Back to Journals » Patient Preference and Adherence » Volume 16
Illness Beliefs, Treatment Beliefs, and Fulfilled Treatment Expectations in Psychosomatic Rehabilitation: Associations with Patient Satisfaction
Authors Glattacker M ![]() , Rudolph M, Bengel J, von der Warth R
, Rudolph M, Bengel J, von der Warth R
Received 20 September 2022
Accepted for publication 1 December 2022
Published 15 December 2022 Volume 2022:16 Pages 3303—3317
DOI https://doi.org/10.2147/PPA.S390596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Manuela Glattacker,1 Matthias Rudolph,2 Jürgen Bengel,3 Rieka von der Warth1
1Section of Health Care Research and Rehabilitation Research, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany; 2Deutsche Rentenversicherung Rheinland-Pfalz (German Statutory Pension Insurance Rhineland Palatinate); Mittelrhein-Klinik (Clinic for Psychosomatic Rehabilitation), Boppard-Bad Salzig, Germany; 3Section of Rehabilitation Psychology and Psychotherapy; Department of Psychology; University of Freiburg, Freiburg, Germany
Correspondence: Manuela Glattacker, Section of Health Care Research and Rehabilitation Research, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Hugstetter Str. 49, Freiburg, D-79106, Germany, Tel +49 761 270 36940, Email [email protected]
Purpose: Patients’ illness and treatment beliefs have been shown to predict health outcomes in many health care settings. However, information about their impact on patient satisfaction is scarce. The aim of this study was to investigate illness- and rehabilitation-related treatment beliefs and met rehabilitation-related treatment expectations and their relationship with patient satisfaction in psychosomatic rehabilitation.
Methods: In a repeated measures study design, patients filled out questionnaires 2 to 3 weeks before the start of rehabilitation and at the end of an inpatient rehabilitation 6 to 7 weeks later. The predictive value of illness beliefs, treatment beliefs, and fulfilled treatment expectations regarding patient satisfaction was analyzed with multiple hierarchical regression analyses controlling for sociodemographic and clinical variables.
Results: Two hundred sixty-four patients participated. The sample was composed of equal numbers of men and women (n = 129 each). The mean age was 50.4 years. Most patients had diagnoses from the ICD– 10 diagnostic group F3 (affective disorders; n = 145) or F4 (neurotic, stress-related and somatoform disorders; n = 94). Sociodemographic and clinical variables were not associated with patient satisfaction. The explained variance of patient satisfaction increased to 10% by adding illness beliefs (namely personal control and coherence) (p = 0.006), to 5% by adding rehabilitation-related treatment beliefs (namely concerns) (p = 0.063), and to 49% by adding fulfilled expectations (namely a positive discrepancy between expectations and experiences related to outcome expectations and related to participation and treatment structure, and a negative discrepancy between expectations and experiences related to concerns) (p < 0.001) as predictor variables.
Conclusion: This study highlights the relationship of fulfilled (rehabilitation-related) treatment expectations with patient satisfaction in psychosomatic rehabilitation. Given the evidence underlining the importance of patients’ illness and treatment beliefs and expectations, it is vital that these constructs are addressed in corresponding interventions.
Keywords: psychosomatic rehabilitation, patient satisfaction, common sense model of self-regulation, illness beliefs, treatment beliefs, fulfillment of treatment beliefs
Introduction
Psychosomatic rehabilitation is a supplement to psychiatric inpatient and psychiatric and psychotherapeutic ambulatory care, and plays a pivotal role in health care for patients with mental health conditions in Germany. Psychosomatic rehabilitation usually takes place in an inpatient setting with an average length of stay of 5 weeks.1 The diagnostic spectrum is wide, with a high proportion of mood disorders, anxiety disorders, adjustment disorders, and somatoform disorders.1 Patients attending psychosomatic rehabilitation usually have been experiencing a chronic course of their mental disorders of at least 6 months, which is associated with significant restrictions in social or occupational participation. Therefore, on the conceptual basis of the biopsychosocial model of the International Classification of Functioning, Disability and Health (ICF),2 psychosomatic rehabilitation offers a holistic approach that focuses on reducing symptoms, improving functioning and participation in social and occupational life, and fostering patients’ self-regulation.1,3 For this purpose, a multimodal program is delivered by a multi-professional team. This program consists most of all of disease-specific individual or group-based psychotherapy, patient education, somatic treatments (eg, medications), and interventions supporting work reintegration.1
Overall, the effectiveness and efficacy of psychosomatic rehabilitation can be considered proven.4 However, a significant number of patients (20–30%) do not respond to inpatient psychosomatic treatment, with up to 10% experiencing a decline in health.5 Furthermore, while patient satisfaction in the rehabilitation context is generally good,6 a survey of more than 17,000 patients in psychosomatic rehabilitation showed that they were significantly less satisfied with their rehabilitation than patients in other rehabilitation contexts, such as orthopedic or cardiac rehabilitation.7
To optimize outcomes for patients who do not respond to treatment or are dissatisfied, a good starting point is to identify potentially modifiable predictors of outcome and of patient satisfaction and incorporate them into treatment.
Regarding treatment outcome, a high symptom burden, chronic disease course, early nonresponse, personality disorder(s), and an insufficient therapeutic alliance have been shown to be significant predictors of a negative treatment outcome in psychosomatic rehabilitation.5 Furthermore, there is evidence for the relevance of patients’ illness and treatment beliefs in predicting health outcomes in (psychosomatic) rehabilitation.8–11 This is consistent with a large body of research in the broader context of mental health12 and in other health care settings.13,14
Regarding predictors of patient satisfaction in psychosomatic rehabilitation, there are comparatively few studies. Of the existing studies, identified predictors include age, chronicity, self-efficacy, goal attainment, patient activation, concerns, (mental) health status, and information provision.15–17 Beyond this health care setting, age seems to be a relatively robust predictor of patient satisfaction in health care in general18,19 as well as in the context of mental health,20 with older people being more satisfied. In addition, illness beliefs, expectations and fulfilled expectations or a lack of unmet expectations respectively, have been identified as important predictors of patient satisfaction.18,19,21,22 For example, a review that examined the factors associated with satisfaction with inpatient psychiatric services demonstrated that service users’ satisfaction was influenced by their perceptions of illness and hospitalization: Coercion was negatively related, and voluntarily admission, open wards, and the perception of the own need of treatment was positively related to satisfaction.23
The results, which show the importance of illness beliefs and treatment beliefs on treatment outcome and patient satisfaction, can be interpreted in the context of a well-known health psychology model, namely the common-sense model of self-regulation (CSM).24,25 According to the CSM, illness and treatment beliefs are conceptualized as core elements of the health-related self-regulation process. Illness beliefs include patients’ perceptions about the symptoms, and beliefs about the cause, timeline, control/cure and consequences of the illness, as well as emotional reactions.25 Treatment beliefs, on the other hand, differ in relation to the treatment and diagnosis. For instance, in the context of drug-based treatments, perceived necessity and concerns are core elements of treatment beliefs.26 Regarding the content of rehabilitation-related treatment beliefs, evidence is scare. However, an explorative qualitative study of patients in psychosomatic rehabilitation showed that psychosomatic-specific rehabilitation-related treatment beliefs include perceived reasons for rehabilitation and a range of expectations, which can be conceptualized as an inherent part of the construct of future-oriented beliefs.27,28 Concretely, psychosomatic-specific rehabilitation related treatment beliefs refer to expectations relating to the process of rehabilitation (eg, organization and content of rehabilitation), expectations relating to the results of rehabilitation (eg, symptom reduction or vocational participation), expectations towards one’s own behaviour during therapy (eg participating actively in therapies), and expectations to rehabilitation-related concerns (eg negative reactions by others).29 These results fit well with psychotherapy research, where outcome expectations and expectation about the process of therapy have been identified as the main patient expectancy factors.30
The aim of our study was to investigate the association of illness beliefs and rehabilitation-related treatment beliefs with patient satisfaction in psychosomatic rehabilitation. In addition, taking into account the evidence for the importance of met expectations in other health care settings, we further analyzed the relevance of the fulfillment of rehab-related expectations.
