Back to Journals » Patient Preference and Adherence » Volume 13
Illness Perceptions, HbA1c, And Adherence In Type 2 Diabetes In Saudi Arabia
Authors Alyami M ![]() , Serlachius A, Mokhtar I, Broadbent E
, Serlachius A, Mokhtar I, Broadbent E ![]()
Received 31 August 2019
Accepted for publication 11 October 2019
Published 25 October 2019 Volume 2019:13 Pages 1839—1850
DOI https://doi.org/10.2147/PPA.S228670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Mohsen Alyami,1 Anna Serlachius,1 Ibrahim Mokhtar,2 Elizabeth Broadbent1
1Department of Psychological Medicine, Faculty of Medical and Health Sciences, The University of Auckland, Auckland, New Zealand; 2Diabetes and Endocrine Centre, Department of Internal Medicine, King Khaled Hospital, Ministry of Health, Najran, Saudi Arabia
Correspondence: Elizabeth Broadbent
Department of Psychological Medicine, Faculty of Medical and Health Sciences, The University of Auckland, Auckland Hospital- Building 599, 2 Park Road, Grafton, Auckland 1023, New Zealand
Tel +64 9 3737599
Fax +64 9 3737013
Email [email protected]
Purpose: Little is known about predictors of adherence to diabetes medication in Saudi Arabia. This study aimed to investigate whether illness perceptions, beliefs about medicine, and God locus of health control beliefs were associated with adherence to medication and glycaemic control (HbA1c) in Saudi patients with type 2 diabetes (T2D).
Patients and methods: A convenience sample of 115 adults with T2D were recruited from a diabetes outpatient clinic. Validated self-reported measures of adherence to medication, illness perceptions, beliefs about medicine, and God locus of health control were administered. Patients’ most recent HbA1c levels were extracted from medical records. Multivariable logistic and linear regressions were used to examine the association between illness perceptions, beliefs about medicine and adherence to medication and HbA1c.
Results: More than two thirds of patients (69%) reported poor adherence to medication. All illness perceptions domains, beliefs about medicine, and God locus of health control beliefs were associated with adherence. Multivariable logistic regression revealed that older age (OR= 3.76, p= 0.023), worse consequences perceptions (OR= 0.21, p= 0.011), worse illness identity (OR= 0.23, p= 0.010), and greater illness coherence (OR= 3.24, p= 0.022) were independent predictors of adherence. Two thirds of patients (67%) had suboptimal HbA1c; and perceptions of a cyclical timeline and lower insulin effectiveness were associated with higher HbA1c. In multiple linear regression, perceptions of a cyclical timeline (β= 0.19, p= 0.040) were an independent significant predictor of HbA1c.
Conclusion: In Saudi Arabia, patients’ perceptions of T2D, beliefs about medicine, and God locus of control beliefs are associated with adherence. These results inform the development of interventions based on the Common-Sense Model (CSM) to encourage improved adherence and glycaemic control among Saudi patients with T2D. Further research with larger and more diverse samples is warranted to expand the generalizability of these findings.
Keywords: type 2 diabetes, adherence, glycaemic control, illness perceptions, Saudi Arabia
Introduction
Diabetes Mellitus is a chronic condition that affects approximately 425 million people worldwide, 79% of whom live in low-and middle-income countries. This estimate is projected to increase to 629 million by 2045.1 Type 2 diabetes (T2D), the most common type of diabetes, is emerging as an epidemic in Saudi Arabia, affecting a large proportion of the population.2 There has been an 8% increase in the prevalence of diabetes over the past 10 years and currently 18.5% of the Saudi population is affected by diabetes.1
Self-management of T2D is crucial in order to minimize the risk of developing complications and improve overall health outcomes.1 Self-management behaviours include taking medications regularly, following a healthy diet, being physical active, blood glucose self-monitoring, foot care and smoking cessation, with an overall goal of achieving and maintaining balanced glycaemic control (HbA1c < 7%).1 There are serious consequences of non-adherence to diabetes medication, including suboptimal glycaemic control,3 increased mortality and hospitalization.4 Considerable evidence indicates that non-adherence to diabetes medication and other self-management behaviours among patients with T2D is common,5 with less than 50% of patients achieving glycaemic control.6 It is well recognized that non-adherence is a multifaceted problem, influenced by a wide range of factors including demographic, personal, social, religious, cultural, condition, treatment and health system related factors.7,8
Research based on the Common-Sense Model (CSM)9,10 has highlighted the role that illness perceptions play in determining health outcomes across a wide range of chronic illnesses.11,12 The CSM proposes that individuals’ mental representations of illness influence their coping behaviours. More specifically, cognitive representations of illness include perceptions about the illness’ identity, timeline, consequences, controllability, and cause, whereas emotional representations include emotions in response to the illness. According to the CSM, these representations shape and guide self-management behaviours (e.g. adherence to medication),9 which in turn affect health outcomes.
Horne and colleagues extended the CSM to integrate patients’ beliefs about treatment and showed that these beliefs affect adherence to treatment regimens.13–15 This extension of the CSM became known as the Necessity-Concerns Framework (NCF). This framework postulates that individuals undertake a cost-benefit analysis, where beliefs about the necessity of medicine are weighed against beliefs concerning potential adverse effects. Individuals who perceive medicines as necessary and have fewer concerns about adverse effects are more likely to adhere to treatment.16
Considerable evidence shows that illness perceptions are associated with adherence to diabetes medication and glycaemic control in patients with T2D. Lower perceptions of consequences, emotional distress, illness identity and higher perceptions of personal control were associated with adherence to diabetes medication in several studies.17 Furthermore, greater perceptions of personal control were associated with lower HbA1c levels, whereas higher perceptions of treatment control and illness identity were associated with higher HbA1c levels.18 A meta-analysis found that greater perceptions of consequences, illness identity, cyclical timeline, emotional distress, and concerns about diabetes were all significantly correlated with higher HbA1c levels.19 On the other hand, stronger perceptions of personal control over diabetes showed a significant correlation with lower HbA1c levels.
Beliefs about medicine have also been found to affect adherence to diabetes medication in patients with T2D, but not glycaemic control. A meta-analysis found that higher perceptions of necessity and fewer concerns about medicine-related adverse effects were associated with adherence to medicine across a number of long-term conditions including diabetes.16 However, necessity and concerns beliefs about medicine did not predict glycaemic control.20,21
Research has shown differences between ethnic groups in how people perceive diabetes, which supports the idea that illness perceptions are influenced by cultural contexts.22,23 For example, Tongan patients reported shorter and more cyclical perceptions of illness timeline, more emotional reactions to diabetes, and lower perceptions of treatment control than New Zealand Europeans, all of which were associated with non-adherence to diabetes medication in this group.22 Pacific Island patients perceived T2D to have more severe consequences, attributed more symptoms to their T2D, and reported greater emotional responses than New Zealand European and South Asian patients.23
Around the time that the Common-Sense Model was being developed, research was being conducted into multidimensional locus of health control beliefs and their influence on self-care behaviours.24,25 Locus of control beliefs include beliefs in self-control over health (internal locus), beliefs in chance health outcomes, and beliefs that powerful others can control health.24 Locus of health control beliefs have been shown to influence adherence to treatment regimens and glycaemic control in patients with diabetes.26 For example, high internal locus of health control beliefs were associated with better adherence to self-management behaviours27 and better glycaemic control in patients with diabetes.28 God Locus of Health Control (GLHC), is a particularly important construct given the dominance of religious beliefs in Saudi Arabia. GLHC refers to the extent to which individuals believe that God is in control of their health.29 Available research indicates that patients with high GLHC beliefs are less likely to adhere to their treatment regimen.30–32
Non-adherence to diabetes medication is a major concern, especially in Saudi Arabia, where the prevalence of diabetes is high and continues to increase dramatically.2 Non-adherence to diabetes medication is highly prevalent among Saudi patients, with reports of non-adherence ranging from 38% to 57%.33–36 Less than 50% of Saudi patients achieve optimal glycaemic control.37,38 It is important that research is conducted into modifiable factors associated with non-adherence so that interventions can be implemented to increase adherence to diabetes medication in this population.
