Back to Journals » OncoTargets and Therapy » Volume 8
IL-2 -330T/G polymorphism and cancer risk: a meta-analysis
Received 6 April 2015
Accepted for publication 14 May 2015
Published 17 July 2015 Volume 2015:8 Pages 1753—1760
DOI https://doi.org/10.2147/OTT.S86136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Daniele Santini
Hongyu Zhao,1,* Rui Wang2,*
1Central Laboratory, The Second Affiliated Hospital of Southeast University, Nanjing, 2Nanjing Kingmed Clinical Laboratory Co., Ltd, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work and share the first authorship
Purpose: Some studies have investigated the association of IL-2 -330T/G (rs2069762) polymorphism with cancer risk, but the previous results were conflicting and had relatively low statistical power. Thus, we performed a meta-analysis to derive a more precise estimation of the association between IL-2 -330T/G polymorphism and cancer risk.
Methods: A literature search was performed systematically using electronic databases. The odds ratio (OR) with 95% confidence interval (CI) was used to estimate the pooled effect.
Results: A total of ten studies including 3,060 cases and 3,435 controls were involved in this meta-analysis. The results indicated that IL-2 -330T/G polymorphism was significantly associated with cancer risk ([OR =2.03, 95% CI =1.40–2.95] for GG vs TT; [OR =1.37, 95% CI =1.11–1.69] for GT vs TT; [OR =1.46, 95% CI =1.18–1.81] for [GG + GT] vs TT; [OR =1.66, 95% CI =1.24–2.23] for GG vs [GT + TT]; and [OR =1.35, 95% CI =1.16–1.57] for G vs T). In the subgroup analysis according to cancer type, significant association was found in lymphoma ([OR =1.46, 95% CI =1.11–1.91] for GT vs TT; [OR =1.58, 95% CI =1.22–2.05] for [GG + GT] vs TT; [OR =1.84, 95% CI =1.22–2.77] for GG vs [GT + TT]) and other cancers, but not in gastric cancer. In the subgroup analysis by ethnicity, the significant risk was found among Asians, but not among Europeans.
Conclusion: This meta-analysis suggests that IL-2 -330T/G polymorphism has an increased risk of cancer in Asians. However, further detailed studies are still required to confirm our findings.
Keywords: IL-2, polymorphism, cancer, risk, meta-analysis
Introduction
Cancer is a major public health problem and one of the leading causes of death around the world. According to the estimation of GLOBOCAN, approximately 12.7 million new cases and 7.6 million deaths of cancer had occurred in 2008.1 Although the pathogenesis of cancer is complex and has not been fully understood, recent studies suggest that genetic factors play critical roles in the pathogenic process of cancer, such as variants in Interleukin-2 (IL-2) gene.
IL-2 is an important immunoregulatory cytokine produced primarily by activated CD4+ T-cells, naïve CD8+ T-cells and dendritic cells.2 It has been reported that IL-2 can stimulate proliferation and differentiation of natural killer cells,3 and promote production of natural killer-derived cytokines such as TNFα, IFNγ and GM-CSF. IL-2-induced proliferation occurs via pro-proliferative signals through the proto-oncogenes c-Fos and c-Myc, in combination with anti-apoptotic signals through Bcl-2 family members.4 In addition, it can also enhance activation-induced cell death in T-lymphocytes and eliminate self-reactive cells.5 The role of IL-2 in B cells has also been identified, mostly pertaining to antibody secretion. In IgM-expressing B cells, IL-2 and IL-5 act synergistically to upregulate expression of heavy and light chain genes as well as inducing de novo synthesis of the immunoglobulin J chain gene.6 The latter is required for oligomerization of the IgM pentamer, and represents a tightly controlled stage in B cell activation.7 Thus, IL-2 has broad essential biological actions, and its dysfunction may have an negative influence on the development of cancer. Human IL-2 gene is located on chromosome 4q26, and in the promoter region, single nucleotide polymorphism -330T/G (rs2069762) has been reported to affect IL-2 production.8 Some studies have investigated the potential association of IL-2 -330T/G polymorphism and cancer risk.9–18 However, the previous results were conflicting and had relatively low statistical power. Considering the important role of IL-2 in tumorigenesis, we performed a meta-analysis on all eligible studies to estimate the overall cancer risk associated with the IL-2 -330T/G polymorphism.
