gene are related to PD-L1 expression and disease risk in non-small cell lung cancer.19,20 Additionally, rs231775 and rs3087243 in CTLA4 have been reported to be associated with cervical cancer risk.21 However, whether these SNPs are linked to chemotherapy resistance in cervical cancer patients remain unclear. Here, we genotyped these SNPs in both drug-resistant and non-drug-resistant cervical cancer patients, and measured the serum levels of PD-1, PD-L1 and CTLA4 in all participants. We further analyzed the correlations of these SNPs and serum biomarkers with platinum-based chemotherapy resistance in cervical cancer.
Materials and Methods
Subjects
This study included a total of 1032 cervical cancer patients who were treated at Shanxi Cancer Hospital between January 2018 to October 2024. All patients received first-line platinum-based chemotherapy. The specific chemotherapy regimen was 175mg/m2 paclitaxel combined with 75mg/m2 cisplatin, administered every three weeks as a cycle. For patients with metastatic/recurrent disease, this constituted first-line palliative chemotherapy (Responders continued the regimen for up to 4–6 cycles or until progression). For those with locally advanced disease, it was administered as part of a curative-intent treatment plan, either as induction chemotherapy prior to concurrent chemoradiotherapy or as adjuvant therapy following surgery. Treatment was discontinued in the event of disease progression, major toxicities, or at the discretion of the patient or physician. Tumor response was assessed by computed tomography scan every two cycles. Responses were assessed using Response Evaluation Criteria in Solid Tumors.22 The definitive classification of chemotherapy resistance was based on the platinum-free interval (PFI), with progression occurring within 6 months of the last platinum dose defining the resistant group. Based on the response to chemotherapy, the patients were divided into two groups: responder: patients with a complete or partial response to the treatment; non-responder: patients with stable or progressive disease.
Strict inclusion and exclusion criteria were applied. Inclusion criteria: (1) age ≥ 18 years; (2) histopathologically confirmed cervical cancer; (3) no prior chemotherapy or radiotherapy. Exclusion criteria: (1) concurrent radiotherapy; (2) presence of other tumors, immune-related diseases and organ dysfunction.
All participants provided informed consent, demonstrating their voluntary participation and understanding of the study’s objectives and potential implications. The study was approved by the Ethics Committee of Shanxi Province Cancer Hospital (No. 2017–033) and was conducted in accordance with the World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects.
Genotyping
Before receiving treatment, all patients had their venous blood collected. The DNA was extracted using the PureLink™ Pro 96 Kit (Invitrogen, USA), and after extraction, the DNA and excess serum were stored at −80°C for future use. After collecting a batch of samples, genotyping was performed using the Sequenom Massarray platform. This platform has the advantages of high throughput, automation and low cost. The specific operation methods can be referred to the previous studies.23,24
Detection of Serum Concentration of PD-1, PD-L1 and CTLA4
Peripheral venous blood was drawn from all patients in the morning (8:00–10:00 AM) after an overnight fast, prior to the initiation of chemotherapy. Samples were collected in serum separator tubes and processed under standardized conditions. After clotting at room temperature for 30 minutes, samples were centrifuged at 3000 rpm for 15 min at 4°C. Serum was aliquoted into cryovials within 2 hours of phlebotomy and immediately stored at −80°C until analysis. To minimize protein degradation, all samples underwent only a single freeze-thaw cycle for the purpose of enzyme-linked immunosorbent assay (ELISA).
Serum levels of PD-1, PD-L1 and CTLA4 were measured using the corresponding ELISA kit following the instructions (CSB-E13643h, CSB-E13644h and CSB-E09171h, CUSABIO, Wuhan, China). Briefly, 100 μL of the standard or sample were added into the coated assay plate for 2h incubation at 37°C. After remove the liquid, 100 μL of the diluted Biotin-antibody were added and incubated for 1h at 37°C. After three times of washing, 100 μL of the diluted HRP-avidin were added and incubated for another 1h. After washing, 90 μL of TMB substrate were added and incubated for 15 min, and 50 μL of stop solution were added. The plate reader (SynergyLX, Bio-tek, USA) set to 450nm were used to obtain the results.
Statistical Analyses
Genotype data were processed with PLINK, and ELISA data were analyzed using GraphPad Prism 8.0. Differences in categorical variables were compared by the chi-square test, while age distributions were compared with the t-test. For genotype analysis, minor allele frequency (MAF) and Hardy–Weinberg equilibrium (HWE) were calculated. Differences in genotype frequencies between groups were assessed using the chi-square test and the logistic regression, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). For the ELISA data, inter-group differences were examined with the t-test, followed by analysis of serum levels across different genotypes. Statistical significance was set at *p < 0.05.
Results
During the study period, we initially identified 3189 cervical cancer patients aged over 18 years. Among them, 1269 patients had received other anti-tumor treatments before admission blood sampling, 589 received palliative radiotherapy concurrently with platinum-based chemotherapy, 232 had other tumors, severe chronic diseases, or immune-related disorders, and 67 were excluded due to incomplete clinical data or loss to follow-up. Consequently, a total of 1032 patients were included in this study.
The patients were classified as responders or non-responders based on their responses to chemotherapy. A total of 537 patients were resistant to platinum-based chemotherapy, while 495 were sensitive. The average age, pathological type and FIGO stage, lymphatic metastasis, menopausal status, pregnancy number, oral contraceptive use, smoking and drinking status information are listed in Table 1. It can be observed that there are no significant statistical differences in the demographic characteristics distribution between the two groups of patients (p > 0.05).
