Back to Journals » International Journal of Women's Health » Volume 18
Hysteroscopic Cold Knife Separation Combined with Autologous Platelet Rich Plasma for the Treatment of Intrauterine Adhesions: A Comparative Study
Authors Li H, Rong Y, Li Y, Wang X
Received 24 June 2025
Accepted for publication 24 January 2026
Published 25 February 2026 Volume 2026:18 549334
DOI https://doi.org/10.2147/IJWH.S549334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Haiyan Li,1 Yajun Rong2 ,† Yanan Li,3 Xiaojing Wang3
1Department of Gynecology, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050011, People’s Republic of China; 2Department of Gastrointestinal Surgery, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050011, People’s Republic of China; 3Department of Traditional Chinese Medicine, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050011, People’s Republic of China
†Dr Yajun Rong passed away on August 22, 2025
Correspondence: Xiaojing Wang, Department of Traditional Chinese Medicine, Shijiazhuang People’s Hospital, No. 11, Hefang Street, Chang’an District, Shijiazhuang, Hebei, 050011, People’s Republic of China, Email [email protected]
Objective: To investigate the preliminary effect of hysteroscopic cold knife separation combined with autologous platelet rich plasma (PRP) in the treatment of intrauterine adhesions (IUA) and prevention of postoperative re-adhesions.
Methods: Retrospectively, 110 patients with IUA treated in our hospital during January 2022 to January 2024 were selected for the study, and divided into 58 cases in the cold knife + PRP group and 52 cases in the cold knife group. Clinical outcomes, surgical parameters, sex hormone levels [estradiol (E2), luteinizing hormone (LH), follicle-stimulating hormone (FSH)], inflammatory markers [C-reactive protein (CRP), matrix metalloproteinase-9 (MMP-9), interleukin-8 (IL-8), interleukin-6 (IL-6)], and postoperative re-adhesion rates were compared between two groups.
Results: The cold knife + PRP group had much higher total efficacy rate of 91.88% than 75.00% in the Cold Knife group (P < 0.05). The cold knife + PRP group had less uterine distention medium absorption and intraoperative blood loss and shorter operative duration and hospitalization time than the cold knife group (P < 0.05). Higher levels of E2 but lower levels of LH and FSH were observed in the cold knife + PRP group than the cold knife group (P < 0.05). After the treatment, the cold knife + PRP group had lower levels of CRP, IL-8 and IL-6 but higher level of MMP-9 than the cold knife group (P < 0.05). The re-adhesion rate at 1, 6, and 12 months postoperatively was significantly lower in the cold knife + PRP group than the cold knife group (P < 0.05).
Conclusion: In this preliminary study, hysteroscopic cold knife dissection combined with PRP showed a trend toward regulating sex hormone levels, mitigating inflammatory responses, and reducing re-adhesion incidence in IUA patients, suggesting its potential as a therapeutic option. However, larger-scale studies are needed to confirm these findings.
Keywords: hysteroscopic cold knife dissection, platelet-rich plasma, uterine adhesion, prevention
Introduction
Intrauterine adhesions (IUA) are a common gynecological disease, usually the pathological result of fibrosis repair after damage to the basal layer of the endometrium. The clinical manifestations of IUA include menstrual abnormalities, infertility, and recurrent miscarriage.1 Epidemiological studies2 have shown that approximately 53.5% of IUA are caused by intrauterine procedures such as induced abortion. The recurrence rate of severe IUA patients after surgery is still as high as 62.5%, and the pregnancy rate is less than 33%, which seriously threatens women’s reproductive health. Hysteroscopic transcervical resection of adhesion (TCRA) is considered as the current gold standard for treatment, but the thermal injury effect of traditional electrocautery may exacerbate the damage to the basal layer of the endometrium, leading to a higher rate of postoperative re-adhesion.3
In recent years, hysteroscopic cold knife technology has gradually become a new choice for the treatment of moderate to severe adhesions due to its advantages of no thermal damage and precise protection of residual endometrium. Research shows that the postoperative re-adhesion rate of hysteroscopic cold knife technology can be reduced to 6.45%, significantly better than traditional electrocautery.4 However, simple surgical intervention is still unable to completely reverse the fibrosis process of the endometrium, so postoperative use of bioactive materials and regenerative medicine methods should be combined to further promote endometrial repair. Autologous platelet-rich plasma (PRP), as a regenerative medicine therapy, releases over 20 active ingredients including vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF) through high concentrations of platelets, effectively activating the proliferation of endometrial stem cells, inhibiting fibrosis pathways, and reshaping the uterine microenvironment.5 Clinical studies have shown that6 PRP intrauterine perfusion can significantly improve endometrial thickness (from 4 mm to 6–8 mm) and increase pregnancy rates to 60%. However, current research mostly focuses on the efficacy evaluation of a single technique (cold knife or PRP), and there is a lack of systematic clinical evaluation of the synergistic effect of the two. Given the complementary role of cold knife and PRP in theory, the cold knife can precisely remove adhesions and avoid thermal damage, while PRP can promote postoperative endometrial regeneration and anti-fibrosis. The combined application of the two becomes a promising treatment strategy.7 However, there is currently a lack of systematic comparative studies on the individual application and combined efficacy of cold knife and PRP.
Therefore, this study aims to preliminarily explore the effect of hysteroscopic cold knife dissection combined with PRP in the treatment of IUA through retrospective analysis, and compare it with cold knife treatment alone, in order to provide preliminary data and references for subsequent more comprehensive randomized controlled studies involving multiple groups (cold knife alone, PRP alone, and combined treatment).
Materials and Methods
Research Design and Quality Control
This study was a single-center, retrospective cohort study, aiming to evaluate the difference in efficacy between hysteroscopic cold knife dissection combined with autologous platelet-rich plasma (PRP) and hysteroscopic cold knife dissection alone in the treatment of IUA. All clinical data were retrospectively collected from the medical record system of our hospital from January 2022 to January 2024. To ensure the accuracy and comparability of the retrospective data as much as possible, the following quality control measures were implemented in this study: 1) The data were independently extracted from the electronic medical record system by two trained researchers, and cross-checked. Any discrepancies were adjudicated by a third researcher. 2) All the diagnostic records, surgical records, and key laboratory indicators (such as sex hormones and inflammatory factors) of the included cases must be complete. Those with missing key data were excluded (Figure 1) The procedures for PRP preparation, surgical operation, and postoperative follow-up all follow the established standard operating procedures (SOP) of our hospital to minimize variations among operators.
