Back to Journals » International Medical Case Reports Journal » Volume 18
Hypothyroidism Due to Thyroid Amyloidosis Simultaneously With AL Renal Amyloidosis to Give Better Idea of Association of the Two Conditions
Authors Guan C, Liu Y ![]() , Chen R
, Chen R ![]() , Zhu Y
, Zhu Y ![]()
Received 30 August 2024
Accepted for publication 7 January 2025
Published 20 January 2025 Volume 2025:18 Pages 139—144
DOI https://doi.org/10.2147/IMCRJ.S489760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Thomas E Hutson
Changrong Guan,1 Yonghua Liu,2 Riqiu Chen,1 Yingbiao Zhu3
1Department of Endocrinology, The Lishui Hospital of Wenzhou Medical University, The First Affiliated Hospital of Lishui University, Lishui People’s Hospital, Lishui, Zhejiang, 323000, People’s Republic of China; 2Department of Hematology, The Lishui Hospital of Wenzhou Medical University, The First Affiliated Hospital of Lishui University, Lishui People’s Hospital, Lishui, Zhejiang, 323000, People’s Republic of China; 3Department of Neurology, The Lishui Hospital of Wenzhou Medical University, The First Affiliated Hospital of Lishui University, Lishui People’s Hospital, Lishui, Zhejiang, 323000, People’s Republic of China
Correspondence: Yingbiao Zhu, Department of Neurology, The Lishui Hospital of Wenzhou Medical University, The First Affiliated Hospital of Lishui University, Lishui People’s Hospital, Lishui, Zhejiang, 323000, People’s Republic of China, Tel +86-18957097750, Email [email protected]
Abstract: Primary amyloidosis (AL type) is a systemic disease that can lead to structural and functional damage to organs and tissues such as the kidney, heart and liver with non-specific symptoms. Most of the affected patients develop thyroid infiltration and thus diffuse enlargement of the thyroid gland, while cases leading to hypothyroidism are exceedingly rare. Some researchers have analyzed thyroid function in newly diagnosed patients with AL amyloidosis, and found that the incidence of overt hypothyroidism is only 7%. In this case, we describe a 66-year-old female patient who visited the nephrology department due to lower limb edema for 2 months and numbness of the extremities for more than 2 years. Examination revealed massive proteinuria and hypoproteinemia, and a needle biopsy of the kidney revealed amyloid deposition. The patient was also found to have hypothyroidism and diffuse enlargement of the thyroid gland. We evaluated the etiology of thyroid disease from the pathogenesis of the disease after consulting an endocrinologist. The result of the thyroid fine needle puncture and pathological examination showed thyroid amyloidosis. The patient received levothyroxine sodium tablets as replacement therapy and received chemotherapy in the hematology department. At the same time, we monitored the improvement in thyroid function and reduction in thyroid volume.
Keywords: thyroid amyloidosis, hypothyroidism, renal amyloidosis, nephrotic syndrome, macroalbuminuria
Introduction
The primary form of amyloidosis occurs when amyloid deposits in the extracellular matrix, which further causes tissue and organ damage. It may also involve organs or tissues such as the kidney, heart, liver, skin and soft tissue, nerves and lungs. There are various components of amyloid such as immunoglobulin light chains, serum amyloid and transthyretin. The most common disease is primary systemic light chain amyloidosis, caused by the deposition of monoclonal immunoglobulin light chains or light chain fragments produced by plasma cells in the bone marrow in the form of amyloid. Glomerular amyloid deposition is characterized by proteinuria, marked nephrotic syndrome and varying degrees of renal insufficiency. The thyroid gland can also be affected by amyloidosis. Goiter following amyloidosis involving the thyroid gland can be found in international reports.1 However, there are few reports of simultaneous thyroid dysfunction in the domestic literature. The thyroid is often overlooked in clinical practice due to the rarity of thyroid involvement. Hypothyroidism is commonly caused by autoimmune diseases (chronic thyroiditis), medications, surgery and a variety of other factors. Several drugs including amiodarone, lithium, interferon and immunosuppressants may induce hypothyroidism. Therefore, thyroid function should be evaluated before prescribing these medications. Thyroid biopsy with fine-needle aspiration is rarely required for these conditions. It is challenging for non-endocrinologists to determine the actual cause of amyloidosis involving the thyroid without performing a thyroid biopsy since thyroid amyloidosis is extremely rare. They should closely monitor this condition. In this case study, we describe a patient who had systemic amyloidosis and hypothyroidism due to thyroid amyloidosis with nephrotic syndrome as a first symptom. The patient did not consume any medications known to affect thyroid function before the diagnosis of hypothyroidism. Therefore, drug-induced hypothyroidism is not considered.
