Back to Journals » Psychology Research and Behavior Management » Volume 14
Identifying Predictive Factors in Compliance with the COVID-19 Containment Measures: A Mediation Analysis
Authors Valenti GD ![]() , Faraci P
, Faraci P ![]()
Received 10 June 2021
Accepted for publication 7 August 2021
Published 25 August 2021 Volume 2021:14 Pages 1325—1338
DOI https://doi.org/10.2147/PRBM.S323617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Giusy Danila Valenti, Palmira Faraci
Faculty of Human and Social Sciences, University of Enna “Kore”, Enna, Italy
Correspondence: Giusy Danila Valenti
Cittadella Universitaria, 94100, Italy
Email [email protected]
Introduction: The outbreak of the COVID-19 pandemic has led governments to implement some containment measures to flatten the curve of the diffusion of the virus. The current study aims to investigate individual differences in compliance with these restrictive behaviors. In a sample of Italian individuals (N = 300), we examined whether sociodemographic factors, personality traits, fatalism, and fear could be considered as possible predictors.
Methods: We performed a series of standard multiple regression analyses and proposed a mediation analysis to test the associations among variables.
Results: Overall, our results suggested that men are less likely to engage in preventive behaviors, younger individuals are more reluctant to adhere to social distancing mandates, and fear has a functional role in predicting positive outcomes.
Conclusion: The results of our analyses are discussed and suggestions for future research are provided.
Keywords: pandemic, restrictions, protective variables, health behaviors
Introduction
Since the last months of 2019, a novel coronavirus, named COVID-19, has spread all over the world, causing serious respiratory health problems and a wide number of deaths. Due to its rapid diffusion, it was declared a global health emergency, and in March 2020 it was recognized a pandemic.1 Since then, individuals’ lifestyles have undoubtedly changed, strongly affecting psychological wellness and health. The severity of the COVID-19 infection, the high rate of mortality, and the ease of its transmission have led governments to put in place some temporary regulations to reduce the probability to infect and to be infected, combating the outbreak of the virus. The main rules involve hygienic measures (washing hands, sanitizing objects, sneezing or coughing into a tissue or into the elbow), and some restrictions and obligations, such as self-isolation, home quarantine, social distancing, and use of face masks. In other words, all these containment measures are strongly recommended to lessen the spread of the virus, and to prevent one’s own and others’ health.2 Despite the usefulness and effectiveness of these measures, some individuals are reluctant to comply with them. From this perspective, several studies have been conducted to identify the predominant factors accounting for individual differences in adhering to the preventive measures against the diffusion of the virus.
Demographics and Compliance with the COVID-19 Containment Measures
Demographic variables are relevant factors associated with health-related behaviors. Several studies have shown that women, older people, and more educated individuals are more likely to perform preventive practices than men, younger people, and individuals with less or no education.3,4 A similar trend has been found in recent studies aimed at examining the associations between sociodemographic factors and compliance with the current COVID-19 regulations.5–9
Personality and Compliance with the COVID-19 Containment Measures
Literature concerning the role of personality in health-related behaviors is broad, suggesting relevant and significant associations. The five-factor model10 is well known and largely accepted among scholars, and many studies are based on this theoretical model.
For instance, individuals with higher scores in conscientiousness are usually diligent, accurate, respectful, and duty-bound; for these reasons, they are inclined to follow rules and obligations, and to engage in healthy behaviors.11 Some studies12–15 have recently reported positive associations between conscientiousness and compliance with the COVID-19 containment measures.
Neuroticism is linked both to healthy and risky behaviors. On the one hand, individuals high in this trait may tend to engage in safe and healthy practices, such as a greater use of screening procedures or health care services,16,17 because they are worried about their own health.18–20 On the other hand, they may engage in unhealthy activities, such as risky sexual behaviors or excessive use of cigarettes, drugs, or alcohol, in order to find emotional comfort and relief.21 From this point of view, past research has shown that people higher in neuroticism often think themselves to be powerless and helpless when facing stressful situations, and rely on emotion-focused rather than problem-focused coping strategies.22,23 Recent studies aimed at examining the associations between neuroticism and compliance with the COVID-19 restrictions are incongruent, showing unclear and conflicting results.11–14,24 However, as mentioned by some authors,24,25 individuals higher in neuroticism may experience increased concerns about the COVID-19 and a greater worry about being infected, showing an inclination for adherence to restrictions in order to protect their health.
Individuals higher in extraversion tend to experience positive affect, have greater global self-efficacy, and more positively evaluate their lives26 and health.27 Extraverted individuals are dominant, assertive, active, and impulsive; they are social and outgoing, and they enjoy being involved in social gatherings and in dynamic activities. Due to these characteristics, people high in extraversion may adhere to healthy practices, but they may find difficult to comply with isolating measures that hinder sociability. Across previous and current studies,11–13,15 extraverted people reported greater reluctance to observe the current regulations, especially social distancing.
Agreeableness indicates how warm, friendly, and tactful a person is. Individuals high in agreeableness are kind, empathic, unselfish, and have cooperative values. In other words, these people usually show prosocial behaviors, and their actions are driven by the goal of protecting and respecting others.28 From this point of view, regarding the pandemic, agreeable people may tend to follow the preventive measures to safeguard others’ health. In recent research,24,29 agreeableness was associated with greater compliance with the anti-COVID-19 measures, confirming this theoretical premise.
Openness means being creative, open to changes and to new ideas. Individuals with a high level of this trait are usually willing to try new experiences, they tend to seek out activities that bring meaning to their lives, and unexpected changes in their routines are welcome. This personality trait suggests that open individuals can perceive both social distancing and self-isolation as opportunities to create and engage in new and innovative activities, developing and cultivating their creativity and imagination. Recent research showed positive associations between openness and adherence to COVID-19 restrictions.11,13,24
Fatalism and Compliance with the COVID-19 Containment Measures
Fatalistic individuals tend to be inactive because they think that everything happening in their life is predetermined and that each outcome derives from external and more powerful forces. In addition, fatalistic people usually tend to have a pessimistic view about future events, not believing that something good can happen.30,31 Some authors32,33 have recently reported that fatalistic individuals are more likely to ignore preventive measures because they think that being infected is a matter of luck or destiny. From this perspective, Akesson et al34 proposed a model explaining how beliefs related to the pandemic could affect the choice of whether to comply with the restrictive measures. They stated:
If individuals come to believe that the virus is more infectious, then they revise upwards their assessment of the probability that they will get the virus even if they socially distance (or follow other best practices such as washing their hands frequently). But if individuals come to believe that they are likely to get the virus no matter what they do, then they may decide to ignore social distancing measures34 (p.19).
Additionally, some authors33 reported that fatalism and its subdimensions increased or decreased fear, which in turn, led to changes in respecting the restrictive measures.
Fear and Compliance with the COVID-19 Containment Measures
Fear is an unpleasant emotional state due to the perception of a threatening stimulus,35 and being afraid of a threatening stimulus is often associated with a greater inclination toward engaging in healthy behaviors and avoidance of risky and unsafe practices.36,37 Furthermore, some authors have recently linked the feeling of fear to compliance with rules dictated by authorities.38 Recent research9,14,39-41 has examined the role of fear in adhering to the COVID-19 restrictions, reporting significant and positive associations. These results suggest that the pandemic is perceived as a threat, acting as a motivational factor causing people to perform preventive behaviors. Some scholars outlined the functional role of fear as increasing the probability of compliance for ameliorating public health.39 Nevertheless, fear of COVID-19 is often associated with a lower grade of wellness, accompanied by depressive and anxious symptoms, and some authors have also argued that high levels of fear lead people to think irrationally when reacting to the pandemic.42
The Current Study
The aim of the current study consists of evaluating the associations between sociodemographic variables, personality traits, fatalistic beliefs, fear of COVID-19, and the engagement in the COVID-19 containment measures. To our knowledge, no existing studies jointly examining the relationships between demographics, dispositional traits, cognitive styles, feelings related to the pandemic, and compliance with the COVID-19 restrictions have been published. Although the relationships between the aforementioned variables and adherence to the COVID-19 containment measures have been extensively documented, we believe that their investigation in the same study sample may contribute to a deeper and more comprehensive evaluation of the phenomenon, allowing an easier identification of the best predictors of the outcome variables. In fact, only when the examined variables are taken into account together it is possible to identify which of them plays a major role in predicting the COVID-19 restrictive measures, thus providing useful information both from a theoretical and a practical perspective. This may be considered the strength of this work.