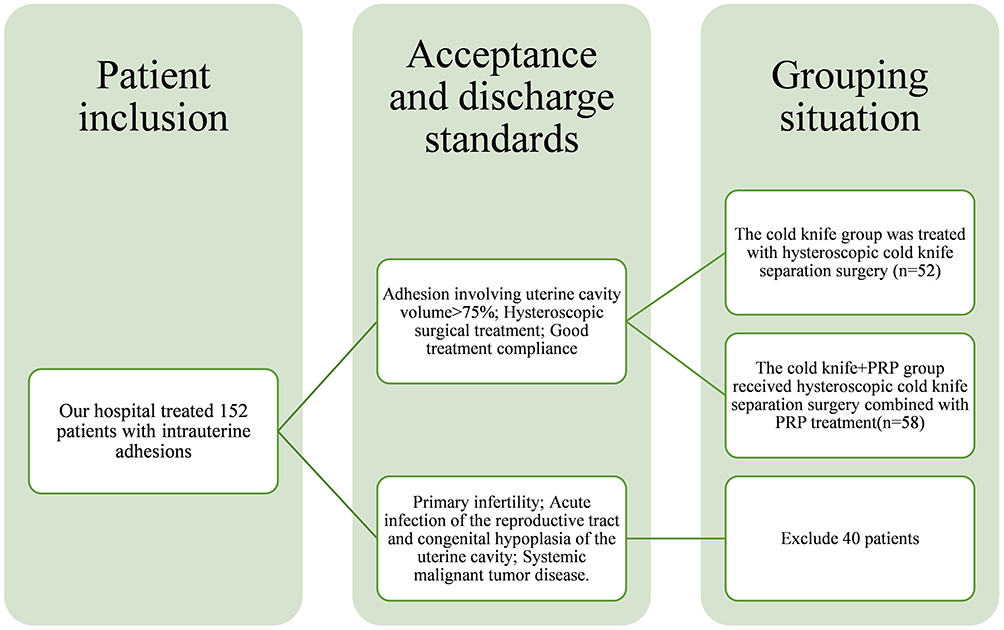 |
Figure 1 Process diagram for patient inclusion. |
Research Subjects and Groupings
A total of 110 patients with IUA treated in our hospital during January 2022 to January 2024 were retrospectively selected for the study and were grouped based on the actual treatment plans they received in clinical practice: the cold knife + PRP group (n = 58): received hysteroscopic cold knife dissection combined with postoperative uterine cavity PRP perfusion; the cold knife group (n = 52): only received hysteroscopic cold knife dissection. The inclusion process of patients was shown in Figure 1. This study was ratified by the Ethics Committee of our hospital.
Sample size calculation explanation: the sample size was estimated based on the primary outcome measure of this study (re-adhesion rate at 12 months after surgery). Based on previous studies,7 it was assumed that the re-adhesion rate of the cold knife group was 30% and that of the cold knife + PRP group was 10%. With α = 0.05 and β = 0.20 set, using the PASS15.0 software for calculation. The minimum required sample size for each group was 45 cases. Considering the cases of follow-up dropout and data missing, the sample size was set as 20%. Eventually, 110 cases were included, which met the sample size requirements for a retrospective intervention study.
Inclusion criteria: (1) Patients met the diagnostic criteria for IUA,8 with adhesions involving more than 75% of the uterine cavity volume; (2) The patient met the indications for surgical treatment in this study (Infertility or oligo-menorrhea patients with strong fertility desire but suffer from IUA due to endometrial damage; Patients with clinical symptoms such as bleeding, pain, amenorrhea, and infertility caused by adhesions of the cervical canal or uterine cavity due to endometrial injury), and received hysteroscopic surgical treatment; (3) Patients with good treatment compliance; (4) Patients with complete clinical data. Exclusion criteria: (1) Patients with primary infertility; (2) Patients with acute infections of the reproductive tract and congenital hypoplasia of the uterine cavity; (3) Patients with menstrual abnormalities caused by other factors; (4) Patients with combined malignant tumor diseases of other systems.
Methods
Cold knife group: Patients underwent hysteroscopic cold knife separation surgery. After general anesthesia, the patient’s cervix was dilated to size 7 using a Hegar dilation rod. Under hysteroscopic guidance, a cold knife (Brand: Storz, Model: 3 mm miniature scissors) was used to remove adhered tissue and restore the anatomical shape of the uterine cavity. After surgery, routine placement of balloon catheter compression hemostasis was performed, and oral administration of estradiol valerate (2 mg bid × 21 days) and progesterone acetate (10 mg bid × 10 days) was administered without PRP perfusion.
Cold knife + PRP group: Patients underwent hysteroscopic cold knife separation surgery combined with PRP treatment. (1) The preparation process of PRP: 20–30 mL of peripheral venous blood was collected from patients using pre-infused anticoagulant (ACD-A) blood collection bags. The collected whole blood was transferred to a medical centrifuge cup and subjected to gradient centrifugation at 5500 rpm for 15 minutes. The upper layer of pale yellow liquid was obtained through professional operation, resulting in a final volume of 5–8 mL of PRP. The entire process from blood collection to PRP preparation was controlled within 30 minutes, and immediately used for uterine cavity perfusion after preparation to ensure platelet activity. Laboratory tests had shown that the platelet concentration of this product could reach 3–5 times the baseline value (1157.8 ± 271.7 × 109/L), and it contained a high concentration of transforming growth factor-β (TGF-β) of 90.9 ± 17.8 ug/L, meeting clinical application standards.9 During the PRP preparation process of this study, the baseline of platelet concentration in whole blood was (256.4 ± 58.3) × 109/L, and the TGF-β concentration was (22.5 ± 4.1) ug/L. This process strictly followed aseptic operation standards, and the temperature was controlled at 20–24°C throughout the entire process. The time limit for each step was controlled within 30 minutes to ensure platelet activity.