Building on the literature, we hypothesized, that threat-related illness beliefs (perceived symptoms, perceived consequences, a perceived chronic disease course and strong emotional reactions to the illness) would be associated with lower patient satisfaction, and that protective illness beliefs (perceived control and coherence) would be associated with higher patient satisfaction. Relating to rehabilitation treatment beliefs, we hypothesized, that expectations towards treatment results would be positively associated and concerns would be negatively associated with patient satisfaction. Lastly, we hypothesized that the fulfillment of rehab-related expectations would be associated with patient satisfaction.
In all of these analyses, we controlled for sociodemographic and clinical variables.
Materials and Methods
The study was conducted at the Medical Center of the University of Freiburg and a cooperating psychosomatic clinic in Rhineland–Palatinate, Germany. Ethical approval was granted by the ethics committee at the University of Freiburg (Approval Number: 231/18). The study was registered in the German Clinical Trial Register (DRKS00014830). The study complies with the Declaration of Helsinki.
Recruitment
Patients were recruited consecutively between April 2019 and January 2020 at the above-mentioned cooperating inpatient psychosomatic rehabilitation clinic. All patients who were registered for inpatient rehabilitation were asked to fill out questionnaires at two measurement points: Illness beliefs, rehabilitation-related treatment beliefs, and sociodemographic and clinical variables were assessed 2 to 3 weeks before the start of rehabilitation (Time 0 [T0]), and fulfillment of rehabilitation-related expectations and patient satisfaction were measured at the end of rehabilitation (Time 1 [T1]), 6 to 7 weeks later. All questionnaires were self-completed by the patients. Along with the first set of questionnaires, patients received written study information by mail that described the study design, terms of voluntary participation, and data protection regulation. All patients gave written informed consent to participate in the study.
Measures
Patient satisfaction was measured using the ZUF–8 (Fragebogen zur Patientenzufriedenheit/Questionnaire to evaluate patient satisfaction),31 whose development is based on the Client Satisfaction Questionnaire.32 The ZUF–8 is a widely used self-report instrument that assesses global patient satisfaction with eight items and four answer options each. The items are summed to a total score ranging from 8 to 32, with higher values representing higher patient satisfaction. The psychometric properties of this questionnaire are good.7 Also in this study, the internal consistency of the ZUF–8 was good, with a Cronbach’s α of 0.9.
Illness beliefs were operationalized using the German version33 of the Illness Perception Questionnaire-Revised (IPQ–R).34 The IPQ–R is based on the aforementioned common-sense model of self-regulation24,25 and assesses nine illness belief dimensions with 64 items: illness identity (symptoms that are attributed to the illness), timeline (chronic vs acute, (example item “My illness will last for a long time”)), timeline cyclical (example item “My symptoms come and go in cycles”), consequences (example item “My illness has major consequences on my life”), personal control (example item “Nothing I do will affect my illness”), treatment control (example item “My treatment will be effective in curing my illness”), coherence (example item “I have a clear picture or understanding of my condition”), emotional representation (example item “I get depressed when I think about my illness”), and cause. In this study, causal beliefs were analyzed via single items. Therefore, this dimension was excluded from our prediction analyses. With the exception of the identity scale, which represents a sum score of symptoms attributed to the illness (range = 1–17), the IPQ–R scale scores range from 4 to 20 (timeline cyclical, personal control, treatment control) and from 5 to 25 (timeline acute–chronic, consequences, coherence, and emotional representations), respectively. High values represent higher levels of the scale constructs (eg, the perception that the illness will have a chronic or cyclic timeline, or that the illness will result in many consequences, or is controllable by the patient (personal control) or by treatment (treatment control)). The psychometric properties of the German version of the IPQ–R are good.35 In this study, the internal consistence was acceptable to good with Cronbach’s α ranging from 0.69 to 0.87.
Rehabilitation-related treatment beliefs were assessed with the Rehabilitation Treatment Beliefs Questionnaire–Psychosomatic (RTBQ–Psych).36 Based on the results of an explorative qualitative study of patients in psychosomatic rehabilitation,29 this questionnaire assesses different aspects of rehabilitation-related treatment beliefs. 30 items form six scales: (1) outcome expectations (example item “I expect this rehabilitation will make me feel better in general.”), (2) process expectations regarding participation and treatment structure (example item “I expect to be involved in the goal setting for this rehabilitation by the doctor.”), (3) process expectations regarding information (example item “I expect the information about my illness and treatment to be sufficient.”), (4) process expectations regarding leisure time and social contacts (example item “I expect to establish new contacts.”), (5) concerns (example item “I am concerned the rehabilitation will overburden me.”), and (6) necessity (example item “Without this rehabilitation, my illness would get worse.”). Scales range from 0 to 10, with higher scores indicating stronger treatment beliefs regarding outcome and process expectations, concerns, and necessity. The psychometric properties of the RTBQ–Psych are satisfactory.36 In this study, internal consistency, measured using Cronbach’s α, ranged from 0.78 to 0.87.
At the end of rehabilitation, the patients’ experience regarding the above-mentioned treatment beliefs was assessed with the same items used in RTBQ–Psych, that could be answered on 5-point Likert scales with response options ranging from not true at all to completely true. Finally, the fulfillment of rehabilitation-related expectations was operationalized as a difference of beliefs (premeasurement: before rehabilitation) and experiences (postmeaseurement: at the end of rehabilitation) relating to outcome and process expectations and concerns. To calculate these scales, we subtracted the premeasurement values from the postmeasurement values. This means that values of 0 represent exactly fulfilled expectations, values <0 represent an underachievement of expectations, and values > represent exceeded expectations.
In addition to predictor and outcome variables, we assessed different sociodemographic and clinical data that were considered as covariates, namely age, gender, initial symptom burden, and diagnostic group. The diagnosis was made by the therapists at the psychosomatic rehabilitation clinic based on the ICD–10 at the beginning of rehabilitation. Age, gender, and initial symptom burden were measured through the patient prior to admission. Initial symptom burden was assessed via the Psychological Well-Being scale of the Hamburger Modules for the Assessment of Psychosocial Health in Clinical Practice.37 This questionnaire is widely used in the context of psychosomatic rehabilitation in Germany and has good psychometric properties.37 Scores on the Psychological Well-Being scale range from 0 to 4, with a high score representing high symptom burden. In our study, internal consistence was good, with a Cronbach’s α of 0.86.
Data Analysis
We analyzed the predictive value of illness beliefs, treatment beliefs, and the fulfillment of rehabilitation-related expectations regarding patient satisfaction by conducting multiple hierarchical regression analyses. Two regression steps were performed with age, gender, diagnostic group (binary F3 or F4 according to the ICD–10), and initial symptom burden relating to psychosocial well-being being included as predictors in the first step. In the second step, the scales of the IPQ–R (Regression I), of the RTBQ–Psych (Regression II) or the differences of beliefs before rehabilitation and experiences (Regression III) were included, respectively.
We tested assumptions for the regression models by checking the plots of residual values (*ZRESID) against predicted values (*ZPRED), normal P–P plots, and the variance inflation factor value, with values above 5 considered an indication of multicollinearity. We also inspected the Durbin–Watson statistic. With a range of 0 to 4, values around 2 are interpreted as indicating no autocorrelation. Missing values were excluded listwise. Analyses were done using IBM SPSS Statistics (Version 27).38
Results
Sample
From a total of 832 eligible patients, 264 (32%) agreed to participate in this study. Because nonparticipants did not provide consent for data collection, the reasons for nonparticipation are unknown. The sample was composed of equal numbers of men and women (n = 129 each), and the mean age was 50.4 years. Most participants had a chronic disease course, with 29% of patients suffering from the disease for more than 10 years. Most patients had diagnoses from the ICD–10 diagnostic group F3 (affective disorders; n = 145) or F4 (neurotic, stress-related and somatoform disorders; n = 94). Within these groups, F33.1 (recurrent depressive disorder, current moderate episode; n = 66), F32.1 (moderate depressive episode; n = 33), and F43.2 (adjustment disorders; n = 31) were diagnosed most often. Data on patient characteristics are displayed in Table 1.
