Back to Journals » Patient Related Outcome Measures » Volume 11
Illness Perceptions and Quality of Life in Patients with Non-Small-Cell Lung Cancer: A 3-Month Follow-Up Pilot Study
Authors Vollmann M ![]() , Matsuda A, Kroep JR
, Matsuda A, Kroep JR ![]() , Kobayashi K, Kubota K, Inoue K
, Kobayashi K, Kubota K, Inoue K ![]() , Yamaoka K, Putter H, Ramai R, Nortier JWR
, Yamaoka K, Putter H, Ramai R, Nortier JWR ![]() , Fischer MJ
, Fischer MJ ![]() , Kaptein AA
, Kaptein AA ![]()
Received 10 November 2019
Accepted for publication 6 February 2020
Published 27 February 2020 Volume 2020:11 Pages 67—71
DOI https://doi.org/10.2147/PROM.S238009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Manja Vollmann,1 Ayako Matsuda,2 Judith R Kroep,3 Kunihiko Kobayashi,4 Kaoru Kubota,5 Kenichi Inoue,6 Kazue Yamaoka,7 Hein Putter,8 Rajen Ramai,9 Johannes WR Nortier,3 Maarten J Fischer,10 Ad A Kaptein10
1Socio-Medical Sciences ESHPM, Erasmus University Rotterdam, Rotterdam, the Netherlands; 2Department of Hygiene and Public Health, Teikyo University School of Medicine, Tokyo, Japan; 3Medical Oncology, Leiden University Medical Center, Leiden, the Netherlands; 4Saitama International Medical Center Saitama, Saitama, Japan; 5Nippon Medical School Hospital, Tokyo, Japan; 6Saitama Cancer Center, Saitama, Japan; 7Teikyo University Graduate School of Public Health, Tokyo, Japan; 8Medical Statistics and Bioinformatics, Leiden University Medical Center, Leiden, the Netherlands; 9Respiratory Medicine, Leiden University Medical Centre, Leiden, the Netherlands; 10Medical Psychology, Leiden University Medical Center, Leiden, the Netherlands
Correspondence: Ad A Kaptein
Department of Medical Psychology, Leiden University Medical Center, PO Box 9600, Leiden 2300 RC, the Netherlands
Email [email protected]
Purpose: Examine illness perceptions, functional health and quality of life of lung cancer patients throughout chemotherapy treatment.
Patients and Methods: Longitudinal design with baseline measure 12 days after the first chemotherapy and follow-up measure 3 months later, where illness perceptions (BIPQ), functional health, and quality of life (EORTC QLQ-C-30) were measured. A total of 21 patients with non-small-cell lung cancer took part. Non-parametric testing was performed given the pilot nature of the study and the associated relatively small sample size.
Results: Small to medium changes in illness perceptions and functional health between the two measurement points were detected, with both becoming more positive. More negative illness perceptions at the beginning of the treatment were associated with less functioning and lower quality of life at both beginning and end of treatment.
Conclusion: Addressing illness perceptions seems a clinically relevant approach in improving functioning and quality of life of patients with non-small-cell lung cancer.
Keywords: lung cancer, illness perceptions, quality of life, longitudinal design, patient reported outcomes
Introduction
In the past decade, a number of advances in the medical treatment and diagnosis of lung cancer have notably increased survival rates.1 Due to this development, the investigation of psychological outcomes as assessed via patient reported outcome measures in lung cancer patients becomes more and more relevant.2,3 Quite a few studies even showed that QOL is a positive predictor of survival in lung cancer patients.4–8 Therefore, understanding determinants of the psychological outcomes such as QOL is crucial in order to maximize QOL and consequently survival.
One of the most promising psychological concepts that is related to various illness outcomes in chronic patients appears to be illness perceptions (IPs). IPs are the cognitive and emotional responses of patients to their illness and its medical management.9 IPs do not necessarily reflect “medically correct facts” and differ quite substantially from accepted medical wisdom. In line with the assumptions of the common-sense model of self-regulation of health and illness,9 various empirical studies showed that IPs have an impact on illness outcomes, such as functional health and QOL, directly and indirectly via illness behavior.10–12 Therefore, addressing IPs and attempting to change them can contribute to the overall well-being of patients.