Although studies have shown that illness perceptions and beliefs about medicine are associated with adherence in T2D in Western countries,16,17,39 only six studies (two studies on illness perceptions, and four studies on beliefs about medicine), have been conducted in the Middle East region using the CSM. In Libya, lower perceptions of treatment control and higher perceptions of illness identity were significant predictors of non-adherence to diabetes medication among patients with T2D.40 In Iran, longer perceptions of chronic timeline predicted adherence to diabetes medication.41 Research on beliefs about medicine and adherence has been conducted in Saudi Arabia,34 Iraq,21 and Palestine42 and findings were consistent with previous work.16 Further research is needed to explore the associations between illness perceptions, medication beliefs, and adherence in Saudi Arabia, including God locus of health control beliefs, given the dominance of religious beliefs in the region.32
It is important to study GLHC and NCF beliefs alongside illness perceptions in this population, because they expand the scope of the CSM and may provide further insights into links between patients’ beliefs and adherence. The aim of this study was to investigate whether illness perceptions, beliefs about medicine, and God locus of health control beliefs were associated with adherence to diabetes medication and glycaemic control in Saudi patients with T2D. We hypothesized that non-adherence to diabetes medication would be associated with greater consequences perceptions, lower personal and treatment control perceptions, shorter timeline perceptions, greater cyclical timeline perceptions, higher illness identity perceptions, higher concern perceptions, lower coherence perceptions, stronger emotional responses, lower beliefs about the necessity of medicine, higher concerns about medicine, and greater God locus of health control beliefs. We hypothesized that suboptimal glycaemic control would be associated with greater consequences perceptions, lower personal control perceptions, greater cyclical timeline perceptions, higher illness identity perceptions, greater concerns, stronger emotional responses, and greater God locus of health control beliefs. Perceptions of treatment control, timeline (acute/chronic), coherence, necessity and concerns beliefs about medicine were hypothesized to be unrelated to glycaemic control.
Materials And Methods
Participants And Sampling
The study sample consisted of Saudi patients with T2D attending a diabetes outpatient clinic. Participants were recruited using a convenience sampling technique. Inclusion criteria were 18 years of age or older, a confirmed diagnosis of T2D for at least one year, and taking oral medications and/or insulin. Patients who were pregnant, ill on the day of recruitment, or not taking any medications for T2D were excluded. The sample size was calculated using G*Power software.43 In the literature, associations between illness perceptions, adherence to medication, and HbA1c range between 0.60 and −0.26 respectively.23,44 Using the lower correlation (r= −0.26) with 80% power and 0.05 alpha,45 113 participants were required.
Design And Setting
A cross-sectional design was employed. This study was conducted at a diabetes outpatient clinic in Najran, Saudi Arabia. The clinic offers various services including clinician consultations, health education, medication dispensing, foot and vision screening. The clinic is also responsible for treating and monitoring patients with diabetes in inpatient units.
Measures
The questionnaire collected information regarding the patients’ age, sex, marital status, educational status, employment status, and monthly income. The questionnaire included questions related to smartphone ownership, access to Internet, use of apps to manage T2D, and patients’ preferences for a future possible intervention (online, face-to-face or group sessions). Other self-report measures were included as detailed below.
Adherence To Medication
Participants’ adherence to diabetes medications was measured using the Arabic version of Medication Adherence Report Scale (MARS-5).15,46 The MARS-5 contains five items that ask about the frequency with which participants did not adhere to their medication. The first item is concerned with forgetfulness (unintentional non-adherence), whereas, the other 4 items are concerned with changing doses, stopping doses, skipping doses, and taking less medication than instructed (intentional non-adherence). The MARS-5 is scored using a five-point Likert scale ranging from “1= always” to “5= never”. The total score ranges between 5 and 25, with higher scores indicating higher self-reported adherence. The MARS-5 was originally developed for and validated in patients with asthma, but also has been used in other long-term conditions including diabetes.44,47,48 The MARS-5 has been translated into other languages including Arabic.49 In this study, internal consistency for the MARS-5 was 0.84.
A clear cut-off point to define non-adherence has not yet been defined, with some studies using a score of ≤ 24 to indicate non-adherence,47 while other studies used a score of > 20 to indicate adherence.48 In this study, scores on the MARS-5 showed a skewed distribution, and hence were dichotomized. Consistent with previous research with Arabic-speaking populations,49 patients with a score of ≥ 24 were considered adherent in this study.
Illness Perceptions
The Arabic version of the Brief Illness Perception Questionnaire (B-IPQ) was used to assess participants’ illness perceptions.18 The B-IPQ consists of nine-items that assess cognitive and emotional perceptions of illness: consequences, timeline, (acute/chronic), personal control, treatment control, illness identity, concern, coherence, and emotional response. The first eight items are scored using a 10-point scale, with higher scores indicating stronger perceptions. The final item is an open-ended question which asks participants to list the three most likely causes of T2D. Responses to this question were categorized into 4 groups (psychosocial factors, behavioural factors, hereditary factors, and God’s will). The B-IPQ has been widely used across a number of illnesses and different ethnic groups.11 The original, as well as the Arabic version of the B-IPQ have demonstrated good psychometric properties.11,18,50
Six additional questions were added to the B-IPQ, extending the item list from 9 to 15. A single item about how patients perceive the cyclical timeline of their T2D was added (How much does your illness vary from day to day?) scored using a 10-point scale, where 0= very stable and 10= very changeable. The remaining five additional questions asked patients about their perceptions of the effectiveness of self-management behaviours (diet, exercise, weight management, oral medication and insulin treatment).17 Format and scoring of these additional questions were similar to the original B-IPQ items.
Beliefs About Medicine
Beliefs about medicine were assessed using the Arabic version of the Beliefs about Medicines Questionnaire-Specific (BMQ-Specific).46 It includes two subscales, which evaluate patients’ perceptions of the necessity of medicine in controlling their illness (Necessity-Specific) and concerns about potential adverse effects of medicine (Concerns-Specific). Each subscale consists of 5 items and is scored on a 5-point Likert scale. High scores on the Necessity-Specific subscale indicate that the patient perceives their medicine as necessary, whereas, high scores on the Concerns-Specific subscale indicate that the patient is concerned about potential adverse effects. The original, as well as the Arabic version of the BMQ have demonstrated good psychometric properties.46,49 In the current study, both subscales demonstrated good internal consistency (α=0.88 for Necessity-Specific; and α=0.77 for Concerns-Specific).