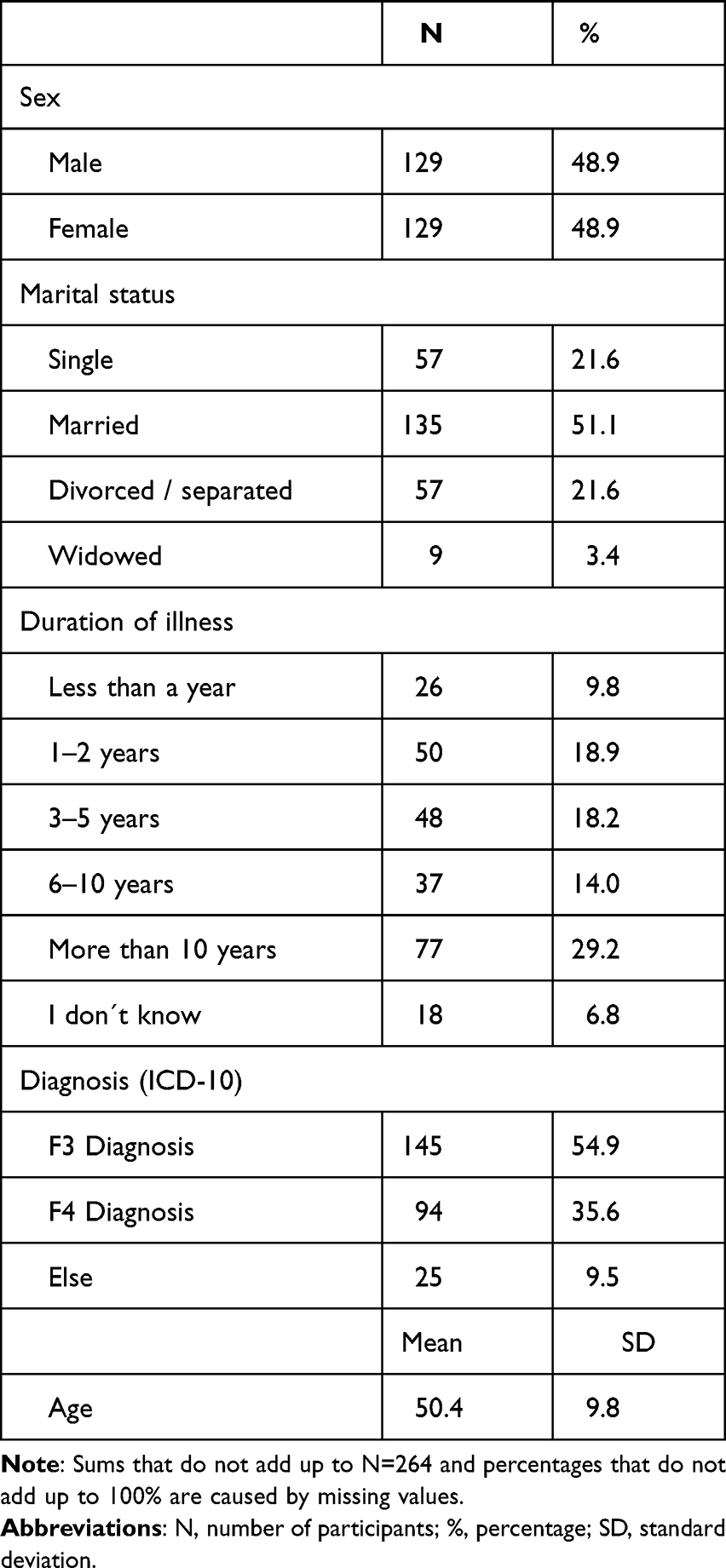 |
Table 1 Sociodemographic Data of Participants (N=264) |
Description of Patient Satisfaction, Illness Beliefs, Rehabilitation-Related Treatment Beliefs, Experiences Relating to Treatment Beliefs, and the Fulfillment of Treatment Expectations
One hundred sixty patients (60.6% of the study participants) filled out the ZUF–8, which assessed patient satisfaction at the end of rehabilitation. Within a range of 8 to 32, the mean of 22.1 (SD = 4.5) showed a relatively high overall level of patient satisfaction. Table 2 summarizes the patients’ illness beliefs and their rehabilitation-related treatment beliefs before the start of rehabilitation as well as their experiences relating to treatment beliefs at the end of rehabilitation.
 |
Table 2 Descriptive Statistics of Illness Beliefs, Treatment Beliefs (Expectations) and Experiences Relating to Treatment Beliefs |
In the context of illness beliefs, patients attributed between eight and nine symptoms to their illness. They perceived their illness as relatively chronic and as having relatively many consequences. On average, treatment control was a little bit higher than perceived personal control. Furthermore, emotional representation was higher than patients’ coherence of their illness.
In regard to rehabilitation-related treatment beliefs, patients had high expectations regarding the outcomes of rehabilitation, the participation in the rehabilitation process and treatment structure, and information provision during rehabilitation. Compared with this, patient’s concerns, and their expectations regarding leisure time and social interaction, were lower.
Looking at the experiences relating to treatment belief domains at the end of rehabilitation, on average, patients most frequently reported on experiences regarding leisure time and social contacts and information provision during rehabilitation. Experiences relating to participation and treatment structure were less often affirmed, followed by experiences relating to outcome expectations. Experiences that addressed patients’ concerns were the least reported.
Data on the fulfillment of treatment expectations as a relation of experiences and beliefs are summarized in Table 3.
 |
Table 3 Descriptive Statistics of the Fulfilment of Treatment Expectations |
On average, treatment expectations were underachieved in terms of rehabilitation outcomes, participation and treatment structure and, to a lesser extent, in terms of information provision and concerns. In contrast, expectations relating to leisure time and social contacts were exceeded. Exactly fulfilled expectations were rare (ranging from 3.1% of patients in terms of outcome expectations to 11.7% patients in terms of participation and treatment structure). For 86.8% of patients, outcome expectations were underachieved, while this proportion was lower for expectations in terms of participation and treatment structure (69.8%) and information provision during rehabilitation (54.3%). Expectations in terms of leisure time and social contacts were exceeded for 71.6% of patients. Patients’ concerns have not occurred as expected for 70.7% of patients.
Associations with Patient Satisfaction
The plots we examined showed no deviations of the residuals from a normal distribution. The variance inflation factor values in the final regression models were all <5. Durbin–Watson values were 1.7, 1.8, and 1.6 respectively. Only patients with a diagnosis of an affective disorder (ICD–10: F3; n = 145) or a neurotic, stress-related, and somatoform disorder (ICD–10: F4; n = 94) were included into the regression analyses because these diagnostic groups accounted for most of the participants. The results regarding illness beliefs, rehabilitation-related treatment beliefs, and fulfilled expectations as predictors of patient satisfaction are displayed in the Tables 4 through 6.