Methods
Literature search strategy
A literature search of the PubMed, Embase, Chinese National Knowledge Infrastructure and Wang Fang databases was carried out (updated up to March 30, 2015) using the following MeSH terms: “polymorphism or variant”, “cancer or tumor” and “IL-2 or Interleukin-2”. We also manually searched the reference lists of all eligible studies and review articles in order to obtain additional usable data that can be included in the current meta-analysis. All articles were written in English or in Chinese.
Inclusion and exclusion criteria
We selected eligible studies according to the following criteria: a) case–control studies; b) investigating the association between the IL-2 -330T/G polymorphism and cancer risk; and c) detailed genotype data for estimating of odds ratio (OR) and 95% confidence interval (CI). Exclusion criteria were the following: a) insufficient information on the distribution of IL-2 -330T/G genotypes; b) case-only studies; and c) duplicated publications. If multiple studies had overlapping or duplicate data, only those with complete data were included.
Quality assessment of eligible studies
Two investigators independently assessed the quality of eligible studies according to the modified STROBE quality checklist. Forty assessment items that related to quality appraisal were used in this meta-analysis with scores ranging from 0 to 40. On the basis of their scores, these eligible studies were classified into three levels: low quality (0–19), moderate quality (20–29), and high quality (30–40). Disagreements were resolved through discussion.
Data extraction
Two independent investigators extracted the data in standardized data-collection forms. The following data were collected from each study: first author name, year of publication, cancer type, country, ethnicity, and genotype distribution of cases and controls. Disputes were settled by discussion.
Statistical analysis
The Hardy–Weinberg equilibrium (HWE) was utilized to compare the observed genotype frequencies with expected genotype frequencies in controls. Crude ORs with 95% CIs were calculated to evaluate the strength of the association between IL-2 -330T/G polymorphism and cancer risk. The pooled ORs were performed for additive model (G vs T), dominant model ([GG + GT] vs TT), recessive model (GG vs [GT + TT]) and codominant model (GG vs TT, GT vs TT). Subgroup analysis by cancer type, ethnicity and PHWE was also performed to further assess if the IL-2 -330T/G polymorphism was associated with cancer susceptibility in each subgroup. A statistical test for heterogeneity was performed based on the Q statistic. If PH<0.05 for Q-test suggested significant heterogeneity, then the random-effects model was conducted to calculate the pooled OR; otherwise, the fixed-effects model was selected. Sensitivity analysis was performed by omitting each study in turn to assess the quality and consistency of the results. Begg’s funnel plot and the Egger’s test were used to evaluate possible publication bias of literatures. All statistical tests were performed by using STATA 12.0 software (Stata Corporation, College Station, TX, USA). All the P-values <0.05 were considered statistically significant.
Results
The flow chart of article selection was presented in Figure 1. A total of 94 literatures were identified through PubMed, Embase, Chinese National Knowledge Infrastructure, and Wang Fang databases. After reviewing the titles and abstracts of the potential available articles, 76 records were excluded mainly because they were of no relevance, were in vitro experiments or were reviews. From the remaining 18 articles, we eliminated five publications due to their nonrelation with IL-2 -330T/G polymorphism, and three publications due to their insufficient genotype data. Finally, ten articles, including ten studies with 3,060 cases and 3,435 controls, were included in this meta-analysis.
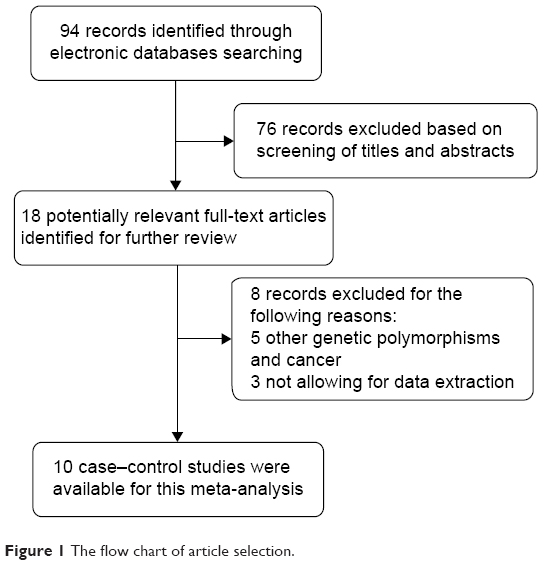 | Figure 1 The flow chart of article selection. |
The main characteristics of eligible studies are listed in Table 1. All quality scores of eligible studies were more than 20 (moderate-high quality). The types of cancers studied included breast cancer,9 lymphoma,10,11 bladder cancer,12 nasopharyngeal carcinoma,13 gastroenteropancreatic neuroendocrine tumors,14 gastric cancer,15,16 chronic myelogenous leukemia,17 and cutaneous malignant melanoma.18 In addition, the populations of the studies included Asians and Europeans. After calculating PHWE in controls, we found that four studies were in agreement with HWE (PHWE≥0.05), and six studies are a deviation from the HWE (PHWE<0.05). Data concerning different cancer types, different populations, and different PHWE status were treated as separate studies in the subgroup analysis.