The aim of the current paper is to investigate the course of IPs and psychological outcomes, ie, functional health and QOL, in lung cancer patients over a 3-month period during chemotherapy. Moreover, the relationships between illness perceptions and psychological outcomes is examined.
Methods
The presented data are part of a larger international, bicenter study on illness perceptions and QOL in cancer patients.13 The study was conducted in line with the Helsinki Declaration. The study protocol was approved by the Medical Ethics Committee of the Leiden University Medical Center, the Netherlands (#P12-090) and written informed consent was obtained from all participants.
Procedure
Patients were recruited in the Leiden University Medical Center, the Netherlands. Patients were included if they had the diagnosis of non-small-cell lung carcinoma (NSCLC) of any stage and were undergoing first-line adjuvant or neo-adjuvant chemotherapy. Patients with EGFR or ALK mutations and patients undergoing concurrent radiotherapy and chemotherapy were excluded, in order to obtain a homogenous sample regarding clinical characteristics and type of therapy.
Data were collected at two-time points, ie, at the beginning of the treatment, approximately 12 days after the first round of chemotherapy and 1 month after the last round of chemotherapy, approximately 3 months later.
Measures
The Dutch version of Brief Illness Perception Questionnaire (Brief IPQ)14 was used to measure five cognitive illness perceptions (ie, consequences, timeline, personal control, treatment control, identity), two emotional illness perceptions (ie, concern, emotions) and illness comprehensibility with one item each (range 0–10). Higher scores indicate stronger perceptions that lung cancer affects the life, has a long duration, can be controlled by own behavior or medical treatment, involves much complaints, elicits concerns, produces negative emotions, and is understandable.
The Dutch version of the EORTC Quality of Life Questionnaire version 3.0 (EORTC QLQ-C30)15 was used to assess functional health and global QOL. Functional health was measured with 15 items that were combined into five subscales, ie, physical, role, emotional, cognitive, and social functioning. Global QOL was measured with two items. All subscales were linearly transformed (range 0 to 100), with higher scores indicating better functional health and higher QOL.
Participants
Thirty patients were included and completed the baseline measurement. Of these, nine patients did not return the follow-up questionnaires, which resulted in a final sample of 21 patients (female: n=13, 61.9%). The sample included 1 patient (4.8%) with stage IIA, 2 patients (9.5%) with stage IIB, 5 patients (23.8%) with stage IIIA, and 13 patients (61.9%) with stage IV non-small-cell lung carcinoma. Most patients (n=17, 81.0%) had no comorbidity. The mean age of the patients was 64.62 years (SD=7.70; range 53–82 years).
Data Analyses
Due to the small sample size, the data were analyzed by using nonparametric statistical tests. To explore the course of IPs, functional health, and QOL throughout chemotherapy, Wilcoxon signed-rank tests comparing scores at baseline with scores at follow-up were computed. The relationships between IPs at baseline and functional health and QOL at baseline and at follow-up were examined by means of Kendall’s tau-b correlations. Due to the small sample size and consequently suboptimal power, significance from p<0.10 is reported and the effect size was taken into account when interpreting the results.
Results
IPs, Functional Health, and QOL at Baseline and Follow-Up
Table 1 (upper part) shows some small changes in IPs between baseline and follow-up. After the chemotherapy, patients reported less perceived consequences, less personal control, less experienced symptoms, and less concern compared to the beginning of the chemotherapy. These changes seem to be discernible also on a few dimensions of functional health. Emotional and cognitive functioning improved moderately and slightly, respectively (lower part Table 1).