Surgical procedure and PRP perfusion process: The patient underwent bladder lithotomy and received intravenous general anesthesia. A Hegar cervical dilation rod (model: Hegar) was adopted to dilate the cervical opening to size 7 and uterine pressure was maintained within the range of 100–150 mmHg through a physiological saline circulation perfusion system. Under hysteroscopic guidance, the same brand (Storz) 3 mm surgical scissor was inserted into the uterus through the instrument hole to remove adhesions. The exposure of bilateral fallopian tube openings was confirmed to restore the normal anatomical shape of the uterine cavity. The prepared PRP was inhaled into a disposable sterile syringe. Before perfusion, the uterine cavity was gently rinsed by with 3–5 mL of sterile normal saline to remove accumulated blood and mucus. To prevent residual PRP in the uterine cavity after surgery, the prepared PRP was inhaled into a sterile syringe and injected into the uterine cavity through a perfusion tube. The method of “slowly withdrawing the tube while evenly pushing” (approximately 1 mL/min) was used to ensure that PRP formed a wide and uniform coating layer along the endometrial wound of the uterine wall, avoiding local accumulation. After the injection was completed, the patient was immediately adjusted to a low-head and high-hip position (about 15–20°), and this position was maintained for 15–20 minutes. This measure aimed to utilize the force of gravity to facilitate the downward (toward the fundus and lateral wall) PRP with gel characteristics to fully cover and infiltrate the wound surface of endometrium, maximizing the contact area and time between bioactive components and the repair target, and at the same time promoting a small amount of excess liquid to flow naturally to the cervical opening. During the maintenance of the above position, a small amount of excess PRP mixture that had not been adsorbed by the endometrium was allowed to naturally flow out of the body through the cervical canal without the routine use of balloon occlusion of the cervical opening, effectively preventing abnormal retention of intrauterine fluid (including PRP).
Both groups were orally administered 2 mg of estradiol valerate (purchased from Peking Union Medical College Pharmaceutical Co., Ltd., specification 0.5 mg, product standard No. H20000031) twice a day for 21 days after surgery. After 10 days of oral administration of estradiol valerate, 10 mg of levonorgestrel (purchased from Yangzhou Aoruite Pharmaceutical Co., Ltd., specification 10 mg, product standard No. H20233769) was added orally, twice a day.
Outcome Measures
Clinical efficacy: The American Fertility Society (AFS) IUA scoring system10 was used to evaluate the clinical efficacy of the two groups after treatment. Significantly effective: Under hysteroscopy, the bilateral fallopian tube openings were clearly visible, the uterine cavity contour was intact, and the area of IUA was reduced by ≥80%; Effective: The overall shape of the uterine cavity had been basically restored, and the area of adhesions in the uterine cavity had been reduced by 50%–79%; Invalid: There was no improvement in the shape of the uterine cavity, or new adhesions appeared. The area of adhesions in the uterine cavity decreased by less than 50%, or even increased. Total effective rate = number of (Significantly effective + effective) cases/total number of cases × 100%.
Surgical indicators: The surgical indicators of two groups were evaluated. The amount of uterine distention medium absorbed, intraoperative bleeding, operation time, and hospital stay were recorded.
Sex hormone indicators: The sex hormone indicators before and after treatment in two groups were evaluated, including estradiol (E2), luteinizing hormone (LH), and follicle stimulating hormone (FSH). About 5 mL of fasting venous blood was collected from patients 1 day before and 1 day after treatment and was centrifuged at 4000 r/min to separate the supernatant. Enzyme-linked immunosorbent assay (ELISA) was used to detect E2, LH, and FSH levels. All operations were strictly carried out according to the instructions in a specific environment, and all reagent kits were purchased from Shanghai Jianglai Biotechnology Co., Ltd.
Inflammatory indicators: the inflammatory indicators before and after treatment in two groups were evaluated, including C-reactive protein (CRP), matrix metalloproteinase-9 (MMP-9), interleukin-8 (IL-8), and interleukin-6 (IL-6). About 5 mL of fasting venous blood was collected from the patient and was centrifuged at 4000r/min to separate the supernatant. ELISA assay was conducted as follows. After diluted as needed, 50 μL sample or standard was added to the microplate. The microplate was sealed and incubated at 37°C in the dark for 1 hour. After incubation, the liquid was discarded and the microplate was patted dry with absorbent paper. Then, 350 μL of washing solution was added to each well, stood for 1 minute and shook dry. The microplate was washed 5 times repeatedly and patted dry after each wash. About 50 μL enzyme conjugate was added to each well and incubated at room temperature in the dark for 1 hour. After incubation, the liquid was discarded and the microplate was patted dry with absorbent paper. Then, 350 μL of washing solution was added to each well, stood for 1 minute and shook dry. The microplate was washed 5 times repeatedly and patted dry after each wash. About 50 μL of substrate solution was added to each well and incubated in the dark for 15 minutes. Then, 50 μL of termination solution was added and the reaction was immediately terminated. The absorbance (OD value) of each well was measured using an ELISA reader at a wavelength of 450 nm. The concentrations of CRP, MMP-9, IL-8, and IL-6 in the sample were calculated based on the standard curve. The CRP kit was purchased from Shenggong Bioengineering (Shanghai) Co., Ltd., item number: 20160812. The MMP-9 kit was purchased from Ruixin Biotechnology Co., Ltd., item number: RX900314M. IL-8 assay kit from Guangzhou Sijia Biotechnology Co., Ltd., item number: 20171106B. IL-6 assay kit from Abbey Company, USA, item number: ab178013.