Drawing on these theoretical premises and on prior research, we posited the following hypotheses:
H1: Sociodemographic factors are associated with compliance with the COVID-19 containment measures. Specifically, we expect to find higher levels of compliance in (i) women, (ii) older people, and (iii) more educated individuals. H2: Personality traits are associated with compliance with the COVID-19 containment measures. Specifically, we expect to find that: H2a: individuals higher in conscientiousness report higher levels of compliance; H2b: individuals higher in neuroticism report higher levels of compliance; H2c: individuals higher in openness report higher levels of compliance; H2d: individuals higher in agreeableness report higher levels of compliance; H2e: individuals higher in extroversion report lower levels of compliance. H3: Fatalism and its subdimensions are negatively associated with compliance with the COVID-19 containment measures. H4: Fear is positively associated with compliance with the COVID-19 containment measures. H5: Fear functions as a mediator in the relationship between fatalism subdimensions and compliance with the COVID-19 containment measures. The hypothesized model (Figure 1) aims at exploring whether and how the association between fatalism subdimensions and the restrictive measures change by introducing fear as a mediator.
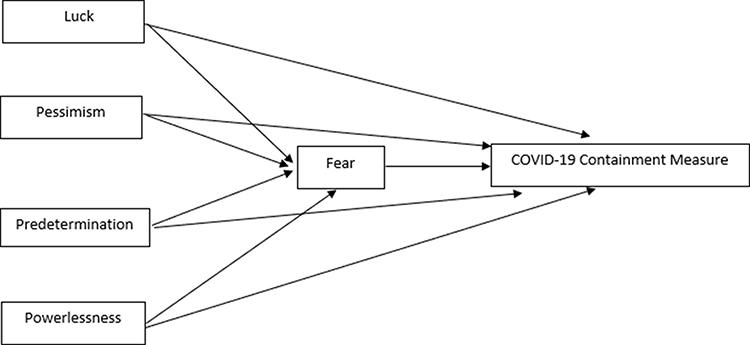 |
Figure 1 Hypothesized mediation model. |
Materials and Methods
Participants and Procedures
A sample of 355 individuals was recruited to fill in an online questionnaire. The initial screening led to elimination of 55 participants because they failed to complete the whole survey, thus reporting a percentage of missing data above the 5%. The final sample was composed of 300 individuals (60% women), aged from 18 to 70 years (M = 33.91, SD =10.97). Regarding educational level, 14.7% held postgraduate degrees (PhD), 44% were college graduates (bachelor’s or master’s degrees), 37% had a high school diploma, and a small portion (4.3%) attained only a junior school diploma. Data were gathered online, by sharing the research link on social media. Respondents were informed that their participation in the study was voluntary, and they were also assured of the confidentiality of the information obtained. Informed consent was given by all participants prior to answering the survey. All procedures were performed in compliance with provisions from the Declaration of Helsinki regarding research on human participants and approved by the UKE Internal Review Board of Research in Psychology.
Instruments
Personality
To assess the personality traits, we used the Big Five Questionnaire (BFQ).43 The BFQ is a 132 item-scale measuring personality facets according to the well-established five-factors model,10 and it uses a 5-point Likert scale (from 1 = absolutely false to me to 5 = absolutely true to me). It provides different normative points for men and women. Reliability coefficients were good for all subscales, ranging from 0.73 to 0.90.
Fatalism
Fatalism was tested by using the Italian version of the Fatalism Scale (FS).44,45 The measure consists of 18 items distributed across four dimensions: Luck (α = 0.93), Powerlessness (α = 0.84), Predetermination (α = 0.82), and Pessimism (α = 0.75). It uses a 5-point Likert scale (from 1 = strongly disagree to 5 = strongly agree), with higher scores indicating a greater level of fatalism.
Fear of COVID-19
To evaluate the degree of fear related to the virus, we used the Fear of COVID-19 Scale,42,46 a 7-item measure using a 5-point Likert scale (from 1 = strongly disagree to 5 = strongly agree), with higher scores suggesting a greater level of fear. Internal reliability was good, with Cronbach’s alpha reaching 0.87.
Compliance with the COVID-19 Restrictions
We created three items, each depicting one of the three containment measures: (i) social distancing (“During conversations, I have respected social distancing”), (ii) hygiene (“I have washed my hands frequently”), and (iii) mask wearing (“I have worn a mask everywhere”). Participants were asked to choose the response best describing how often they had performed each preventive behavior in the previous 30 days (from 1 = never to 5 = always). Higher scores are associated with a greater level of compliance with the COVID-19 containment measures.
Data Analysis
The percentage of missing values across the investigated variables was <5%, which was handled through the mean imputation technique. According to past literature,47,49 this procedure can be adequately used when the percentage of missing data is low, and when data can be considered as missing completely at random (MCAR). A preliminary check of multivariate normality was done to assess the extent to which procedures based on normal distribution theory could be applied. Mardia’s multivariate kurtosis index (307.92) indicated the absence of multivariate normality. Multivariate outliers (n = 5) were then removed, and the assumption of multivariate distribution was then accomplished. Subsequent analyses were performed on a sample of 295 participants, except for the BFQ scores’ interpretations, in which men’s and women’s scores were considered separately because the measure provides different normative points for the two sexes. Prior to conducting the main analyses, we performed a correlation inspection between the study variables. After that, three standard multiple regression analyses were computed, one for each containment measure. A mediation analysis was also proposed in which fear was introduced as a mediator in the relationships between the four fatalism subdimensions and the outcome variables, and sex and age were entered as covariates. Data were analyzed using IBM SPSS (Version 20) for the descriptives, correlations, and standard multiple regression analyses, and jamovi (Version 1.6.23),50 with jAMM module51 to test the mediation model. Specifically, the jAMM package allows estimation of the direct and indirect effects of the independent variables (the fatalism subscales) on the dependent variables (the three compliance behaviors), by also examining all paths of the mediation model components (eg, the associations between the independent variables and the mediator and the associations between the mediator and the dependent variables).
Results
Descriptives and Correlations Between Variables
In Table 1 the descriptives for all the investigated variables are reported. BFQ raw scores were first converted into T scores and all the results were around the mean (extroversion: Tmen = 49, Twomen = 53; neuroticism: T = 51 for both sexes; openness: Tmen = 52, Twomen= 53; conscientiousness: T = 57 for both sexes; agreeableness: Tmen = 54, Twomen = 56). However, we opted to report BFQ raw scores instead of T scores in Table 1, to make them uniform with the scores obtained in all the other measures. Fatalism scores indicated that participants scored around average levels on each subdimension – luck, pessimism, predetermination, and powerlessness – suggesting that fatalistic beliefs are not predominant in our study sample, whereas fear scores were quite high. Regarding compliance with the three containment measures – social distancing, hygiene, and mask wearing – high levels were reported in all cases. Though a low level of variability was estimated in relation to the degree of compliance, we wanted to examine whether any individual differences existed.