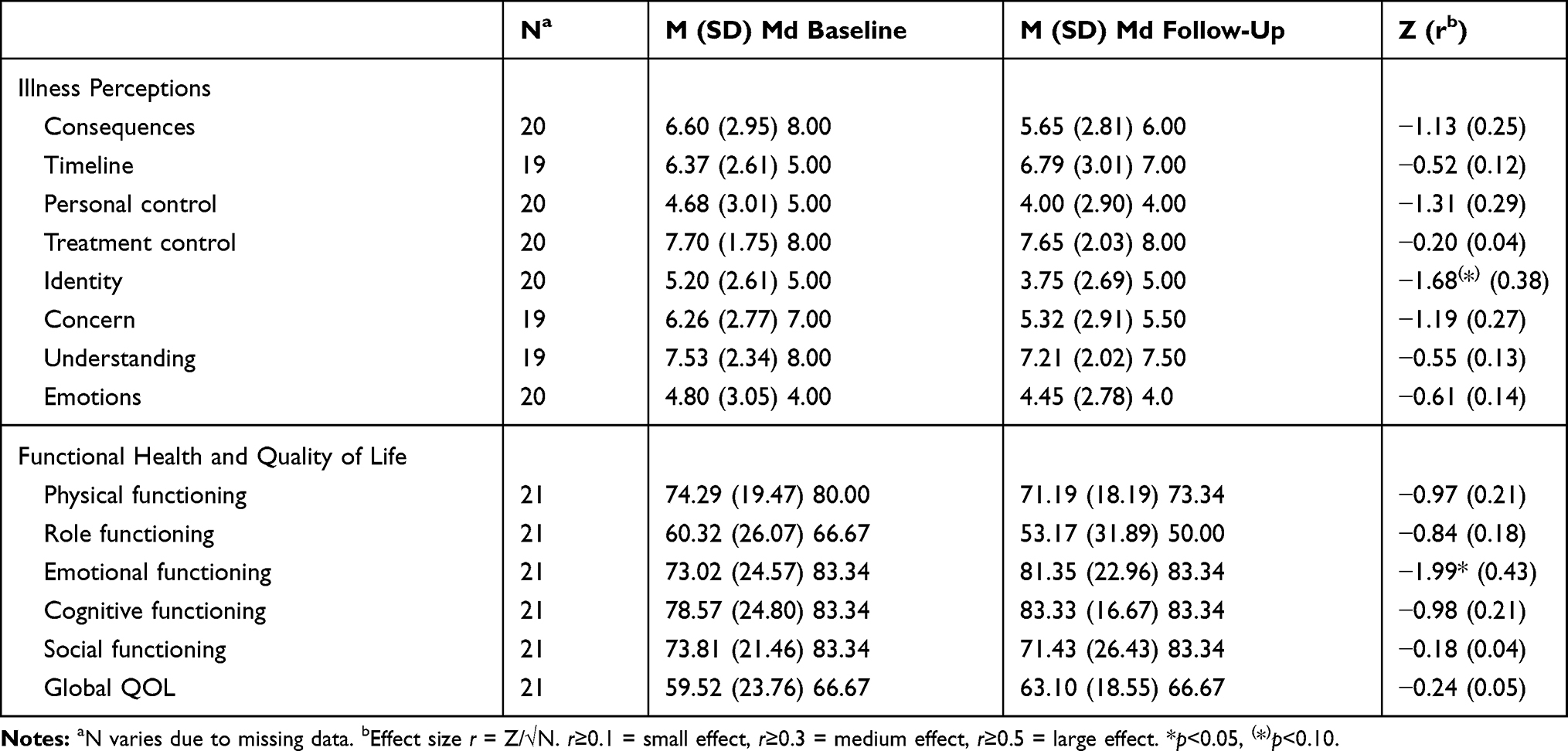 |
Table 1 Comparisons of Illness Perceptions, Functional Health, and Quality of Life at Baseline and Follow-Up (Wilcoxon Signed-Rank Test) |
Relationships Between IPs and Functional Health and QOL
Table 2 shows a large number of meaningful relationships of IPs at baseline with functional health and global QOL at baseline and follow-up. The IPs consequences, timeline, personal control, identity, concern, and understanding showed the most and the strongest correlations with various dimensions of functional health and QOL at both measurement points.