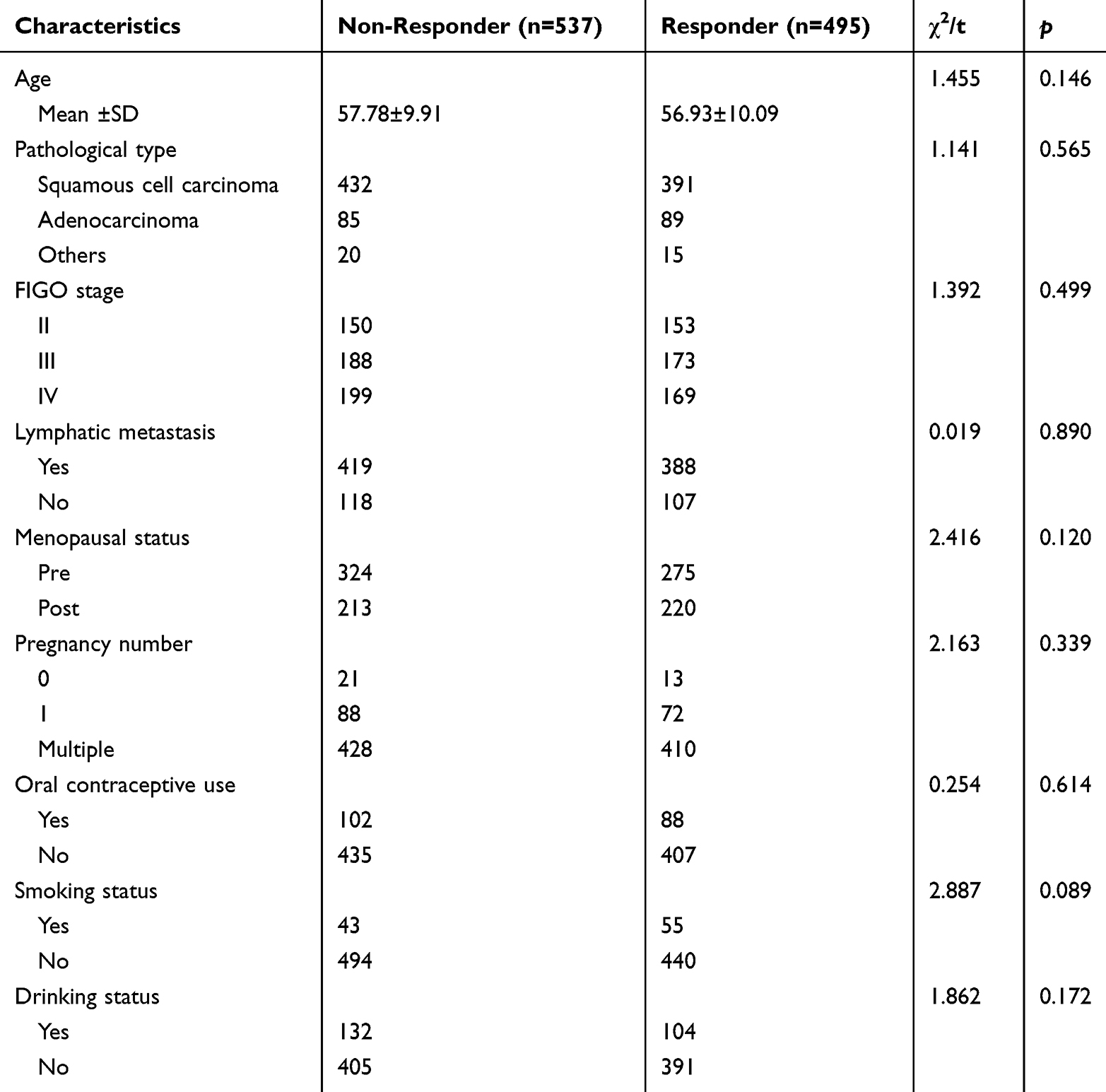 |
Table 1 The Demographic Characteristics of the Subjects |
In this study, seven SNPs on three immune checkpoint-related genes, PDCD1, CD274 and CTLA4, were selected and genotyped. The chromosomal locations, alleles, mutation types and the MAFs of these SNPs in the two groups of patients are listed in Table 2. It can be observed that the MAFs of all SNPs in the responder group is close to the data of the East Asian population in the 1000 Genomes database. All of the SNPs were consistent with HWE in non-responder and responder groups (HWE p > 0.05). After comparing the MAF of each SNP in the two groups of patients, we found that the frequencies of minor allele A of PDCD1- rs2227982, CD274-rs2890658 and CTLA4- rs3087243 were significantly higher in non-responders than that in responders, and therefore correlated with platinum-based chemotherapy resistance in cervical cancer (p rs2227982 = 0.00001, p rs2890658 = 0.0001, p rs3087243 <0.00001).
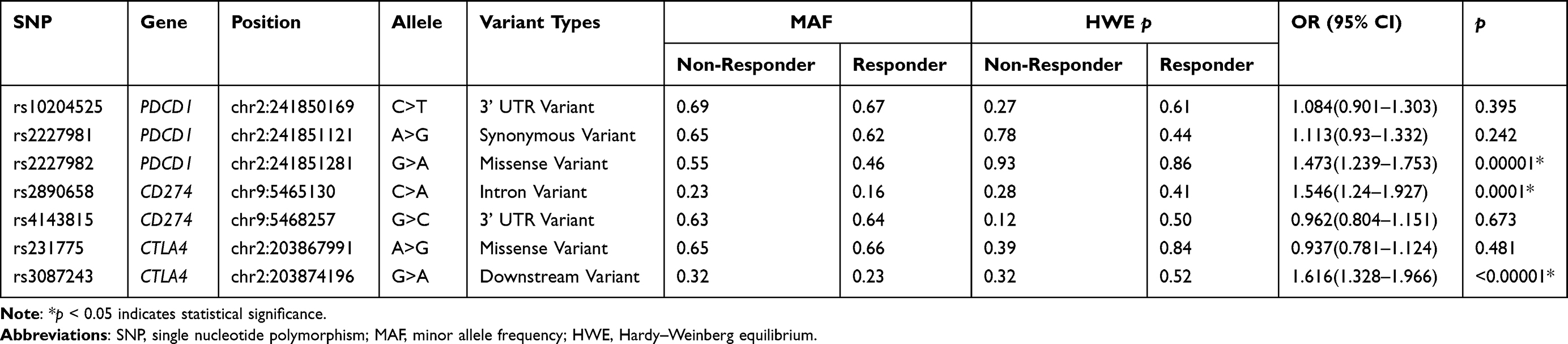 |
Table 2 Prevalence of the Minor Allele of PDCD1, CD274 and CTLA4 Between Non-Responders and Responders |
We further analyzed the genotype data of the two groups of patients, using the wild genotype of each SNP as a reference, to compare the differences in the distribution of heterozygous and homozygous mutant genotypes between the two groups (Table 3). We found that the frequencies of the PDCD1- rs2227982-GA/AA, CD274-rs2890658-CA/AA and CTLA4- rs3087243-GA/AA genotypes in the non-responder group were significantly higher than those in the responder group. Therefore, the carriers of these genotypes were more likely to develop resistance to platinum-based chemotherapy. Especially, the homozygous mutant genotype AA of the three SNPs was associated with a 2.24, 3.78 and 2.71-fold increase in platinum resistance, respectively (p rs2227982 <0.0001, p rs2890658 = 0.0001, p rs3087243 <0.0001).