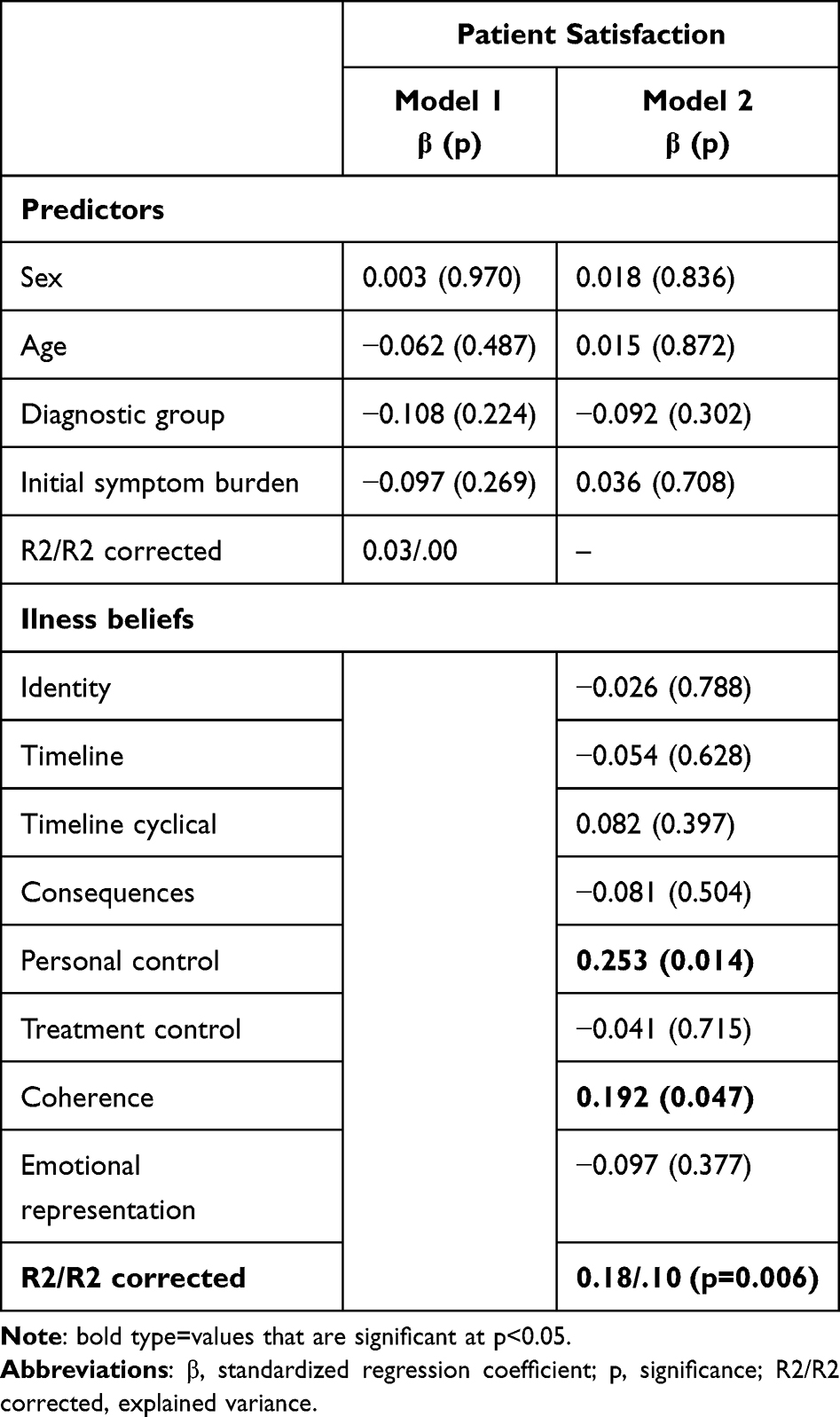 |
Table 4 Illness Beliefs as Predictors of Patient Satisfaction - Regression Analyses (N=133) |
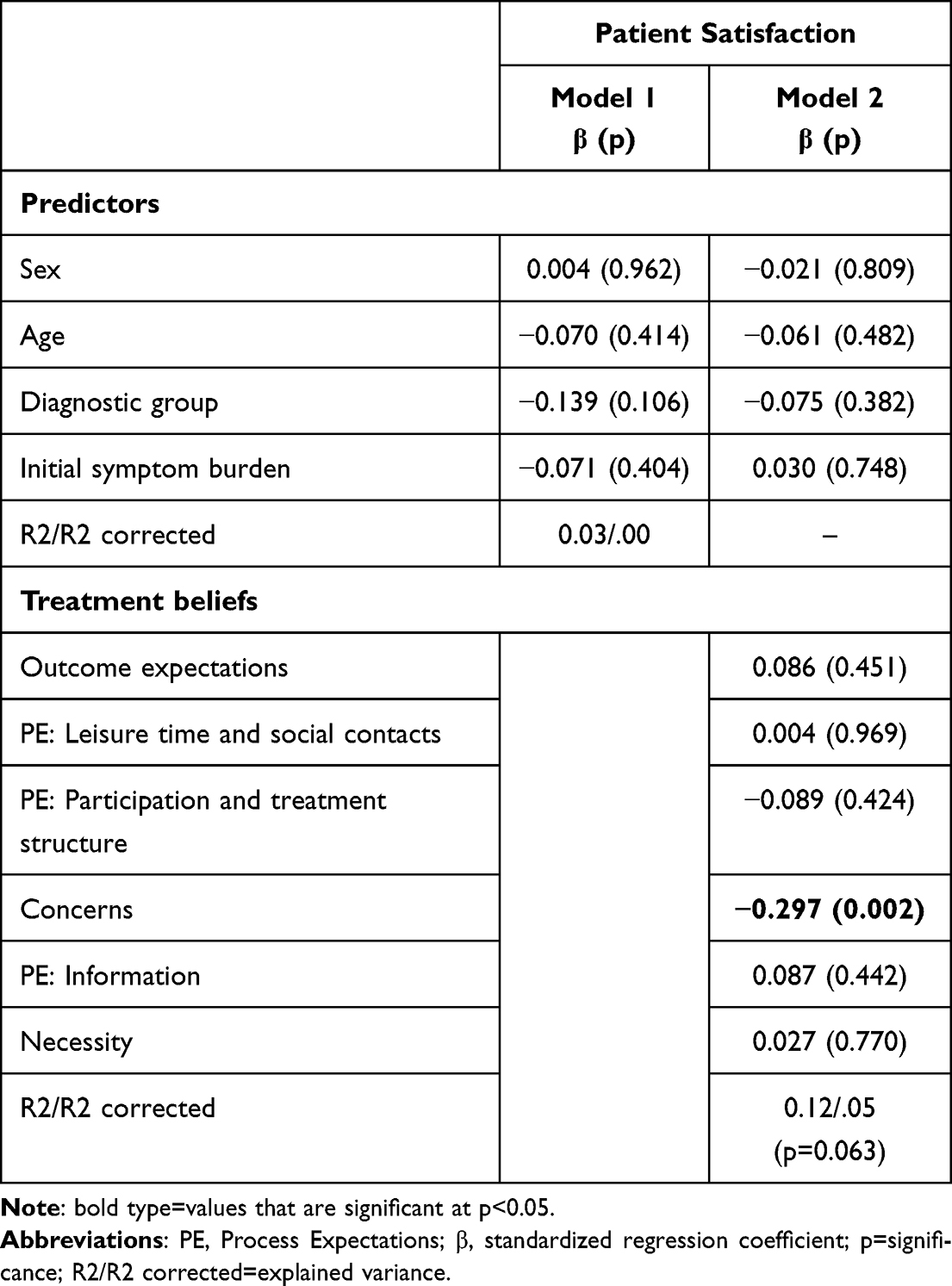 |
Table 5 Treatment Beliefs as Predictors of Patient Satisfaction - Regression Analyses (N=140) |
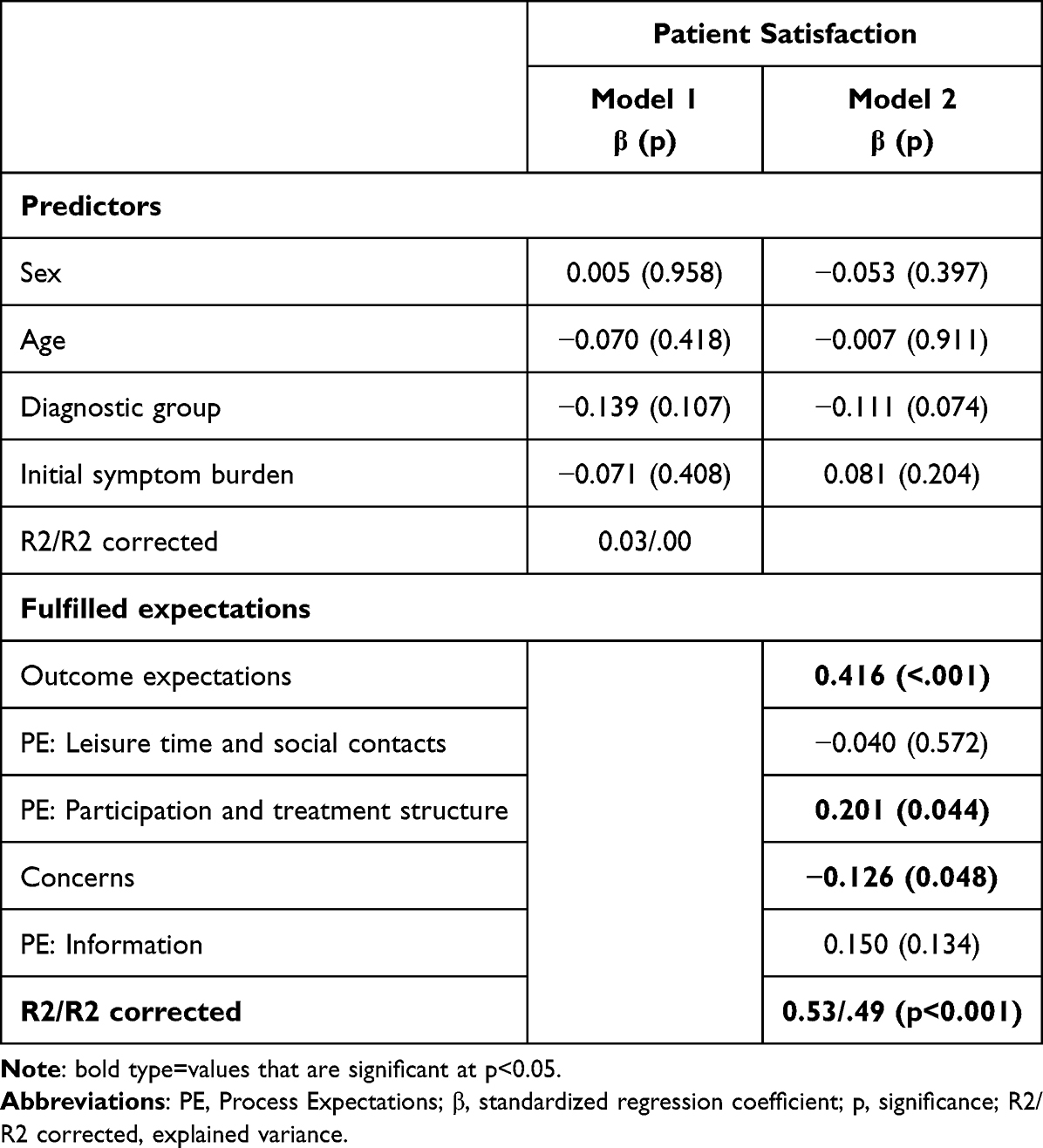 |
Table 6 Fulfilled Expectations as Predictors of Patient Satisfaction - Regression Analyses (N=139) |
Age, sex, diagnostic group, and initial symptom burden relating to psychosocial well-being were not associated with patient satisfaction in any of the regression analyses (R2corr = 0.00). The explained variance of patient satisfaction increased to 10% by adding illness beliefs (Table 4), to 5% by adding rehabilitation-related treatment beliefs (Table 5), and to 49% by adding fulfilled expectations (Table 6) as predictor variables. The whole regression model predicting patient satisfaction via treatment beliefs was not significant, while the other two models were.
