Back to Journals » Patient Preference and Adherence » Volume 19
Identifying Dimensions and Items for a Questionnaire to Assess Medication Adherence in Men and Women with Ischemic Heart Disease: Insights from the GENADHECAR Study
Authors Carbonell-Soliva Á ![]() , Nouni-García R, Quesada JA, González-Llopis F, Cordero A
, Nouni-García R, Quesada JA, González-Llopis F, Cordero A ![]() , Bertomeu-González V
, Bertomeu-González V ![]() , Orozco-Beltrán D, Verdú-Soriano J, Nolasco A
, Orozco-Beltrán D, Verdú-Soriano J, Nolasco A ![]() , Pérez-Jover V
, Pérez-Jover V ![]() , Mira JJ
, Mira JJ ![]() , López-Pineda A, Guillén-García S, Martínez-Pérez P, Carratalá-Munuera C, Gil-Guillén VF
, López-Pineda A, Guillén-García S, Martínez-Pérez P, Carratalá-Munuera C, Gil-Guillén VF
Received 5 February 2025
Accepted for publication 23 June 2025
Published 11 August 2025 Volume 2025:19 Pages 2429—2444
DOI https://doi.org/10.2147/PPA.S516285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Álvaro Carbonell-Soliva,1,2,* Rauf Nouni-García,2– 5,* Jose A Quesada,1,2,4 Francisco González-Llopis,6 Alberto Cordero,7– 9 Vicente Bertomeu-González,10 Domingo Orozco-Beltrán,1,2,4 José Verdú-Soriano,11 Andreu Nolasco,12 Virtudes Pérez-Jover,13 Jose Joaquín Mira,13,14 Adriana López-Pineda,1,2,4 Silvia Guillén-García,15 Pablo Martínez-Pérez,16 Concepción Carratalá-Munuera,1,2,4,* Vicente F Gil-Guillén,1,2,4,* Collaborators Leticia Fernández Friera, Julio Osende Olea, Avelino Pereira Expósito, Eduardo Paya Mora, Joaquina Díaz Torres On behalf of GENADHECAR Group
Cardiology Section, HM Sanchinarro Hospital, 28050 Madrid, Spain.; Cardiology Section, HM Sanchinarro Hospital, 28050 Madrid, Spain.; General University Hospital of Elda, 03600 Elda, Alicante, Spain; General University Hospital of Elda, 03600 Elda, Alicante, Spain; General University Hospital of Elda, 03600 Elda, Alicante, Spain; 1Clinical Medicine Department, Miguel Hernández University of Elche, San Juan de Alicante, 03550, Spain; 2Primary Care Research Center, Miguel Hernández University of Elche, San Juan de Alicante, 03550, Spain; 3Pathology and Surgery Department, Miguel Hernández University of Elche, San Juan de Alicante, 03550, Spain; 4Network for Research on Chronicity, Miguel Hernández University of Elche, San Juan de Alicante, 03550, Spain; 5Diagnostic Center, Institute of Health and Biomedical Research of Alicante, General University Hospital of Alicante, Alicante, 03110, Spain; 6General University Hospital of Elda, Elda, 03600, Spain; 7Biomedical Research Networking Center on Cardiovascular Diseases (CIBERCV), Madrid, 28029, Spain; 8Cardiology Department, IMED Hospital, Elche, 03203, Spain; 9Cardiology Research Unit, Foundation for the Promotion of Health and Biomedical Research of the Valencian Community (FISABIO), Valencia, 46020, Spain; 10Hospital Clinica Benidorm, Benidorm, 03501, Spain; 11Community Nursing, Preventive Medicine, Public Health and History of Science Department, University of Alicante, San Vicente Del Raspeig, 03690, Spain; 12Department of Community Nursing, Preventive Medicine, Public Health, and History of Science, University of Alicante, San Vicente del Raspeig, 03690, Spain; 13Department of Health Psychology, Miguel Hernández University of Elche, Elche, 03202, Spain; 14Centro de Salud Hospital Plá, Alicante, 03013, Spain; 15Cardiology Section, General University Hospital of Elda, Elda, 03600, Spain; 16Department of Clinical Medicine, Miguel Hernández University of Elche, San Juan de Alicante, 03550, Spain
*These authors contributed equally to this work
Correspondence: Adriana López-Pineda, Clinical Medicine Department, School of Medicine, University of Miguel Hernández de Elche, San Juan de Alicante, 03550, Spain, Tel +34 96 591 9309, Email [email protected]
Purpose: The objective of this study was to identify dimensions and items for a future questionnaire aimed at measuring medication nonadherence in people with ischemic heart disease, considering gender differences and incorporating the views of healthcare professionals, researchers, and patients.
Patients and Methods: We conducted a mixed-method cross-sectional study at San Juan de Alicante University Hospital and Miguel Hernández University (Spain). The methods used to identify dimensions included a consensus group of healthcare and scientific professionals, an open-response survey for community pharmacists, a closed-response patient survey, and patient focus groups. When drafting the item list, we followed international recommendations related to the number and wording of items. Our study also included a qualitative review of the item list and response scales by psychologists.
Results: The resulting item list includes 41 potential items grouped into 26 dimensions and five domains: “patient”, “treatment”, “disease”, “health professional-patient relationship” and “healthcare system”. It covers aspects such as personal beliefs, mood, polypharmacy, disease symptoms, patient-healthcare professional interaction and healthcare system factors. Response options are presented on a 5-point Likert scale, including agreement-level responses and frequency-level responses.
Conclusion: With the collaboration of patients, researchers, and healthcare providers, we potentially identified five domains, 26 dimensions, and 41 items with 5-point Likert scale response options. These will be considered in the subsequent development and validation of a questionnaire to measure medication adherence in patients with ischemic heart disease.