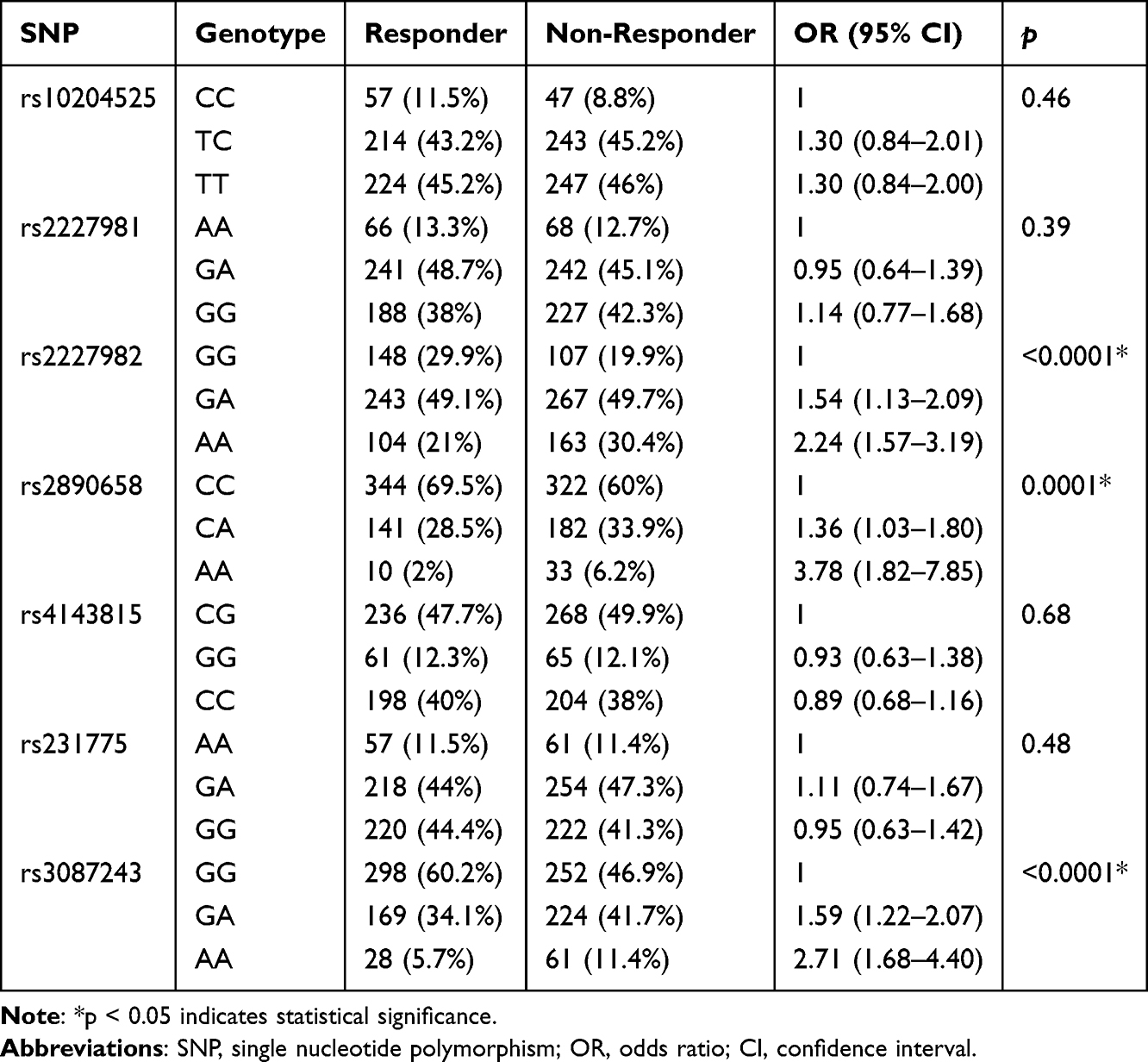 |
Table 3 Differences in the Genotype Frequencies Among Non-Responders and Responders |
Next, we conducted a logistic regression analysis to examine the correlation between each SNP and chemotherapy resistance under different genetic models (Table 4). It can be observed that the polymorphism of rs2227982 is associated with cisplatin resistance in all three genetic models (p dominant = 0.0001, p recessive = 0.0004, p log-additive <0.0001) and so are rs2890658 and rs3087243. Especially under the recessive model, the polymorphisms of rs2890658 and rs3087243 may increase the risk of cisplatin resistance by 3.45 and 2.23 times, respectively (p rs2890658 = 0.0003, p rs3087243 = 0.0005).