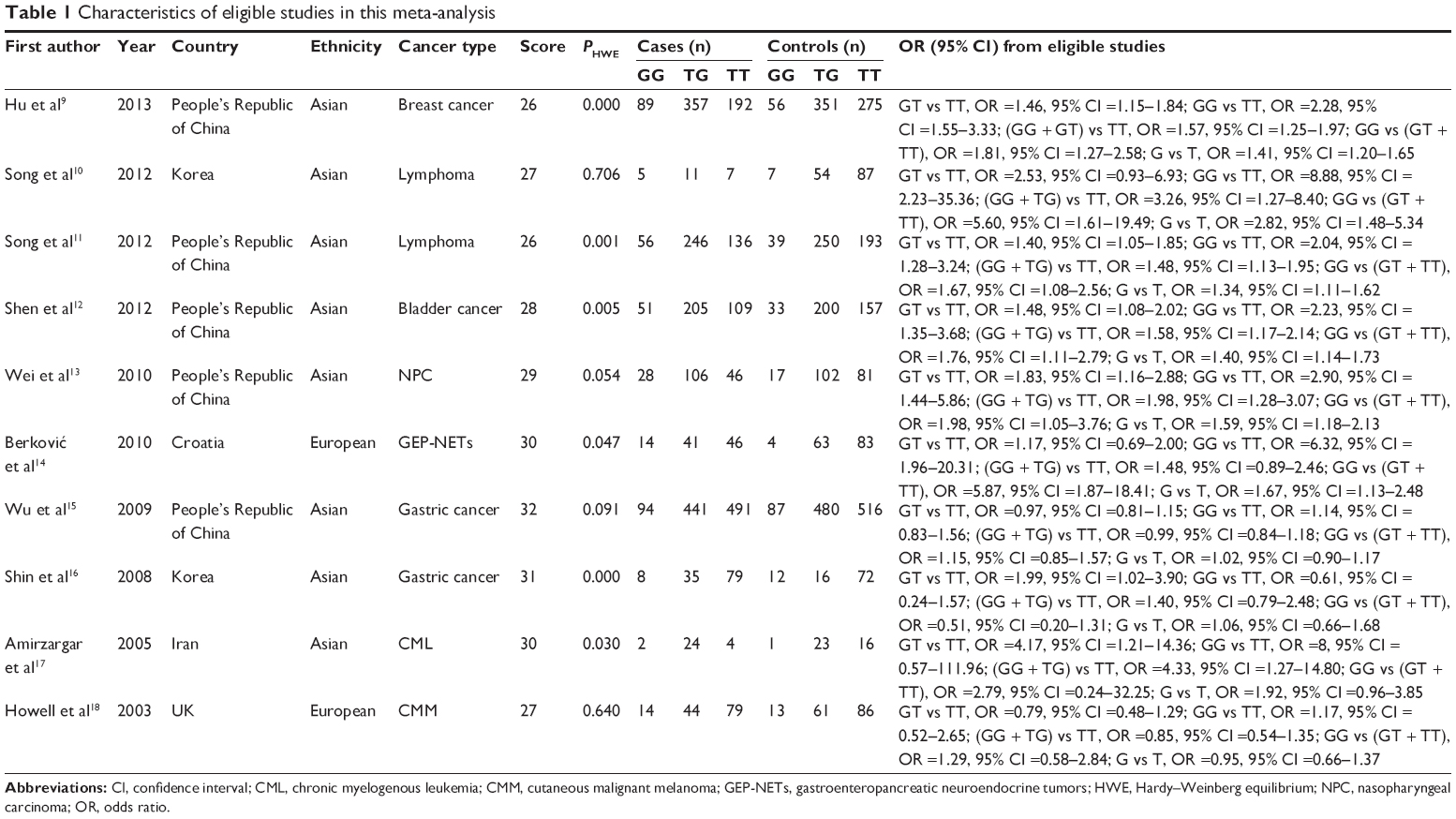 | Table 1 Characteristics of eligible studies in this meta-analysis |
The evaluations of the association of IL-2 -330T/G polymorphism with cancer risk are shown in Table 2 and Figure 2. Overall, IL-2 -330T/G polymorphism was significantly associated with overall cancer risk ([OR =2.03, 95% CI =1.40–2.95] for GG vs TT; [OR =1.37, 95% CI =1.11–1.69] for GT vs TT; [OR =1.46, 95% CI =1.18–1.81] for [GG + GT] vs TT; [OR =1.66, 95% CI =1.24–2.23] for GG vs [GT + TT]; and [OR =1.35, 95% CI =1.16–1.57] for G vs T). In the stratified analysis by cancer types, we found that IL-2 -330T/G polymorphism was significantly associated with the risk of lymphoma ([OR =1.46, 95% CI =1.11–1.91] for GT vs TT; [OR =1.58 95% CI =1.22–2.05] for [GG + GT] vs TT; [OR =1.84, 95% CI =1.22–2.77] for GG vs [GT + TT]) and other cancer ([OR =2.34, 95% CI =1.81–3.02] for GG vs TT; [OR =1.41 95% CI =1.21–1.65] for GT vs TT; [OR =1.53 