In the context of illness beliefs, two dimensions turned out to be significant predictor variables: Perceived personal control and perceived coherence prior to rehabilitation were associated with higher patient satisfaction at the end of rehabilitation.
In the context of rehabilitation-related treatment beliefs, only one dimension reached the significance threshold: Patients who had fewer concerns prior to rehabilitation were more satisfied with rehabilitation.
With regard to fulfilled expectations, three of the five dimensions were found to be significant predictor variables of patient satisfaction: A (positive) discrepancy between expectations and experiences related to outcome expectations, and related to participation and treatment structure, as well as a (negative) discrepancy between expectations and experiences related to concerns, were associated with higher patient satisfaction.
Discussion
We investigated the relationship of illness beliefs and rehabilitation-related treatment beliefs as well as the fulfillment of rehabilitation-related expectations with patient satisfaction in psychosomatic rehabilitation, controlling for sociodemographic and disease-related variables, applying a repeated measures design.
With a mean of 22.1 on the ZUF–8, patient satisfaction was relatively high but lower than in other studies in the context of psychosomatic rehabilitation, with means of 26.4,15 and 25.3, respectively.7 Furthermore, patients in our study expressed more threat-related illness beliefs (eg, more perceived consequences and a perceived chronic course of the disease) than patients with depression from a previous psychosomatic rehabilitation study.39 Because we used a new questionnaire to assess rehabilitation-related treatment beliefs,36 there is no study with which to compare our results in this regard. However, it became apparent that, at the end of rehabilitation, patients reported comparatively fewer experiences in the dimensions characterized by high expectations and more experiences in dimensions characterized by lower expectations. Thus, patients’ treatment expectations were underachieved in terms of rehabilitation outcomes, participation, and treatment structure and, to a lesser extent, in terms of information provision and concerns, whereas expectations regarding leisure time and social contacts were exceeded. Exactly met expectations were rare.
When we analyzed relationships with patient satisfaction, we found that sociodemographic variables were not associated with patient satisfaction in our study. Related to age, this contradicts findings from earlier studies, which have shown older age to be associated with higher patient satisfaction in the context of psychosomatic rehabilitation,15 in the broader mental health context20 and beyond.18,19 Apart from that, our findings are consistent with those of other studies showing that sociodemographic variables have a weak, an inconsistent, or no association with patient satisfaction.20,23 In regard to clinical variables, our results did not confirm the association of initial burden regarding mental health status with patient satisfaction from earlier studies.15 However, this result might be explained by the different operationalization of initial burden in these studies.
In contrast to sociodemographic and illness-related variables, illness beliefs, treatment beliefs, and met treatment expectations were associated with patient satisfaction. In sum, this result fits well into a body of research showing the impact of these variables on different outcomes in many samples and settings.
Regarding illness beliefs, protective illness belief dimensions—namely, perceived personal control and perceived illness coherence prior to rehabilitation—were associated with higher patient satisfaction. This confirms our hypothesis and coincides with previous findings on the prediction of health outcomes through protective illness beliefs in the context of psychosomatic rehabilitation,40,41 in meta-analyses of physical illnesses,14 medically unexplained symptoms,42 and mental illness.12 However, those studies also found an association between threat-related illness beliefs (eg, perceived consequences or perceived chronicity of the illness) for worse health outcomes. Contrary to our corresponding hypothesis, this was not the case in our study.
Regarding rehabilitation-related treatment beliefs, the whole regression model failed to reach statistical significance. However, patients’ concerns turned out to be related with patient satisfaction. This is consistent with our hypothesis and with other studies that have shown the relevance of this dimension in predicting health outcomes in psychosomatic rehabilitation.15,40,41 Other dimensions of treatment beliefs, such as outcome and process expectations, have not been associated with patient satisfaction. This contradicts our hypothesis and findings of placebo research,43–46 psychotherapy research30,47,48 and rehabilitation research,40,41 which show that patient expectations are among the strongest predictors of treatment outcomes in many conditions. However, although outcome and process expectations per se were not related to patient satisfaction in our sample, met expectations relating to these dimensions were. This is consistent with our hypothesis. In particular, a (positive) discrepancy between expectations and experiences related to outcome expectations, and related to participation and treatment structure as well as a (negative) discrepancy between expectations and experiences related to concerns were associated with higher patient satisfaction. These findings are in line with those of recent studies that have demonstrated the high relevance of met expectations predicting patient satisfaction and other outcomes in, for example, orthopedic patients and in general medicine.19,21,22,49
The explained variance in patient satisfaction ranged from low (5% by rehabilitation-related treatment beliefs or 10% by illness beliefs) to relatively good, with 49% by met expectations. Overall, this is consistent with other studies, often explaining only a small portion of the variance in satisfaction—almost always considerably less than 50%.19 Therefore, it is still in part unknown which factors contribute to patient satisfaction. This might be discussed along with the basic criticisms of the patient satisfaction construct, namely, its rare theoretical or conceptual development; its low standardization and reliability; and its uncertain validity, which is also reflected in difficulties relating to its measurement.50 In this context, it is important to consider whether unmet expectations in this study are a cause or operationalization of patient satisfaction19 because—among other conceptualizations50 —patient satisfaction can be explicitly defined as a function of patients’ responses to experienced care mediated by their preferences and expectations.51
The setting of our study is psychosomatic rehabilitation, which is quite specific to the German health care context. Psychosomatic rehabilitation focuses on reducing symptoms, improving functioning and participation in social and occupational life, and fostering patients’ self-regulation. For this purpose, a multimodal program is delivered with disease-specific individual or group-based psychotherapy as a key focus. The diagnostic spectrum in psychosomatic rehabilitation is wide, with a high proportion of disorders such as mood disorders or anxiety disorders, which also are highly prevalent in the overall context of mental health. Due to these diagnostic and treatment overlaps, we argue that our main results describing the association of illness beliefs, treatment beliefs and fulfilled expectations with patient satisfaction might be of relevance also for other health care settings for individuals with mental health. This is underlined by the results and conclusions of the above mentioned meta-analysis in the context of mental illnesses including 28 independent samples representing 3051 patients with mood, anxiety, schizophrenia spectrum, substance use and eating disorders from twelve different countries in Africa, Asia, North America, and Europe.12 However, studies in some diagnostic groups are lacking, and most studies are cross-sectional. Therefore, additional research is needed to analyse the dynamic and causal relationships between patient beliefs and outcomes in mental illnesses.