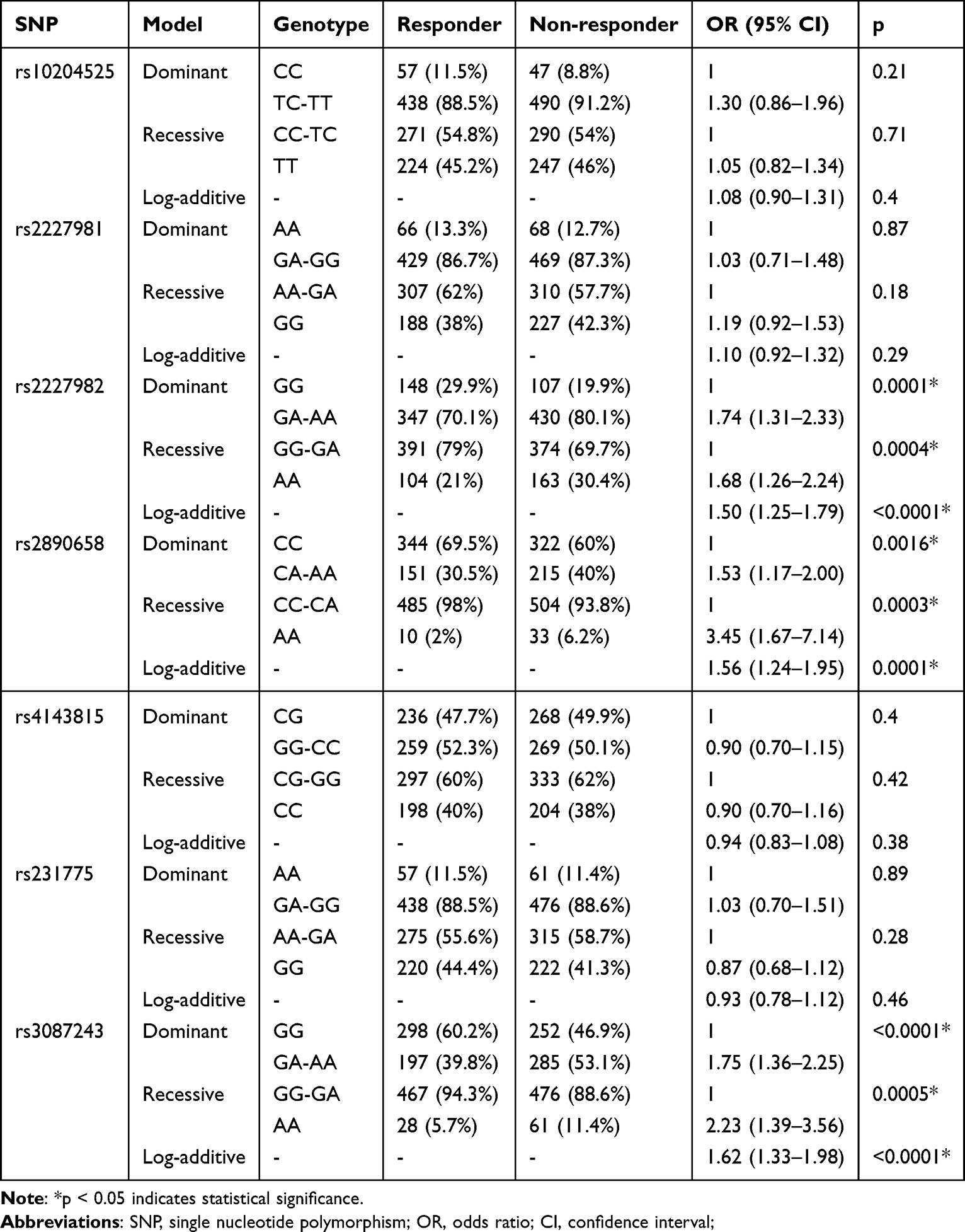 |
Table 4 The Association Between PDCD1, CD274 and CTLA4 Polymorphisms and Response to Platinum-Based Chemotherapy in Cervical Cancer |
Furthermore, considering the differences in the pathogenesis, treatment strategies and responses among various types of cervical cancer, we conducted stratified analysis of patients with squamous cell carcinoma and adenocarcinoma (Table 5). In patients with squamous cell carcinoma, polymorphisms in the three SNPs—PDCD1-rs2227982, CD274-rs2890658, and CTLA4-rs3087243—showed significant associations with chemotherapy resistance (p < 0.01) in the genotypic, dominant, recessive, and additive models, except for CD274-rs2890658 under the dominant model. In adenocarcinoma patients, PDCD1-rs2227982 was associated with chemotherapy resistance only under the dominant model (p = 0.04). CD274-rs2890658 showed significant associations in the genotypic, dominant, and additive models (p ≤ 0.001), while CTLA4-rs3087243 was significantly associated with resistance across all four genetic models (p < 0.05).
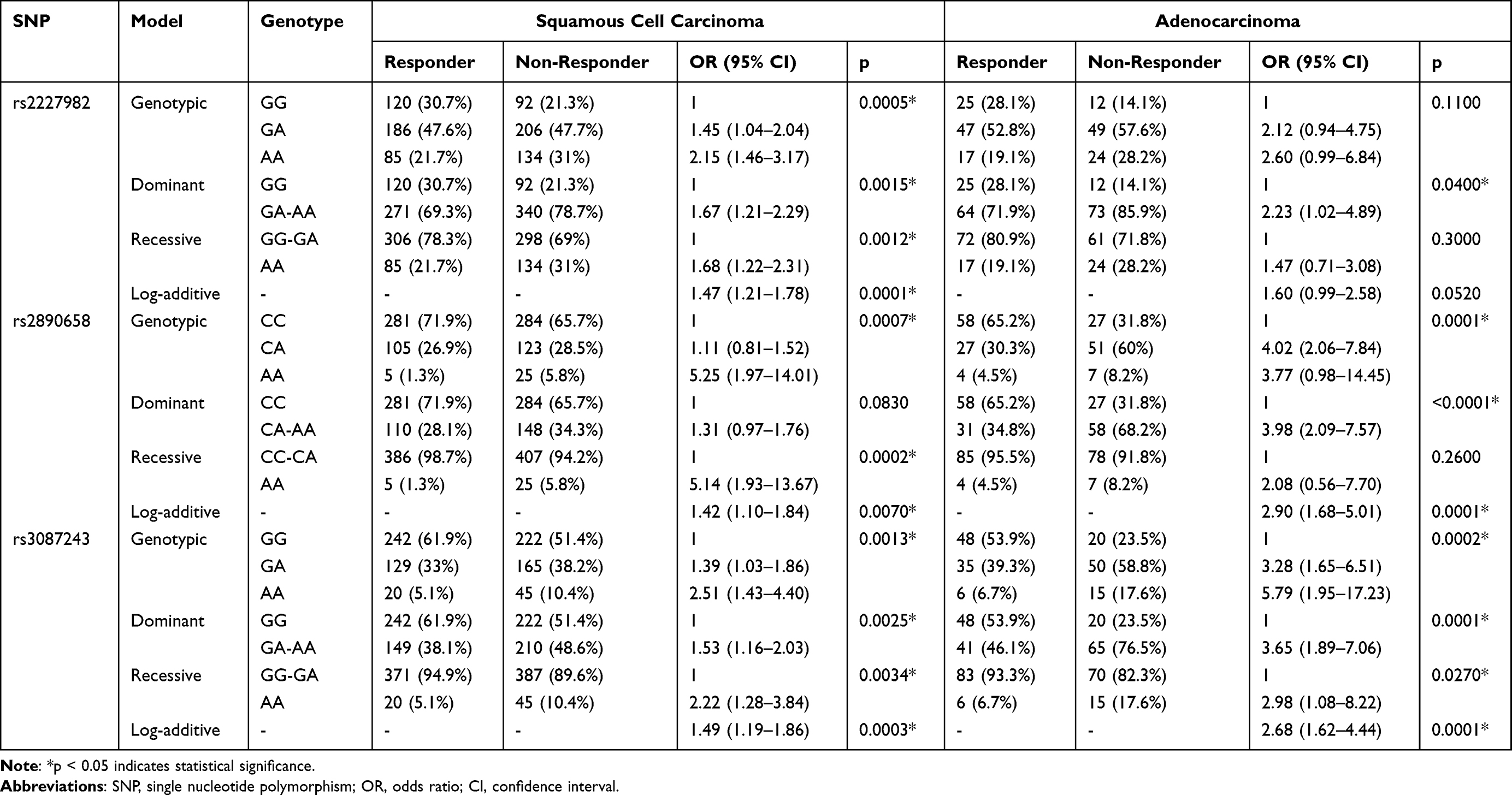 |
Table 5 The Association Between Susceptible SNPs and Resistance to Platinum-Based Chemotherapy in Squamous Cell Carcinoma and Adenocarcinoma Subgroups |
In addition, we also measured the serum levels of PD-1, PD-L1 and CTLA4 of all patients and made a comparison (Figure 1). It can be observed that there was no significant difference in the serum PD-1 levels between the two groups of patients, while the serum concentrations of PD-L1 and CTLA4 in the non-responder group were significantly higher than those in the responder group (p < 0.0001) (Figure 1A). We further compared the levels of three serum indicators in patients with different genotypes. We found that there was no significant difference in the serum PD-1 levels among carriers of different genotypes of PDCD1- rs2227982. However, compared to patients carrying the wild-type CC genotype of CD274-rs2890658, those with the CA and AA genotypes exhibited significantly higher serum PD-L1 levels (CA vs CC: p < 0.0001; AA vs CC: p < 