Keywords: cardiovascular disease, medication nonadherence, item development, mixed-methods research, gender perspective
Introduction
Patient nonadherence to prescribed medications remains a challenge worldwide. This situation has driven multiple studies and the development of intensive improvement strategies over the past decades.1 In 2012, researchers proposed a new terminology for the concept of medication adherence, which they defined as “the process by which patients take their medication as prescribed, further divided into three quantifiable phases: ‘Initiation’, ‘Implementation’ and ‘Discontinuation’”.2 Initiation is when the patient takes the first dose of their medication. Implementation describes how closely patients follow the prescribed regimen from the first to the last dose. Discontinuation is the end of therapy, when a patient stops taking the medication.2
Nonadherence to medication is a major cause of treatment failure, which can impair quality of life, increase healthcare costs, and hinder favorable clinical outcomes.1 Adherence is a complex phenomenon influenced by several factors that fall into five main categories: 1) socioeconomic factors, such as income and place of residence; 2) patient factors, such as beliefs and education; 3) disease factors, such as symptoms; 4) medication factors, such as polypharmacy and treatment complexity; and 5) healthcare system factors, such as communication and trust.3,4 It is crucial to understand these contributing factors to effectively address medication nonadherence, which the World Health Organization (WHO) considers a priority in view of its clinical, psychosocial, and economic consequences.5
According to one study, 33.5% of all deaths in western Europe in 2019 were caused by cardiovascular disease (CVD), predominantly ischemic heart disease (IHD), which accounted for 15.6% of all deaths.6 In Spain, data reported in a press release from the National Statistics Institute showed that CVD caused an estimated 114,865 deaths in 2023, or 26.5% of all deaths, and was the second leading cause of mortality after cancer.7 Medication nonadherence is common in people with CVD and has a considerable negative impact.8 Although clinical practice guidelines emphasize the importance of medication adherence in this population,8,9 published data show that one month after a heart attack, 30% of people will have stopped taking one or more of their prescribed medications,8 and only 43% are adherent after one year of treatment with aspirin, statins, and angiotensin-converting enzyme inhibitors.10 Several recent studies have described interventions aimed at improving both medication adherence and health outcomes in people with CVD. These include dietary interventions, polypills, and mobile applications.11–13
Currently, the most widely used instruments for measuring adherence among CVD patients in clinical practice are the Morisky-Green test14 and the Haynes-Sackett test,15 both of which were originally developed and validated in patients with hypertension. However, both instruments have a low predictive value and low sensitivity and are sometimes used to measure adherence in diseases for which they have not been validated,16 such as IHD. They were developed using a partially integrative approach, as the construct definition and subsequent item development were based solely on the researchers’ perspective, guided by previously published evidence. The process did not incorporate input from other key stakeholders with valuable opinions on the phenomenon of medication adherence. Furthermore, these questionnaires do not incorporate the gender perspective, although sex and gender influence patients’ attitudes towards taking medication. In the context of CVD, several studies have demonstrated the impact of gender differences on adherence and disease outcomes.17,18
Questionnaire effectiveness depends on the validity of verbal information provided by respondents about their perceptions, feelings, attitudes, and behaviors, although this information is difficult to verify and translate to a measuring scale or scoring system.19 To build a robust and reliable adherence questionnaire for people with IHD, we must establish the key dimensions and a list of items that describe these dimensions. With this foundation, and after designing a draft version of the questionnaire with all the items and dimensions, we can validate the instrument to guarantee its effectiveness. The aim of this study was to identify dimensions and items associated with medication nonadherence in people with ischemic heart disease, as an initial stage in the development and validation of a questionnaire to measure medication adherence in this population, integrating the gender perspective and the opinions of professionals, researchers, and patients.
Materials and Methods
This article is part of the first phase of the GENADHECAR research project, whose protocol was published elsewhere.20
Study Design
We conducted a mixed-methods cross-sectional study in the Cardiology Department of San Juan de Alicante University Hospital and Miguel Hernández University (Spain) between January 2022 and December 2022. A visual description of the study’s mixed methods design is provided in Figure 1.
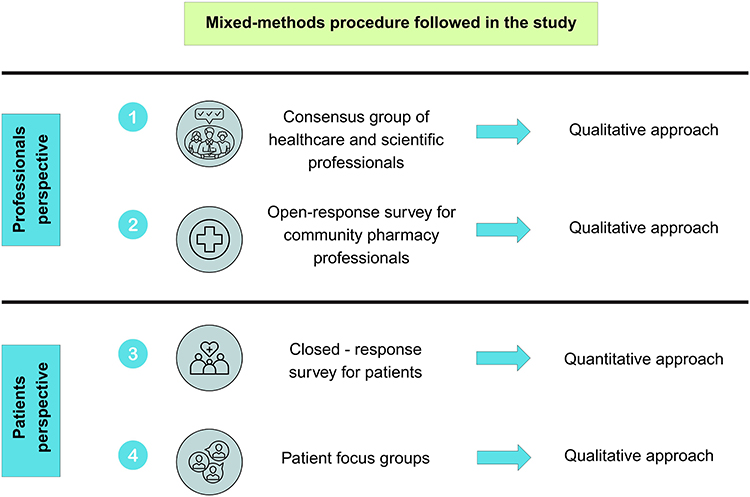 |
Figure 1 Diagram of the study’s mixed methods design. |
Population and Scope of Study
We included two types of participants: professionals from multiple disciplines (healthcare professionals and health researchers), and adults (aged ≥ 18 years) with a diagnosis of IHD who had been receiving treatment for at least one year (target population of the questionnaire) and who were managed in the Cardiology Department of San Juan de Alicante University Hospital (Spain).
Identifying Questionnaire Dimensions
Following a literature search in MEDLINE and Scopus based on the theoretical framework of medication adherence, we used qualitative and quantitative techniques to explore the perspectives of the different study participants and identify key characteristics. This process involved a consensus group of healthcare and scientific professionals, an open-response survey administered to a panel of community pharmacists, a closed-response patient survey, and patient focus groups.
Consensus Group of Healthcare and Scientific Professionals
We held an in-person meeting lasting 2.5 hours in January 2022 with a multidisciplinary panel of professionals to identify possible questionnaire dimensions, in line with the recommendations of other authors.21,22
Seven researchers with previous experience in medication adherence, five health providers (two primary care physicians, two cardiologists and one primary care nurse), one biostatistician, and one methodologist received a formal email invitation to participate in the panel. The literature offers no consensus on the appropriate number of experts to include in qualitative studies, and no established criteria to judge whether the sample size is sufficient.23 However, the sample size of professionals in our study was similar to that of previous studies.24,25
The consensus group of healthcare and scientific professionals involved five consecutive phases: 1) presenting the problem and objectives, 2) stimulating debate and exploring ideas, 3) recording the ideas raised, 4) discussing and evaluating the ideas as a group, and 5) taking consensus-based decisions (Figure 2).