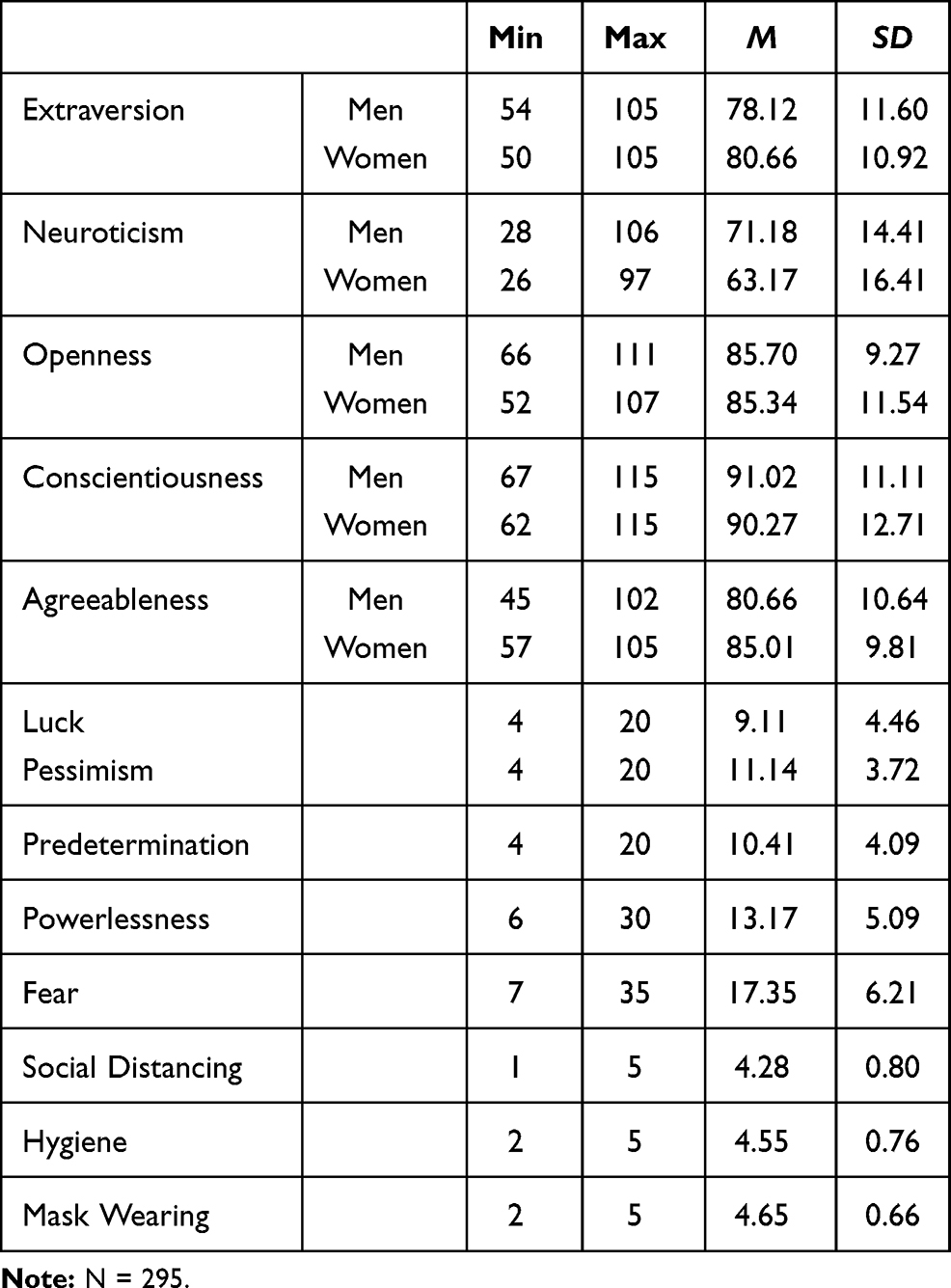 |
Table 1 Descriptives |
Table 2 shows the correlations between the investigated variables. On the whole, weak and positive relationships were estimated between fear and the three compliance behaviors, suggesting that individuals with higher levels of fear tend to be more inclined to adhere to the COVID-19 restrictive measures. For all the other variables we found weaker or nonsignificant associations with the outcome variables.
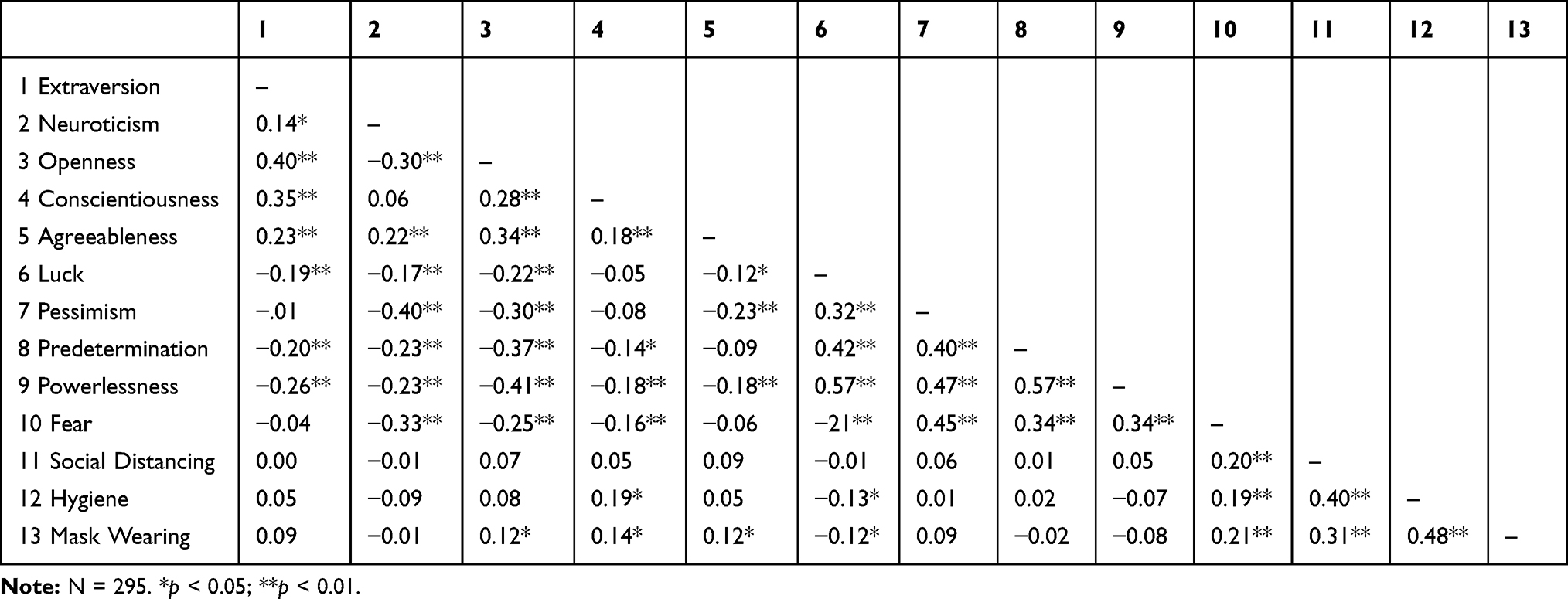 |
Table 2 Correlations Between the Study Variables |
Regression Analyses
In the following sections, the results of standard multiple regression analyses are reported. A complete description of the outcomes is shown in Table 3.