0.0001). Notably, serum PD-L1 levels were significantly higher in patients with the AA genotype than in those with the CA genotype (p < 0.0001). Similarly, patients with the GA or AA genotypes of CTLA4-rs3087243 showed elevated serum CTLA4 levels compared to GG carriers (GA vs GG: p < 0.0001; AA vs GG: p < 0.0001), with the AA genotype showing the highest levels (AA vs GA: p < 0.0001) (Figure 1B).
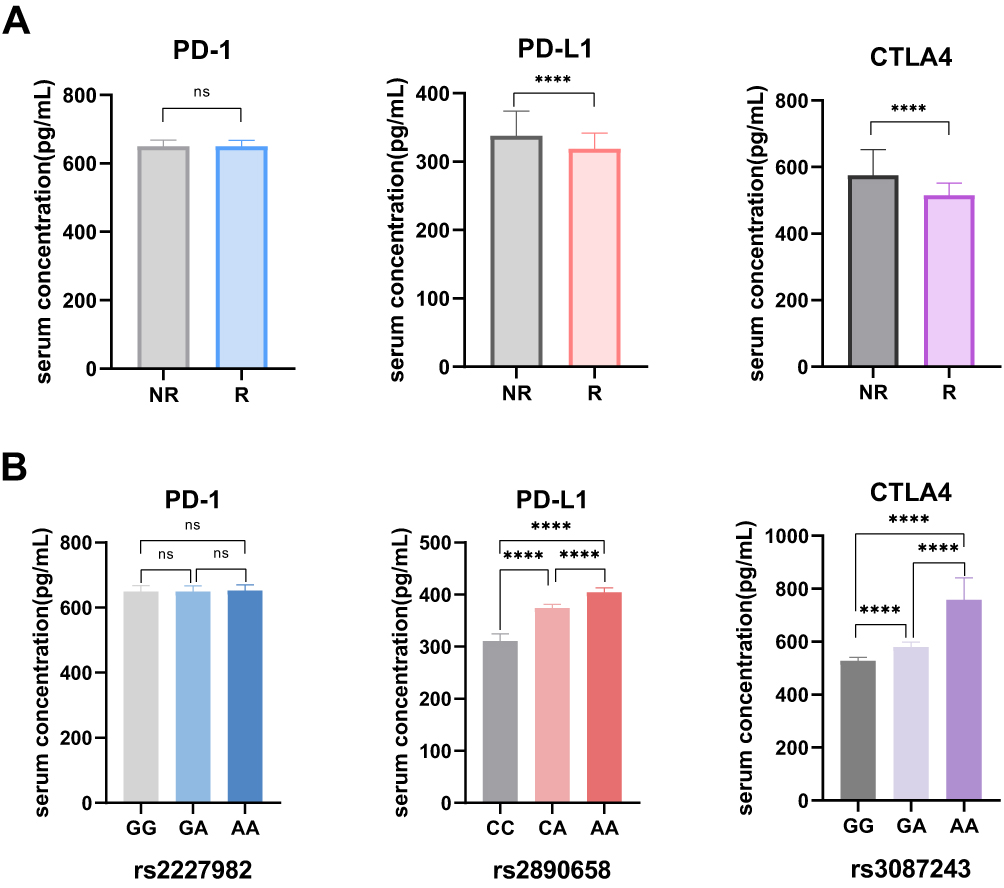 |
Figure 1 The serum concentration of PD-1, PD-L1 and CTLA among the participants. (A) No significant difference was observed in the serum concentration of PD-1 between non-responders (NR) and responders (R), while the serum level of PD-L1 and CTLA4 were significantly higher in non-responders than that in responders. (B) There is no significant differences in serum level of PD-1 among the individuals with different genotype of rs2227982, while the patients with AA genotype of rs2890658 and rs3087243 exhibited higher serum concentrations of PD-L1 and CTLA, respectively. ****p < 0.0001. Abbreviation: ns, no significance. |
Discussion
Platinum-based drugs are the main chemotherapy drugs for treating cervical cancer. However, some patients are prone to develop chemotherapy resistance, which significantly reduces the efficacy of platinum-based drugs.25 Moreover, as the chemotherapy cycles progress, patient mortality shows an upward trend. Overcoming chemotherapy resistance in solid tumors is therefore crucial for improving the treatment outcomes in cervical cancer patients.26 This study focus on polymorphism in immune checkpoint-related genes, aiming to identify patients at high risk of resistance at an early stage. This could allow for timely consideration of alternative or combination therapies, supporting more efficient clinical decision-making and potentially improving prognosis. We identified that three SNPs, PDCD1- rs2227982, CD274-rs2890658 and CTLA4- rs3087243, associated with an increased risk of cisplatin resistance in cervical cancer patients. Additionally, elevated serum level of PD-L1 and CTLA4 were also indicative of cisplatin resistance.