95% CI =1.32–1.78] for [GG + GT] vs TT; [OR =1.88, 95% CI =1.49–2.39] for GG vs [GT + TT]; [OR =1.41, 95% CI =1.27–1.56] for G vs T), but not of gastric cancer. In addition, subgroup analyses were performed by ethnicity. Significantly increased cancer risks were found among Asians ([OR =1.97, 95% CI =1.33–2.93] for GG vs TT; [OR =1.49, 95% CI =1.18–1.87] for GT vs TT; [OR = 1.56, 95% CI =1.22–1.98] for [GG + GT] vs TT; [OR =1.58, 95% CI =1.18–2.11] for GG vs [GT + TT]; and [OR =1.37, 95% CI =1.16–1.61] for G vs T), but not among Europeans. Stratified analyses by PHWE showed that IL-2 -330T/G polymorphism was associated with cancer risk in both PHWE<0.05 ([OR =2.13, 95% CI =1.69–2.70] for GG vs TT; [OR =1.47, 95% CI =1.27–1.70] for GT vs TT; [OR =1.56, 95% CI =1.35–1.79] for [GG + GT] vs TT; [OR =1.73, 95% CI =1.39–2.15 for GG vs [GT + TT]; and [OR =1.39, 95% CI =1.26–1.54] for G vs T) and PHWE≥0.05 ([OR =1.34, 95% CI =1.04–1.73] for GG vs [GT + TT]).
