Back to Journals » Drug Design, Development and Therapy » Volume 20
Hypericin as a Photodynamic Immunomodulator: A Natural Compound for Dermatological Therapy
Authors Ma H, Zhang X, Li R, Qu B, Liu Y, Cui Y, Zhang T, Zhao J ![]()
Received 6 August 2025
Accepted for publication 17 November 2025
Published 8 January 2026 Volume 2026:20 558923
DOI https://doi.org/10.2147/DDDT.S558923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Huike Ma,* Xiawei Zhang,* Ruonan Li,* Baoquan Qu, Yuchen Liu, Yunran Cui, Tianlu Zhang, Jingxia Zhao
Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Institute of Chinese Medicine, Beijing, 100010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingxia Zhao, Email [email protected]
Abstract: Hypericin, a polycyclic quinone derived from *Hypericum perforatum* (St. John’s Wort), has gained attention for its broad pharmacological activities, including anti-inflammatory, antimicrobial, and antitumor effects. It modulates key signaling pathways like NF-κB and MAPK, reducing chronic inflammation and making it effective in treating autoimmune and infectious skin conditions. As a photosensitizer, hypericin also induces apoptosis in abnormal cells through photodynamic therapy (PDT), showing promising results in treating cutaneous T-cell lymphoma (CTCL), psoriasis, and fungal infections. While its solubility and bioavailability remain challenges, hypericin’s favorable safety profile and therapeutic potential position it as a valuable option for managing refractory dermatological conditions.
Keywords: hypericin, anti-inflammatory, PDT, ROS, psoriasis, CTCL
Introduction
Hypericin is a naturally occurring polycyclic quinone compound predominantly extracted from St. John’s Wort (Hypericum perforatum), which has attracted considerable attention for its diverse pharmacological properties, including anti-inflammatory, antimicrobial, and antitumor effects. Research has demonstrated that hypericin can modulate cytokine production and influence critical signaling pathways, such as the NF-κB and MAPK pathways highlighting its crucial role in immune responses.1–3 This ability to regulate pro-inflammatory cytokines and alleviate chronic inflammation makes hypericin a promising candidate for managing autoimmune diseases and skin infections, where immune dysregulation plays a central role.4,5
While hypericin is traditionally recognized for its antidepressant effects, this review narrows the focus to its applications in dermatology. The therapeutic application of hypericin in skin disorders is gaining increasing recognition, particularly in photodynamic therapy (PDT).6 Hypericin’s role as a photosensitizer enables it to generate reactive oxygen species (ROS) under specific light conditions, offering a targeted approach to treating various skin disorders.7 Given the increasing burden of refractory dermatological diseases such as Cutaneous T-cell Lymphoma (CTCL) and psoriasis, hypericin’s potential in these areas is of growing interest.5,8 Additionally, its antioxidant properties can mitigate oxidative stress in the skin and enhance wound healing processes.9,10
Despite promising preclinical and early clinical findings, significant gaps remain in the literature regarding the full scope of hypericin’s therapeutic mechanisms and clinical efficacy in dermatology. The existing research predominantly focuses on its basic pharmacological properties, but comprehensive reviews synthesizing its specific applications in dermatology are limited. Additionally, there is a lack of clarity on optimizing hypericin’s delivery mechanisms, dosages, and treatment protocols in the context of skin diseases. This review seeks to address these gaps by providing an in-depth analysis of hypericin’s chemical characteristics, its immune-modulatory effects, and its potential in photodynamic therapies for skin disorders.
Chemistry and Pharmacology of Hypericin
Chemical Structure and Properties of Hypericin
Hypericin, a natural polycyclic aromatic compound and a prominent phloroglucinol derivative, is recognized as one of the main active constituents of Hypericum perforatum. This plant has been employed in traditional medicine for centuries, leveraging the therapeutic properties attributed to hypericin.
Chemical Structure of Hypericin
The chemical structure of hypericin exhibits a complex arrangement of molecular components that underpin its unique properties. At its core is a tricyclic phloroglucinol framework, which consists of two fused benzene rings integrated into a six-membered ring.11 This structural foundation contributes to the molecule’s stability and reactivity. Additionally, hypericin incorporates an anthraquinone moiety, which provides significant aromatic characteristics and a quinone functional group; these elements not only give hypericin its distinctive deep red coloration but also enhance its photodynamic properties. The molecule features cyclic alkyl groups, including cyclohexane and cyclopentane rings, that interconnect with the anthraquinone structure, thereby reinforcing the compound’s overall stability. The presence of multiple hydroxyl groups fosters essential intermolecular interactions, such as hydrogen bonding, which are critical for its diverse biological activities. The molecular formula of hypericin is C30H20O8, reflecting its intricate structural complexity12,13 (Figure 1).