Acquired drug resistance in cervical cancer is closely related to the tumor microenvironment. High expression of PD-1 on T cells and PD-L1 on dendritic cells can inhibit T cell proliferation, thereby impairing immune function and promoting tumor progression.27 Some indicators have been linked to platinum-based chemotherapy drug resistance in cervical cancer tissues, including levels of CD83+ and CD4+ T cells, as well as Th17 cells.28 Th17 cells have been shown to induce cisplatin resistance in cervical cancer cells in an IL-17-dependent manner, and IL-17 is known to upregulatePD-L1 expression in various tumors.29 Xue et al noted that platinum-based chemotherapy may upregulate PD-L1 expression in tumor tissues, which is associated with poor prognosis in cervical cancer.30 Consistent with these findings, our study showed that cervical cancer patients with higher serum PD-L1 levels before receiving platinum-based chemotherapy were more likely to develop drug resistance, supporting the potential utility of these biomarkers in pretreatment risk assessment.
PD-1 and PD-L1 may also interact synergistically with other chemotherapy resistance-related signaling pathways, including the PI3K/AKT, NF-κB and JAK/STAT3 pathways. Wu et al reported that in gastric cancer, PD-1 and P-gp are highly expressed in drug-resistant cells, and PD-L1 can activate the PI3K/AKT pathway to upregulate P-gp expression, thereby enhancing drug resistance.31 Wu et al found that increased NF-κB expression was associated with chemotherapy resistance and poor prognosis in cervical cancer.32 Meanwhile, Cai et al observed that PD-L1 and IFI16 were abnormally highly expressed in HPV-positive cervical cancer. Mechanism studies revealed that IFI16 activates STING-TBK1-mediated immune regulation and the NF-κB pathway, thereby promoting PD-L1 expression.33 Furthermore, Shen et al reported that in lung cancer, activation of JAK/STAT3 could upregulate PD-L1 expression in cisplatin-resistant cells, further supporting the interaction between PD-L1 and this signaling pathway in mediating cell resistance.34 In this study, we found that polymorphisms in the genes encoding PD-1 and PD-L1, PDCD1-rs2227982 and CD274-rs2890658, were significantly associated with platinum-based chemotherapy resistance in cervical cancer patients. Rs2227982 is a missense mutation that may directly alter PD-1 expression levels, while rs2890658 is located in the intron and may influence PD-L1 levels through synergistic interactions with other factors. HaploReg database indicates that rs2890658 resides within a genomic region harboring histone activation marks (H3K4me1, H3K4me3, H3K27ac) in immune cells. We speculated that rs2890658 polymorphism may alter the binding affinity for key immune-related transcription factors, thereby modulating enhancer activity. This could, in turn, influence CD274 promoter efficiency via chromatin looping interactions in tumor or tumor-infiltrating immune cells. Future functional studies are needed to validate these mechanistic hypotheses. Although previous studies have linked these two SNPs breast cancer18 and lung cancer19 risk, respectively, this study is the first to associate them with chemotherapy resistance in cervical cancer. These results indicates that cervical cancer patients carrying genotypes linked to resistance (AA genotype of PDCD1-rs2227982, CD274-rs2890658) may warrant caution when opting for standard cisplatin-based chemotherapy, and alternative approaches could be considered.
A well-established cause of cervical cancer is persistent infection with human papillomavirus (HPV).35 Therefore, this study also examined polymorphism and serum levels of the CTLA4. CTLA4 is a key regulatory factor for T-cell homeostasis and self-tolerance and function as a negative stimulator of T-cell activation.36 Its expression is induced upon antigen engagement. By binding to the B7 ligand, CTLA4 modulates the balance of T-lymphocyte subsets. During chronic infection, high expression of CTLA4 can inhibit T-cell activation, leading to T-cell exhaustion and ultimately impairing viral control.37 Previous study have shown that the CTLA4 polymorphisms, rs231775 and rs3087243, are associated with cervical cancer risk.21 Our study is the first to investigate the correlation between these SNPs and chemotherapy resistance in cervical cancer. The results indicate that CTLA4- rs3087243 and elevated serum CTLA4 levels may contribute to chemotherapy resistance. This could be due to increased CTLA4 levels inhibiting T-cell activation and function, thereby disrupting the immune mediated cell death induced by chemotherapy and impairing the immune system’s ability to eliminate tumor cells. Therefore, for cervical cancer patients carrying the CTLA4-rs3087243-AA genotype, exploring combination therapies that include CTLA4 inhibition might be a rational direction for future research.