Case Report
A 66-year-old female with hoarseness visited the Nephrology Department due to numbness of four extremities distributed in the shape of gloves and socks since January 2018 and edema of lower extremities in February 2020.
Examination revealed diffuse grade 1 enlargement of the thyroid gland, mild pitting edema of both lower limbs, loss of knee tendon reflexes and Achilles tendon reflexes, hypoesthesia of temperature sensation in the left lower limb, and hypoesthesia of tactile muscle vibration sensation in both lower limbs. The patients had a few symptoms of hypothyroidism such as fatigue, hoarseness and hypersomnia at the time of onset.
The patient received renal biopsy because urinalysis showed urine protein 3+, 24h urine protein 3.05 g/24 h, albumin 25.8 g/L, serum-free Lambda light chain 1710 mg/L (normal 5.71–26.30), immune solid-phase electrophoresis showed IgG positive, λ chain positive. Renal pathology report (Guangzhou KingMed Center for Clinical Laboratory KB2006889): Congo red positive and oxidized Congo red positive, consistent with amyloidosis nephropathy, AL type (Figure 1); immunohistochemical examination of kidney tissue showed Lambda positive and Kappa negative (Figure 2). The patient was diagnosed with renal amyloidosis (AL type) and transferred to the hematology department for chemotherapy with PTD (bortezomib, thalidomide and dexamethasone) regimen.
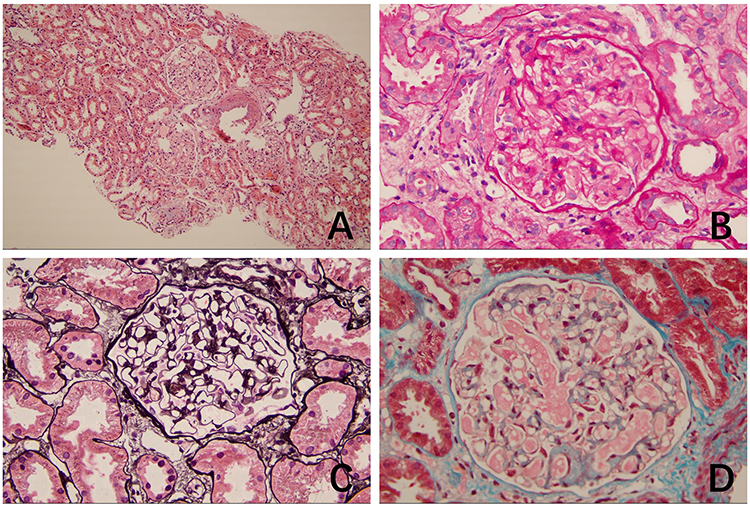 |
Figure 1 Kidney HE, PAS, PASM and Masson staining. A HE Dyeing 100X; B PAS Dyeing 400X; C PASM Dyeing 400X; D Masson Dyeing 400X. The glomerular mesangial area has a powdery homogeneous deposition of unstructured material, which widens part of the glomerular mesangial area (A). The glomerular capsule wall and tubular basement membrane were not thickened (B). The segmental mesangial area of the glomerulus was widened, and the glomerular basement membrane showed segmental lash-like changes (C). No significant deposits of eosinophilic proteinaceous material were observed in the subepithelial, subendothelial, or mesangial areas of the glomeruli (D). |
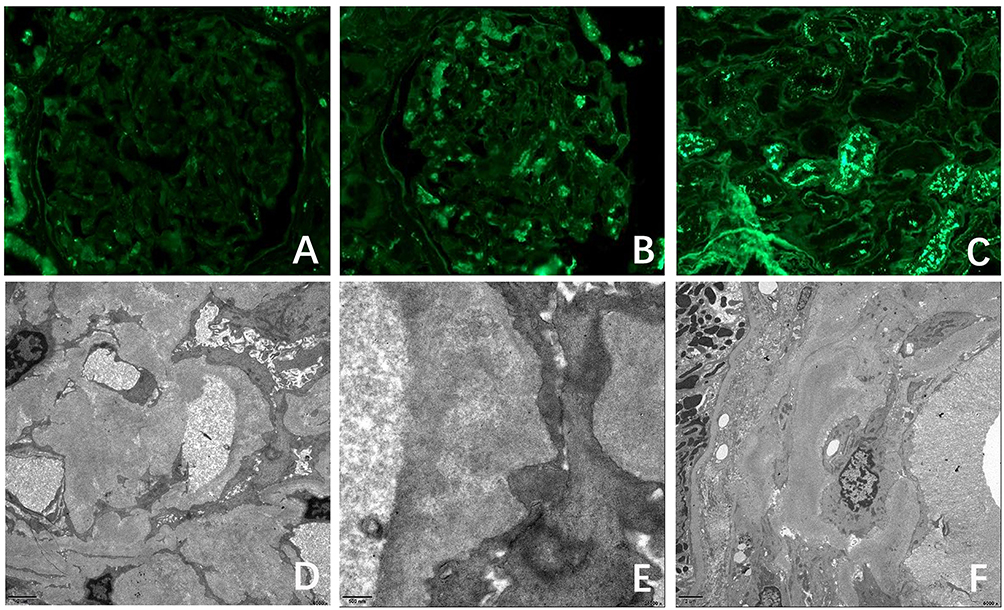 |