 |
Figure 1 Chemical structure of Hypericin. |
Properties of Hypericin
Hypericin is distinguished by its remarkable photodynamic properties, allowing it to absorb light and facilitate photochemical reactions that generate reactive ROS. This characteristic underlies its role as a photosensitizer in PDT, enabling targeted treatments for various diseases. In addition to its photodynamic activity, hypericin has demonstrated antidepressant effects, possibly through the modulation of neurotransmitters such as serotonin, dopamine, and norepinephrine, thereby influencing mood regulation.14–17 Furthermore, extensive research highlights hypericin’s antiviral and antimicrobial effects, which inhibit viral replication and bacterial growth, positioning it as a potential therapeutic agent in infectious disease management.18–20 Recent studies also suggest that hypericin exhibits anti-inflammatory properties, potentially via the inhibition of pro-inflammatory mediator production, thus broadening its therapeutic applications.21,22 However, the sensitivity of hypericin to light necessitates proper storage and handling under low-light conditions to preserve its stability. Additionally, hypericin’s solubility profile reveals poor water solubility while demonstrating increased solubility in organic solvents like ethanol and methanol, a characteristic that impacts its formulation and bioavailability in pharmaceutical contexts.
Synthesis and Extraction Methods
Hypericin is sourced from Hypericum perforatum or produced synthetically. Natural extraction chiefly uses ethanol or methanol; the crude liquor is evaporated or chromatographed to purity.23–25 Supercritical CO2 extraction avoids organic solvents and gives cleaner concentrates.26,27 Ultrasonic-assisted extraction mechanically disrupts cell walls, raising yield and shortening time.27,28 Synthetic options include multi-step chemical total synthesis from simple aromatics, semi-synthesis from emodin-type anthraquinones,29,30 or biosynthesis in genetically tuned microbes or plant-cell cultures.30,31
Synthetic options include multi-step chemical total synthesis from simple aromatics, semi-synthesis from emodin-type anthraquinones, or biosynthesis in genetically tuned microbes or plant-cell cultures.28,32 Natural methods are sustainable but require bulky biomass and careful purification; synthetic routes offer higher purity and controlled output yet incur greater cost and technical complexity. Continuous improvements in both lines are enhancing efficiency, scalability and environmental footprint.
Pharmacokinetics and Metabolism
After oral intake, lipophilic hypericin is absorbed in the small intestine; co-administered fat increases uptake.33–35 The molecule distributes widely, crosses the blood–brain barrier—critical for antidepressant activity—and accumulates in adipose tissue, prolonging its systemic half-life.36,37
In the liver, CYP3A4 and related isoforms convert hypericin to several phenolic and quinoid metabolites that retain partial activity. Excretion is overwhelmingly fecal (>90%), with minor renal clearance.38,39 Excretion is overwhelmingly fecal (>90%), with minor renal clearance.40
Dose level, formulation (cyclodextrin, lipid carrier)34,41 and concurrent CYP modulators can double or halve systemic exposure;42,43 thus dose individualisation and interaction screening are mandatory for safe clinical use.
Safety Profile and Toxicological Considerations
The safety profile of hypericin is critical, particularly in the context of its clinical application and use as a dietary supplement. Although hypericin has been traditionally employed for various therapeutic purposes, a comprehensive assessment of its toxicological properties is essential to ensure safe administration.34
Hypericin is characterized by relatively low acute toxicity, with mild and reversible symptoms typically observed following single high-dose exposure. However, chronic use, especially at elevated doses, may lead to potential hepatic and gastrointestinal adverse effects, necessitating careful monitoring for individuals undergoing prolonged treatment.44,45 Photosensitivity is a well-documented side effect associated with hypericin, highlighting the need for precautionary measures regarding sun exposure in patients.44,45 Additionally, hypericin’s ability to interact with drugs metabolized by the cytochrome P450 enzyme system emphasizes the importance of considering potential drug–drug interactions, which may alter the pharmacokinetics of concurrently administered medications.46
Although allergic reactions to hypericin are possible, they are generally rare and may manifest as skin rashes or gastrointestinal disturbances. Toxicological evaluations also encompass considerations of carcinogenicity; while no definitive evidence currently links hypericin to cancer, its capacity to generate ROS warrants ongoing investigation. The teratogenic and reproductive toxicity profiles of hypericin remain largely underexplored, suggesting a need for caution during pregnancy and lactation.47,48 Furthermore, while significant neurotoxic effects have not been identified at therapeutic doses, the potential for neurotoxicity at high doses or in sensitive individuals cannot be ruled out. In summary, hypericin generally presents a favorable safety profile; however, it is not without potential risks.