God Locus Of Health Control
The God Locus of Health Control (GLHC) is a self-report, unidimensional scale that assesses the extent to which individuals believe that God has control over their health.29 The GLHC consists of 6-items scored on a 6-point Likert scale (1= strongly disagree to 6= strongly agree). Item scores are summed to give a total score ranging between 6 and 36, with higher total scores indicating a greater belief that God has control over one’s health. The original, as well as the Arabic version of the GLHC have demonstrated adequate reliability and validity.29,31 The GLHC exhibited excellent internal consistency in the present study (α=0.97). Responses on the GLHC were positively skewed and hence scores were dichotomized into two categories (a score of 36 indicates that God is in total control and a score of ≤ 35 indicates that God is somewhat in control).
Clinical Data
Information regarding BMI, duration of diabetes, type and number of prescribed medications, number of comorbid conditions, number of diabetes-related complications, and patients’ most recent HbA1c levels were extracted from medical records. HbA1c levels of ≥ 8% indicated suboptimal glycaemic control in patients with T2D and increase the risk of diabetes-related complications and serious comorbid conditions.51
Data Collection
The first author approached and screened potential participants for eligibility at the diabetes outpatient clinic waiting areas. Patients who were eligible and provided written informed consent were asked to complete the questionnaires while waiting for their appointments. Participants who were old or unable to read the questionnaire independently were assisted by the first author. Data collection occurred between 18th of Feb and 18th of March 2019. Patients received no compensation for participation. This study was approved by the Saudi Ministry of Health, King Fahad Medical City (IRB 18-353E). Ethics approval was also ratified by the University of Auckland Human Participants Ethics Committee. This study complied with the Declaration of Helsinki.
Statistical Analysis
Kolmogorov–Smirnov and Levene’s tests were used to inspect the normality and homogeneity of variance of the data. Non-parametric tests were used when distributions did not meet parametric assumptions. Correlation analyses (Spearman’s rho and point biserial coefficients), logistic regression, chi square, and ANOVA were used to examine the relationships between variables. Logistic regression and hierarchical multiple linear regression were used to examine predictors of adherence to diabetes medication and HbA1c respectively. In all tests, statistical significance was set at p < 0.05 (two-tailed). When data were missing for one or two items, scores were imputed using the mean score, however, when data was missing for a whole scale, scores were excluded from analysis. Data analysis was conducted using the IBM SPSS Statistics version 25.52
Results
Descriptive Statistics
A total of 173 patients were approached and screened for eligibility. Forty-six patients did not meet the inclusion criteria (22 patients had type 1 diabetes; 8 patients were too ill, 6 patients had T2D for less than a year, 3 patients were pregnant, and 7 patients were not taking diabetes medication). Of the 127 patients who were eligible, 115 participants agreed to participate (91% response rate).
All participants were Muslim Saudi nationals, with a mean age of 56 years (SD 12.43). The majority of the sample were male (58%) and married (72%). Less than one third of the sample had tertiary education (24%), were employed (28%), and earned 5000 Saudi Riyal (≈ 1333 USD) or less a month (21%). The mean BMI was 30.94 (SD 5.05), with the majority of patients either overweight (32%) or obese (56%). Most patients were non-smokers (78%).
The mean time since diagnosis was 10.33 years (SD 7.60). More than half of patients (56%) were prescribed both oral medications and insulin. There were significant comorbidities, including dyslipidaemia, hypothyroidism, and hypertension. Diabetes-related complications were also common among patients, including coronary heart disease, retinopathy, and nephropathy. The mean HbA1c was 8.72% (SD 1.37), with 67% of patients exhibiting suboptimal glycaemic control (HbA1c > 8%).
Less than half of patients (47%) reported that they owned a smartphone, had frequent access to the Internet (37%), often used apps (38%), and none of the patients had used apps to help them manage their T2D. In addition, the majority of patients reported that they would prefer a face-to-face intervention (89%) delivered in Arabic language, compared to group-based (5%) and online-based intervention (7%).
Table 1 shows the mean scores for illness perceptions, beliefs about medicine, GLHC, and medication adherence. Based on the cut off point for the MARS-5, adherence to diabetes medication was suboptimal for 69% of patients.
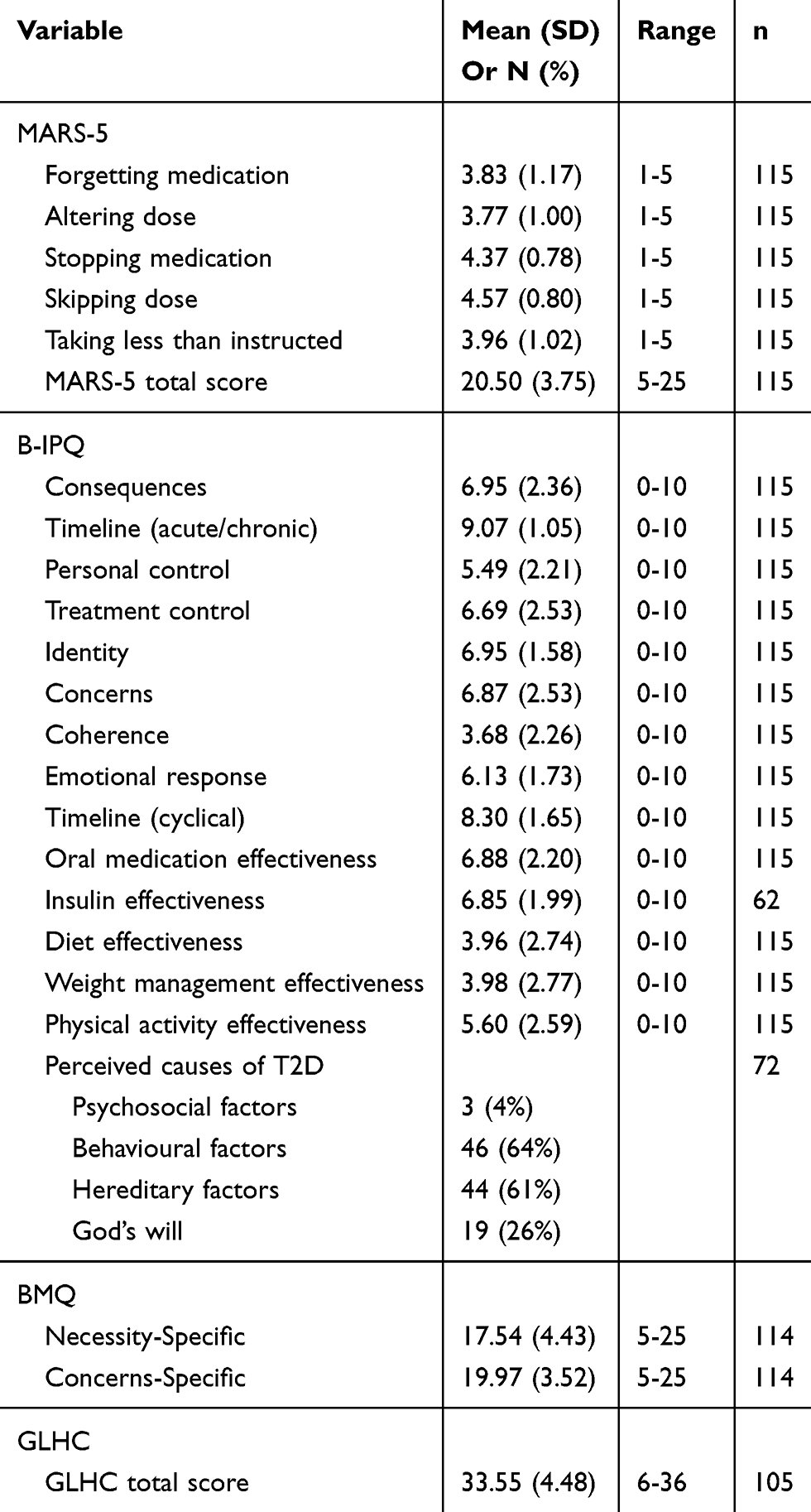 |
Table 1 Means And Standard Deviations For Study Variables |
Bivariate Relationships With Adherence To Medication And HbA1c
None of the demographical or clinical variables showed significant correlations with adherence (p > 0.05). Illness perception domains, beliefs about medicine and the belief that God is in less control were all associated with adherence to diabetes medication (see Table 2).