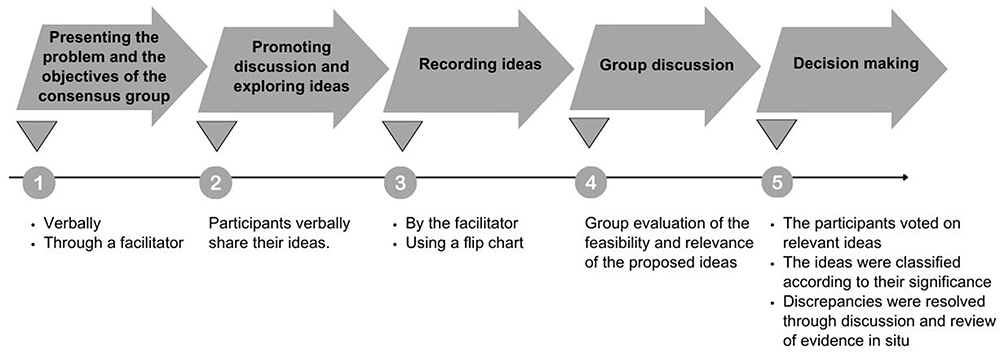 |
Figure 2 Consecutive phases of healthcare and scientific professionals consensus group. |
Open-Response Survey for Community Pharmacists
To identify the dimensions that influence medication adherence from the perspective of community pharmacists, we carried out a qualitative study using a survey with four open-response questions. Through this instrument, community pharmacists could provide their detailed opinions on medication adherence.
We included pharmacists who had at least one year of experience working in a community pharmacy and who responded to the survey before the proposed deadline. Participants were recruited using snowball sampling, a convenience sampling method suited for accessing hard-to-reach populations, in which initial participants recruit others from their social networks who meet the inclusion criteria.26 In line with this approach, we sent a formal email invitation to eligible pharmacists, requesting that they recommend other professionals who met our eligibility criteria. This non-probabilistic convenience sampling method was based on the sufficiency criterion to guarantee information integrity and quality.27
Participants were asked to answer four questions about the behavior and profile of nonadherent patients, types of treatment with low adherence, and barriers to adherence. The estimated time to complete the survey was approximately 15 to 20 minutes. They were invited to send their open responses by email within 15 days. After collecting all the responses in a single document, we identified the most repeated concepts through a manual thematic analysis; these were considered the key ideas. Figure 3 illustrates the process of participant recruitment, data collection, and data analysis.
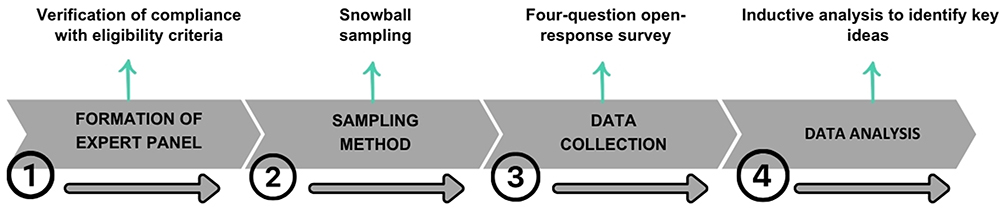 |
Figure 3 Process of recruiting community pharmacists and collecting and analyzing data. |
Closed-Response Survey for Patients
To explore IHD patients’ opinions and perceptions on the aspects with the greatest influence on medication nonadherence, we administered patient surveys in February and March 2022. With the results of this cross-sectional survey, we estimated the frequency of the phenomenon, identified differences between groups, and studied associations between key variables.28
Participants were people aged 18 years and over with a diagnosis of IHD, who had begun pharmacological treatment at least one year previously as part of secondary prevention, and who were receiving ongoing care in the Cardiology Department of San Juan de Alicante University Hospital. No formal sample size calculation was performed due to the exploratory nature of the study, and we planned to include a balanced sample of 20 men and 20 women.
We designed a survey comprising 39 closed-ended statements, based on the dimensions identified through the literature search and professional opinions (Supplementary Material S1; Spanish and English version). Survey respondents had to specify their age and sex. A 3-point Likert scale (not at all, a little, a lot) reflected the extent to which different aspects influenced medication nonadherence, according to the patients. The cardiologist consecutively invited eligible patients to participate in the study when they visited the office during the inclusion period. After receiving information about the study, patients who agreed to participate signed an informed consent form and completed the paper questionnaire. The informed consent included permission for the publication of anonymized data and contained a statement ensuring the anonymization of the participants responses. At the end of the inclusion period, we performed a descriptive analysis of the data, calculating absolute and relative frequencies for the responses to each question, stratified by sex. We then listed the statements in descending order of frequency of the “a lot” response to identify the dimensions patients considered most influential.
Patient Focus Groups
To gather further insights and identify, where appropriate, new dimensions not considered in previous steps, we performed an exploratory and phenomenological study through focus groups of men and women diagnosed with IHD. The focus group discussions took place in March and June 2022, and the results were published in January 2024.29
Defining the Item List
Initial Draft
We drafted a list of items based on the previously identified dimensions, adapting them to the target population. A psychologist revised this initial list of items to ensure they were appropriate and clear. We then revised the instrument according to international recommendations on questionnaire design, focusing on the item number and wording.21,28,30–34
Defining the Number of Items
Several authors recommend including two to three times as many items in the preliminary questionnaire as will be in the final version, to ensure the instrument is highly reliable.28,32,33 Based on these recommendations, we decided to eliminate only duplicate items (those that elicited similar information to other items) and items considered possible predictors of adherence rather than measures of adherence (eg age, sex, alcohol consumption).