The occurrence of re-adhesion: the occurrence of re-adhesion was evaluated at 1 month, 3 months, 6 months, and 12 months after treatment in both groups. The patient underwent hysteroscopy examination to observe whether there was any newly added adhesive tissue in the uterine cavity, whether the original adhesive site had closed again, or whether fibrous scar tissue had appeared. Among them, under hysteroscopy, membrane like, fibrous cord like, or muscular adhesive tissue could be seen in the original surgical area, resulting in partial or complete occlusion of the uterine cavity and obstruction or inability to expose the opening of the fallopian tube, which was judged as re-adhesion. The total incidence of re-adhesions = actual total number of re-adhesions/total number of cases × 100%.
Statistical Analysis
Statistical analysis was conducted using SPSS 27.0. The measurement data that conformed to normal distribution were represented by ( ). Paired sample t-test was used for comparison between different time points between groups and independent sample t-test was used for comparison between groups. The measurement data was represented as [cases (%)], and the comparison between groups was tested using χ2 or Fisher’s exact probability method. P < 0.05 was considered statistically significant.
). Paired sample t-test was used for comparison between different time points between groups and independent sample t-test was used for comparison between groups. The measurement data was represented as [cases (%)], and the comparison between groups was tested using χ2 or Fisher’s exact probability method. P < 0.05 was considered statistically significant.
Results
Comparison of General Information
There was no statistically significant difference between the two groups of general information (age, disease duration, and cause of onset) (P > 0.05, Table 1).
 |
Table 1 Comparison of General Information [Cases (%)] |
Comparison of Clinical Efficacy
The cold knife + PRP group had much higher total efficacy rate of 91.88% than 75.00% in the Cold Knife group (P < 0.05, Table 2 and Figure 2).
 |
Table 2 Comparison of Clinical Efficacy [Cases (%)] |
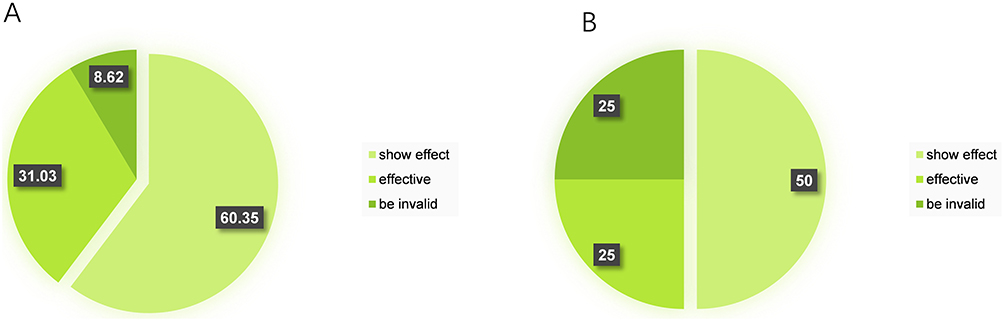 |
Figure 2 Comparison of clinical efficacy distribution. (A) Cold knife + PRP group; (B) Cold knife group. |
Comparison of Surgical Indicators
The cold knife + PRP group had less uterine distention medium absorption volume and intraoperative blood loss and shorter operative duration and hospitalization time than the cold knife group (P < 0.05, Table 3).
 |
Table 3 Comparison of Two Surgical Indicators |
Comparison of Sex Hormone Indicators