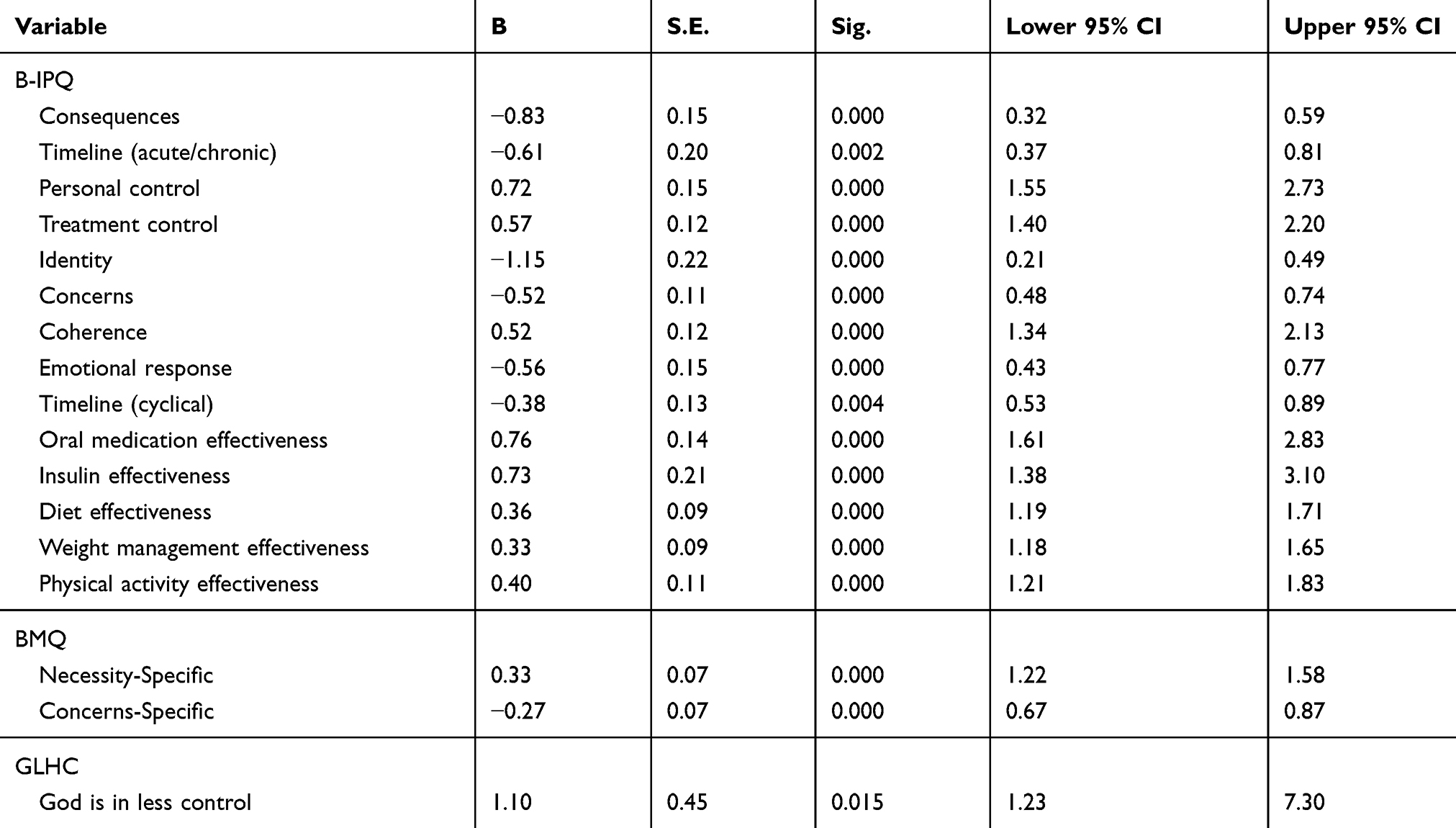 |
Table 2 Relationships Between Adherence To Medication And Study Variables Using Binary Logistic Regression |
Females exhibited higher HbA1c levels (mean 9.05%, SD 1.41) than males did (mean 8.48%, SD 1.31) (p= 0.027). The number of comorbid conditions was also associated with HbA1c F (2, 112) = 3.250, p= 0.042. Tukey HSD post-hoc analysis indicated that patients with one comorbid condition exhibited significantly higher HbA1c than patients with no comorbidities (mean difference: 0.72, p= 0.034, 95% CI: 0.04, 1.40). The differences in HbA1c between patients with one comorbid condition and those with two or more comorbid conditions (mean difference: 0.42, p= 0.425, 95% CI: −0.38, 1.21) and between patients with no comorbidities and those with two or more comorbid conditions (mean difference: −0.30, p= 0.662, 95% CI: −1.13, 0.53) were not statistically significant. HbA1c showed a positive association with perceptions of cyclical timeline (r= 0.20, p= 0.033) and negative association with perceptions of insulin effectiveness (r= −0.26, p= 0.044).
The majority of patients perceived their T2D was caused by behavioural factors (64%), followed by hereditary factors (61%), God’s will (26%), and psychosocial factors (4%). Patients in the adherent group were more likely to perceive behaviour as a cause (χ2=10.65, df= 1, p= 0.001), less likely to perceive hereditary factors as a cause (χ2=8.79, df= 1, p= 0.003), and less likely to perceive God’s will as a cause of their T2D (χ2=4.62, df= 1, p= 0.032) than those who were non-adherent. In addition, patients in the adherent group were more likely to endorse psychosocial factors as a cause of T2D than those who were non-adherent as assessed by Fisher’s exact test (χ2=5.54, df= 1, p= 0.044).