Notably, the subgroup analyses in this study revealed potential heterogeneity. In adenocarcinoma patients, the association between the PDCD1-rs2227982 polymorphism and platinum-based chemotherapy resistance did not reach statistical significance under the genotypic, recessive, or additive models. This result may be attributed to inherent molecular and pathological differences between adenocarcinoma and squamous cell carcinoma. For example, differences in the tumor microenvironment, driver mutation profiles, and therapeutic response mechanisms between the two subtypes may lead to divergent regulatory roles of immune checkpoint genes. Moreover, the relatively small sample size of the adenocarcinoma subgroup (85 non-responders and 89 responders) limited statistical power, potentially precluding the detection of small to moderate effect sizes. Therefore, the association of PDCD1-rs2227982 with chemotherapy resistance may be primarily relevant in squamous cell carcinoma or requires further validation in larger adenocarcinoma cohorts. Furthermore, the observation that CD274-rs2890658 exhibited model-specific associations in adenocarcinoma and squamous cell carcinoma also supports this heterogeneity. Future studies are warranted to validate the predictive role of these genetic polymorphisms in different histological subtypes of cervical cancer using larger, histology-stratified prospective cohorts.
This study has several limitations that should be acknowledged. First, as a single-center study with a relatively modest sample size, our findings may be susceptible to selection bias and may not be fully generalizable to other populations with different genetic backgrounds or clinical practices. Second, the observational nature of our design precludes the establishment of causal relationships between the identified SNPs and chemotherapy resistance; it can only demonstrate associations. Third, the SNPs we identified, particularly the non-coding CD274-rs2890658, may be in strong linkage disequilibrium with other unmeasured functional variants in the surrounding genomic region. Subsequent functional experiments are essential to validate the biological impact of specific variants and to pinpoint the true causal variants underlying the observed associations. Additionally, although we adjusted for major clinical confounders, residual confounding by unmeasured or incompletely measured factors could still influence the observed associations. Future studies should employ genome-wide or high-density SNP data to conduct principal component analysis and include the top principal components as covariates in statistical models to rigorously adjust for stratification. Furthermore, replication in independent cohorts of diverse ethnic and geographic backgrounds is essential to determine the generalizability of these genetic associations.
Conclusions
Overall, this study identified three immune checkpoint-related gene polymorphisms, PDCD1- rs2227982, CD274-rs2890658 and CTLA4- rs3087243, that are associated with platinum-based chemotherapy resistance in cervical cancer. Additionally, elevated serum levels of PD-L1 and CTLA4 were found to potentially predict chemotherapy resistance in these patients. If these findings can be further validated in larger, multicenter, studies, they could provide valuable guidance for personalized treatment decisions in clinical practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Basic Research Program of Shanxi Province (202403021222453).
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Yadav G, Srinivasan G, Jain A. Cervical cancer: novel treatment strategies offer renewed optimism. Pathol Res Pract. 2024;254:155136. doi:10.1016/j.prp.2024.155136
2. Mayadev JS, Ke G, Mahantshetty U, et al. Global challenges of radiotherapy for the treatment of locally advanced cervical cancer. Int J Gynecol Cancer. 2022;32(3):436–445. doi:10.1136/ijgc-2021-003001
3. Gentilin E. New advancements in cisplatin-based treatments. Int J Mol Sci. 2023;24(6):5920. doi:10.3390/ijms24065920
4. Bhattacharjee R, Dey T, Kumar L, et al. Cellular landscaping of cisplatin resistance in cervical cancer. Biomed Pharmacother. 2022;153:113345. doi:10.1016/j.biopha.2022.113345
5. Dasari S, Tchounwou PB. Cisplatin in cancer therapy: molecular mechanisms of action. Eur J Pharmacol. 2014;740:364–378. doi:10.1016/j.ejphar.2014.07.025
6. Liu G, Li L, Shang D, et al. BRSK1 confers cisplatin resistance in cervical cancer cells via regulation of mitochondrial respiration. J Cancer Res Clin Oncol. 2023;149(11):8803–8815. doi:10.1007/s00432-023-04821-z
7. Liu C, Zhou L, Chen J, et al. Galectin-7 promotes cisplatin efficacy by facilitating apoptosis and G3BP1 degradation in cervical cancer. Biochem Pharmacol. 2023;217:115834. doi:10.1016/j.bcp.2023.115834
8. Ma T, Guo J, Han J, et al. Circ_0001589/miR-1248/HMGB1 axis enhances EMT-mediated metastasis and cisplatin resistance in cervical cancer. Mol Carcinog. 2023;62(11):1645–1658. doi:10.1002/mc.23605
9. Ali A, Mohan J, Nadaf TAA, et al. Bioinformatics-driven discovery of signaling pathwaysand genesinfluencing cervical cancer. SN Computer Science. 2024;5(8):1–7. doi:10.1007/s42979-024-03347-6
10. Vitiello PP, Rousseau B, Chilà R, et al. Cisplatin and temozolomide combinatorial treatment triggers hypermutability and immune surveillance in experimental cancer models. Cancer Cell. 2025;43(7):1296–1312.e7. doi:10.1016/j.ccell.2025.05.014
11. Miyake M, Oda Y, Owari T, et al. Probiotics enhances anti-tumor immune response induced by gemcitabine plus cisplatin chemotherapy for urothelial cancer. Cancer Sci. 2023;114(3):1118–1130. doi:10.1111/cas.15666