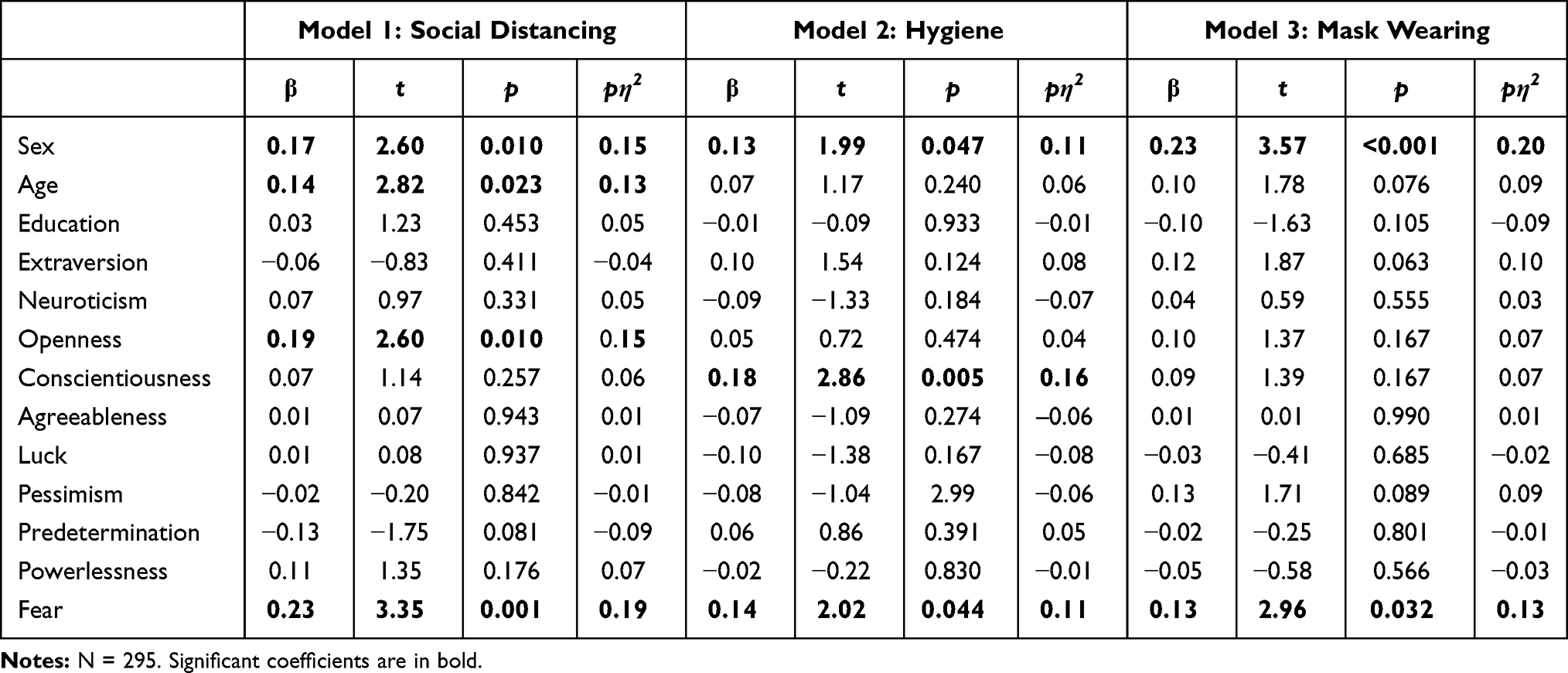 |
Table 3 Regression Coefficients of Demographics, Personality, Fatalism, and Fear on Compliance with the COVID-19 Containment Measures |
Predicting Social Distancing from Demographics, Personality Traits, Fatalism, and Fear
Our findings showed a significant model fit, and the independent variables accounted for almost 14% of the total amount of variation (R2 = 0.135, p < 0.001, f2 = 0.16). Regarding demographics, sex (β = 0.17, t = 2.60, p = 0.01, partial η2= 0.15) and age (β = 0.12, t = 2.01, p = 0.045, partial η2= 0.13) were significant predictors. Specifically, the significant associations for sex indicated that women complied more readily than men, and that younger individuals were more reluctant to respect social distancing. Openness was the only personality trait reporting significant associations (β = 0.19, t = 2.60, p = 0.010, partial η2= 0.15), whereas the fatalism subdimensions did not report any significant relationships. Furthermore, fear was positively associated with the outcome variable (β = 0.23, t = 3.35, p = 0.001, partial η2= 0.19).
Predicting Hygiene from Demographics, Personality Traits, Fatalism, and Fear
As previously, the overall model fit was significant, and the independent variables accounted for almost 12% of the total amount of variation (R2 = 0.117, p = 0.001, f2 = 0.13). Sex (β = 0.13, t = 1.99, p = 0.047, partial η2= 0.11) was the only demographic factor significantly associated with the dependent variable, indicating that women were more likely than men to adopt COVID-related hygienic practices. As far as it concerns personality, except for conscientiousness, which showed significant positive associations (β = 0.18, t = 2.87, p = 0.005, partial η2= 0.16), the other personality traits were unrelated to compliance with the hygienic practices. Fatalism and its four subdimensions, did not report any significant relationships, whereas fear revealed significant results (β = 0.14, t = 2.02, p = 0.044, partial η2= 0.11).
Predicting Mask Wearing from Demographics, Personality Traits, Fatalism, and Fear
The overall model fit showed statistically significant results (R2 = 0.142, p < 0.001, f2 = 0.17). Among demographics variables, sex was the only factor reporting significant results (β = 0.23, t = 3.57, p < 0.001, partial η2= 0.20), suggesting, also in this case, that women were more likely to respect preventive measures than men. Age and education did not show significant associations. Following, neither the personality traits nor the fatalism subdimensions reported significant effects, whereas fear was positively associated with the outcome variable (β = 0.13, t = 2.96, p = 0.032, partial η2= 0.13).
Mediation Analyses
Three separate mediation models were examined in which fear was inserted as a mediator in the relationship between the fatalism subdimensions and each containment measure. Because data were normally distributed, confidence intervals were computed using the standard method (Delta method).
Associations Among Fatalism Subdimensions and Compliance with Social Distancing Mediated by Fear
Though none of the fatalism subscales directly predicted compliance with social distancing, by introducing fear as a mediator, we estimated significant indirect effects for pessimism (β = 0.053, p = 0.019, 95% CI [0.001, 0.021]) and predetermination (β = 0.024, p = 0.043, 95% CI [0.001, 0.013]). Specifically, both subscales increased fear, which in turn positively affected the respect for social distancing rules. For more detailed information about the associations among variables, please see Table 4 and Figure 2.
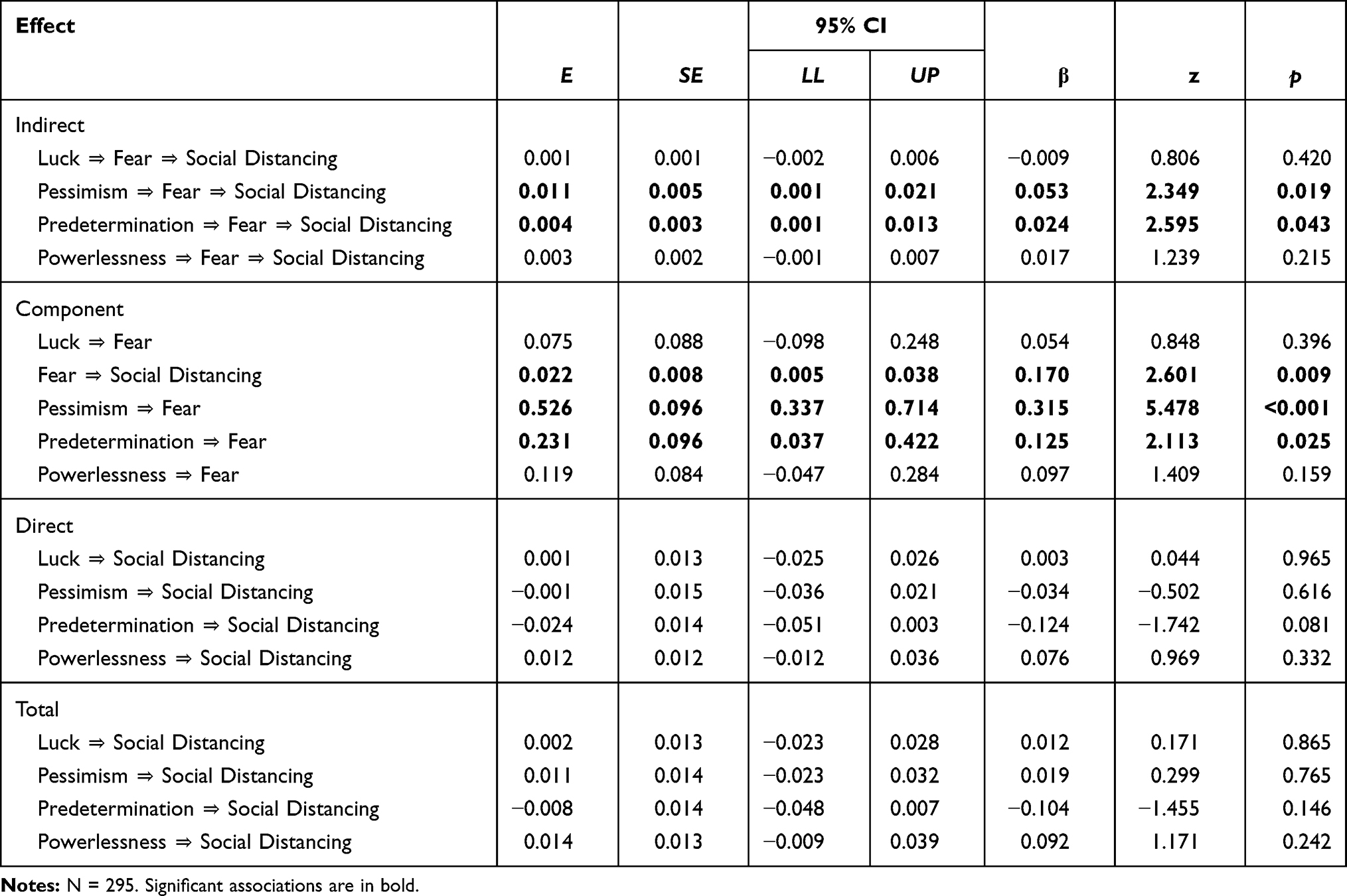 |
Table 4 Associations Among Fatalism Subdimensions and Compliance with Social Distancing Mediated by Fear |
 |
Figure 2 Relationships among fatalism subscales and social distancing through fear. Notes: Direct effects are in parentheses. *p < 0.05; **p<0.01; ***p < 0.001. |
Associations Among Fatalism Subdimensions and Compliance with Hygiene Mediated by Fear
Among the four fatalism subdimensions, findings from mediation analyses showed that pessimism and predetermination reported indirect effects (β = 0.034, p = 0.025, 95% CI [0.002, 0.032] and β = 0.043, p = 0.046, 95% CI [0.002, 0.027], respectively) on hygiene. Both subdimensions were positively associated with fear, which in turn positively affected compliance with the outcome variable. Table 5 and Figure 3 display all the associations among the variables taken into account.