There were no statistically significant differences in HbA1c between patients who listed psychosocial factors as a cause (mean HbA1c 8.90, SD 1.47) and those who did not (mean 8.54, SD 1.36), [F (1, 70) = 0.198, p= 0.658]. There were also no significant differences in HbA1c between those who endorsed behavioural factors (mean 8.52, SD 1.34) and those who did not (mean 8.62, SD 1.41), [F (1, 70) = 0.095, p= 0.758]. Those who cited hereditary factors had similar HbA1c levels (mean 8.64, SD 1.36) to those who did not (mean 8.43, SD 1.36), [F (1, 70) = 0.384, p= 0.537). Finally, patients who endorsed God’s will had similar HbA1c levels (mean 8.63, SD 1.45) to those who did not (mean 8.53, SD 1.34), [F (1, 70) = 0.077, p= 0.782).
Predictors Of Adherence To Diabetes Medication And HbA1c
Binary logistic regression analyses revealed that all the independent variables from Table 2 remained significant predictors of adherence after controlling for demographic covariates (age, sex and education) (p < 0.05). Analysis of inter-item correlations revealed high inter-correlations between the predictors. Collinearity statistics confirmed this observation for several predictors including perceptions of personal control, cyclical timeline, oral medication effectiveness, insulin effectiveness, diet effectiveness, weight management effectiveness, physical activity effectiveness, and GLHC beliefs (VIF > 10 & tolerance statistics < 0.2). Therefore, several predictors were dropped from the regression model, while retaining the essential predictors in this study as recommended by Leech and colleagues.53
A multivariable binomial logistic regression analysis was conducted to examine associations with adherence to diabetes medication. The analysis initially adjusted for age, sex, and education (model 1) as these variables have been associated with adherence in previous studies.33,40,54 In model 2, variables that were associated with adherence to diabetes medication were added; perceptions of consequences, timeline (acute/chronic), treatment control, illness identity, coherence, emotional response, and beliefs about necessity and concerns of medicine. All the IVFs were well below 10 and tolerance statistics were all above 0.02, suggesting that there was no collinearity within the data (IVF < 1; tolerance > 0.3).
Model 1 was not significant (χ2= 1.79, df= 5, p= 0.877); model 2 was significant (χ2= 80.55, df= 8, p < 0.001). Of the predictor variables, age, perceptions of consequences, illness identity and coherence were significant individual predictors of adherence to diabetes medication (see Table 3). Greater perceptions of consequences and illness identity were associated with a reduction in the likelihood of optimal adherence to diabetes medication, whereas older age and greater perceptions of coherence were associated with an increased likelihood of optimal adherence to diabetes medication.
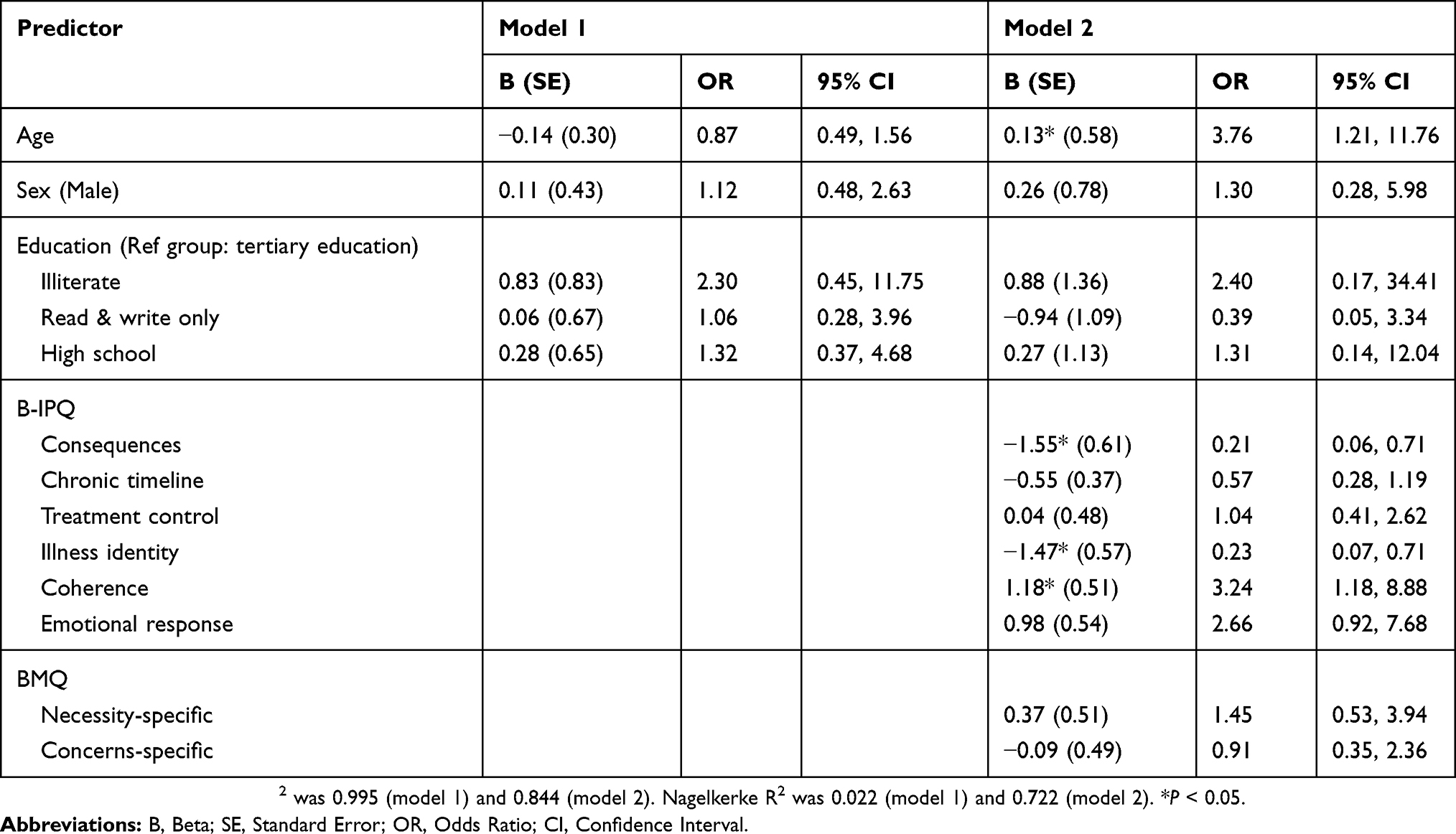 |
Table 3 Logistic Regression With Adherence To Medication As The Dependent Variable (n= 114) |
Simple linear regression analyses showed that only perception of cyclical timeline, but not perceived insulin effectiveness, was a significant independent predictor of HbA1c (β= 0.22, p= 0.016) after controlling for demographic covariates (age, sex, education). In the hierarchical multiple linear regression, the model initially adjusted for age, sex and education (Model 1) based on previous literature.37,55 Model 1 was not significant (F (5, 109) = 1.37, p= 0.242, R2 = 0.06). In Model 2, perception of cyclical timeline was added. Model 2 was significant (F (1, 108) = 4.31, p= 0.040, R2 = 0.10) explaining an additional 4% of the total variance in HbA1c (see Table 4, model 2). Perceptions of cyclical timeline independently predicted HbA1c when controlling for known covariates (β= 0.19, p= 0.040, 95% CI: 0.01, 0.52).