Response Scales
The item list comprised items specifically designed to capture patients’ opinions and experiences. All responses were based on a 5-point Likert scale, including a neutral option to represent intermediate positions. Response options for opinion items reflected level of agreement (1. strongly agree, 2. agree, 3. neither agree nor disagree, 4. disagree, 5. strongly disagree), where number one indicates complete agreement and number five indicates complete disagreement. Response options for experience items reflected frequency (1. always, 2. usually, 3. sometimes, 4. rarely, 5. never), where number one indicates the highest level of frequency and number five the lowest level of frequency. This structure captured nuances in responses, ensuring accuracy and validity while keeping the response process simple for patients.35,36
Results
Identifying Questionnaire Dimensions
Consensus Group of Healthcare and Scientific Professionals
Seven professionals took part in the group. For the questionnaire domains, the group adopted the five risk factors for nonadherence defined by WHO. From these domains, they identified specific dimensions of medication adherence. Table 1 shows the 35 dimensions identified by healthcare and scientific professionals consensus group. Within each domain, the dimensions are ranked according to the degree of importance established by consensus.
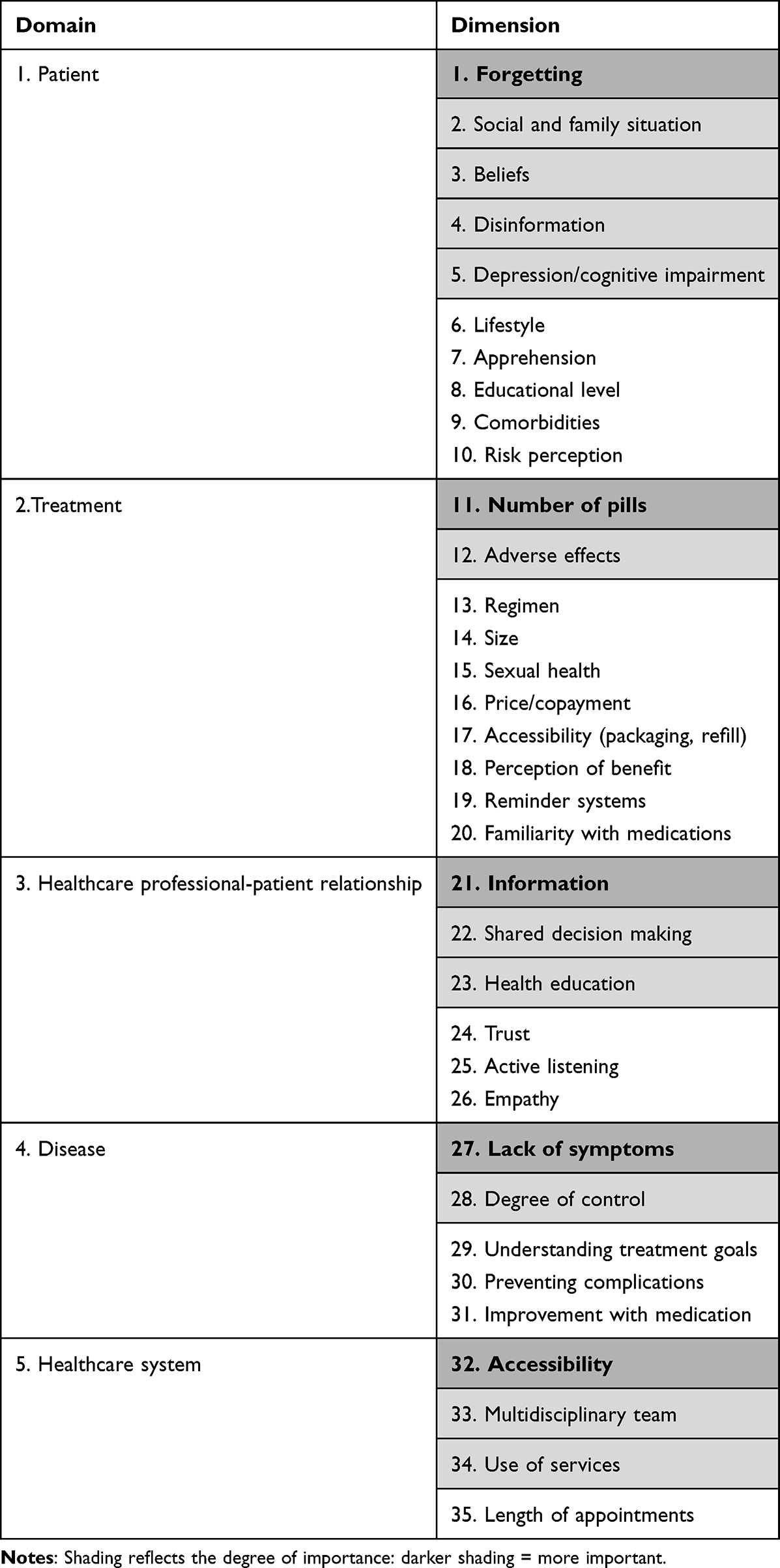 |
Table 1 Dimensions Proposed by Healthcare and Scientific Professionals Consensus Group |
According to healthcare and scientific professionals, the key dimensions of the questionnaire were: “forgetting” in the patient domain, “number of pills” in the treatment domain, “information” in the healthcare professional-patient relationship domain, “lack of symptoms” in the disease domain, and “accessibility” in the healthcare system domain. The next most important dimensions were: “social and family situation” (patient), “adverse effects” (treatment), “information” (healthcare professional-patient relationship), “degree of control” (disease), and “multidisciplinary team” (healthcare system).
Open-Response Survey for Community Pharmacists
Seven community pharmacists answered the four survey questions by email. Table 2 presents the ideas we identified after analyzing the responses. For each question, the ideas are listed in descending order according to percentage of interparticipant agreement.
 |
Table 2 Analysis of Community Pharmacists’ Responses to Four Open-Ended Questions on Medication Adherence |
According to the community pharmacists, patients with “undispensed medication” have the lowest medication adherence (five matches). The patient profile with the lowest medication adherence, according to the pharmacists, is “older people who take multiple medications” (four matches), followed by “asymptomatic patients” and patients with “cognitive impairment” (two matches). The types of medication patients are least likely to adhere to are “calcium supplements” and “maintenance inhalers” (four matches)—neither of which are IHD treatments—followed by “lipid-lowering agents” (three matches). The most common problem in adhering to treatment is “forgetting” (four matches), followed by “polypharmacy” (three matches), “lack of disease awareness” (two matches), “treatment complexity” (two matches), and “breaks from treament” (two matches). Supplementary Material S2 presents the complete responses of each pharmacist.