12. Chen JL, Yang S-J, Pan C-K, et al. Cisplatin and albumin-based gold-cisplatin nanoparticles enhance ablative radiation therapy-induced antitumor immunity in local and distant tumor microenvironment. Int J Radiat Oncol Biol Phys. 2023;116(5):1135–1149. doi:10.1016/j.ijrobp.2023.02.014
13. Kryczka J, Kryczka J, Czarnecka-Chrebelska KH, et al. Molecular mechanisms of chemoresistance induced by cisplatin in NSCLC cancer therapy. Int J Mol Sci. 2021;22(16):8885. doi:10.3390/ijms22168885
14. Zhang H, Dai Z, Wu W, et al. Regulatory mechanisms of immune checkpoints PD-L1 and CTLA-4 in cancer. J Exp Clin Cancer Res. 2021;40(1):184. doi:10.1186/s13046-021-01987-7
15. Lee SY, Jung DK, Choi JE, et al. PD-L1 polymorphism can predict clinical outcomes of non-small cell lung cancer patients treated with first-line paclitaxel-cisplatin chemotherapy. Sci Rep. 2016;6(1):25952. doi:10.1038/srep25952
16. Zang B, Chen C, Zhao JQ. PD-1 gene rs10204525 and rs7421861 polymorphisms are associated with increased risk and clinical features of esophageal cancer in a Chinese Han population. Aging. 2020;12(4):3771–3790. doi:10.18632/aging.102845
17. Cevik M, Namal E, Iner-Koksal U, et al. Association of PD-1 and PDL-1 gene polymorphisms with colorectal cancer risk and prognosis. Mol Biol Rep. 2022;49(3):1827–1836. doi:10.1007/s11033-021-06992-9
18. Karami S, Sattarifard H, Kiumarsi M, et al. Evaluating the possible association between PD-1 (Rs11568821, Rs2227981, Rs2227982) and PD-L1 (Rs4143815, Rs2890658) polymorphisms and susceptibility to breast cancer in a sample of Southeast Iranian women. Asian Pac J Cancer Prev. 2020;21(10):3115–3123. doi:10.31557/APJCP.2020.21.10.3115
19. Wang G, Dong Y, Yang Y, et al. PD-L1 rs2890658 polymorphism increases risk for non-small-cell lung cancer in northern china population based on experimental data and meta-analysis. Contrast Media Mol Imaging. 2022;2022(1):8433489. doi:10.1155/2022/8433489
20. Ohhara Y, Tomaru U, Kinoshita I, et al. Polymorphisms of the PD-L1 gene 3′-untranslated region are associated with the expression of PD-L1 in non-small cell lung cancer. Genes Chromosomes Cancer. 2024;63(1):e23216. doi:10.1002/gcc.23216
21. Cao S, Zheng L. Impacts of CD152 polymorphisms on cervical cancer susceptibility. Pathol Res Pract. 2020;216(8):152918. doi:10.1016/j.prp.2020.152918
22. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
23. Gabriel S, Ziaugra L, Tabbaa D. SNP genotyping using the Sequenom MassARRAY iPLEX platform. Curr Protoc Hum Genet. 2009;Chapter 2:
24. Peng S, Duan Z, Zhang K, et al. Genetic polymorphisms of IFNL3 are associated with risk of immune checkpoint inhibitor-related pneumonitis in lung cancer patients. Cytokine. 2025;194:157002. doi:10.1016/j.cyto.2025.157002
25. Jin SK, Baek KH. Unraveling the role of deubiquitinating enzymes on cisplatin resistance in several cancers. Biochim Biophys Acta Rev Cancer. 2025;1880(2):189297. doi:10.1016/j.bbcan.2025.189297
26. Mukherjee A, Manna S, Singh A, et al. Investigating cisplatin resistance in squamous cervical cancer: proteomic insights into DNA repair pathways and omics-based drug repurposing. J Proteome Res. 2025;24(6):2628–2642. doi:10.1021/acs.jproteome.4c00885
27. Xu M, Cao C, Wu P, et al. Advances in cervical cancer: current insights and future directions. Cancer Commun. 2025;45(2):77–109. doi:10.1002/cac2.12629
28. Alves JJP, De Medeiros Fernandes TAA, De Araújo JMG, et al. Th17 response in patients with cervical cancer. Oncol Lett. 2018;16(5):6215–6227. doi:10.3892/ol.2018.9481
29. Theobald L, Stroeder R, Melchior P, et al. Chemoradiotherapy-induced increase in Th17 cell frequency in cervical cancer patients is associated with therapy resistance and early relapse. Mol Oncol. 2021;15(12):3559–3577. doi:10.1002/1878-0261.13095
30. Xue Y, Gao S, Gou J, et al. Platinum-based chemotherapy in combination with PD-1/PD-L1 inhibitors: preclinical and clinical studies and mechanism of action. Expert Opin Drug Deliv. 2021;18(2):187–203. doi:10.1080/17425247.2021.1825376
31. Wu L, Cai S, Deng Y, et al. PD-1/PD-L1 enhanced cisplatin resistance in gastric cancer through PI3K/AKT mediated P-gp expression. Int Immunopharmacol. 2021;94:107443. doi:10.1016/j.intimp.2021.107443
32. Wu Z, Li J, Zhang Y, et al. Synchronous co‑expression of Id‑1 and nuclear NF‑κB p65 promotes cervical cancer progression and malignancy, and is associated with a poor prognosis and chemosensitivity. Oncol Rep. 2019;42(5):2075–2086. doi:10.3892/or.2019.7301
33. Cai H, Yan L, Liu N, et al. IFI16 promotes cervical cancer progression by upregulating PD-L1 in immunomicroenvironment through STING-TBK1-NF-kB pathway. Biomed Pharmacother. 2020;123:109790. doi:10.1016/j.biopha.2019.109790
34. Shen M, Xu Z, Xu W, et al. Inhibition of ATM reverses EMT and decreases metastatic potential of cisplatin-resistant lung cancer cells through JAK/STAT3/PD-L1 pathway. J Exp Clin Cancer Res. 2019;38(1):149. doi:10.1186/s13046-019-1161-8
35. Włoszek E, Krupa K, Skrok E, et al. HPV and cervical cancer-biology, prevention, and treatment updates. Curr Oncol. 2025;32(3):122. doi:10.3390/curroncol32030122
36. Hosseini A, Gharibi T, Marofi F, et al. CTLA-4: from mechanism to autoimmune therapy. Int Immunopharmacol. 2020;80:106221. doi:10.1016/j.intimp.2020.106221
37. Van Coillie S, Wiernicki B, Xu J. Molecular and cellular functions of CTLA-4. Adv Exp Med Biol. 2020;1248:7–32.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.