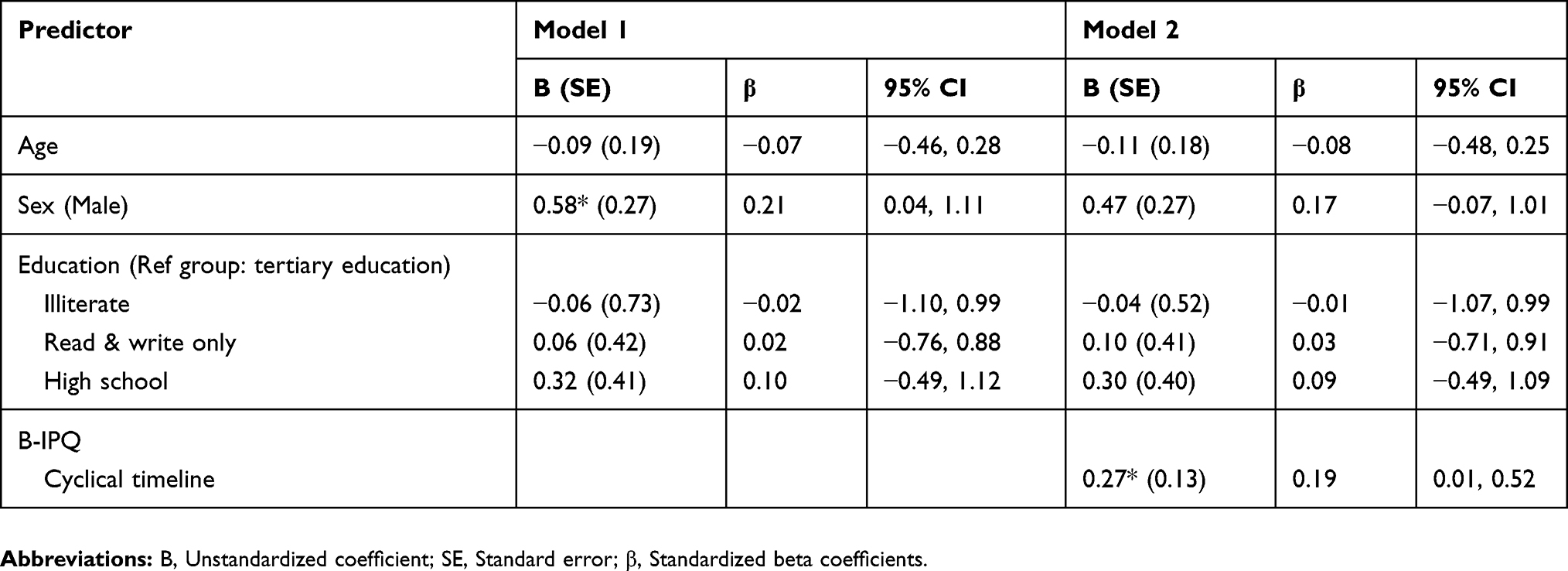 |
Table 4 Hierarchical Linear Regression With HbA1c As The Dependent Variable (n= 115) |
Discussion
This was the first study to investigate whether illness perceptions, beliefs about medicine, and God locus of health control beliefs were associated with adherence to diabetes medication and glycaemic control among Saudi patients with T2D. There were two main findings: illness perceptions, beliefs about medicine, and God locus of health control were associated with adherence to diabetes medication, and only illness perceptions (perceptions of cyclical timeline and insulin effectiveness) were associated with glycaemic control.
Approximately two thirds of patients reported non-adherence to diabetes medication and had suboptimal glycaemic control. These rates are consistent with earlier research on Saudi patients with diabetes.33,34,36,38 None of the demographic and clinical variables showed any association with adherence to diabetes medication. A recent systematic review of factors associated with medication adherence among patients with diabetes in the Middle East found mixed evidence for the associations between demographic, clinical variables and adherence to medication.54 This inconsistency in the literature may be due to methodological variations across studies in terms of study design, sample size, population under investigation, measurement tools, and statistical analyses.
All the illness perceptions showed significant bivariate relationships with adherence in the hypothesized directions, which supports previous findings.17,22,23,40 These relationships remained significant when each independent variable was examined separately controlling for the demographic covariates. Of the illness perception domains, three illness perceptions remained independent predictors of adherence in the fully adjusted model. Greater perceptions of consequences and illness identity were associated with a reduction in the likelihood of optimal adherence, whereas greater coherence was associated with an increased likelihood of optimal adherence. Consistent with our findings, earlier research has shown that greater perceptions of consequences,44 illness identity,40 and lower coherence39 were significant predictors of non-adherence to diabetes medication among patients with T2D.
There is mixed evidence for the association between perceptions of coherence and adherence. Some earlier studies failed to find a significant relationship.22,40 Coherence perceptions may be more relevant to other self-management behaviours, such as foot care among patients with diabetes.56
Behavioural and psychosocial causal beliefs were associated with adherence to medication, whereas perceiving hereditary factors and God’s will as the cause of diabetes were associated with non-adherence to medication. This finding is in line previous research showing that perceived external causes of T2D including God’s will and environmental pollution were associated with non-adherence to diabetes medication.22
Although perceptions of cyclical timeline and insulin effectiveness were associated with glycaemic control in the bivariate analysis, only perceptions of cyclical timeline were significant independent predictors of glycaemic control adjusting for the demographic covariates. Patients who perceived the course of T2D as unstable were significantly more likely to exhibit suboptimal glycaemic control, which supports previous research. In a meta-analytical review, perception of cyclical timeline was found to have the largest correlation with glycaemic control.19
Beliefs about necessity and concerns about medicine were significantly correlated with adherence. Earlier studies in the Middle East region have found similar results.34,42 In these studies, patients who perceived medication as necessary for controlling diabetes and had fewer concerns about medicine reported optimal adherence. A meta-analytical review of beliefs about medicine concluded that higher perceptions of necessity of medicine and fewer concerns about medicine were associated with optimal adherence to medicine across a number of long-term conditions including diabetes.16 In this study, beliefs about medicine did not show significant correlation with glycaemic control, which is also in line with previous research.20,21
Consistent with other research,31,32 religious beliefs were associated with how patients managed their T2D. The majority of our sample believed that God was in total control of their health and illness. This belief was associated with worse adherence to diabetes medication in the bivariate analysis. Patients who scored high on the GLHC scale were less likely to adhere to diabetes medication. This finding supports previous research with asthma patients.30 Stronger GLHC beliefs may discourage patients from taking active control in managing their illness and following their treatment regimen. No association was found between religious beliefs and HbA1c, which may be because HbA1c levels are not solely dependent on adherence. Although God-centred locus of control is indeed consistent with the Islamic faith,57 Islamic teachings at the same time encourage individuals to look after their health and wellbeing.