There was no statistically significant difference in the levels of sex hormones (E2, LH, FSH) between the two groups before intervention (P > 0.05). Compared with before intervention, the E2 levels in both groups showed an upward trend after treatment, and the cold knife + PRP group had significantly higher E2 levels than the cold knife group (P < 0.05). After treatment, both groups showed a decreasing trend in LH and FSH levels, and the cold knife + CRP group had significantly lower LH and FSH levels than the cold knife group (P < 0.05, Table 4 and Figure 3).
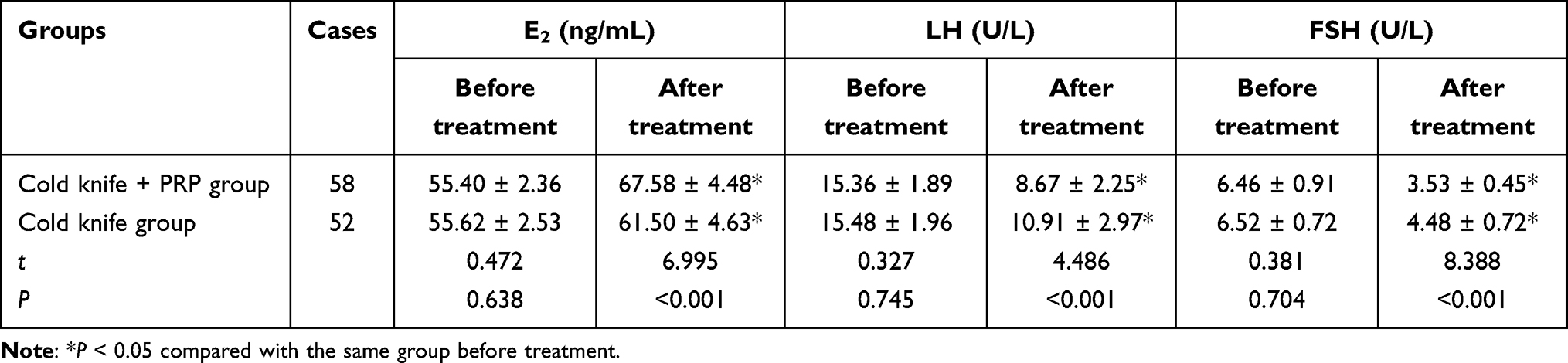 |
Table 4 Comparison of Sex Hormone Indicators |
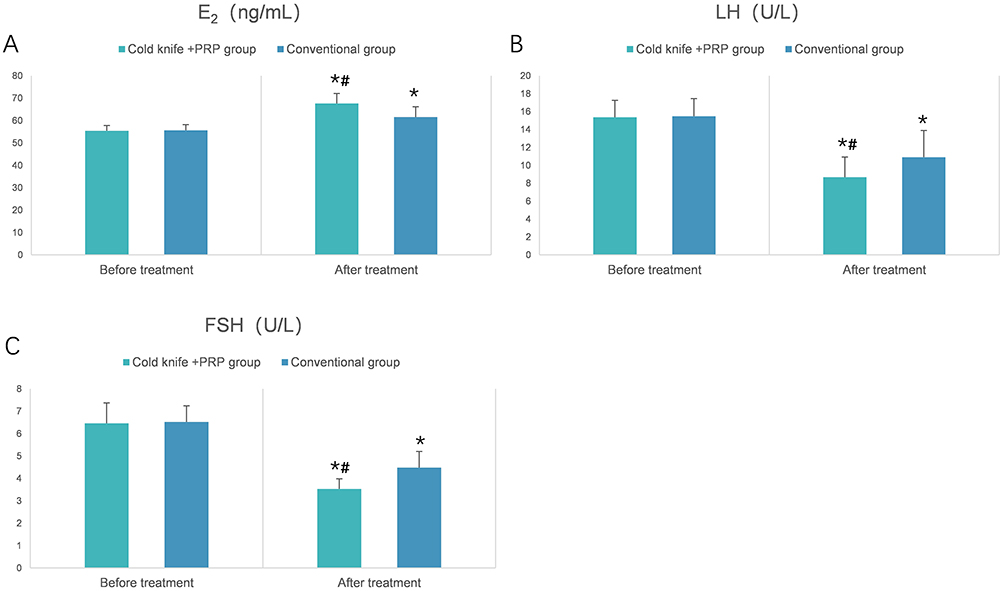 |
Figure 3 Comparison of hormone levels. (A) Comparison of E2 levels; (B) Comparison of LH levels; (C) Comparison of FSH levels. Note: *P < 0.05 compared with the same group before treatment; #P < 0.05 compared with the cold knife group after treatment. |
Comparison of Inflammatory Indicators
There was no statistically significant difference in the inflammatory indicators (CRP, MMP-9, IL-8, and IL-6) between the two groups before intervention (P > 0.05). After the treatment, inflammatory markers (CRP, IL-8, IL-6, MMP-9) were increased in both groups. At the same time, the cold knife + PRP group had lower levels of CRP, IL-8 and IL-6 and higher level of MMP-9 than the cold knife group (P < 0.05, Table 5).
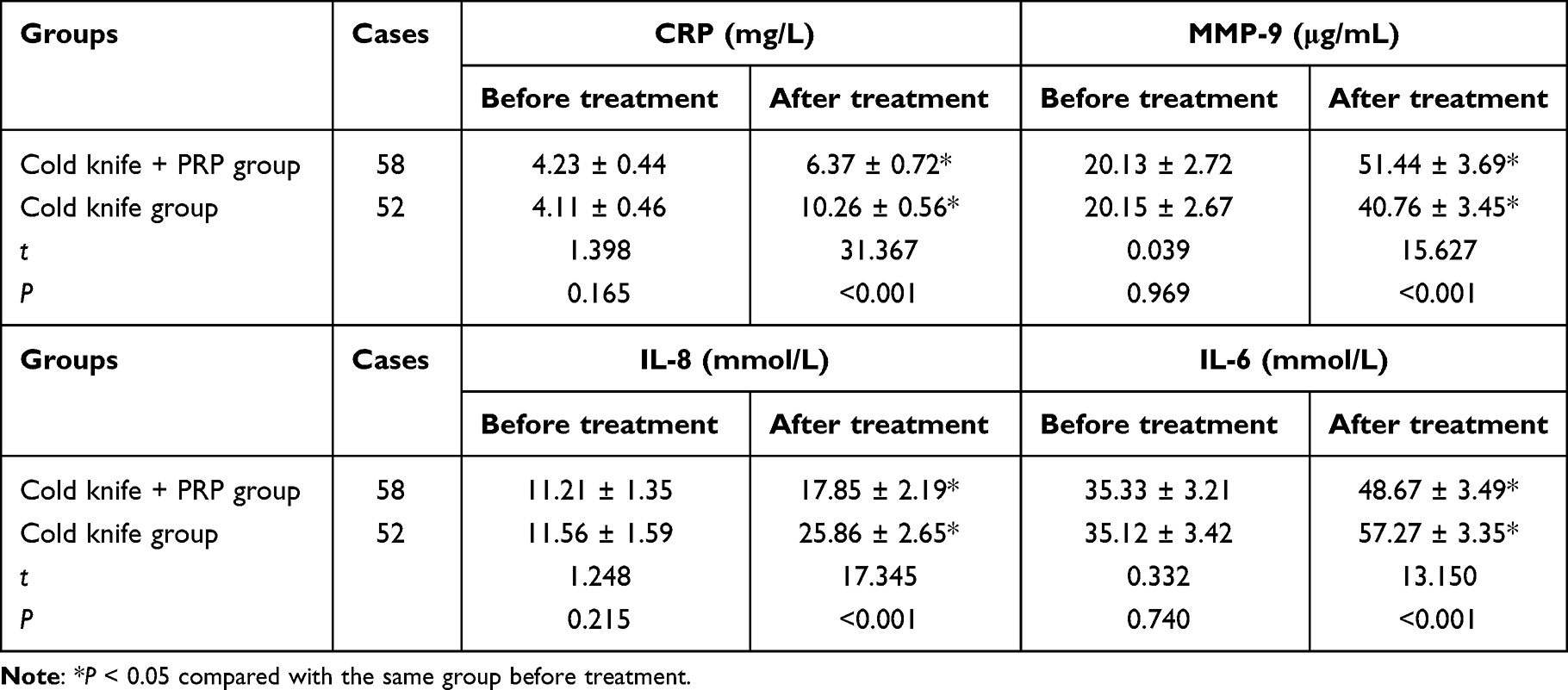 |
Table 5 Comparison of Inflammatory Indicators |
Comparison of Re-Adhesion Incidence
The re-adhesion rates of the cold knife + PRP group at various time points after surgery were 0% (0/58), 1.72% (1/58), 3.45% (2/58), and 5.17% (3/58), respectively, with no significant trend over time within the group (P = 0.213). The re-adhesion rate of the cold knife group showed an increasing trend over time, with values of 7.69% (4/52), 9.62% (5/52), 15.38% (8/52), and 17.31% (9/52), respectively, with significant differences within the group (P = 0.048). The re-adhesion rate at 1, 6, and 12 months postoperatively was significantly lower in the cold knife + PRP group than the cold knife group (P < 0.05, Table 6).
 |
Table 6 Comparison of Re-Adhesion Incidence [Cases (%)] |
Comparison of the Absolute Changes in Various Indicators
To further verify the degree of difference in the therapeutic effects between the two groups, the absolute change values of each indicator before and after treatment (post-treatment indicator value − pre-treatment indicator value) were calculated, and comparisons were made between the groups. The results showed that in terms of the absolute changes in indicators related to sex hormone regulation and inflammatory response improvement, the cold knife + PRP group had statistically significant differences compared to the cold knife group (P < 0.001), and the change trend was highly consistent with the research conclusion (Table 7).