Figure 2 The results of renal immunofluorescence and electron microscopy. (A) kappa (-), (B) lambda (+), (C) ALB (-); (D) mesangial area in diameter, (E)basement membrane and (F) arterioles. The lower row shows a large amount of fibroid material deposition in the renal tissue by ultramicroscopic electron microscopy, about 8–12 nm. Note: The upper row is the immunofluorescence staining method. |
Upon thyroid function showing 0.78 pmol/L free thyroid 3 (normal 3.1–6.80), 0.84 pmol/L free thyroid 4 (normal 12.00–22.00), TSH >100 mIU/L (normal 0.27–4.20), thyroglobulin antibody >4000.0 IU/mL (normal 115.0), thyroid peroxidase antibody 447.7 IU/mL (normal 0–34.0), the patient was diagnosed with primary hypothyroidism and thyroid ultrasound showed diffuse thyroid lesions with enlargement (right lobe: left and right diameters 23 mm and anteroposterior diameters 19 mm; left lobe: left and right diameters 21 mm and anteroposterior diameters 19 mm). The patient was started on levothyroxine.
The patient was consulted by an endocrinologist due to hypothyroidism and diffuse enlargement of the thyroid gland. Based on the molecular pathogenesis of thyroid disease, the patient was considered whether the etiology of her thyroid disease was similar to the etiology of her kidney disease. Thus, the patient underwent thyroid fine-needle aspiration. Her thyroid pathology results (Guangzhou KingMed Center for Laboratory Medicine 20104173) showed positive Congo red and positive oxidized Congo red, consistent with amyloidosis. Type AL (Figure 3) demonstrates that hypothyroidism is also caused by amyloidosis.
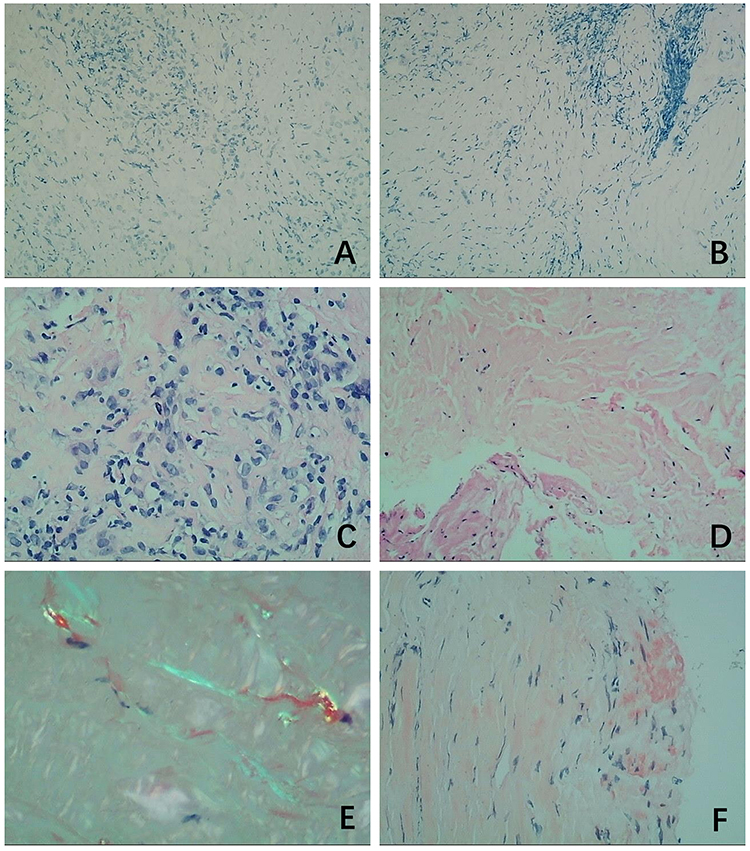 |
Figure 3 Thyroid pathology H&E, Congo red staining and immunohistochemistry. (A and B) is immunohistochemistry, AA (-); (C and D) is HE staining, (C) 400X, (D) 200X; (E and F) is special staining, (E) is Congo red + polarized light, and (F)is Congo red. The thyroid interstitium shows pale red staining with unstructured material deposition and a large number of lymphocyte infiltration (A and B). Congo red staining shows amyloid as brick red (C) under a light microscope and apple-green birefringence (D) under a polarized light microscope. Immunohistochemistry reveals AA- (E and F). |
Discussion