The results of this study provide support for the utility of considering patients’ illness perceptions, beliefs about the necessity and concerns about medication, as well as GLHC beliefs in patients with T2D in Saudi Arabia. They suggest that studies using typical measures of illness perceptions based on the CSM, may benefit by including measures of closely related concepts that lie within the model’s wider bounds. These results provide a framework to develop future interventions targeting maladaptive illness and treatment perceptions to improve adherence and glycaemic control in this population.
Strengths And Limitations
This study used valid and reliable measures, although many were self-reported. Self-reported measures of adherence tend to overestimate adherence levels.58 Patients may be inaccurate at estimating their adherence to medication over time or patients may be reluctant to admit to non-adherence because they know they are being observed or wanting to avoid disapproval from their physicians. Nevertheless, previous research has shown that self-report measures of adherence demonstrate moderate to high correlations with more objective measures such as electronic monitoring devices.59 A strength was the inclusion of analysis of causal perceptions. Previous research on illness perceptions in diabetes and other conditions has often omitted the B-IPQ item on causal beliefs.11 A limitation is the cross-sectional design meaning that causal inferences cannot be made. A second limitation is that our findings may not be generalisable to all Saudi patients with T2D given that participants were recruited from a single diabetes outpatient clinic using convenience sampling.
Future research in Saudi Arabia could also develop and test interventions to change illness perceptions to improve adherence and glycaemic control in patients with T2D, as has been shown in New Zealand60 and Ireland.61 Such interventions should be tailored to meet the patients’ needs and preferences expressed in this research, including local language and face to face sessions.
Conclusion
Amongst the study participants, illness perceptions and treatment beliefs were consistently associated with adherence to medication, but less consistently with glycaemic control. These findings expand the existing literature on the importance of patients’ perceptions of illness and treatment in relation to coping behaviours and health outcomes to the Saudi population. The study also paves the way for interventions based on the CSM to be developed in order to enhance adherence among Saudi patients with T2D. Further research with larger and more diverse samples is warranted to extend the generalisability of these results.
Abbreviations
T2D, type 2 diabetes; CSM, common sense model; NCF, necessity-concerns framework; GLHC, God locus of health control; MARS-5, medication adherence report scale; B-IPQ, brief illness perception questionnaire; BMQ, beliefs about medicines questionnaire.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank the General Directorate for Research and Studies, Saudi Ministry of Health and the Diabetes and Endocrine Centre at King Khaled Hospital for their cooperation. We would also like to thank the men and women who generously participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Robert AA, Al Dawish MA. The worrying trend of diabetes mellitus in Saudi Arabia: an urgent call to action. Curr Diabetes Rev. 2019. doi:10.2174/1573399815666190531093735
3. Capoccia K, Odegard PS, Letassy N. Medication adherence with diabetes medication: a systematic review of the literature. Diabetes Educ. 2016;42(1):34–71. doi:10.1177/0145721715619038
4. Currie CJ, Peyrot M, Morgan CL, et al. The impact of treatment noncompliance on mortality in people with type 2 diabetes. Diabetes Care. 2012;35(6):1279–1284. doi:10.2337/dc11-1277
5. Krass I, Schieback P, Dhippayom T. Adherence to diabetes medication: a systematic review. Diabet Med. 2015;32(6):725–737. doi:10.1111/dme.12651
6. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1307. doi:10.2147/PPA.S106821
7. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
8. Shahin W, Kennedy GA, Stupans I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: a systematic review. Patient Prefer Adherence. 2019;13:1019–1035. doi:10.2147/PPA.S212046
9. Leventhal H, Brissette I, Leventhal EA. The common-sense model of self-regulation of health and illness. In: Cameron LD, Leventhal H, editors. The Self-Regulation of Health and Illness Behaviour. New York: Routledge; 2003:42–65.
10. Diefenbach MA, Leventhal H. The common-sense model of illness representation: theoretical and practical considerations. J Soc Distress Homeless. 1996;5(1):11–38. doi:10.1007/BF02090456
11. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychol Health. 2015;30(11):1361–1385. doi:10.1080/08870446.2015.1070851
12. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143(11):1117–1154. doi:10.1037/bul0000118
13. Horne R. Treatment perceptions and self-regulation. In: Cameron LD, Leventhal H, editors. The Self-Regulation of Health and Illness Behaviour. London: Routledge; 2003:138–153.
14. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
15. Horne R, Weinman J. Self-regulation and self-management in asthma: exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol Health. 2002;17(1):17–32. doi:10.1080/08870440290001502
16. Horne R, Chapman SCE, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
17. Broadbent E, Donkin L, Stroh JC. Illness and treatment perceptions are associated with adherence to medications, diet, and exercise in diabetic patients. Diabetes Care. 2011;34(2):338–340. doi:10.2337/dc10-1779
18. Broadbent E, Petrie KJ, Main J, Weinman J. The Brief Illness Perception Questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
19. Mc Sharry J, Moss‐Morris R, Kendrick T. Illness perceptions and glycaemic control in diabetes: a systematic review with meta-analysis. Diabet Med. 2011;28(11):1300–1310. doi:10.1111/j.1464-5491.2011.03298.x
20. Aikens JE, Piette JD. Diabetic patients’ medication underuse, illness outcomes, and beliefs about antihyperglycemic and antihypertensive treatments. Diabetes Care. 2009;32(1):19–24. doi:10.2337/dc08-1533
21. Hussein EA, Kadhim DJ, Al-Auqbi TF. Belief about medications among type 2 diabetic patients attending the National Diabetes Center in Iraq. Iraqi J Pharm Sci. 2017;26(2):66–74.
22. Barnes L, Moss-Morris R, Kaufusi M. Illness beliefs and adherence in diabetes mellitus: a comparison between Tongan and European patients. N Z Med J. 2004;117(1188):U743.
23. Bean D, Cundy T, Petrie KJ. Ethnic differences in illness perceptions, self-efficacy and diabetes self-care. Psychol Health. 2007;22(7):787–811. doi:10.1080/14768320600976240
24. Wallston BS, Wallston KA, Kaplan GD, Maides SA. Development and validation of the health locus of control (HLC) scale. J Consult Clin Psychol. 1976;44(4):580–585. doi:10.1037/0022-006X.44.4.580
25. Lau RR. Origins of health locus of control beliefs. J Pers Soc Psychol. 1982;42(2):322–334. doi:10.1037/0022-3514.42.2.322
26. O’Hea EL, Moon S, Grothe KB, et al. The interaction of locus of control, self-efficacy, and outcome expectancy in relation to HbA1c in medically underserved individuals with type 2 diabetes. J Behav Med. 2009;32(1):106–117. doi:10.1007/s10865-008-9188-x
27. Morowatisharifabad MA, Mahmoodabad SSM, Baghianimoghadam MH, Tonekaboni NR. Relationships between locus of control and adherence to diabetes regimen in a sample of Iranians. Int J Diabetes Dev Ctries. 2010;30(1):27–32. doi:10.4103/0973-3930.60009
28. Al Nawafa’h DN, Hamdan-Mansour AM. Correlates of health locus of control among patients diagnosed with type-II diabetes mellitus. J Diabetes Mellit. 2015;05(1):190–197. doi:10.4236/jdm.2015.53023
29. Wallston KA, Malcarne VL, Flores L, et al. Does god determine your health? The god locus of health control scale. Cogn Ther Res. 1999;23(2):131–142. doi:10.1023/A:1018723010685
30. Ahmedani BK, Peterson EL, Wells KE, Rand CS, Williams LK. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol. 2013;110(2):75–79.e2. doi:10.1016/j.anai.2012.11.006
31. Albargawi M, Snethen J, Gannass AAL, Kelber S. Perception of persons with type 2 diabetes mellitus in Saudi Arabia. Int J Nurs Sci. 2016;3(1):39–44. doi:10.1016/j.ijnss.2016.02.007
32. Jeragh-Alhaddad FB, Waheedi M, Barber ND, Brock TP. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2015;9:1491–1503. doi:10.2147/PPA.S86719
33. Ahmed NO, Abugalambo S, Almethen GH. Adherence to oral hypoglycemic medication among patients with diabetes in Saudi Arabia. Int J Health Sci. 2017;11(3):45–49.