Closed-Response Survey for Patients
We recruited 34 patients: 20 men (58.8%) with a mean age of 70 years, and 14 women (41.2%) with a mean age of 62 years. It was not possible to recruit more women within the established period because IHD prevalence is lower among women compared with men. Nonetheless, the sex distribution was reasonably balanced.37 Only 30 participants responded to all the items (mean age 67 years, age range 41 to 97 years).
Supplementary Table S1 (responses of male patients) and Supplementary Table S2 (responses of female patients) present the survey results. The statement that most men considered influenced “a lot” in nonadherence was “I take medicines more than once a day” (statement A12; 45.0%), followed by “I don’t think I’ll suffer any complications if I stop taking my medication” (statement A30; 44.4%), and “I don’t think stopping my medication can have negative consequences for my health” (Statement A9; 42.1%). The statement that most women considered influenced “a lot” in nonadherence was “I have felt sad or depressed in the last week” (statement A8; 35.7%), followed by “I don’t notice any improvement when I take the medicines” (statement A27; 33.3%) and “I don’t think I’ll suffer any complications if I stop taking my medication” (statement A30; 33.3%).
Patient Focus Groups
The results of this qualitative study were published previously.29 A total of 12 patients (6 men and 6 women) participated in the study, which included two in-person focus groups and one remote semi-structured interview. The mean age of participants was 63.5 years, and all were Caucasian. All sessions were led by a member of the research team with extensive experience in qualitative methodology and in moderating focus groups. After inductive coding of the discourse, the emergent dimensions were, in order of number of mentions: taking medication (122 mentions), beliefs (110 mentions), lifestyle (104 mentions), healthcare professional-patient relationship (82 mentions), fear (55 mentions), symptoms (49 mentions), and perception of medications (41 mentions).
Developing the Item List
After identifying all possible dimensions that the questionnaire could include to measure medication nonadherence, we drafted an initial list of 61 items, grouped into 35 dimensions and five domains (Supplementary Material S3, Spanish and English version), based on the dimensions identified by healthcare and scientific professionals consensus group. We then applied recommendations concerning item wording and the number of items to improve the initial list. Figure 4 shows the flow of items, which we reduced to 40 after the qualitative review.
 |
Figure 4 Flowchart illustrating the qualitative review of the initial list of items: exclusion, unchanged items, reformulation, and inclusion of new items. |
Nine dimensions were removed during the qualitative review for the following reasons: 1) the items they included will be considered study variables in the second phase of this research project; 2) other dimensions had a similar meaning; or 3) the items they included were better suited to another dimension/domain. We reformulated the wording of nine dimensions to make them more coherent with the items they contained (Figure 5). Supplementary Material S4 (Spanish and English version) shows the proposed items and dimensions following the first review of the item list, as well as the response scales for each item. This revised version included five domains, 26 dimensions, and 40 items.
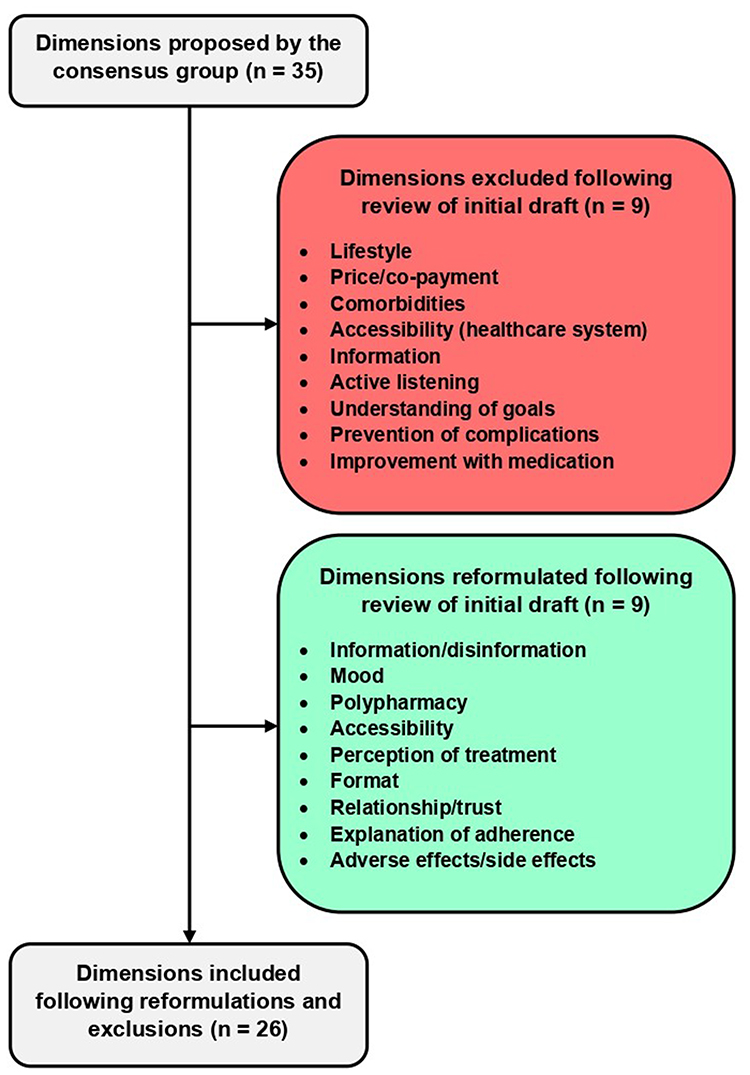 |
Figure 5 Flowchart illustrating the qualitative review of the initial list of items: exclusion and reformulation of dimensions. |
Two psychologists with experience in questionnaire construction reviewed the proposed items and response scales, and suggested modifications related to lexicon/syntax, wording, verb forms and tenses, and choice of response scale. They also suggested including a control item (item 29: “My heart disease is not dangerous for my health”; opposite of item 1) and grouping the items according to type of response scale, domain, and dimension (Supplementary Material S5, Spanish and English version). We made changes based on these recommendations. Our updated version of the item list will be considered in the questionnaire development process in the second phase of the GENADHECAR project20 (Supplementary Material S6, Spanish and English version).