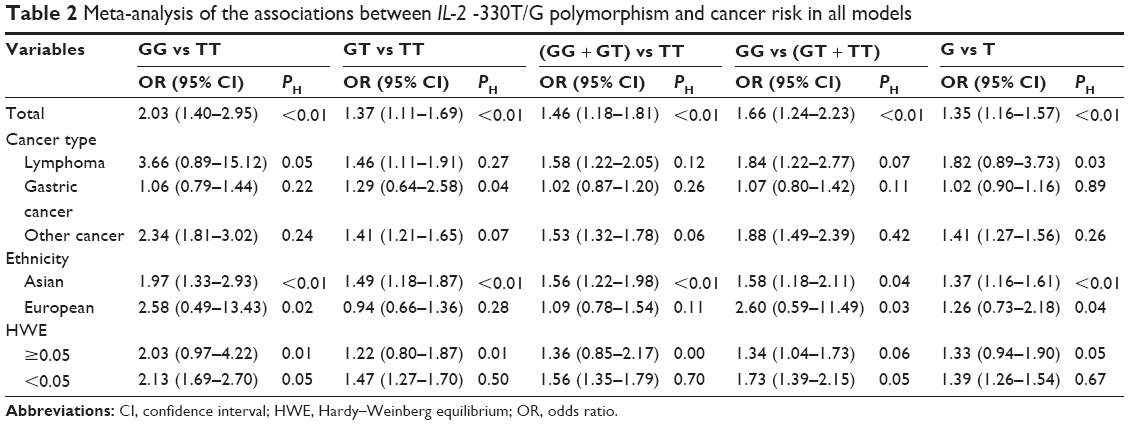 | Table 2 Meta-analysis of the associations between IL-2 -330T/G polymorphism and cancer risk in all models |
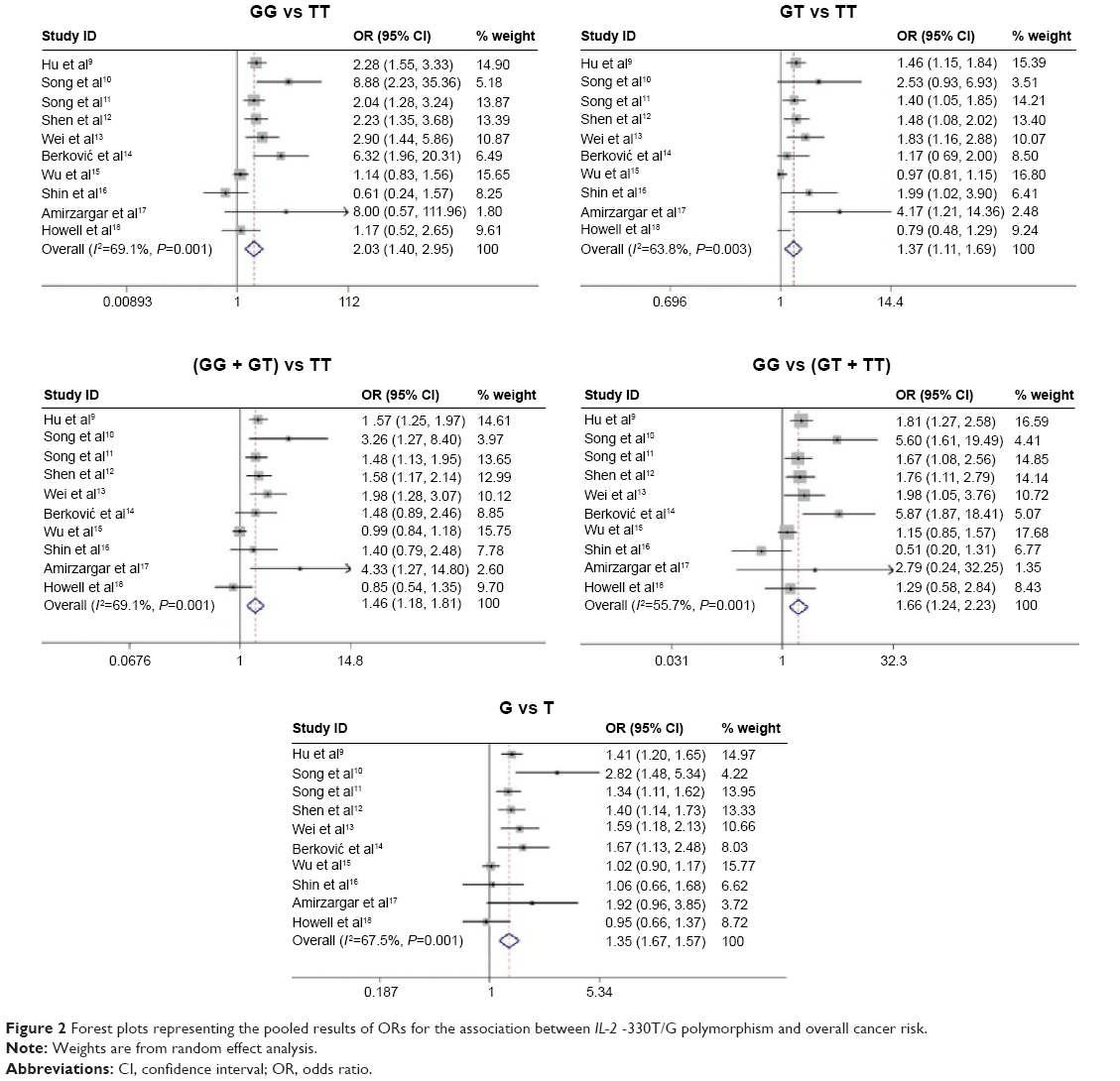 | Figure 2 Forest plots representing the pooled results of ORs for the association between IL-2 -330T/G polymorphism and overall cancer risk. |
As shown in Figure 3, sensitivity analysis indicated that current results were stable and credible. Publication bias was assessed by Begg’s funnel plot and Egger’s test. The shape of the Begg’s funnel plots seemed symmetrical in all genetic models, suggesting the absence of publication bias (Figure 4). Then, the Egger’s test was performed to provide statistical evidence of funnel plots symmetry. The results also indicated a lack of publication bias of the current meta-analysis (P=0.14 for GG vs TT; P=0.08 for GT vs TT; P=0.07 for [GG + GT] vs TT; P=0.17 for GG vs [GT + TT]; and P=0.11 for G vs T).