Primary amyloidosis can involve multiple endocrine glands including the thyroid, pituitary, parathyroid, pancreas, adrenal glands and gonads. The incidence of primary amyloidosis involving the thyroid gland resulting in hypothyroidism is infrequent. A case of systemic amyloidosis in a patient on dialysis with goiter and hypopituitarism secondary to thyroid amyloidosis reported by Didem Ozdemir et al was suspected that the hypopituitarism may be caused by pituitary amyloid infiltration. Therefore, we recommended that amyloid infiltration should be considered in patients with systemic amyloidosis who present with rapidly enlarging thyroid glands and signs of hypopituitarism.2 M Nistal et al have performed histochemical and ultrastructural studies of the testis, epididymis and spermatic cord in six adult males with amyloidosis secondary to several diseases.3 In addition, the lamina propria of seminiferous tubules, testis, epididymis and spermatic cord were primarily composed of AA protein. Compared with the aforementioned endocrine glands, amyloidosis involving the thyroid gland is relatively rare, whereas thyroid enlargements are mainly caused by thyroid amyloidosis. A case of goiter due to thyroid amyloidosis in a 48-year-old woman with secondary rheumatoid arthritis and renal failure was once reported by B. López-Muñoz et al.4 Some foreign researchers have also analyzed the thyroid function of patients with newly diagnosed AL amyloidosis, and found that the proportion of patients with subclinical hypothyroidism with TSH values was 19% higher than the upper limit of normal. In comparison, the proportion with overt hypothyroidism is only 7%.5 Referring to the domestic literature, it was found that only two reports suggested thyroid involvement by amyloidosis in 2007 and 2008,6,7 but the thyroid function of the patients in both of these reports was normal. Another report indicated that renal amyloidosis was associated with hypothyroidism.8 However, there is no evidence that thyroid amyloidosis is the cause of hypothyroidism. This article reports a case of hypothyroidism caused by thyroid amyloidosis along with renal amyloidosis, which is the first case reported in China because of thyroid amyloidosis.