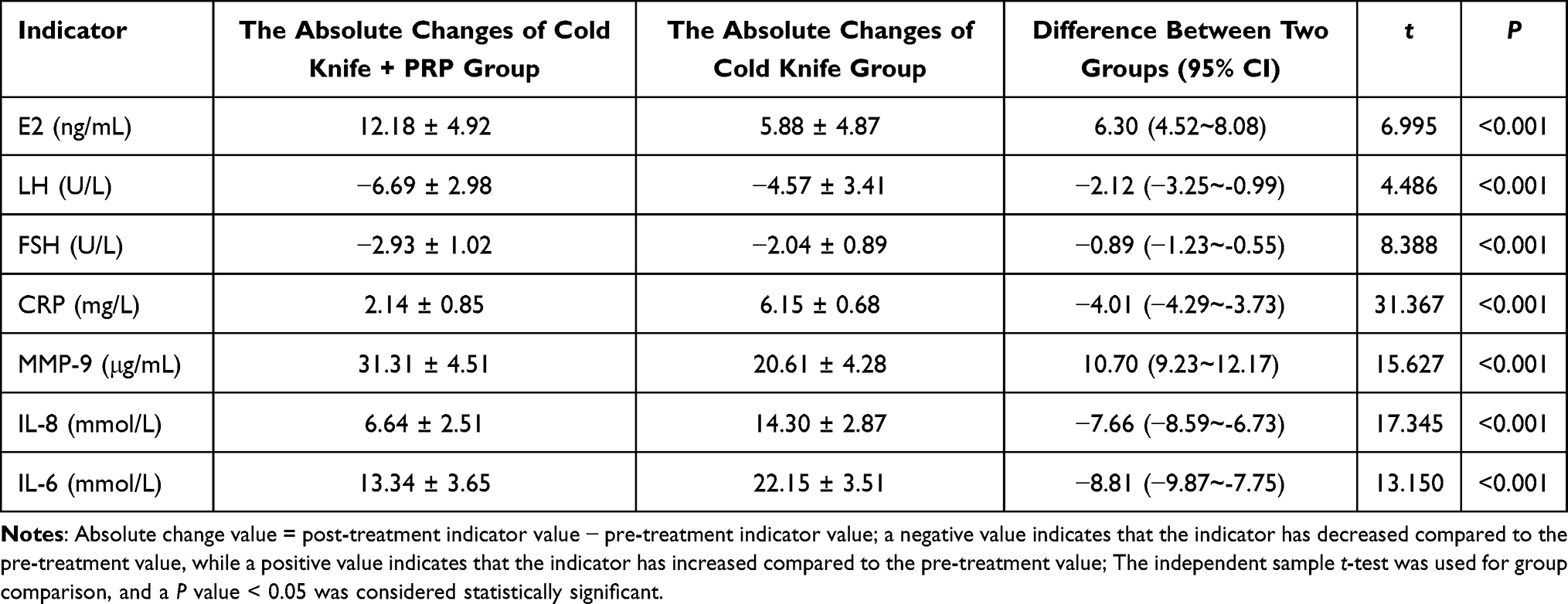 |
Table 7 Comparison of the Absolute Changes in Various Indicators |
Discussion
IUA is a common complication in gynecology, and its main pathological mechanism lies in the abnormal fibrotic repair process that occurs after damage to the basal layer of the endometrium. Epidemiological data shows that iatrogenic procedures such as induced abortion accounts for 53.5% of the pathogenic factors of IUA. The postoperative recurrence rate of severe IUA patients is as high as 62.5%, and the pregnancy success rate is less than one-third, seriously threatening women’s reproductive health.11 Although traditional hysteroscopic resection is considered the gold standard for treatment, its thermal injury effect may further damage residual endometrial basal layer cells, resulting in a postoperative re-adhesion incidence of approximately 35%–40%.12 This study found that compared with the total effective rate of 75.00% in the cold knife group, the combination of cold knife technology and PRP treatment significantly improved the total effective rate of IUA patients, reaching 91.88%. This advantage may be related to the synergistic effect of the two technologies. Cold knife instruments use mechanical cutting without using electrical energy, thus avoiding damage to the endometrium caused by electric heating, helping to reduce the occurrence of postoperative IUA, and protecting the patient’s fertility. At the same time, high concentrations of growth factors such as VEGF and FGF in PRP activate the proliferation of endometrial stem cells and inhibit the fibrosis process mediated by TGF-β.13 Compared to a single treatment strategy, the combination of cold knife technology and PRP treatment effectively maintains the integrity of the uterine cavity and provides a new treatment approach for improving the fertility prognosis of patients.