From a clinical perspective, the current state of evidence from primary studies and meta-analyses involving many diseases and health care settings highlighted patient beliefs and expectations as important targets for the development of interventions. However, eliciting and addressing (unmet) expectations in the health care sector—such as in primary care52 and especially in the context of mental illness – is not new. For example, referring to expectations as a common factor of psychotherapy, Greenberg et al23 pointed out that “the reshaping of patient expectations (or assumptions) appears to be at the foundation of virtually every major model of psychotherapy”,30 and they proposed clinical strategies for fostering patients’ positive expectations. These include clinicians being attentive to patients’ beliefs about the nature of treatment and addressing any concerns or discrepancies.
In addition, explicit expectation-focused psychological interventions have been developed and applied in the context of various diseases, such as coronary heart disease, cancer44 and mental health.53,54 These interventions emphasise expectations as a central feature of mental disorders and use expectancy change as a central treatment mechanism. So far, only a few studies have investigated the effects of these interventions, with mainly positive results.44
Finally, health psychology theories, such as the common-sense model of self-regulation, provide a theory-driven way to specify and discuss the concrete content of patients’ illness and treatment beliefs. Therefore, these constructs have been considered in some common-sense model of self-regulation-based interventions. For example, in two own studies with patients with depression or with chronic back pain,39,55 we aimed at improving provision of information on illness and treatment during inpatient rehabilitation by tailoring the information to patient’s illness and treatment beliefs. The intervention consisted of three twenty-minute patient sessions with a trained physician and a psychologist at cooperating rehabilitation centres. The content of each patient’s intervention was based on an individual assessment of their illness and treatment beliefs, for example regarding the symptoms they attributed to the illness, the perceived chronicity and consequences or controllability of the illness. The results of this assessment was summarised in an individual “feedback form”, which was used by physicians and psychologists as a guide for tailoring the information. Overall, such common-sense model of self-regulation-based interventions have produced encouraging results,56–62 in the (psychosomatic) rehabilitation context as well.39,55
Despite these efforts, the explicit and focused clinical addressing of patients beliefs and expectations may have been undervalued so far30– also in the treatment of mental illnesses.12 Thus, we conclude that it would be worthwhile to further develop interventions that take into account both patients’ illness beliefs and treatment-specific treatment beliefs more precisely, ie depending on the treatment focus, beliefs about medication (such as fear of side effects or as becoming dependent on antidepressants), beliefs about psychotherapy (such as presumed effectiveness of psychotherapy), or – as in our study – beliefs about (psychosomatic) rehabilitation. The latter could be done discussing, patients’ concrete outcome and process expectations, and their concerns about rehabilitation. Doing so, professionals could check whether unrealistic expectations can be changed to be more realistic or whether and how realistic expectations (eg, regarding patients’ participation in the rehabilitation process) can be met. Such interventions would fit well with the patient-centered approach used in (psychosomatic) rehabilitation to ultimately promote patients’ self-regulation.
Limitations and Strengths
Our study has some limitations. Only 32% of the eligible patients agreed to participate; thus, we cannot rule out a selection bias. In addition, only 60% of the participants filled out the questionnaire assessing patient satisfaction. Reasons for dropout are unknown but could lead to further bias.
In contrast to a previous meta-analysis that examined the effectiveness of psychosomatic rehabilitation, our sample was older (50.4 years vs 41.8 years) and included more men (48.9% vs 36.0%).4 The higher proportion of male participants can be explained by the occupancy of the cooperating rehabilitation clinic. The clinic is predominantly delivered by the German Pension Insurance Rhineland-Palatinate (former state insurance institution/Landesversicherungsanstalt), where traditionally more men were insured.
Our study participants represented their illness as more severe than patients from another study in the context of psychosomatic rehabilitation,39 and patient satisfaction was somewhat lower than in other studies from this field.7,15 Therefore, it is possible that we included rather burdened patients, which may have influenced their patient satisfaction ratings as well. Furthermore, we do not know whether—relative to the initial sample—the patients who participated in the survey were overall rather satisfied or dissatisfied, limiting the generalizability of our results. With respect to diagnoses, we considered in our analyses only patients with a diagnosis of affective disorders or neurotic, stress-related, and somatoform disorders. These diagnostic groups accounted for the majority of the participants in our study (91%) and represent the most common diagnoses in psychosomatic rehabilitation. However, our results may not be generalizable to patients with other diagnoses who are also treated in psychosomatic rehabilitation, such as patients with hyperkinetic disorders.
A further limitation refers to the operationalization of the multidimensional concept of patient satisfaction50 using an unidimensional score assessing global patient satisfaction. However, the ZUF–8 is a widely used instrument, whose development is based on the well-established Client Satisfaction Questionnaire,32 and it has good psychometric properties.7
Some of the predictors, especially process expectations and outcome expectations, had ceiling effects. This might have reduced their predictive value. However, as we had no indication, that a linear model does not fit our data, we refrained from transforming the predictor variables.
In addition, because of methodological considerations, we decided to include only some basic sociodemographic and clinical covariables into our analyses that we considered most important. However, other variables, such as duration of illness or rehabilitation experience, could have been relevant potential predictor variables of patient satisfaction. In order to include more confounding variables, a bigger sample size would have been needed.
Last, we used a fairly new questionnaire to assess rehabilitation-related treatment beliefs. The psychometric quality of this questionnaire is acceptable,36 however, further psychometric testing is pending.
Strengths of our study are its longitudinal design, which accounted for potential confounding sociodemographic and clinical variables, a sufficient sample size (based on the “one in ten rule” for multiple regressions63), and the use of reliable and valid instruments to assess patient satisfaction and the predictor variables. Furthermore, assessing the fulfillment of expectations, we directly related rehabilitation-related experiences at the end of rehabilitation to prerehabilitative expectations, something that is often neglected in studies that examine the fulfillment of expectations.21 However, when we refer to “fulfilled expectations” here, we must keep in mind that exactly met expectations were rare and that our variable instead represented discrepancies between expectations and experiences, including an overfulfillment of expectations.
Conclusion
Illness and treatment beliefs are predictors of outcomes in psychosomatic rehabilitation.41 In addition to these constructs, our study highlighted the relevance of fulfilled (rehabilitation-related) treatment expectations on patient satisfaction. Given the evidence underlining the importance of patients’ illness and treatment beliefs and expectations in many somatic and mental diseases and health care settings, their explicit and focused clinical addressing seems vital. The applicability of health psychology theories such as the common-sense model of self-regulation as a theory-driven basis for such interventions has been demonstrated in the rehabilitation setting and beyond. For the context of psychosomatic rehabilitation, it seems worthwhile to further develop and evaluate such interventions.
Further suggestions for future research can be derived from the limitations of our study. In addition, following the common-sense model of self-regulation, the process of health-related self-regulation is highly dynamic containing reciprocal interactions between its elements. This means that not only illness beliefs and treatment beliefs affect coping procedures and health outcomes, but also that, for example, health outcomes affect illness and treatment beliefs.
Future research should clarify these dynamic aspects of the components of the CSM.64 For the context of mental health this is predominantly interesting as many psychotherapeutic interventions explicitly target modification of patients’ illness and treatment beliefs. Therefore, the development of functional illness beliefs can be seen as a treatment outcome in itself.
Finally, the self-regulation process is continuously affected by contextual factors such as illness and treatment experiences or interaction with professionals or family members.65 These context variables should be another focus for future research.66
Data Sharing Statement
Data can not be shared because of our data protection guidelines. Because the patients in this project are all recruited within one rehabilitation clinic during a specific time period, it cannot be ruled out that patients could be identified despite anonymisation of the data (for example through combinatorics of sociodemographic or clinical data). Thus, data protection is part of informed consent and of the ethics approval.
Acknowledgments
This work was funded by the German Federal Pension Insurance Rhineland Palatinate [432 – 01 – 3351]. The authors are responsible for the content of the article. We thank the patients for participating in this study. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Funding
This work was funded by the German Federal Pension Insurance Rhineland Palatinate [432 – 01 – 3351]. The authors are responsible for the content of the article. The sponsor had no involvement in the study nor in the publication.