34. AlHewiti A. Adherence to long-term therapies and beliefs about medications. Int J Fam Med. 2014;2014:279596. doi:10.1155/2014/479596
35. Almaghaslah D, Abdelrhman AK, Al-Masdaf SK, et al. Factors contributing to non-adherence to insulin therapy among type 1 and type2 diabetes mellitus patients in Asser region, Saudi Arabia. Biomed Res. 2018;29(10):2090–2095. doi:10.4066/biomedicalresearch.29-18-503
36. Rasheed MK, Aljameely A, Alharbi M. Medication adherence among diabetic and hypertensive patients in Al-Qassim region of Saudi Arabia. Br J Pharm. 2016;1:100–105. doi:10.5920/bjpharm.2016.10
37. Alramadan MJ, Magliano DJ, Almigbal TH, et al. Glycaemic control for people with type 2 diabetes in Saudi Arabia – an urgent need for a review of management plan. BMC Endocr Disord. 2018;18(1):62. doi:10.1186/s12902-018-0292-9
38. Alzaheb RA, Altemani AH. The prevalence and determinants of poor glycemic control among adults with type 2 diabetes mellitus in Saudi Arabia. Diabetes Metab Syndr Obes Targets Ther. 2018;11:15–21. doi:10.2147/DMSO.S156214
39. Mann DM, Ponieman D, Leventhal H, Halm EA. Predictors of adherence to diabetes medications: the role of disease and medication beliefs. J Behav Med. 2009;32(3):278–284. doi:10.1007/s10865-009-9202-y
40. Ashur ST, Shah SA, Bosseri S, Morisky DE, Shamsuddin K. Illness perceptions of Libyans with T2DM and their influence on medication adherence: a study in a diabetes center in Tripoli. Libyan J Med. 2015;10(1):29797. doi:10.3402/ljm.v10.29797
41. Aflakseir A. Role of illness and medication perceptions on adherence to medication in a group of Iranian patients with type 2 diabetes. J Diabetes. 2012;4(3):243–247. doi:10.1111/j.1753-0407.2012.00183.x
42. Sweileh WM, Zyoud SH, Abu Nab’a RJ, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14:94–102. doi:10.1186/1471-2458-14-94
43. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
44. Owiredua C, Quarshie EN-B, Atorkey P. Living with diabetes: an exploratory study of illness representation and medication adherence in Ghana. Cogent Med. 2018;5(1):1463599. doi:10.1080/2331205X.2018.1463599
45. Cohen J. Statistical power analysis. Curr Dir Psychol Sci. 1992;1(3):98–101. doi:10.1111/1467-8721.ep10768783
46. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
47. McAdam‐Marx C, Bellows BK, Unni S, et al. Determinants of glycaemic control in a practice setting: the role of weight loss and treatment adherence (The DELTA Study). Int J Clin Pract. 2014;68(11):1309–1317. doi:10.1111/ijcp.12502
48. Wei L, Champman S, Li X, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ Open. 2017;7(10):e017293. doi:10.1136/bmjopen-2017-017293
49. Alsous M, Alhalaiqa F, Farha RA, Jalil MA, McElnay J, Horne R. Reliability and validity of Arabic translation of Medication Adherence Report Scale (MARS) and Beliefs about Medication Questionnaire (BMQ)–specific for use in children and their parents. PLoS One. 2017;12(2):e0171863. doi:10.1371/journal.pone.0171863
50. Saarti S, Jabbour H, El Osta N, Hajj A, Khabbaz LR. Cross-cultural adaptation and psychometric properties of an Arabic language version of the Brief Illness Perception Questionnaire in Lebanon. Libyan J Med. 2016;11(10):3402. doi:10.3402/ljm.v11.31976
51. American Diabetes Association. Standards of medical care in diabetes—2019 abridged for primary care providers. Clin Diabetes. 2019;37(1):11–34. doi:10.2337/cd18-0105
52. IBM Corp. IBM SPSS Statistics for Macintosh, Version 25.0. Armonk (NY): IBM Corp; 2017.
53. Leech NL, Barrett KC, Morgan GA. IBM SPSS for Intermediate Statistics: Use and Interpretation.
54. Jaam M, Ibrahim MIM, Kheir N, Awaisu A. Factors associated with medication adherence among patients with diabetes in the Middle East and North Africa region: a systematic mixed studies review. Diabetes Res Clin Pract. 2017;129:1–15. doi:10.1016/j.diabres.2017.04.015
55. Almetwazi M, Alwhaibi M, Balkhi B, et al. Factors associated with glycemic control in type 2 diabetic patients in Saudi Arabia. Saudi Pharm J. 2019;27(3):384–388. doi:10.1016/j.jsps.2018.12.007
56. Vedhara K, Dawe K, Wetherell MA, et al. Illness beliefs predict self-care behaviours in patients with diabetic foot ulcers: a prospective study. Diabetes Res Clin Pract. 2014;106(1):67–72. doi:10.1016/j.diabres.2014.07.018
57. Yosef AR. Health beliefs, practice, and priorities for health care of Arab Muslims in the United States: implications for nursing care. J Transcult Nurs. 2008;19(3):284–291. doi:10.1177/1043659608317450
58. Forbes CA, Deshpande S, Sorio-Vilela F, et al. A systematic literature review comparing methods for the measurement of patient persistence and adherence. Curr Med Res Opin. 2018:1–27. doi:10.1080/03007995.2018.1477747
59. Shi L, Liu J, Koleva Y, Fonseca V, Kalsekar A, Pawaskar M. Concordance of adherence measurement using self-reported adherence questionnaires and medication monitoring devices. Pharmaco Econ. 2010;28(12):1097–1107. doi:10.2165/11537400-000000000-00000
60. Dobson R, Whittaker R, Jiang Y, et al. Effectiveness of text message based, diabetes self management support programme (SMS4BG): two arm, parallel randomised controlled trial. BMJ. 2018;361:k1959. doi:10.1136/bmj.k1959
61. Keogh KM, Smith SM, White P, et al. Psychological family intervention for poorly controlled type 2 diabetes. Am J Manag Care. 2011;17(2):105–113.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.