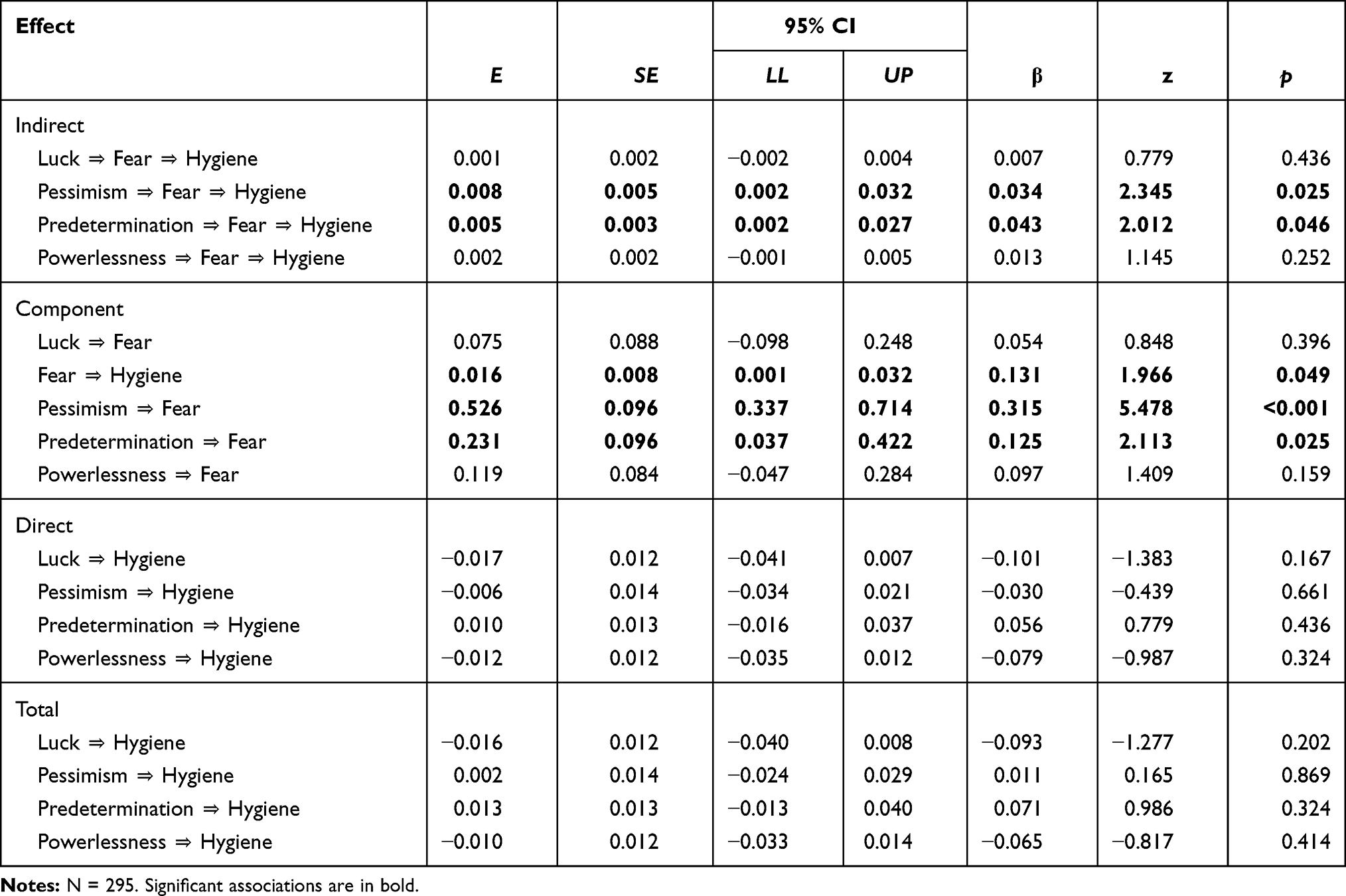 |
Table 5 Associations Among Fatalism Subdimensions and Compliance with Hygiene Mediated by Fear |
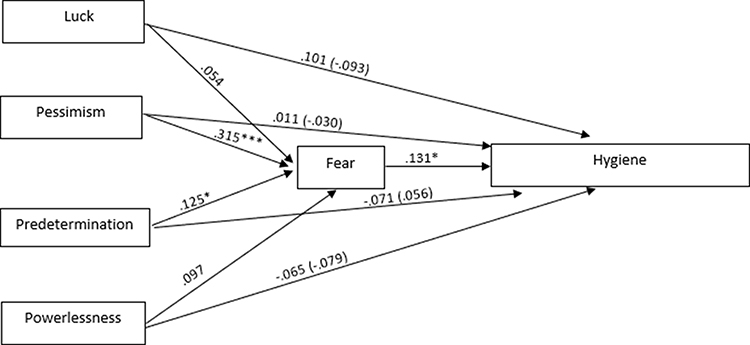 |
Figure 3 Relationships among fatalism subscales and hygiene through fear. Notes: Direct effects are in parentheses. *p < 0.05; ***p < 0.001. |
Associations Among Fatalism Subdimensions and Compliance with Mask Wearing Mediated by Fear
The results of our analyses revealed that only pessimism reported an indirect effect (β = 0.054, p = 0.045, 95% CI [0.006, 0.027]) on mask wearing. Also in this case pessimism was positively associated with fear, and this latter was linked to a greater probability of compliance. In Table 6 and Figure 4 all the associations among the variables are shown.