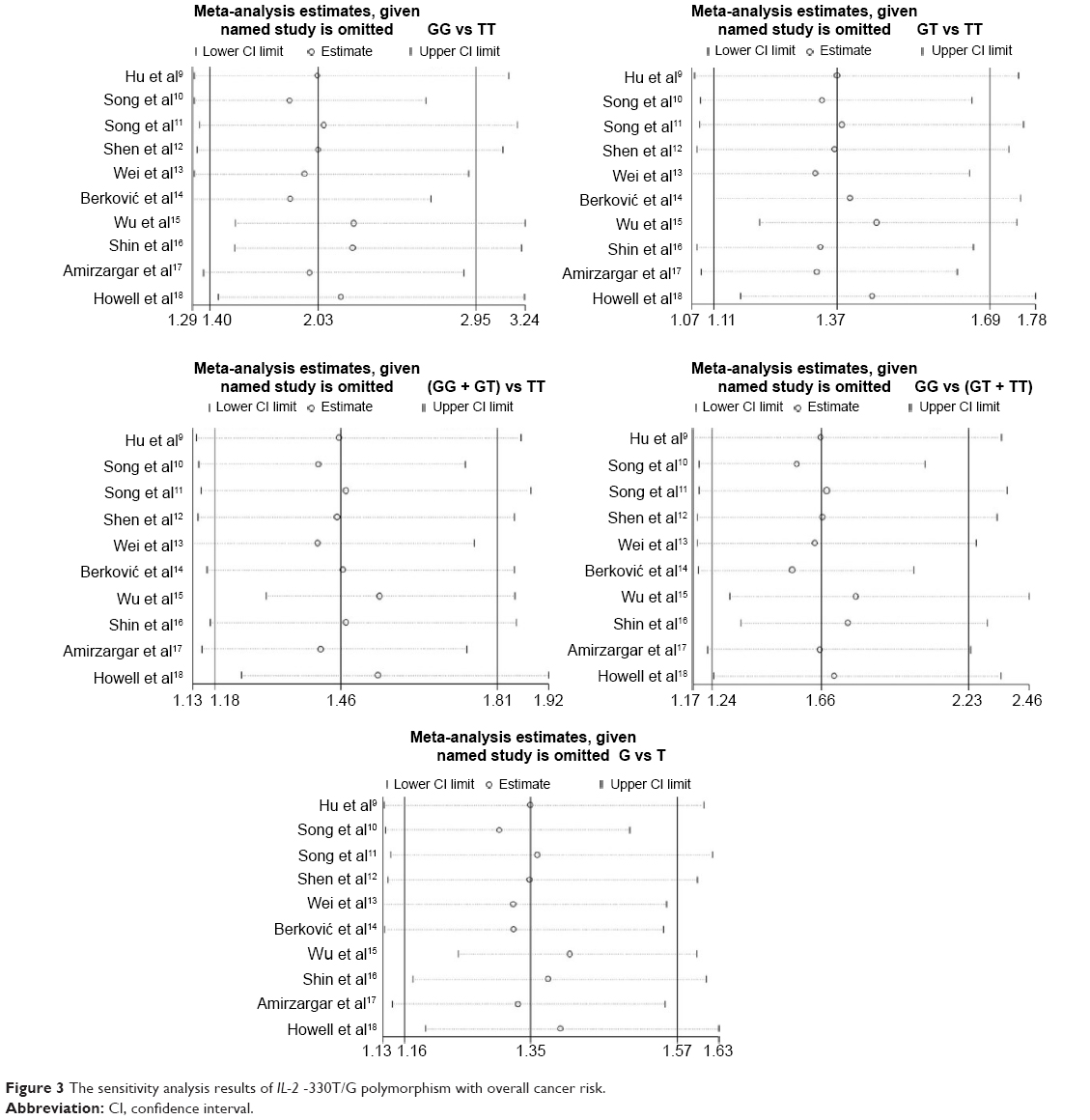 | Figure 3 The sensitivity analysis results of IL-2 -330T/G polymorphism with overall cancer risk. |
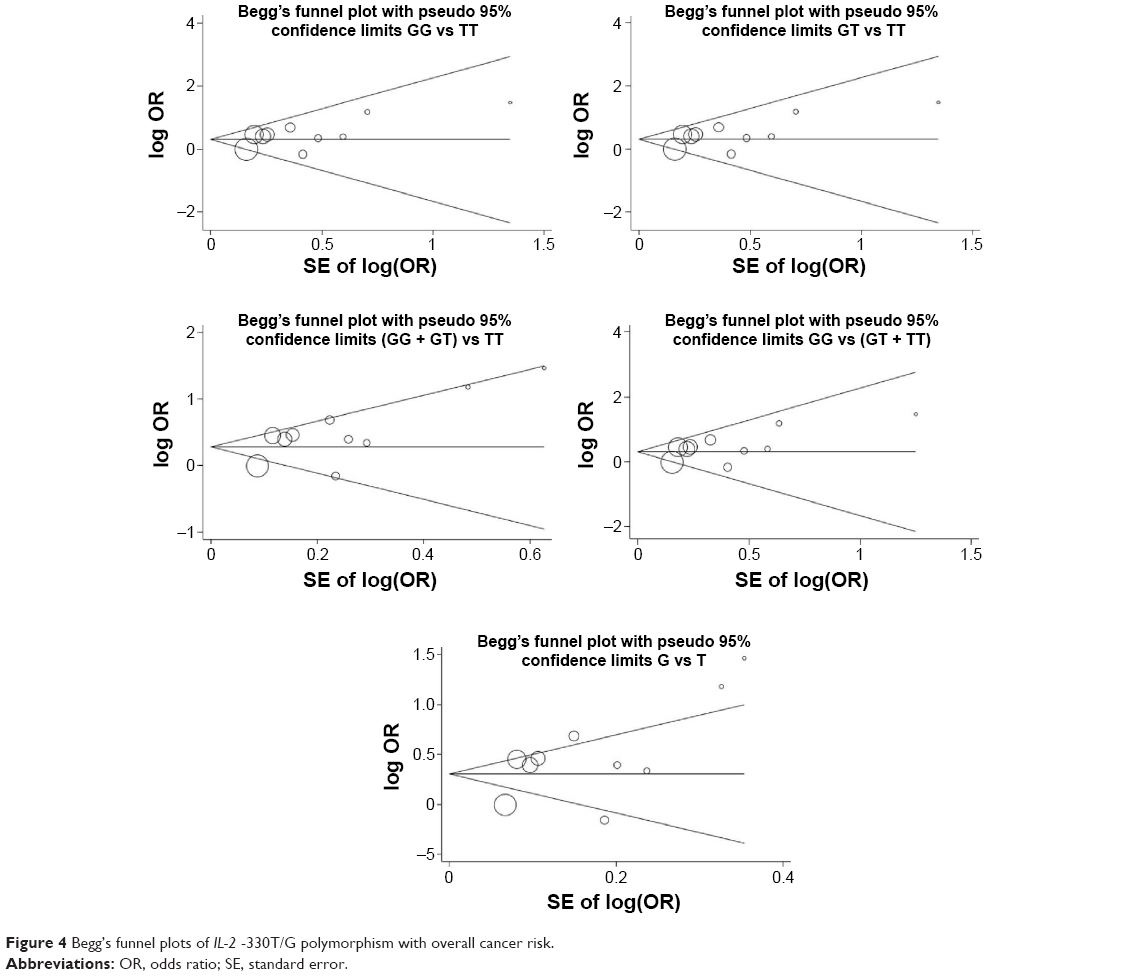 | Figure 4 Begg’s funnel plots of IL-2 -330T/G polymorphism with overall cancer risk. |
Discussion
Some studies showed that IL-2 -330T/G polymorphism was associated with the risk of cancer, including nasopharyngeal carcinoma, gastric cardia cancer, lymphoma, non-Hodgkin lymphoma, bladder cancer, breast cancer, and gastroenteropancreatic neuroendocrine tumor.9–15 However, other studies indicated that IL-2 -330T/G polymorphism was not associated with cancer risk, such as gastric cancer and cutaneous malignant melanoma.16,18 Meta-analysis has been recognized as an important way to detect the effect of selected genetic polymorphisms on disease risk precisely.19 To the best of our knowledge, the current study was the first meta-analysis providing comprehensive insights into the association of IL-2 -330T/G polymorphism with cancer risk. Our results indicated that IL-2 -330T/G polymorphism might contribute to the development of cancer. Subgroup analysis by cancer type demonstrated an increased risk of lymphoma strongly associated with IL-2 -330T/G polymorphism. Conversely, the relationship of gastric cancer with IL-2 -330T/G polymorphism turned out to be non-significant. In addition, we conducted stratified analyses based on ethnicity and found a significant association in Asian, but not in European populations. This might reflect the fact that the development of cancer was associated with different genetic background in different ethnicities. Stratified analyses by PHWE showed significant association in both PHWE<0.05 and PHWE≥0.05, indicating that PHWE status did not affect the relationship of IL-2 -330T/G polymorphism with cancer risk.