Discussion
Our research team identified potential dimensions and items to be considered in the development of a medication adherence questionnaire for people with IHD, integrating individual, relational, and structural factors. These findings are based on a mixed-methods approach combining qualitative and quantitative data, which allowed us to explore the phenomenon from different angles and enrich the item development process. The results offer greater insight into the domains that influence medication adherence in this population, and in men and women separately. Taking into account the opinions of patients, multidisciplinary professionals, and researchers, we identified five domains, 26 dimensions, and 41 items, covering key and multidimensional aspects such as personal beliefs, mood, polypharmacy, disease symptoms, the patient-healthcare professional interaction, and factors related to the healthcare system.
The “patient” domain includes items that reflect personal beliefs, forgetfulness, risk perception, mood, family support, and educational level. Different studies have shown that all these factors influence medication adherence. Having a high educational level and a solid support network have been associated with better adherence,38 in line with our findings. Previous studies have highlighted the relevance of personal beliefs, which can be modified through effective health education from healthcare professionals.39,40 Another critical dimension identified in the literature and reported by professionals in our study is forgetfulness.41,42 Research has linked depression or depressive mood—common in people with IHD—with lower adherence,43 especially in people with complex regimens or who take several medications.44
The “treatment” domain includes items related to adverse effects, polypharmacy, accessibility, format, regimen, perception of treatment, reminder systems, identification, and size of the medication. Previous studies have linked the secondary effects of statins with lower adherence, especially in women.45,46 The “disease” domain includes items related to lack of symptoms and degree of disease control. A lack of symptoms has been associated with risk underestimation and low adherence,47,48 whereas good control of the disease, usually due to health education and patient motivation, has been associated with optimal adherence.49 These findings underline the importance of including the above-mentioned dimensions in an instrument for measuring adherence.
The domains “healthcare professional-patient relationship” and “healthcare system” include items about trust, explanation of adherence, shared decision making, multidisciplinary teams, length of appointments, and use of services. The literature confirms that a good relationship with professionals and sufficient health education—two aspects covered in our item list—are essential for improving adherence.49,50 Instruments such as the 8-item Morisky Medication Adherence Scale (MMAS-8),14 the Haynes-Sackett test,15 and the Adherence to Refills and Medications Scale (ARMS)51 focus on medication-taking behavior; and the Beliefs about Medicines Questionnaire (BMQ)52 focuses on patient beliefs about medications. However, adopting a holistic and integrative approach in the item list development process could facilitate the inclusion of additional factors influencing medication adherence beyond the patient’s will or attitude.
Incorporating the gender perspective into the process of identifying items and dimensions was fundamental for capturing important differences in adherence between men and women. While female participants in the closed-response survey listed depressive symptoms and difficulty attending medical appointments as key determinants of nonadherence, men considered number of daily doses, lack of symptoms, and low perception of the seriousness of the disease were more influential. In line with these observations, previous studies have reported that women usually bear a greater psychosocial burden due to imposed gender roles, which could impact their level of medication adherence.53
This item list will remain publicly available for consultation by researchers and healthcare professionals, who may use it to develop instruments for measuring medication adherence (as our team will do in the second phase of the GENADHECAR research project).20 In this way, we aim to ensure an integrative approach to the construct definition. Additionally, the proposed item list could be useful for measuring medication adherence in CVDs other than IHD, as well as in other clinical settings and populations.
This study has some limitations. First, we had difficulty recruiting female patients, although the sex distribution was reasonably balanced (around 40%/60%). Second, as the consensus group of healthcare and scientific professionals involved a face-to-face meeting, some professionals might have felt uncomfortable sharing their opinions or discussing the views of others. To address this limitation, the facilitator created a supportive environment that encouraged active participation and open dialogue. Third, in patient focus groups, there is a risk that some participants will have little knowledge or few opinions on the topics covered, which could limit the depth of the group discussion. To overcome this limitation, during the participant selection phase, we selected individuals who were best suited to address the research objective. Participants were selected by cardiologists from the research team based on their cognitive ability to participate in discussion, their willingness to share personal experiences, and their communication skills, in order to ensure rich and meaningful contributions to the group sessions. In addition, the use of purposive and convenience sampling strategies may have introduced selection bias, potentially limiting the representativeness of the participants and the generalizability of the findings. Furthermore, in the case of community pharmacists, the relatively low number of responses and the lack of thematic saturation, where only a few items were mentioned by more than one participant, may have limited the depth and completeness of the qualitative analysis. A higher participation rate could have revealed additional relevant themes or shifted the relative importance of those identified. Finally, regarding the open and closed-ended surveys administered to patients, it is possible that respondents did not always answer truthfully or did not fully understand the questions posed, leading to response bias. More specifically, in the open-ended responses, the answers may generate a large amount of data that could become unmanageable or include unnecessary information for the research objectives.
Despite its limitations, our study has several strengths. We included professionals from different disciplines, as well as researchers and patients, to achieve a broad and diverse perspective on medication adherence among people with IHD. By using a mixed-method design, we integrated as many dimensions and items as possible, facilitating a deeper understanding of medication adherence. Furthermore, by including various stakeholders with valuable opinions on medication adherence, we incorporated a wide range of perspectives on the phenomenon. This approach integrates not only the views of the individuals directly affected, but also those of healthcare providers and researchers, as medication adherence must be understood and addressed by considering the perspectives of all relevant groups.
Conclusion
With the collaboration of patients, professionals, and researchers, we potentially identified five domains, 26 dimensions, and 41 items (with 5-point Likert scale response options) associated with medication nonadherence in people with IHD. The items cover personal beliefs, mood, patient-healthcare professional interaction, and healthcare system factors, while incorporating the gender perspective.
Abbreviations
CVD, cardiovascular disease; IHD, ischemic heart disease; WHO, World Health Organization; CPP, community pharmacy professional.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the interests of confidentiality.