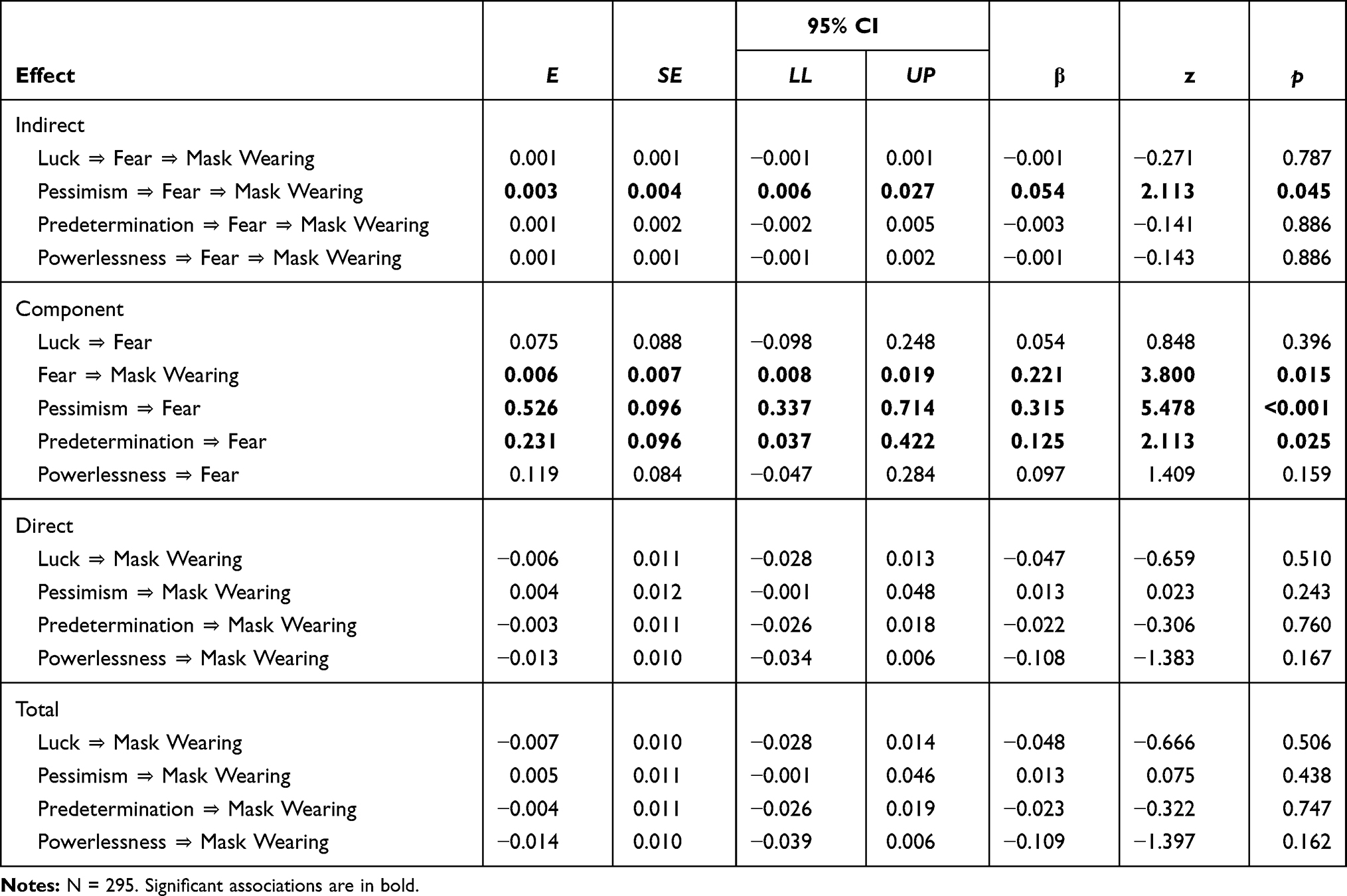 |
Table 6 Associations Among Fatalism Subdimensions and Compliance with Mask Wearing Mediated by Fear |
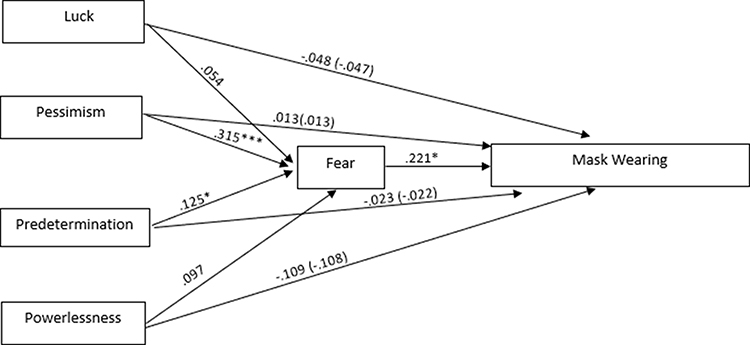 |
Figure 4 Relationships among fatalism subscales and mask wearing through fear. Notes: Direct effects are in parentheses. *p < 0.05; ***p < 0.001. |
Discussion
The current study sought to determine which factors best predicted adherence to the restrictive measures implemented by governments to reduce the spread of the COVID-19. Though several studies have recently been conducted to identify which variables account for individual differences in compliance with the preventive measures,24,29,32,40 this work has the advantageous to take into account sociodemographic factors, personality traits, fatalistic beliefs, and fear in a single study sample.
Overall, our results indicated that scores were average for each independent variable, except for fear, which was moderate. Concerning the three containment measures – social distancing, hygiene, mask wearing – high levels of compliance were reported in all cases.
H1 was partially supported because among the sociodemographic variables, only sex was related to the three outcome variables in the hypothesized direction, whereas age was associated with respect for social distancing only. As a viable explanation, maintaining social distancing may be more difficult for younger people, who suffer from the lack of any kind of entertainment or opportunities for gathering with friends, showing a higher degree of willingness to gather as they used to before the pandemic. Hygienic practices and mask wearing have a lesser impact on social life, and thus affect individuals regardless of age. In addition, in Bish’s and Michie’s52 review about the associations between demographic and protective behaviors during a pandemic, some studies reported that age was not related to the chance of carrying out the preventive practices.53,54 Further, contrary to our hypotheses, education was not associated with compliance with the COVID-19 measures. Although a majority of research suggests that more educated people are more inclined to adopt precautionary behaviors,55-59 studies examining individual differences in behaviors during previous pandemics did not find any associations between education level and containment measures,53,54,60 suggesting that the pattern of relationships between one’s educational background and the likelihood of adhering to preventive behaviors is unclear.
Surprisingly, except for openness (which was related to social distancing) and conscientiousness (which was associated with hygiene), we found no significant associations between personality traits and compliance with the COVID-19 restrictions (H2). Both openness and conscientiousness affected the outcome variables in the hypothesized direction, though we expected to find positive relationships with the three containment measures. From this perspective, our results are in line with previous research according to which the COVID-19 restrictive measures represent distinct behaviors predicted by different factors.61 To plausibly explain the limited influence of personality traits on adherence to the restrictive measures, we put forth the “strong situation hypothesis” which asserts that when strong situations– such as the COVID-19 pandemic – occur, dispositional traits play a minor role in predicting behaviors compared to situational cues.62 This in turn implies lesser individual differences and similar perceptions across people. Previous research has also supported this hypothesis.29,63
Next, by examining the relationships between fatalism and its subdimensions and the outcome variables (H3), we found no statistically significant associations; thus, we could not confirm our hypothesis. These unexpected results may be read in the light of the time perspective theory proposed by Zimbardo and Boyd,64 which suggests that people differ from each other regarding which specific segment of time – past, present, or future – they mainly concentrate on. This theoretical framework takes into account different types of time perspectives: past positive or negative perspective; hedonistic (positive future appraisal) and fatalistic (negative future appraisal) perspectives; and carpe diem perspective, which is the tendency to focus on the present. A recent study conducted by Sobol et65 al indicated that only the carpe diem time perspective significantly predicted health regulation behaviors during the COVID-19 pandemic, pointing out that the focus on the “here and now”, together with what an individual actually does in the present has a crucial role in promoting positive outcomes.
Moreover, we also investigated whether adopting the restrictive measures was related to fear (H4). Consistent with our hypotheses and in line with previous works,9,14,39 fear was positively associated with each outcome variable, supporting the idea proposed by Harper et39 al who emphasized the functional role of fear in promoting health-related behaviors during the pandemic.
Finally, we proposed a mediation model (H5) in which the relationship between fatalism (and its subdimensions) and the containment measures was examined via fear. Specifically, we performed three separate mediation analyses, in which fear was introduced as a mediator in the relationship between the fatalism subdimensions and each containment measure. The mediation hypothesis was partially confirmed because the indirect effects were not always estimated. Specifically, we found that pessimism and predetermination indirectly affected compliance with social distancing and hygiene, whereas fear mediated the relationship between pessimism and mask wearing. When indirect effects were estimated, greater scores in each fatalism subscale corresponded to increased fear, which in turn positively affected compliance behaviors. From this point of view, our findings are contrast somewhat to some previous works in which belief in predetermination and luck were found to reduce levels of fear, whereas pessimism produced an increase of fear.33 As a possible explanation, because people higher in predetermination think that everything that happens in their lives depends on fate, they may show greater fear due to the fact that they do not know what destiny has in store for them, thus showing feelings of discomfort toward uncertainty and the unknown. Notably, neither luck nor powerlessness affected the levels of fear. Likely, believing that health conditions are a matter of luck, may be more closely linked to hope than to fear, and belief in human powerlessness against illness and disease may induce individuals to feel a sense of meaninglessness, flattening any kind of emotion.