Disclosure
Matthias Rudolph as employee of the German Federal Pension Insurance Rhineland Palatine, helped conceptualize the study and supported the recruitment of participants, but was not further engaged into the analysis of the data. Manuela Glattacker, Jürgen Bengel and Rieka von der Warth declare that they have no competing interests.
References
1. Linden M. Psychosomatic inpatient rehabilitation: the German model. Psychother Psychosom. 2014;83(4):205–212. doi:10.1159/000358852
2. Weltgesundheitsorganisation. International Classification of Functioning, Disability and Health. ICF; 2005.
3. Maes S, Karoly P. Self-regulation assessment and intervention in physical health and illness: a review. Appl Psychol. 2005;54(2):267–299. doi:10.1111/j.1464-0597.2005.00210.x
4. Steffanowski A, Löschmann C, Schmidt J, Wittmann WW, Nübling R. Meta-Analyse der Effekte Stationärer Psychosomatischer Rehabilitation (Mesta-Studie) [Meta-Analysis of the Effects of Inpatient Psychosomatic Rehabilitation (Mesta Study)]. Huber; 2007.
5. Reuter L, Bengel J, Scheidt CE. Therapie-Non-Response in der psychosomatischen Krankenhausbehandlung und Rehabilitation – eine systematische Übersicht [Nonresponse to therapy in acute and rehabilitative psychosomatic inpatient care – a systematic review]. Zeitschrift für Psychosomatische Medizin und Psychotherapie. 2014;60(2):121–145. doi:10.13109/zptm.2014.60.2.121
6. Widera T. Aktuelles Aus der Reha-Qualitätssicherung - Neue Ergebnisse der Rehabilitandenbefragung [Current News from Rehabilitation Quality Assurance - New Results of the Rehabilitation Patient Survey]. RVaktuell: Deutsche Rentenversicherung; 2010:153–159.
7. Kriz D, Nübling R, Steffanowski A, Wittmann W, Juergen S. Patientenzufriedenheit in der stationären Rehabilitation: psychometrische Reanalyse des ZUF-8 auf der Basis multizentrischer Stichproben verschiedener Indikation [Patients’ satisfaction in inpatient rehabilitation. Psychometrical evaluation of the ZUF-8 based on a multicenter sample of different indications]. Zeitschrift für Medizinische Psychologie. 2008;17(2–3):67–79.
8. French DP, Cooper A, Weinman J. Illness perceptions predict attendance at cardiac rehabilitation following acute myocardial infarction: a systematic review with meta-analysis. J Psychosom Res. 2006;61(6):757–767. doi:10.1016/j.jpsychores.2006.07.029
9. Glattacker M, Giesler JM, Klindtworth K, Nebe A. Rehabilitation use in multiple sclerosis: do illness representations matter? Brain Behav. 2018;8(6):e00953. doi:10.1002/brb3.953
10. Glattacker M, Opitz U, Jäckel WH. Illness representations in women with fibromyalgia. Br J Health Psychol. 2010;15(2):367–387. doi:10.1348/135910709X466315
11. Glattacker M, Heyduck K, Meffert C. Illness beliefs and treatment beliefs as predictors of short-term and medium-term outcome in chronic back pain. J Rehabilit Med. 2013;45(3):268–276. doi:10.2340/16501977-1104
12. Cannon M, Credé M, Kimber JM, Brunkow A, Nelson R, McAndrew LM. The common-sense model and mental illness outcomes: a meta-analysis. Clin Psychol Psychother. 2022;29(4):1186–1202. doi:10.1002/cpp.2721
13. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143(11):1117–1154. doi:10.1037/bul0000118
14. Hagger MS, Orbell S. A meta-analytic review of the common-sense model of illness representations. Psychol Health. 2003;18(2):141–184. doi:10.1080/088704403100081321
15. Richter M, Schmid-Ott G, Muthny FA. Patientenzufriedenheit in der psychosomatischen Rehabilitation [Patient satisfaction in psychosomatic rehabilitation]. Nervenheilkunde. 2010;29(06):386–392. doi:10.1055/s-0038-1628782
16. Richter M, Schmid-Ott G, Muthny FA. Informationsvermittlung und Partizipation aus Sicht von psychosomatischen Rehabilitanden [Information and participation of patients in psychosomatic rehabilitation occurrence and relations to patient satisfaction treatment outcome]. Psychiatr Prax. 2011;38(05):237–243. doi:10.1055/s-0030-1266068
17. Richter M, Schmid-Ott G, Muthny FA. Subjektive Anforderungen an die psychosomatische Rehabilitation und ihr Einfluss auf die Patientenzufriedenheit – „Basis-, Leistungs- und Begeisterungsfaktoren” nach dem Kano-Modell [Subjective Requirements for Psychosomatic Rehabilitation and their Influence on Patient Satisfaction – “Basic, Performance and Excitement Factors” According to Kano]. Das Gesundheitswesen. 2011;73(3):169–176. doi:10.1055/s-0030-1249645
18. Sitzia J, Wood N. Patient satisfaction: a review of issues and concepts. Soc Sci Med. 1997;45(12):1829–1843. doi:10.1016/s0277-9536(97)00128-7
19. Jackson JL, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52(4):609–620. doi:10.1016/s0277-9536(00)00164-7
20. Priebe S, Miglietta E. Assessment and determinants of patient satisfaction with mental health care. World Psychiatry. 2019;18(1):30–31. doi:10.1002/wps.20586
21. Hafkamp FJ, Gosens T, de Vries J, den Oudsten BL. Do dissatisfied patients have unrealistic expectations? A systematic review and best-evidence synthesis in knee and Hip arthroplasty patients. EFORT Open Rev. 2020;5(4):226–240. doi:10.1302/2058-5241.5.190015
22. Palazzo C, Jourdan C, Descamps S, et al. Determinants of satisfaction 1 year after total Hip arthroplasty: the role of expectations fulfilment. BMC Musculoskelet Disord. 2014;15(1):53. doi:10.1186/1471-2474-15-53
23. Woodward S, Berry K, Bucci S. A systematic review of factors associated with service user satisfaction with psychiatric inpatient services. J Psychiatr Res. 2017;92:81–93. doi:10.1016/j.jpsychires.2017.03.020
24. Hagger MS, Orbell S. The common sense model of illness self-regulation: a conceptual review and proposed extended model. Health Psychol Rev. 2021. doi:10.1080/17437199.2021.1878050
25. Leventhal H, Leventahl EA, Cameron LD. Representations, procedures, and affect in illness self-regulation: a perceptual-cognitive model. In: Baum A, Revenson TA, Singer JE, editors. Handbook of Health Psychology. Lawrence Erlbaum; 2001:19–48.
26. Horne R. Patients’ beliefs about treatment: the hidden determinant of treatment outcome? J Psychosom Res. 1999;47(6):491–495. doi:10.1016/S0022-3999(99)00058-6
27. Cameron LD, Leventhal H. Self-regulation, health, and illness. An overview. In: Cameron LD, Leventhal H, editors. The Self-Regulation of Health and Illness Behaviour. Routledge; 2003:1–13.
28. Kube T, D’Astolfo L, Glombiewski JA, Doering BK, Rief W. Focusing on situation-specific expectations in major depression as basis for behavioural experiments – development of the depressive expectations scale. Psychol Psychother. 2017;90(3):336–352. doi:10.1111/papt.12114
29. von der Warth R, Nau A, Rudolph M, Stapel M, Bengel J, Glattacker M. Treatment beliefs in patients with mental disorders in psychosomatic rehabilitation - a qualitative analysis. Eur J Health Psychol. 2022;29(2):107–117. doi:10.1027/2512-8442/a000087
30. Greenberg RP, Constantino MJ, Bruce N. Are patient expectations still relevant for psychotherapy process and outcome? Clin Psychol Rev. 2006;26(6):657–678. doi:10.1016/j.cpr.2005.03.002
31. Schmidt J, Lamprecht F, Wittmann WW. Zufriedenheit mit der stationären Versorgung. Entwicklung eines Fragebogens und erste Validitätsuntersuchungen. [Satisfaction with inpatient care: development of a questionnaire and first validity assessments.]. Psychother Psychosom Med Psychol. 1989;39(7):248–255.