Ethics Approval
This study adhered to the ethical principles of the Declaration of Helsinki (1964) and was approved by the Research Ethics Committee of San Juan de Alicante University Hospital (ref. 21/037).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Health Research Projects—Strategic Action in Health (reference: PI20/01304) of the Spanish Fondo de Investigación Sanitaria—Instituto de Salud Carlos III, cofunded by the European Regional Development Fund/European Social Fund: “A Way to Make Europe/Investing in Your Future” and Spanish Ministry of Science and Innovation (MICINN) and Carlos III Health Institute (ISCIII)/European Regional Development Fund (ERDF) (RICAPPS: RD21/0016/0024). This funding source had no role in the design of the study, its execution and analyses, the interpretation of the data, or the decision to submit results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ortega Cerda JJ, Sánchez Herrera D, Rodríguez Miranda ÓA, et al. Adherencia terapéutica: un problema de atención médica. Acta méd Grupo Ángeles. 2018;6(3):226–232.
2. Vrijens B, de Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
3. Gagnon MD, Waltermaurer E, Martin A, Friedenson C, Gayle E, Hauser DL. Patient beliefs have a greater impact than barriers on medication adherence in a community health center. J Am Board Fam Med. 2017;30(3):331–336. doi:10.3122/jabfm.2017.03.160129
4. Yap AF, Thirumoorthy T, Kwan YH. Systematic review of the barriers affecting medication adherence in older adults. Geriatr Gerontol Int. 2016;16(10):1093–1101. doi:10.1111/ggi.12616
5. Pagès-Puigdemont N, Valverde-Merino I. Adherencia terapéutica: factores modificadores y estrategias de mejora [Medication adherence: modifiers and improvement strategies]. Ars Pharm. 2018;59(4):251–258. doi:10.30827/ars.v59i4.7357
6. Mubarik S, Luo L, Naeem S, et al. Epidemiology and demographic patterns of cardiovascular diseases and neoplasms deaths in Western Europe: a 1990–2019 analysis. Public Health. 2024;231:187–197. doi:10.1016/j.puhe.2024.04.003
7. Instituto Nacional de Estadística (INE) [homepage on the Internet]. Madrid: Instituto Nacional de Estadística; 2023. Available from: https://www.ine.es/dyngs/Prensa/es/pEDCM2023.htm.
8. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
9. Visseren F, Mach F, Smulders YM, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
10. Martell N. Consecuencias de la falta de adherencia sobre los resultados en salud y calidad de vida. In: Grupo OAT, Fundación Weber, editors. Libro Blanco de la Adherencia en España.
11. Parati G, Kjeldsen S, Coca A, Cushman WC, Wang J. Adherence to single-pill versus free-equivalent combination therapy in hypertension: a systematic review and meta-analysis. Hypertension. 2021;77(2):692–705. doi:10.1161/HYPERTENSIONAHA.120.15781
12. Theodoridis X, Chourdakis M, Chrysoula L, et al. Adherence to the DASH diet and risk of hypertension: a systematic review and meta-analysis. Nutrients. 2023;15(14):3261. doi:10.3390/nu15143261
13. Bingham JM, Black M, Anderson EJ, et al. Impact of telehealth interventions on medication adherence for patients with type 2 diabetes, hypertension, and/or dyslipidemia: a systematic review. Ann Pharmacother. 2021;55(5):637–649. doi:10.1177/1060028020950726
14. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
15. Sackett DL, Haynes RB, Gibson ES, Taylor DW, Roberts RS, Johnson AL. Patient compliance with antihypertensive regimens. Patient Couns Health Educ. 1978;1(1):18–21. doi:10.1016/s0738-3991(78)80033-0
16. Culig J, Leppée M. From Morisky to Hill-bone; self-reports scales for measuring adherence to medication. Coll Antropol. 2014;38(1):55–62.
17. Venditti V, Bleve E, Morano S, Filardi T. Gender-related factors in medication adherence for metabolic and cardiovascular health. Metabolites. 2023;13(10):1087. doi:10.3390/metabo13101087
18. Barrett E, Paige E, Welsh J, et al. Differences between men and women in the use of preventive medications following a major cardiovascular event: Australian prospective cohort study. Prev Med Rep. 2021:22. doi:10.1016/j.pmedr.2021.101342.
19. García de Yébenes Prous MJ, Rodríguez Salvanés F, Carmona Ortells L. Validación de cuestionarios [Validation of questionnaires]. Reumatol Clin. 2009;5(4):171–177. doi:10.1016/j.reuma.2008.09.007
20. Lopez-Pineda A, Cordero A, Nouni-García R, et al. Design and validation of a new questionnaire with a gender perspective to measure medication adherence for secondary prevention of ischaemic heart disease: study protocol. BMJ Open. 2023;13. doi:10.1136/bmjopen-2023-077982
21. Rosellini AJ, Brown TA. Developing and validating clinical questionnaires. Annu Rev Clin Psychol. 2021;17:55–81. doi:10.1146/annurev-clinpsy-081219-115343
22. Krause N. A comprehensive strategy for developing closed-ended survey items for use in studies of older adults. J Gerontol B Psychol Sci Soc Sci. 2002;57(5):S263–274. doi:10.1093/geronb/57.5.s263
23. Argimón-Pallas JM, Jiménez-Villa J. Métodos de investigación aplicados a la atención primaria de salud.
24. Carrillo I, López-Pineda A, García-Díaz S, et al. Proposals for the incorporation of the nursing role in the certification of axial spondyloarthritis units: literature review and expert consensus. Reumatol Clin. 2022;18(10):580–586. doi:10.1016/j.reumae.2021.09.004
25. Rosenberg RP, Benca R, Doghramji P, Roth T. A 2023 update on managing insomnia in primary care: insights from an expert consensus group. Prim Care Companion CNS Disord. 2023;25(1). doi:10.4088/PCC.22nr03385
26. Naderifar M, Goli H, Ghaljaie F. Snowball sampling: a purposeful method of sampling in qualitative research. Strides Dev Med Educ. 2017;14(3). doi:10.5812/sdme.67670