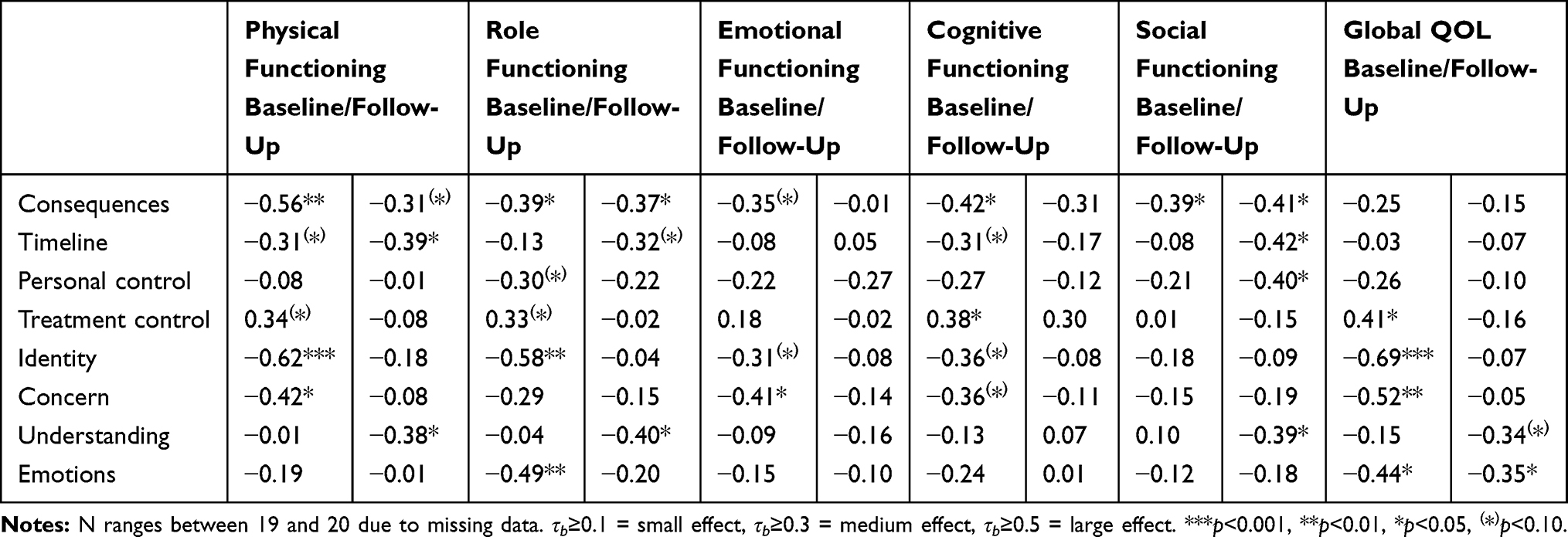 |
Table 2 Kendall’s Tau-b Correlations Between Illness Perceptions at Baseline and Functional Health and Quality of Life at Baseline and Follow-Up |
Discussion
IPs and psychological outcomes of our patients at the beginning of the chemotherapy are comparable to earlier findings in lung cancer patients.13 Previous research showed that chemotherapy negatively affects the generalized health-related quality of life.16 We expand this finding by showing that IPs become slightly more positive and aspects of functional health slightly increase after chemotherapy. Interestingly, in the present study, QOL seems not to improve after chemotherapy.
At the beginning of chemotherapy, IPs were significantly associated with various aspects of functional health and QOL. More importantly, IPs at the beginning of chemotherapy were also prospectively related to these outcome measures after chemotherapy. Specifically, the perception of more serious consequences, a longer timeline, more personal control, more negative emotions, and a better understanding of lung cancer predict lower functional health and QOL. These findings are largely in line with previous research in cancer patients,17 except from the remarkable finding that a better understanding of lung cancer has a negative effect on the outcome measures.