Immunomodulatory Effects of Hypericin
A Multi-Faceted Regulator of Immune and Tissue Cells
Hypericin, a natural photosensitizer extracted from Hypericum perforatum, has garnered significant attention for its multifaceted regulatory effects on immune and tissue cells, demonstrating broad potential in immunomodulation, anti-fibrosis, and skin cancer treatment (Figure 2).
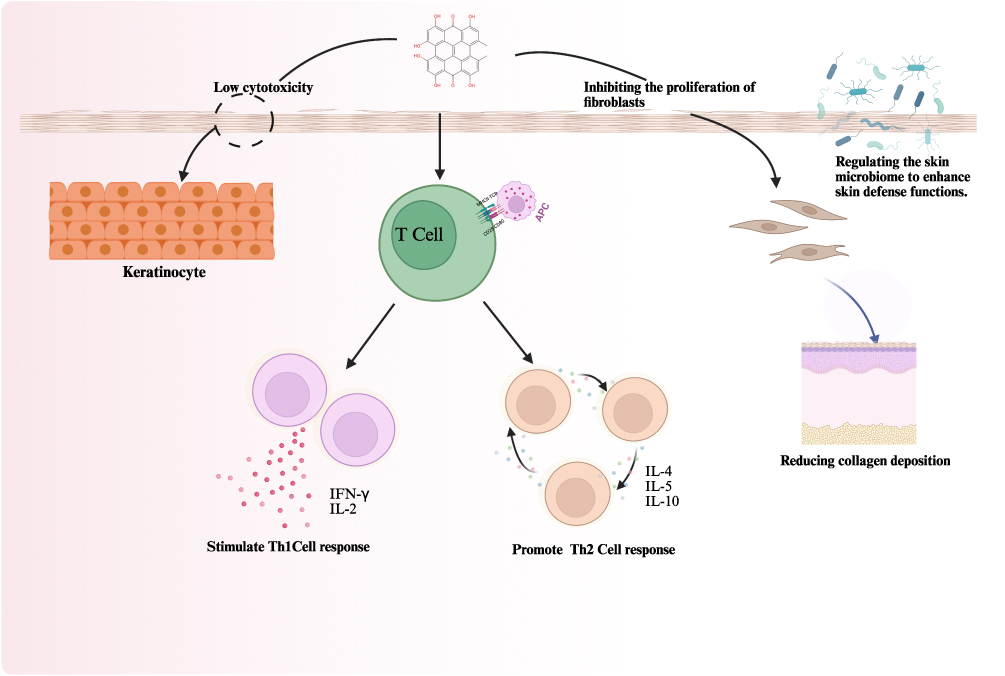 |
Figure 2 The Pleiotropic Immunomodulatory Mechanism of Hypericin in Skin Homeostasis. (1) Inhibition of fibrotic activity via suppression of fibroblast proliferation and collagen deposition; (2) Stimulation of a Th1-cell response via cytokines like IFN-γ and IL-2; (3) Promotion of a Th2-cell response via cytokines like IL-4, IL-5, and IL-10; and (4) Regulation of the skin microbiome to enhance barrier defense. The overall effect is a shift in immune balance with low cytotoxicity to keratinocytes. Figure created with BioRender.com. |
T-Cells
T-cells play a pivotal role in cell-mediated immunity, and hypericin’s effects on T-cell function are an important focus of research. Studies indicate that hypericin interacts with T-cells, influencing both their proliferation and cytokine secretion, which are crucial determinants of the adaptive immune response.49 Notably, hypericin can affect the differentiation of T-helper (Th) cells, which is essential in directing the immune response. Depending on the specific context, hypericin has been shown to promote a Th1 response characterized by increased production of interferon-gamma (IFN-γ) and interleukin-2 (IL-2), thereby enhancing cellular immunity against intracellular pathogens.50 Conversely, hypericin may also favor a Th2 response marked by the secretion of IL-4, IL-5, and IL-10, which plays a vital role in humoral immunity and defense against extracellular parasites.51 This ability of hypericin to sway Th cell differentiation could prove instrumental in therapeutic strategies aimed at recalibrating immune responses in conditions like autoimmunity and chronic infections.