From a practical perspective, the results of our study suggest that government should create health policies to promote and deliver personality-tailored messages aimed at sensibilizing individuals with the lowest inclination toward compliance with the COVID-19 restrictions – such as younger people and men – and foster knowledge about the risks linked to nonadherence to pandemic-related health policies.
Ultimately, although our study contributes to further understanding individual differences in compliance with the COVID-19 restrictions, the small portion of the total variance explained by the investigated variables leads us to argue that alternative or further factors may meaningfully improve predictive power. For example, individuals may differ in their general risk perception, their degree of trust in science or in government, or the overall levels of personal morality. It is plausible that all these variables affect willingness to adhere to the COVID-19 containment measures.
Limitations and Future Directions
The results of the current study should be read in light of some limitations. First, data were collected from digital sources due to the specific conditions caused by the restrictions related to the virus; hence, it was not possible to obtain a randomly sampled selection. Second, we used single items to measure engagement in the containment behaviors, evaluating individuals’ declarations about compliance rather than their actual behavior. Nevertheless, no validated scales assessing compliance with the COVID-19 restrictions exist, and the use of a set of items as a scale without adequate psychometric studies would likely have produced distorted results.
Additionally, we asked individuals to choose the response best describing how often they had performed each preventive behavior in the previous 30 days, probably too wide a period for assessing a concrete behavior using single-item scales. Future research may include a larger set of items for each restrictive measure and evaluate compliance over a shorter period (eg, last week). Furthermore, we also argue that asking whether people adhere to the COVID-19 restrictive measures through Self-Report may be subject to bias. Indeed, compliance is a socially desirable behavior, thus responses may be easily affected by social desirability, decreasing the trustworthiness of the results. A further limitation is the cross-sectional nature of the study, so we cannot claim the causality of the estimated relationships. From this perspective, longitudinal studies are needed and highly recommended.
Conclusion
The present study adds to the growing literature about individual differences in compliance with the COVID-19 restrictions an examination of a broad set of variables within a single study sample. Overall, our work suggested that sociodemographic factors and fear play relevant roles in shaping how people behave during the pandemic. Specifically, compared to men and younger individuals, women and older people showed higher levels of inclination toward compliance. In addition, findings from our analyses pointed out that fear has a functional role in increasing people’s inclination toward engagement in the containment measures. In light of these results, we suggest that researchers and mental health professionals pay attention to the specific context within which negative emotional states are experienced before considering whether such emotional states are detrimental to psychological health and wellness. That is, in such circumstances, fear seems to have a protective role, acting as a motivating factor for changing behaviors. This does not mean that those working in the public services should promote an excessive increase of fear, leading individuals to act irrationally, rather, we encourage favoring and publicizing clear messages about the risks associated with reluctance to comply. Deeper knowledge of the current period we are experiencing is fundamental to improve individuals’ awareness regarding their own actions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Coronavirus disease 2019 (COVID-19) situation report (report N° 51); 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
2. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020;20(5):Article e102–e107. doi:10.1016/S1473-3099(20)30129-8
3. Deeks A, Lombard C, Michelmore J, et al. The effects of gender and age on health- related behaviors. BMC Public Health. 2009;2009(9):213. doi:10.1186/1471-2458-9-213
4. Vaidya V, Parth G, Karmakar M. Gender differences in utilization of preventive care services in the United States. J Womens Health. 2012;21(2):140–145. doi:10.1089/jwh.2011.2876
5. Abolfotouh MA, Almutairi AF, Banimustafa A, et al. Behavior responses and attitude of the public to COVID-19 pandemic during movement restrictions in Saudi Arabia. Int J Gen Med. 2021;14:741–753. doi:10.2147/IJGM.S296867
6. Brankston G, Merkley E, Fisman DN, et al. Socio-demographic disparities in knowledge, practices, and ability to comply with COVID-19 public health measures in Canada. Can J Public Health. 2021;112(3):363–375. doi:10.17269/s41997-021-00501-y
7. Carlucci L, D’Ambrosio I, Balsamo M. Demographic and attitudinal factors of adherence to quarantine guidelines during COVID-19: the Italian model. Front Psychol. 2020;11:559288. doi:10.3389/fpsyg.2020.559288
8. Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health. 2020;17(14):4924. doi:10.3390/ijerph17144924
9. Yıldırım M, Geçer E, Akgül Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviors against COVID-19. Psychol Health Med. 2020. doi:10.1080/13548506.2020.1776891
10. McCrae RR, John OP. An introduction to the five-factor model and its applications. J Person. 1992;60(2):175–215. doi:10.1111/j.1467-6494.1992.tb00970.x
11. Nofal AM, Caciotti G, Lee N. Who complies with COVID-19 transmission mitigation behavioral guidelines? PLoS One. 2020;15(10):Article e0240396. doi:10.1371/journal.pone.0240396
12. Abdelrahman M. Personality traits, risk perception, and protective behaviors of Arab residents of Qatar during the COVID-19 pandemic. Int J Ment Health Addict. 2020:1–2. doi:10.1007/s11469-020-00352-7
13. Ashwanden D, Strickhouser JE, Sesker AA, et al. Psychological and behavioural responses to Coronavirus disease 2019: the role of personality. Eur J Pers. 2020;35(1):51–66. doi:10.1002/per.2281
14. Brouard S, Vasilopoulos P, Becher M. Sociodemographic and psychological correlates of compliance with the COVID-19 public health in France. Can J Polit Sci. 2020;53(2):253–258. doi:10.1017/S0008423920000335
15. Carvalho LF, Pianowski G, Gonçalves G. Personality differences and COVID-19: are extroversion and conscientiousness personality traits associated with engagement with containment measures? Trend Psychiatr Psychother. 2020;42(2):179–184. doi:10.1590/2237-6089-2020-0029
16. Aschwanden D, Gerend MA, Luchetti M, et al. Personality traits and preventive cancer screenings in the health retirement study. Prev Med. 2019;126:105763. doi:10.1016/j.ypmed.2019.105763
17. Cuijpers P, Smit F, Penninx BWJ, et al. Economic costs of neuroticism: a Population-Based Study. Arch Gen Psychiatry. 2010;67(10):1086–1093. doi:10.1001/archgenpsychiatry.2010.130
18. Friedman HS. Long-term relations of personality and health: dynamisms, mechanisms, tropisms. J Person. 2000;68(6):1089–1107. doi:10.1111/1467-6494.00127
19. Van Dijk SDM, Hanssen D, Naarding P, et al. Big five personality traits and medically unexplained symptoms in later life. Eur Psychiatry. 2016;38:23–30. doi:10.1016/j.eurpsy.2016.05.002
20. Weiss A, Deary IJ. A new look at neuroticism: should we worry so much about worrying? Curr Dir Psychol Sci. 2020;29(1):92–101. doi:10.1177/0963721419887184
21. Mõttus R, Realo A, Allik J, et al. History of the diagnosis of a sexually transmitted disease is linked to normal variation in personality traits. J Sex Med. 2012;9(11):2861–2867. doi:10.1111/j.1743-6109.2012.02891.x
22. Carver CS, Connor-Smith J. Personality and coping. Annu Rev Psychol. 2010;61(1):679–704. doi:10.1146/annurev.psych.093008.100352
23. Luhmann M, Eid M. Does it really feel the same? Changes in life satisfaction following repeated life events. J Pers Soc Psychol. 2009;97(2):363–381. doi:10.1037/a0015809
24. Han H. Exploring the association between compliance with measures to prevent the spread of COVID-19 and big five traits with Bayesan generalized linear model. Pers Individ Differ. 2021;176:110787. doi:10.1016/j.paid.2021.110787
25. Qian K, Yahara T, Hashimoto K. Mentality and behavior in COVID-19 emergency status in Japan: influence of personality, morality and ideology. PLoS One. 2020;15(7):Article e0235883. doi:10.1371/journal.pone.0235883
26. Soto CJ. Is happiness good for your personality? Concurrent and prospective relations of the big five with subjective wellbeing. J Pers. 2015;83(1):45–55. doi:10.1111/jopy.12081
27. Sutin AR, Terracciano A. Five-factor model personality traits and the objective and subjective experience of body weight: personality and body weight. J Pers. 2016;84(1):102–112. doi:10.1111/jopy.12143
28. Wilkowski BM, Robinson MD, Meier BP. Agreeableness and the prolonged spatial processing of antisocial and prosocial information. J Res Pers. 2006;40(6):1152–1168. doi:10.1016/j.jrp.2005.12.004
29. Zajenkowski M, Jonason PK, Leniarska M, Kozakiewicz Z. Who complies with the restrictions to reduce the spread of COVID-19? Personality and perceptions of the COVID-19 situation. Pers Individ Differ. 2020;166:1–6. doi:10.1016/j.paid.2020.110199
30. Flórez KR, Aguirre AR, Viladrich A, et al. Fatalism or destiny? A qualitative study and interpretative framework on Dominican women’s breast cancer beliefs. J Immigr Minor Health. 2009;11(4):291–301. doi:10.1007/s10903-008-9118-6
31. Powe BD, Finnie R. Cancer fatalism: the state of the science. Cancer Nurs. 2003;26(6):454–465. doi:10.1097/00002820-200312000-00005
32. Jimenez T, Restar A, Helm PJ, et al. Fatalism in the context of COVID-19: perceiving coronavirus as a death sentence predict reluctance to perform recommended preventive behaviors. SSM Popul Health. 2020;11:100615. doi:10.1016/j.ssmph.2020.100615
33. Ozdil K, Büyüksoy GDB, Çatiker A. Fatalism, fear, and compliance with preventive measures in COVID-19 pandemic: a structural equation model analysis. Public Health Nurs. 2021. doi:10.1111/phn.12898
34. Akesson J, Ashworth-Hayes S, Hahn R, et al. Fatalism, Beliefs, and Behaviors During the COVID-19 Pandemic (No. W27245). National Bureau of Economic Research; 2020.