This study found that the cold knife together PRP group had less absorption volume of uterine distention medium and shorter surgery and hospitalization time than the cold knife group. This indicated that cold knife separation combined with PRP treatment had a better promoting effect on the recovery of uterine cavity morphology, with smaller surgical trauma. This might be related to the “single cut-synchronous hemostasis” technology of the cold knife system. When cutting adhesions with micro scissors, the built-in negative pressure suction device can synchronously remove bleeding from the wound, avoiding multiple hemostasis operations.14 PRP contains multiple growth factors. Among them, abnormally elevated levels of TGF-β can induce phenotypic transformation from fibroblasts to myofibroblasts, drive abnormal deposition of extracellular matrix, promote the progression of endometrial fibrosis, and enhance vascular wall stability.15 The combination of cold knife separation and PRP had a synergistic effect, significantly improving the clinical efficacy of patients. Sharon A et al16 found that hysteroscopic cold knife dissection could improve the postoperative recurrence rate of endometrial polyp patients, reduce postoperative vaginal bleeding time, and improve clinical efficacy. Although the research subjects are different (this study aimed on IUA patients), they all indicated that hysteroscopic cold knife separation surgery had similar clinical efficacy in different diseases, providing a basis for its widespread application. This study found that, compared with the cold knife group, the E2 level in the cold knife + PRP group was significantly higher, while the LH and FSH levels were significantly lower, indicating that hysteroscopic cold knife separation combined with PRP treatment effectively improved the sex hormone levels of IUA patients and controlled disease progression. The technical core of hysteroscopic cold knife separation lies in the physical mechanism without thermal radiation effect, which can accurately avoid accidental damage to surrounding normal tissues caused by thermal injury and promote the epithelialization of the remaining basal layer of the endometrium. Through the neuroendocrine regulation of the hypothalamic pituitary ovarian axis, it can effectively improve normal ovarian function and enhance the sensitivity of the endometrium to sex hormones.17 Intrauterine infusion of PRP can deliver PRP into the uterine cavity, thereby releasing VEGF, directly promoting angiogenesis and cell proliferation, accelerating endometrial repair, restoring its periodic shedding and regeneration function, and maintaining the dynamic balance of sex hormone levels.18 The combination of cold knife separation and PRP has a complementary effect, better regulating the secretion of sex hormones. Hajipour H et al19 found that PRP could improve estrogen levels in patients with uterine and ovarian related infertility, thereby enhancing their endometrial implantation ability and regenerating ovarian function. Although there existed differences in the research subjects compared to Hajipour H, it also indicated that PRP had a higher effect on improving estrogen levels than conventional treatment, providing important theoretical basis for the results of this study.
In this study, the levels of inflammatory factors such as CRP, IL-8, IL-6 were significantly increased in both groups of patients after treatment compared to before treatment. This phenomenon was related to the stress response and tissue repair process induced by surgical trauma. Surgical invasiveness may activate the immune system, leading to a brief release of inflammatory factors.20 However, the levels of CRP, IL-8, and IL-6 in the cold knife + PRP group were much lower than those in the cold knife group after treatment, indicating that combination therapy can alleviate excessive inflammatory response through a dual mechanism. The possible reason for this might be that abundant platelet-derived growth factor (PDGF) and TGF-β in PRP could regulate the expression of matrix metalloproteinase-9 (MMP-9). Although both groups showed an increase in MMP-9 levels, the combined group showed a more significant increase. The result indicated that MMP-9 accelerated the clearance of fibrosis products by enhancing collagen degradation ability. In contrast, the conventional group inhibited MMP-9 activity due to thermal injury, leading to extracellular matrix accumulation and exacerbating the inflammatory microenvironment.21 Therefore, the combination of cold knife and PRP reduced the release of pro-inflammatory cytokines driven by thermal injury. The VEGF and other factors released by PRP could promote endothelial repair, shorten the inflammatory phase, accelerate tissue remodeling, and further inhibit the sustained release of acute phase proteins such as CRP, thus achieving better anti-inflammatory effects.22
This study for the first time evaluated the preventive effect of cold knife combined with PRP treatment on long-term postoperative re-adhesion in IUA patients systematically. The results showed that the re-adhesion rate of the cold knife + PRP group was much lower than that of the cold knife group at 1, 6, and 12 months after treatment. In addition, through continuous observation for up to 12 months, it was found that the re-adhesion rate of the cold knife + PRP group increased significantly less over time than that of the cold knife group. The results indicated that cold knife + PRP not only had significant short-term effects but also formed a long-term anti fibrotic microenvironment through the sustained release of growth factors by PRP and the preservation of endometrial barrier function by the cold knife.23 This contrasted with the short-term advantages of single cold knife or PRP treatment, suggesting that their synergy might reshape the dynamic balance of uterine cavity repair.
This study still has several limitations: firstly, as a retrospective cohort study, non-randomized grouping may result in selection bias. Secondly, although the sample size has been estimated and meets the minimum statistical requirements, it still belongs to a small sample study, and extrapolation of conclusions should be cautious. Furthermore, the lack of a separate PRP treatment group as a control makes it difficult to clearly distinguish the individual contributions of cold knife and PRP. In addition, retrospective data collection may be limited by the completeness of medical records and the consistency of measurement standards. Although we have implemented several quality control measures, we still cannot completely eliminate the influence of confounding factors. Future research should further validate the findings of this study through prospective, multicenter, large-sample randomized controlled trials. It is recommended to establish three parallel comparisons: cold knife alone, PRP alone, and cold knife combined with PRP to systematically evaluate the additional benefits and mechanisms of combination therapy. At the same time, the preparation and injection protocol of PRP can be further optimized. The optimal concentration, timing and frequency should be explored, and longer follow-up periods are needed, especially to observe the impact on pregnancy outcomes. This will provide higher-level clinical evidence for individualized and comprehensive treatment of IUA.
Conclusion
In general, the combination of hysteroscopic cold knife separation surgery and PRP treatment showed a trend of regulating the sex hormone levels of patients with IUA, reducing the body’s inflammatory response, and decreasing the recurrence rate of postoperative re-adhesions. This combination may have clinical value as a potential combined treatment strategy.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by The Ethics Committee of Shijiazhuang People’s Hospital. Written informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the standards upheld with those of the 1964 Helsinki Declaration and its later amendments for ethical research involving human subjects.
Consent to Participate
Informed consent was obtained from every human participant in the study and the patients participating in the study all agree to publish the research results.
Informed Consent
Informed consent was obtained from participants for the participation in the study and all methods were carried out in accordance with relevant guidelines and regulations.