In addition, E Muchtar et al also performed a binary logistic regression analysis of thyroid function in patients with newly diagnosed AL amyloidosis and found that age ≥65 years, female gender, renal involvement, liver involvement and kappa light chain restriction were independently associated with hypothyroidism.5 The conclusions of this study were consistent with the morbidity characteristics of the patients in this paper. The study also pointed out that hypothyroidism was an independent predictor of survival in such patients. Compared with the euthyroid group, the 4-year survival rate was only 36% in the hypothyroid group. Most patients were initially diagnosed in the nephrology department due to edema or proteinuria. After nephrotic syndrome was confirmed to be amyloidosis, the patients were then transferred to the hematology department for chemotherapy. In contrast to doctors in the endocrinology department, doctors in the hematology department could not observe thyroid dysfunction acutely and may overlook the importance of thyroid dysfunction in these patients. Hypothyroidism in one patient was not detected by the nephrology department and the hematology department during hospitalization, which was later discovered by accident. Based on the pathophysiological mechanisms of the disease, we considered that hypothyroidism in this patient may be caused by thyroid amyloidosis. Thyroid histopathology was further confirmed. The optimal treatment time may be delayed for some patients who are not actively treated or have limited finances. We recommend thyroid function testing for all patients with primary amyloidosis. Hypothyroidism may be diagnosed through a thyroid biopsy to determine the cause. The association between hypothyroidism and lower survival rates in amyloidosis patients underscores the importance of encouraging early treatment to achieve better outcomes. Reviewing the diagnosis and treatment of this case, we obtained the following treatment experiences: (1) The incidence of hypothyroidism caused by thyroid amyloidosis was low, and most of these patients had life-threatening diseases such as kidney damage and heart damage for the first time, which was easy to miss the etiological exploration of “trivial” hypothyroidism in clinical practice. Therefore, it is recommended that thyroid function tests should be perfected in patients with amyloidosis who visit the nephrology department or the hematology department. If hypothyroidism is found, it is necessary to warn of the limited life expectancy of patients and perform active treatment. (2) For hypothyroid patients who present to the department of endocrinology, attention should be paid that it may be related to this disease if massive proteinuria, hypoproteinemia, or abnormal renal function are also found. Congo red staining is recommended during pathological examination of thyroid puncture. (3) The guidelines for the diagnosis and treatment of systemic light chain amyloidosis state that the positive rate of symptomatic organ biopsy is >95%.9 Thyroid puncture poses fewer risks of bleeding and infection than renal puncture due to its simplicity. For patients with nephrotic syndrome combined with hypothyroidism who are unable to undergo renal biopsy due to obesity or other reasons, thyroid biopsy may be considered to assist in diagnosis. The renal and thyroid function of the patient must also be closely monitored to allow timely adjustments to the treatment plan. Upon detecting amyloidosis involving the thyroid gland and kidneys, we should promptly initiate thyroid hormone replacement therapy and correct hypoproteinemia. Regular evaluation of the functions of other affected organs is also necessary to achieve the best therapeutic outcomes.
Conclusion
Primary amyloidosis rarely affects the thyroid gland. This case highlights the importance of conducting thorough thyroid function tests in patients with primary amyloidosis (AL type). In conclusion, our findings suggest that prompt treatment should be administered to avoid delaying the appropriate intervention when hypothyroidism is detected.
Consent for Publication
This manuscript adheres to CARES guidelines. The patient described in this case report provided written informed consent, which can be provided upon request. Institutional approval was not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by the Project from the Zhejiang Provincial Medical and Health Science and Technology Program (2021KY1233), China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chraibi A, Msyah L, Laaribi O, et al. Amyloid Goiter: first Sign of Systemic Amyloidosis. Ann Endocr. 2009;70(1):80–82. doi:10.1016/j.ando.2007.10.002
2. Didem Ozdemir 1, Selcuk D, Tomris E, et al. Amyloid Goiter and Hypopituitarism in a Patient with Systemic Amyloidosis. Amyloid. 2011;18(1):32–34. doi:10.3109/13506129.2010.545961
3. Nistal M, Santamaria L, Codesal J, et al. Secondary Amyloidosis of the Testis: an Electron Microscopic and Histochemical Study. Appl Pathol. 1989;7(1):2–7.
4. López-Muñoz B, Greco Bermúdez L, Marín-Jiménez D, et al. An Unusual Amyloid Goiter in a 48-Year-Old Woman With Rheumatoid Arthritis, Secondary Amyloidosis and Renal Failure. Case Rep Endocrinol. 2019;2019:1–4. doi:10.1155/2019/4291486
5. Muchtar E, Dean DS, Dispenzieri A, et al. Prevalence and Predictors of Thyroid Functional Abnormalities in Newly Diagnosed AL Amyloidosis. J Intern Med. 2017;281(6):611–619. doi:10.1111/joim.12617
6. Wenlun H. Huang Chaoxing. A case of renal amyloidosis with thyroid amyloidosis and literature review [J]. J Wenzhou Medi Col. 2007;37(6):594–595.
7. Zhen S, Chaoxing H, Fanfan L, et al. Two cases of renal amyloidosis with thyroid amyloidosis [J]. Chinese Med J. 2008;88(21):1511–1512.
8. Zhaoyun Liu. Two cases of renal amyloidosis with Budd-Chiari syndrome and hypothyroidism [J]. J Pract Med. 2012;28(11):1924–1925.
9. National Clinical Research Center for Renal Diseases, Chinese Systemic Amyloidosis Collaborative Group. Guidelines for the Diagnosis and Treatment of Systemic Light Chain Amyloidosis. Chinese Med J. 2016;96(44):3540–3548.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.