35. de Hoog N, Stroebe W, de Wit JB. The processing of fear‐arousing communications: how biased processing leads to persuasion. Soc Influ. 2008;3(2):84–113. doi:10.1080/15534510802185836
36. Lerner JS, Keltner D. Fear, anger, and risk. J Pers Soc Psychol. 2001;81(1):146–159. doi:10.1037/0022-3514.81.1.146
37. Marcus GEW, Neuman R, MacKuen. M. Affective Intelligence and Political J Udgment. Chicago: University of Chicago Press; 2000.
38. Vasilopoulos P, Marcus GE, Foucault M. Emotional responses to the Charlie Hebdo attacks: addressing the authoritarianism puzzle. Polit Psychol. 2018;39(3):557–575. doi:10.1111/pops.12439
39. Harper CA, Satchell LP, Fido D, et al. Functional fear predicts public health compliance in the COVID-19 pandemic. Int J Ment Health Addic. 2020:1–4. doi:10.1007/s11469-020-00281-5
40. Melki J, Tamim H, Hadid D. et al. Media exposure and health behavior during pandemics: the mediating effect of perceived knowledge and fear on compliance with COVID-19 prevention measures. Health Commun. 2020:1–11. doi:10.1080/10410236.2020.1858564
41. Wang J, Rao N, Han B. Pathways improving compliance with preventive behaviors during the remission period of the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(7):3512. doi:10.3390/ijerph18073512
42. Ahorsu DK, Lin C, Imani V, et al. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. 2020:1–9. doi:10.1007/s11469-020-00270-8
43. Crapara GV, Barabaranelli C, Borgogni L, Perugini M. The “big five questionnaire”: a new questionnaire to assess the five factor model. Pers Individ Differ. 1993;15(3):281–288. doi:10.1016/0191-8869(93)90218-R
44. Shen L, Condit CM, Wright L. The psychometric property and the validation of a fatalism scale. Psychol Health. 2009;24(5):597–613. doi:10.1080/08870440801902535
45. Faraci P, Valenti GD. Dimensionality and accuracy based on item response theory in the fatalism scale during the COVID pandemic in Italy. Int J Psychol. 2021. (under review).
46. Soraci P, Ferrari A, Abbiati FA, et al. Validation and psychometric evaluation of the Italian version of the fear of Covid-19 scale. Int J Ment Health Addict. 2020:1–10. doi:10.1007/s11469-020-00277-1
47. Cook RM. Addressing missing data in quantitative counseling research. Couns Outcome Res Evaluation. 2020;1–11. doi:10.1080/21501378.2019.1711037
48. Parent MC. Handling item-level missing data: simpler is just as good. Couns Psychol. 2012;41(4):568–600. doi:10.1177/0011000012445176
49. Scheffer J. Dealing with missing data. Res Lett Inf Math Sci. 2002;2002(3):153–160.
50. The Jamovi Project. Jamovi. (version 1.6.23). [Computer Software]; 2021. Available from https://www.jamovi.org.
51. Gallucci M. jAMM: jamovi advanced mediation models. [jamovi module]. Available from: https://jamovi-amm.github.io/.
52. Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010;15(4):797–824.
53. Lau JT, Yang X, Tsui HY, et al. SARS related preventive and risk behaviors practiced by Hong Kong–mainland China cross border travelers during the outbreak of the SARS epidemic in Hong Kong. J Epidemiol Community Health. 2004a;58(12):988–996. doi:10.1136/jech.2003.017483
54. Lau JT, Yang X, Tsui HY, et al. SARS preventive and risk behaviors of Hong Kong air travelers. Epidemiol Infect. 2004b;132(4):727–736. doi:10.1017/S0950268804002225
55. Barr M, Raphael B, Taylor M, et al. Pandemic influenza in Australia: using telephone surveys to measure perceptions of threat and willingness to comply. Infect Dis. 2008;8:117–130. doi:10.1186/1471-2334-8-117
56. Leung GM, Lam TH, Ho LM, et al. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J Epidemiol Community Health. 2003;57(11):857–863. doi:10.1136/jech.57.11.857
57. Leung GM, Quah S, Ho LM, et al. A tale of two cities: community psycho behavioral surveillance in Hong Kong and Singapore during the severe acute respiratory syndrome epidemic. Infect Control Hosp Epidemiol. 2004;25(12):1033–1041. doi:10.1086/502340
58. Tang CSK, Wong CY. Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among Chinese in Hong Kong. Prev Med. 2004;39(6):1187–1193. doi:10.1016/j.ypmed.2004.04.032
59. Lau JT, Kim JH, Tsui HY, et al. Anticipated and current preventive behaviours in response to an anticipated human-to-human H5N1 epidemic in the Hong Kong Chinese general population. BMC Infect Dis. 2007;7(18):18–29. doi:10.1186/1471-2334-7-18
60. Tang CSK, Wong CY. An outbreak of the severe acute respiratory syndrome: predictors of health behaviours and effect of community prevention measures in Hong Kong, China. Am J Public Health. 2003;9(11):1887–1888. doi:10.2105/AJPH.93.11.1887
61. Wisman A, Letina S, Thurik R, et al. Hygiene and social distancing as distinct public health related behaviours among university students during the COVID-19 pandemic. Soc Psychol Bull. 2020;1–20.
62. Cooper WH, Withey MJ. The strong situation hypothesis. Pers Soc Psychol Rev. 2009;13(1):62–72. doi:10.1177/1088868308329378
63. Kuper N, Modersitzki N, Vy Pan L, et al. The situation during the COVID-19 pandemic: a snapshot in Germany. PLoS One. 2021;16(2):Article e0245719. doi:10.1371/journal.pone.0245719
64. Zimbardo PG, Boyd JN. Putting time in perspective: a valid, reliable individual-differences metric. J Pers Soc Psychol. 1999;77(6):1271–1288. doi:10.1037/0022-3514.77.6.1271
65. Sobol M, Blachnio A, Przepiórka A. Time of pandemic: temporal perspectives related to compliance with public health regulations concerning the COVID-19 pandemic. Soc Sci Med. 2020;265:113408. doi:10.1016/j.socscimed.2020.113408
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.