Conclusion and Future Directions
The number of respondents in our study must be deemed to be rather small. Patients in whom NSCLC has been diagnosed become quite ill quite soon, and they find it burdensome to fill out questionnaires, limiting empirical studies on quality of life (in a broad sense) in these patients.18–20 Despite this limitation, our findings suggest that IPs of lung cancer patients play an important role in functional health and QOL, and should therefore be taken into consideration during medical treatment. Communicating about emotions and concerns seems to be most critical.21 Purely providing patients with clinical information in order to satisfy their information needs22 without discussing psychosocial issues23 might be detrimental as our findings indicate that a better understanding of lung cancer worsens functioning and QOL in the long run. Teaching physicians to address, discuss and help adjust unhelpful illness perceptions in patients with NSCLC leads to less adjustment problems in the patients and their caregivers.24,25 Future studies with larger sample sizes should investigate whether addressing IPs in lung cancer patients impact on patient related outcome measures.
Abbreviations
ALK, anaplastic lymphocyte kinase; BIPQ, Brief Illness Perception Questionnaire; EGFR, epidermal growth factor receptor; EORTC QLQ -C30, European Organisation for the Treatment of Cancer Quality of Life Questionnaire C30; IPs, illness perceptions; NSCLC, non-small-cell lung cancer; QOL, Quality of Life.
Ethics Statement
The study complied with the Declaration of Helsinki. Ethics approval for the study was provided by the Leiden University Medical Center Medical Ethics Committee (#P12-090), and written informed consent was obtained from all participants.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Bernadette Bos, Respiratory Medicine, LUMC, for help with collecting patient data.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Professor Kunihiko Kobayashi reports personal fees from AstraZeneca, Boehringer, Pfizer, Onto Pharmaceutical company, and Chennai Pharmaceutical company, outside the submitted work. Professor Kaoru Kubota reports grants and personal fees from Boehringer Ingelheim and Ono, personal fees from Chugai MSD, AstraZeneca, Eli Lilly, Daiichi Sankyo, and Bristol Myers Squibb, outside the submitted work. Dr Kenichi Inoue reports grants and personal fees from Eisai, Chugai, Pfizer, Eli Lilly, grants from Novartis, Daiichi-Sankyo, Parexel/Puma Biotechnology, MSD, and Bayer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Jones GS, Baldwin DR. Recent advances in the management of lung cancer. Clin Med. 2018;18(Suppl 2):s41–s46. doi:10.7861/clinmedicine.18-2-s41
2. Ambroggi M, Biasini C, Toscani I, et al. Can early palliative care with anticancer treatment improve overall survival and patient-related outcomes in advanced lung cancer patients? A review of the literature. Supp Care Cancer. 2018;26:2945–2953. doi:10.1007/s00520-018-4184-3
3. Eichler M, Hechtner M, Wehler B, et al. Psychological distress in lung cancer survivors at least 1 year after diagnosis. Psychooncol. 2018;27:2002–2008. doi:10.1002/pon.4760
4. Pinheiro LC, Reeve BB. Investigating the prognostic ability of health-related quality of life on survival: a prospective cohort study of adults with lung cancer. Supp Care Cancer. 2018;26:3925–3932. doi:10.1007/s00520-018-4265-3
5. Fiteni F, Vernerey D, Bonnetain F, et al. Prognostic value of health-related quality of life for overall survival in elderly non-small-cell lung cancer patients. Eur J Cancer. 2016;52:120–128. doi:10.1016/j.ejca.2015.10.004
6. Lemonnier I, Guillemin F, Arveux P, et al. Quality of life after the initial treatments of non-small cell lung cancer: a persistent predictor for patients’ survival. Health Qual Life Outcomes. 2014;12:73. doi:10.1186/1477-7525-12-73
7. Sloan JA, Zhao X, Novotny PJ, et al. Relationship between deficits in overall quality of life and non-small-cell lung cancer survival. J Clin Oncol. 2012;30(13):1498–1504. doi:10.1200/JCO.2010.33.4631
8. Maione P, Perrone F, Gallo C, et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: a prognostic analysis of the multicenter italian lung cancer in the Elderly Study. J Clin Oncol. 2005;23:6865–6872. doi:10.1200/JCO.2005.02.527
9. Leventhal H, Brissette I, Leventhal EA. The common-sense model of self-regulation of health and illness. In: Cameron LD, Leventhal H, editors. The Self-Regulation of Health and Illness Behaviour. New York: Routledge; 2003:42–65.
10. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143:1117–1154. doi:10.1037/bul0000118
11. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the brief illness perception questionnaire. Psychol Health. 2015;30:1361–1385. doi:10.1080/08870446.2015.1070851
12. Hagger MS, Orbell S. A meta-analytic review of the common-sense model of illness representations. Psychol Health. 2003;18(2):141–184. doi:10.1080/088704403100081321
13. Kaptein AA, Yamaoka K, Snoei L, et al. Illness perceptions and quality of life in Japanese and Dutch patients with non-small-cell lung cancer. Lung Cancer. 2011;72:384–390. doi:10.1016/j.lungcan.2010.09.010
14. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60:631–637. doi:10.1016/j.jpsychores.2005.10.020
15. Aaronson NK, Ahmedzai S, Bergman B, et al. European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. doi:10.1093/jnci/85.5.365
16. van der Kloot WA, Uchida Y, Inoue K, et al. The effects of illness beliefs and chemotherapy impact on quality of life of Japanese and Dutch patients with breast or lung cancer. Chin Clin Oncol. 2016;5:3.
17. Richardson EM, Schüz N, Sanderson K, Scott JL, Schüz B. Illness representations, coping, and illness outcomes in people with cancer: a systematic review and meta‐analysis. Psycho‐oncology. 2017;26:724–737. doi:10.1002/pon.v26.6
18. Bouazza YB, Chiairi I, El Kharbouchi O, et al. Patient-reported outcome measures (PROMs) in the management of lung cancer: a systematic review. Lung Cancer. 2017;113:140–151. doi:10.1016/j.lungcan.2017.09.011
19. Lehto RH. Psychosocial challenges for patients with advanced lung cancer: interventions to improve well-being. Lung Cancer. 2017;8:79–90.
20. Reale ML, De Luca E, Lombardi P, et al. Quality of life analysis in lung cancer: a systematic review of Phase III trials published between 2012 and 2018. Lung Cancer. 2020;139:47–54. doi:10.1016/j.lungcan.2019.10.022
21. Hill KM, Amir Z, Muers MF, Connolloy CK, Round CE. Do newly diagnosed lung cancer patients feel their concerns are being met? Eur J Cancer Care. 2003;12:35–45. doi:10.1046/j.1365-2354.2003.00324.x
22. Jenkins V, Fallowfield L, Saul J. Information needs of patients with cancer: results from a large study in UK cancer centres. Br J Cancer. 2001;84:48–51. doi:10.1054/bjoc.2000.1573
23. Faller H, Koch U, Brähler E, et al. Satisfaction with information and unmet information needs in men and women with cancer. J Cancer Surviv. 2016;10:62–70. doi:10.1007/s11764-015-0451-1
24. Salsman JM, Pustejovsky JE, Schueller SM, et al. Psychosocial interventions for cancer survivors: a meta-analysis of effects on positive affect. J Cancer Surviv. 2019;13:943–955. doi:10.1007/s11764-019-00811-8
25. Licqurish SM, Cook OY, Pattuwage LP, et al. Tools to facilitate communication during physician-patient consultations in cancer care: an overview of systematic reviews. CA Cancer J Clin. 2019;69:497–520. doi:10.3322/caac.v69.6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.