Despite our great efforts to examine the association between IL-2 -330T/G polymorphism and cancer risk, some limitations should be considered. First, lack of the original data of included studies limited our precise evaluation of the association, which might cause information bias. Second, the included studies for subgroup analyses were limited. For example, there were only two studies included in the analysis of European population, which might limit our precise evaluation of risk factor. Third, our analysis did not consider the possibility of gene-environment interactions or the possibility of linkage disequilibrium between gene polymorphisms.
Conclusion
Our meta-analysis suggested that IL-2 -330T/G polymorphism was a potentially risk factor for the development of cancer in Asian populations. However, due to the limitations mentioned above, further detailed studies are still required to confirm our findings.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | ||
Nelson BH. IL-2, regulatory T cells, and tolerance. J Immunol. 2004;172(7):3983–3988. | ||
Abbas KA. Cellular and Molecular Immunology. 5th ed. Philadelphia, PA: Saunders Elsevier; 2005. | ||
Miyazaki T, Liu ZJ, Kawahara A, et al. Three distinct IL-2 signaling pathways mediated by bcl-2, c-myc, and lck cooperate in hematopoietic cell proliferation. Cell. 1995;81(2):223–231. | ||
Wang R, Ciardelli TL, Russell JH. Partial signaling by cytokines: cytokine regulation of cell cycle and Fas-dependent, activation-induced death in CD4+ subsets. Cell Immunol. 1997;182(2):152–160. | ||
Blackman MA, Tigges MA, Minie ME, Koshland ME. A model system for peptide hormone action in differentiation: interleukin 2 induces a B lymphoma to transcribe the J chain gene. Cell. 1986;47(4):609–617. | ||
Koshland ME. The coming of age of the immunoglobulin J chain. Annu Rev Immunol. 1985;3:425–453. | ||
Hoffmann SC, Stanley EM, Darrin Cox E, et al. Association of cytokine polymorphic inheritance and in vitro cytokine production in anti-CD3/ CD28-stimulated peripheral blood lymphocytes. Transplantation. 2001;72(8):1444–1450. | ||
Hu XB, Ouyang LZ, Tang LL. Interleukin-2 gene polymorphisms and prognosis of breast cancer. Genet Test Mol Biomarkers. 2013;17(6):453–457. | ||
Song N, Han S, Lee KM, et al. Genetic variants in interleukin-2 and risk of lymphoma among children in Korea. Asian Pac J Cancer Prev. 2012;13(2):621–623. | ||
Song H, Chen L, Cha Z, et al. Interleukin 2 gene polymorphisms are associated with non-Hodgkin lymphoma. DNA Cell Biol. 2012;31(7):1279–1284. | ||
Shen Y, Liu Y, Liu S, et al. The association between -330T/G polymorphism of interleukin 2 gene and bladder cancer. DNA Cell Biol. 2012;31(6):983–987. | ||
Wei YS, Lan Y, Zhang L, et al. Association of the interleukin-2 polymorphisms with interleukin-2 serum levels and risk of nasopharyngeal carcinoma. DNA Cell Biol. 2010;29(7):363–368. | ||
Berković MC, Jokić M, Marout J, et al. IL-2 -330 T/G SNP and serum values – potential new tumor markers in neuroendocrine tumors of the gastrointestinal tract and pancreas (GEP-NETs). J Mol Med (Berl). 2010;88(4):423–429. | ||
Wu J, Lu Y, Ding YB, et al. Promoter polymorphisms of il2, il4, and risk of gastric cancer in a high-risk chinese population. Mol Carcinog. 2009;48(7):626–632. | ||
Shin WG, Jang JS, Kim HS, et al. Polymorphisms of interleukin-1 and interleukin-2 genes in patients with gastric cancer in Korea. J Gastroenterol Hepatol. 2008;23(10):1567–1573. | ||
Amirzargar AA, Bagheri M, Ghavamzadeh A, et al. Cytokine gene polymorphism in iranian patients with chronic myelogenous leukaemia. Int J Immunogenet. 2005;32(3):167–171. | ||
Howell WM, Turner SJ, Theaker JM, et al. Cytokine gene single nucleotide polymorphisms and susceptibility to and prognosis in cutaneous malignant melanoma. Eur J Immunogenet. 2003;30(6):409–414. | ||
Ying H, Wang J, Gao X. CCL5-403, CCR5-59029, and Delta32 polymorphisms and cancer risk: a meta-analysis based on 20,625 subjects. Tumour Biol. 2014;35:5895–5904. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.