32. Attkisson CC, Zwick R. The client satisfaction questionnaire: psychometric properties and correlations with service utilization and psychotherapy outcome. Eval Program Plann. 1982;5(3):233–237. doi:10.1016/0149-7189(82)90074-X
33. Gaab J, Bunschoten SL, Sprott H, Ehler U. Psychometric evaluation of a German translation of the illness perception questionnaire.
34. Moss-Morris R, Weinman J, Horne R, Cameron LD, Buick D, Buick D. The Revised Illness Perception Questionnaire (IPQ-R). Psychol Health. 2002;17:1–16. doi:10.1080/08870440290001494
35. Glattacker M, Bengel J, Jäckel WH. Die deutschsprachige version des Illness Perception Questionnaire-Revised: psychometrische evaluation an patienten mit chronisch somatischen erkrankungen [German version of the Illness Perception Questionnaire-Revised (IPQ-R): psychometric evaluation in patients with chronic somatic illness]. Zeitschrift für Gesundheitspsychologie. 2009;17(4):158–169. doi:10.1026/0943-8149.17.4.158
36. Nau A, Metzner G, von der Warth R, et al. Psychometric properties of a questionnaire of beliefs about psychosomatic rehabilitation; n.d.
37. Rabung S, Harfst T, Koch U, Wittchen H-U, Schulz H. “Hamburger Module zur Erfassung allgemeiner Aspekte psychosozialer Gesundheit für die therapeutische Praxis (HEALTH)”-psychometrische Überprüfung eines neuen Selbstbeurteilungsinstruments zur multidimensionalen Erfassung psychosozialer Gesundheit. Physikalische Medizin, Rehabilitationsmedizin, Kurortmedizin. 2007;17(03):133–140. doi:10.1055/s-2007-940198
38. SPSS IBM. Statistics for Windows. Version 27.0. IBM Corp; 2020.
39. Glattacker M, Heyduck K, Meffert C, Jakob T. Illness beliefs, treatment beliefs and information needs as starting points for patient information: the evaluation of an intervention for patients with depression. J Clin Psychol Med Settings. 2018;25(3):316–333. doi:10.1007/s10880-018-9551-1
40. Glattacker M, Heyduck K, Meffert C. Illness beliefs and treatment beliefs as predictors of short and middle term outcome in depression. J Health Psychol. 2013;18(1):139–152. doi:10.1177/1359105311433907
41. von der Warth R, Nau A, Rudolph M, Bengel J, Glattacker M. Illness and treatment beliefs as predictors of rehabilitation outcome in patients with mental disorders. J Psychosom Res. 2022;155:110750. doi:10.1016/j.jpsychores.2022.110750
42. McAndrew LM, Crede M, Maestro K, Slotkin S, Kimber J, Phillips LA. Using the common-sense model to understand health outcomes for medically unexplained symptoms: a meta-analysis. Health Psychol Rev. 2019;13(4):427–446. doi:10.1080/17437199.2018.1521730
43. Auer CJ, Glombiewski JA, Doering BK, et al. Patients’ expectations predict surgery outcomes: a meta-analysis. Int J Behav Med. 2016;23(1):49–62. doi:10.1007/s12529-015-9500-4
44. Kube T, Glombiewski JA, Rief W. Using different expectation mechanisms to optimize treatment of patients with medical conditions: a systematic review. Psychosom Med. 2018;80(6):535–543. doi:10.1097/psy.0000000000000596
45. Rief W, Shedden-Mora MC, Laferton JA, et al. Preoperative optimization of patient expectations improves long-term outcome in heart surgery patients: results of the randomized controlled PSY-HEART trial. BMC Med. 2017;15(1):4. doi:10.1186/s12916-016-0767-3
46. Rief W, Glombiewski JA. Erwartungsfokussierte Psychotherapeutische Interventionen (EFPI) [Expectation-Focused Psychotherapeutic Interventions (EFPI)]. Verhaltenstherapie. 2016;26(1):47–54. doi:10.1159/000442374
47. Barrett MS, Chua W-J, Crits-Christoph P, Gibbons MB, Casiano D, Thompson D. Early withdrawal from mental health treatment: implications for psychotherapy practice. Psychotherapy. 2008;45(2):247–267. doi:10.1037/0033-3204.45.2.247
48. Constantino MJ, Vîslă A, Coyne AE, Boswell JF. A meta-analysis of the association between patients’ early treatment outcome expectation and their posttreatment outcomes. Psychotherapy. 2018;55(4):473–485. doi:10.1037/pst0000169
49. Kästner A, Ng Kuet Leong VSC, Petzke F, et al. The virtue of optimistic realism - expectation fulfillment predicts patient-rated global effectiveness of total Hip arthroplasty. BMC Musculoskelet Disord. 2021;22(1):180. doi:10.1186/s12891-021-04040-y
50. Gill L, White L. A critical review of patient satisfaction. Leader Health Serv. 2009;22(1):8–19. doi:10.1108/17511870910927994
51. Ware JE, Snyder MK, Wright WR, Davies AR. Defining and measuring patient satisfaction with medical care. Eval Program Plann. 1983;6(3–4):247–263. doi:10.1016/0149-7189(83)90005-8
52. Georgy EE, Carr EC, Breen AC. Met or matched expectations: what accounts for a successful back pain consultation in primary care? Health Expect. 2013;16(2):143–154. doi:10.1111/j.1369-7625.2011.00706.x
53. Rief W, Glombiewski JA, Gollwitzer M, Schubö A, Schwarting R, Thorwart A. Expectancies as core features of mental disorders. Curr Opin Psychiatry. 2015;28(5):378–385. doi:10.1097/yco.0000000000000184
54. Rief W, Joormann J. Revisiting the cognitive model of depression: the role of expectations. Clin Psychol Europe. 2019;1(1):1–19. doi:10.32872/cpe.v1i1.32605
55. Glattacker M, Heyduck K, Meffert C. Illness beliefs, treatment beliefs and information needs as starting points for patient information--evaluation of an intervention for patients with chronic back pain. Patient Educ Couns. 2012;86(3):378–389. doi:10.1016/j.pec.2011.05.028
56. Broadbent E, Ellis CJ, Thomas J, Gamble G, Petrie KJ. Further development of an illness perception intervention for myocardial infarction patients: a randomized controlled trial. J Psychosom Res. 2009;67(1):17–23. doi:10.1016/j.jpsychores.2008.12.001
57. de Ridder DT, Theunissen NC, van Dulmen SM. Does training general practitioners to elicit patients’ illness representations and action plans influence their communication as a whole? Patient Educ Couns. 2007;66(3):327–336. doi:10.1016/j.pec.2007.01.006
58. Goulding L, Furze G, Birks Y. Randomized controlled trials of interventions to change maladaptive illness beliefs in people with coronary heart disease: systematic review. J Adv Nurs. 2010;66(5):946–961. doi:10.1111/j.1365-2648.2010.05306.x
59. Jones CJ, Smith HE, Llewellyn CD. A systematic review of the effectiveness of interventions using the Common Sense Self-Regulatory Model to improve adherence behaviours. J Health Psychol. 2015;21(11):2709–2724. doi:10.1177/1359105315583372
60. Petrie KJ, Cameron LD, Ellis CJ, Buick D, Weinman J. Changing illness perceptions after myocardial infarction: an early intervention randomized controlled trial. Psychosom Med. 2002;64(4):580–586. doi:10.1097/00006842-200207000-00007
61. Petrie KJ, Perry K, Broadbent E, Weinman J. A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication. Br J Health Psychol. 2012;17(1):74–84. doi:10.1111/j.2044-8287.2011.02033.x
62. Phillips LA, Leventhal H, Leventhal EA. Physicians’ communication of the common-sense self-regulation model results in greater reported adherence than physicians’ use of interpersonal skills. Br J Health Psychol. 2012;17(2):244–257. doi:10.1111/j.2044-8287.2011.02035.x
63. Harrell FEJ. Regression Modeling Strategies. Springer Series in Statistics. Springer; 2015.
64. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. doi:10.1007/s10865-016-9782-2
65. Yardley L, Sharples K, Beech S, Lewith G. Developing a dynamic model of treatment perceptions. J Health Psychol. 2001;6(3):269–282. doi:10.1177/135910530100600301
66. DeLongis A, Morstead T, Kouvousis C, Ray CM, Wyrough A, Rhodes RE. Bringing the social context into research using the common sense model. Health Psychol Rev. 2019;13:1–3. doi:10.1080/17437199.2019.1652107
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.