Funding
This study was funded by Shijiazhuang Science and Technology Bureau Project (No. 221460423).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhao G, Hu Y. Mechanistic insights into intrauterine adhesions. Semin Immunopathol. 2024;47(1):3. doi:10.1007/s00281-024-01030-9
2. Mentula M, Männistö J, Gissler M, Heikinheimo O, Niinimäki M. Intrauterine adhesions following an induced termination of pregnancy: a nationwide cohort study. BJOG. 2018;125(11):1424–12. doi:10.1111/1471-0528.15216
3. Shen M, Duan H, Chang Y, et al. Prevalence and risk factors of intrauterine adhesions in women with a septate uterus: a retrospective cohort study. Reprod Biomed Online. 2022;44(5):881–887. doi:10.1016/j.rbmo.2022.02.004
4. Gao Y, Wang H, Xiao Y. The effect of cold-knife conization on pregnancy outcomes in patients with cervical lesions. PLoS One. 2022;17(12):e0278505. doi:10.1371/journal.pone.0278505
5. Wang G, Zhu Y, Duan N, Guo C, Liu N, Huang H. Does platelet-rich plasma improve adhesion recurrence and pregnancy outcomes in women with intrauterine adhesions? A systematic review and meta-analysis. J Minim Invasive Gynecol. 2025;32(2):133–142.e7. doi:10.1016/j.jmig.2024.10.013
6. Qiu D, Xiao X, Wang W, Zhang W, Wang X. Platelet-rich plasma improves pregnancy outcomes in moderate to severe intrauterine adhesion: a retrospective cohort study. J Clin Med. 2023;12(4):1319. doi:10.3390/jcm12041319
7. Shen M, Duan H, Lv R, Lv C. Efficacy of autologous platelet-rich plasma in preventing adhesion reformation following hysteroscopic adhesiolysis: a randomized controlled trial. Reprod Biomed Online. 2022;45(6):1189–1196. doi:10.1016/j.rbmo.2022.07.003
8. Ding C, Wei W, Ding F, et al. Ultrasound diagnostic of intrauterine adhesions: systematic review and meta-analysis. J Obstet Gynaecol Res. 2024;50(9):1681–1686. doi:10.1111/jog.16027
9. Mahajan U, Papaleontiou A, Imam MA, et al. Assessing standardisation in Platelet-Rich Plasma (PRP) injections for the management of Greater Trochanteric Pain Syndrome (GTPS): a systematic review of the available literature. Cureus. 2024;16(11):e74690. doi:10.7759/cureus.74690
10. Yang L, Ma N, Song D, et al. The effect of estrogen in the prevention of adhesion reformation after hysteroscopic adhesiolysis: a prospective randomized control trial. J Minim Invasive Gynecol. 2022;29(7):871–878. doi:10.1016/j.jmig.2022.04.004
11. Roy KK, Baruah J, Sharma JB, Kumar S, Kachawa G, Singh N. Reproductive outcome following hysteroscopic adhesiolysis in patients with infertility due to Asherman’s syndrome. Arch Gynecol Obstet. 2010;281(2):355–361. doi:10.1007/s00404-009-1117-x
12. Li Y, Li Y, Wang Y, et al. Comparison of hysteroscopic adhesiolysis with electrosurgery instrument or hysteroscopic scissors in the treatment of intrauterine adhesions of infertile or recurrent pregnancy loss women. Arch Gynecol Obstet. 2025;311(4):1063–1071. doi:10.1007/s00404-024-07866-8
13. ALunardon T, Sumner SM, Mollabashi M, Darzenta N, Davis E, Naskou MC. Growth factor and cytokine characterization of canine platelet lysate with variable leukocyte concentration, plasma content, and heat-sensitive proteins. Front Vet Sci. 2024;11:1408080. doi:10.3389/fvets.2024.1408080
14. Ali MM, Kamel M, Ragab A, et al. Holmium laser versus cold knife visual internal urethrotomy for management of short segment urethral stricture: a prospective randomized clinical trial. World J Urol. 2023;41(7):1897–1904. doi:10.1007/s00345-023-04434-8
15. Liu X, Li X, Wei W, et al. Local autologous platelet rich plasma injection combined with platelet rich fibrin filling as the main treatment for refractory wounds: a case series. Front Surg. 2023;9:1003691. doi:10.3389/fsurg.2022.1003691
16. Sharon A, Zidane M, Aiob A, et al. Nonelectric shaving of endometrial polyp by hysteroscopy - A new technique to eliminate thermal damage. Eur J Obstet Gynecol Reprod Biol. 2023;285:170–174. doi:10.1016/j.ejogrb.2023.04.018
17. Ferrari F, Bonetti E, Oliveri G, et al. Cold knife versus carbon dioxide for the treatment of preinvasive cervical lesion. Medicina. 2024;60(7):1056. doi:10.3390/medicina60071056
18. Ruiz-Muñoz M, Martinez-Barrios FJ, Fernandez-Torres R, et al. Autologous platelet-rich plasma (APRP) in diabetes foot disease: a meta-analysis. J Diabetes Complications. 2024;38(2):108690. doi:10.1016/j.jdiacomp.2024.108690
19. Hajipour H, Farzadi L, Latifi Z, et al. An update on platelet-rich plasma (PRP) therapy in endometrium and ovary related infertilities: clinical and molecular aspects. Syst Biol Reprod Med. 2021;67(3):177–188. doi:10.1080/19396368.2020.1862357
20. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
21. Nosalski R, Maffia P, Guzik TJ. Monocytes M(MP)aking way for T-cell vascular infiltration. Circ Res. 2018;123(6):638–640. doi:10.1161/CIRCRESAHA.118.313668
22. Lee HM, Shen EC, Shen JT, Fu E, Chiu HC, Hsia YJ. Tensile strength, growth factor content and proliferation activities for two platelet concentrates of platelet-rich fibrin and concentrated growth factor. J Dent Sci. 2020;15(2):141–146. doi:10.1016/j.jds.2020.03.011
23. Farzadiniya P, Keihan AM, Jokar Borazjani S. Comparison of the effects of platelet-rich plasma and platelet-rich fibrin on the healing process of a rat’s mucosal wound. J Tissue Viability. 2024;33(3):425–432. doi:10.1016/j.jtv.2024.05.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.