27. Miguel VS. Técnicas cualitativas de investigación social: Reflexión metodológica y práctica profesional.
28. Casas Anguita J, Repullo Labrador JR, Donado Campos J. La encuesta como técnica de investigación. Elaboración de cuestionarios y tratamiento estadístico de los datos (I). [The survey as a research technique. Development of questionnaires and statistical treatment of the data (I)]. Aten Primaria. 2003;31(8):527–538. doi:10.1016/S0212-6567(03)70728-8
29. Carbonell-Soliva Á, Nouni-García R, López-Pineda A, et al. Opinions and perceptions of patients with cardiovascular disease on adherence: a qualitative study of focus groups. BMC Prim Care. 2024;25(1):1–11. doi:10.1186/s12875-024-02286-8
30. Arribas MCM. Diseño y validación de cuestionarios. Formación continuada. El cuestionario es un instrumento para la recogida de información, diseñado para cuantificarla y universalizarla. [Design and validation of questionnaires. Continuing education. The questionnaire is an instrument for data collection, designed to quantify it and universalize it]. Matronas Profesión. 2004;5(17):23–29.
31. Jones TL, Baxter M, Khanduja V. A quick guide to survey research. Ann R Coll Surg Engl. 2013;95(1):5–7. doi:10.1308/003588413X13511609956372
32. Clark LA, Watson D. Constructing validity: new developments in creating objective measuring instruments. Psychol Assess. 2019;31(12):1412–1427. doi:10.1037/pas0000626
33. Argimon JM, Jiménez J. Métodos de investigación clínica y epidemiológica.
34. Vallejo PM. Guía para construir cuestionarios y escalas de actitudes. [Guide to constructing questionnaires and attitude scales]. Universidad Rafael Landívar, Facultad de Humanidades CINDEG; 2011. Available from: http://www.upcomillas.es/personal/peter/otrosdocumentos/Guiaparaconstruirescalasdeactitudes.pdf.
35. Simms LJ, Zelazny K, Williams TF, Bernstein L. Does the number of response options matter? Psychometric perspectives using personality questionnaire data. Psychol Assess. 2019;31(4):557–566. doi:10.1037/pas0000648
36. Preston CC, Colman AM. Optimal number of response categories in rating scales: reliability, validity, discriminating power, and respondent preferences. Acta Psychologica. 2000;104(1):1–15. doi:10.1016/S0001-6918(99)00050-5
37. Lucas-Domínguez R, Aragonés González M, Sixto-Costoya A, Ruiz-Martínez E, Alonso-Arroyo A, Valderrama-Zurián JC. The inclusion of the gender perspective in oncology research with Spanish participation. Heliyon. 2024;10(9):e30043. doi:10.1016/j.heliyon.2024.e30043
38. Desai NR, Farbaniec M, Karalis DG. Nonadherence to lipid-lowering therapy and strategies to improve adherence in patients with atherosclerotic cardiovascular disease. Clin Cardiol. 2023;46(1):13–21. doi:10.1002/clc.23935
39. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687–1698. doi:10.2147/PPA.S169236
40. Shahin W, Kennedy GA, Stupans I. The consequences of general medication beliefs measured by the Beliefs about Medicine Questionnaire on medication adherence: a systematic review. Pharmacy. 2020;8(3):147. doi:10.3390/pharmacy8030147
41. Krishnamoorthy Y, Rajaa S, Rehman T, Thulasingam M. Patient and provider’s perspective on barriers and facilitators for medication adherence among adult patients with cardiovascular diseases and diabetes mellitus in India: a qualitative evidence synthesis. BMJ Open. 2022;12(3):e055226. doi:10.1136/bmjopen-2021-055226.3
42. Pokharel P, Jha SK, Adhikari A, et al. Non-adherence to anti-hypertensive medications in a low-resource country Nepal: a systematic review and meta-analysis. Ann Med Surg. 2023;85(9):4520–4530. doi:10.1097/MS9.0000000000001088
43. Gold SM, Köhler-Forsberg O, Moss-Morris R, et al. Comorbid depression in medical diseases. Nat Rev Dis Primers. 2020;6(1):69. doi:10.1038/s41572-020-0200-2
44. Srithumsuk W, Chaleoykitti S, Jaipong S, Pattayakorn P, Podimuang K. Association between depression and medication adherence in stroke survivor older adults. Jpn J Nurs Sci. 2021;18(4). doi:10.1111/jjns.12434
45. Hope HF, Binkley GM, Fenton S, Kitas GD, Verstappen SMM, Symmons DPM. Systematic review of the predictors of statin adherence for the primary prevention of cardiovascular disease. PLoS One. 2019;14(1):e0201196. doi:10.1371/journal.pone.0201196
46. Ju A, Hanson CS, Banks E, et al. Patient beliefs and attitudes to taking statins: systematic review of qualitative studies. Br J Gen Pract. 2018;68(671):e408–e419. doi:10.3399/bjgp18X696365
47. Dalal JJ, Kerkar P, Guha S, et al. Therapeutic adherence in hypertension: current evidence and expert opinion from India. Indian Heart J. 2021;73(6):667–673. doi:10.1016/j.ihj.2021.10.007
48. Kvarnstrom K, Airaksinen M, Liira H. Barriers and facilitators to medication adherence: a qualitative study with general practitioners. BMJ Open. 2018;8(1):e015332. doi:10.1136/bmjopen-2017-019377
49. Purcell DJ, Cavanaugh G, Thomas-Purcell KB, et al. e-Health literacy scale, patient attitudes, medication adherence, and internal locus of control. Health Lit Res Pract. 2023;7(2):80–88. doi:10.3928/24748307-20230411-01
50. Gast A, Mathes T. Medication adherence influencing factors-an (updated) overview of systematic reviews. Syst Rev. 2019;8(1):112. doi:10.1186/s13643-019-1014-8
51. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the Adherence to Refills and Medications Scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118–123. doi:10.1111/j.1524-4733.2008.00437.x
52. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
53. Boyd A, van de Velde S, Vilagut G, et al. Gender differences in mental disorders and suicidality in Europe: results from a large cross-sectional population-based study. J Affect Disord. 2015;173:245–254. doi:10.1016/j.jad.2014.10.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.