Keratinocyte
Hypericin exhibits selective phototoxicity in PDT, showing significant cytotoxicity against skin cancer cells while sparing normal keratinocytes. For example, a study using 3 µM hypericin combined with PDT demonstrated no significant cytotoxicity in normal keratinocytes (HaCaT cell line), whereas fibroblasts and melanocytes exhibited notable toxicity.52 This cell selectivity suggests that hypericin preferentially targets cancer cells with minimal damage to normal keratinocytes.53 In addition to its phototoxic effects, hypericin also possesses immunomodulatory properties. At low doses, it can alter the morphology and function of keratinocytes without significantly affecting cell viability. In skin inflammation models, hypericin modulates cytokine release through PDT, with no significant impact on interleukin-2 (IL-2) secretion, indicating potential therapeutic benefits for inflammatory skin diseases such as psoriasis and atopic dermatitis.52 The underlying mechanism of hypericin’s phototoxicity involves the generation of ROS that induce apoptosis in target cells.53 However, the relatively low phototoxicity observed in keratinocytes may be attributed to their robust antioxidant defense mechanisms, as well as the cell membrane permeability and antioxidant enzyme activity of these cells.54
Fibroblast
Hypericin has emerged as a promising bioactive compound with significant potential in regulating fibroblast function, particularly in the contexts of anti-fibrosis and wound healing. Hypericin exerts its anti-fibrotic effects by inhibiting the proliferation of fibroblasts and reducing collagen deposition, thereby alleviating the development of fibrosis.55 Additionally, its anti-inflammatory and antioxidant properties further contribute to the mitigation of fibrosis. In wound healing, hypericin promotes tissue regeneration and rational collagen deposition by modulating fibroblast activity. For instance, composite hydrogel dressings loaded with hypericin have demonstrated excellent biocompatibility and wound-healing capabilities in both in vitro and in vivo studies. These dressings inhibit excessive fibroblast proliferation while promoting angiogenesis and re-epithelialization, significantly improving wound healing outcomes.55 Moreover, hypericin has shown potential applications in PDT due to its natural photosensitizing properties. Under light irradiation, hypericin generates ROS that induce apoptosis in fibroblasts, making it a promising candidate for treating fibrosis-related skin diseases.7 The clinical application of hypericin is supported by its multifaceted mechanisms in regulating fibroblast function, which not only inhibit fibrosis but also facilitate the repair and regeneration of damaged tissues.
Impact on Cytokine Production and Signaling Pathways
Hypericin, a naturally occurring photosensitizer, has garnered significant attention for its broad potential in immunomodulation, particularly in regulating cytokine production and signaling pathways. Research has demonstrated that hypericin modulates cytokine production and signaling through multiple mechanisms, thereby influencing immune responses and inflammatory processes. In PDT, hypericin activates the TLR3 signaling pathway, promoting the maturation of dendritic cells (DCs) and subsequently regulating cytokine production.50,56 This process involves the activation of key molecules in the TLR3 pathway and their downstream gene expression, enhancing the functionality of immune cells and thereby influencing overall immune responses. Additionally, hypericin regulates intracellular signaling pathways by increasing ROS production and intracellular Ca2+ levels, activating endoplasmic reticulum stress-related pathways and inducing pyroptosis, a mechanism particularly evident in triple-negative breast cancer (TNBC) cells.57 This highlights hypericin’s capacity to modulate cytokine production and cell death processes through intracellular signaling regulation. Moreover, hypericin’s regulatory effects on the NF-κB and MAPK signaling pathways are integral to its immunomodulatory properties. NF-κB plays a critical role in inflammation and immune responses, while MAPK pathways are involved in cell proliferation, differentiation, apoptosis, and inflammatory reactions. Hypericin inhibits the activation of NF-κB and MAPK pathways, reducing the production of pro-inflammatory cytokines such as TNF-α and IL-1β, and activates JNK and p38 MAPK pathways to promote apoptosis while inhibiting the ERK pathway. This dual regulation of signaling pathways underscores hypericin’s potential in anti-inflammatory and immunomodulatory applications.16 Its use in PDT has also shown therapeutic potential for various diseases, including skin cancer and inflammatory conditions.
Hypericin in the Treatment of Specific Dermatological Conditions
Hypericin, a naturally occurring compound from St. John’s wort, has garnered significant attention for its therapeutic applications across various medical disciplines, particularly in dermatology. This compound is recognized for its pharmacological properties as well as its potential as a photosensitizer in PDT for treating dermatological conditions. Upon exposure to specific wavelengths of light, hypericin produces ROS, which have been shown to exhibit potent anticancer and antimicrobial effects, making it an attractive option for conditions such as CTCL, psoriasis, and fungal infections, including mycosis fungoides58–60 (Table 1 and Figure 3).
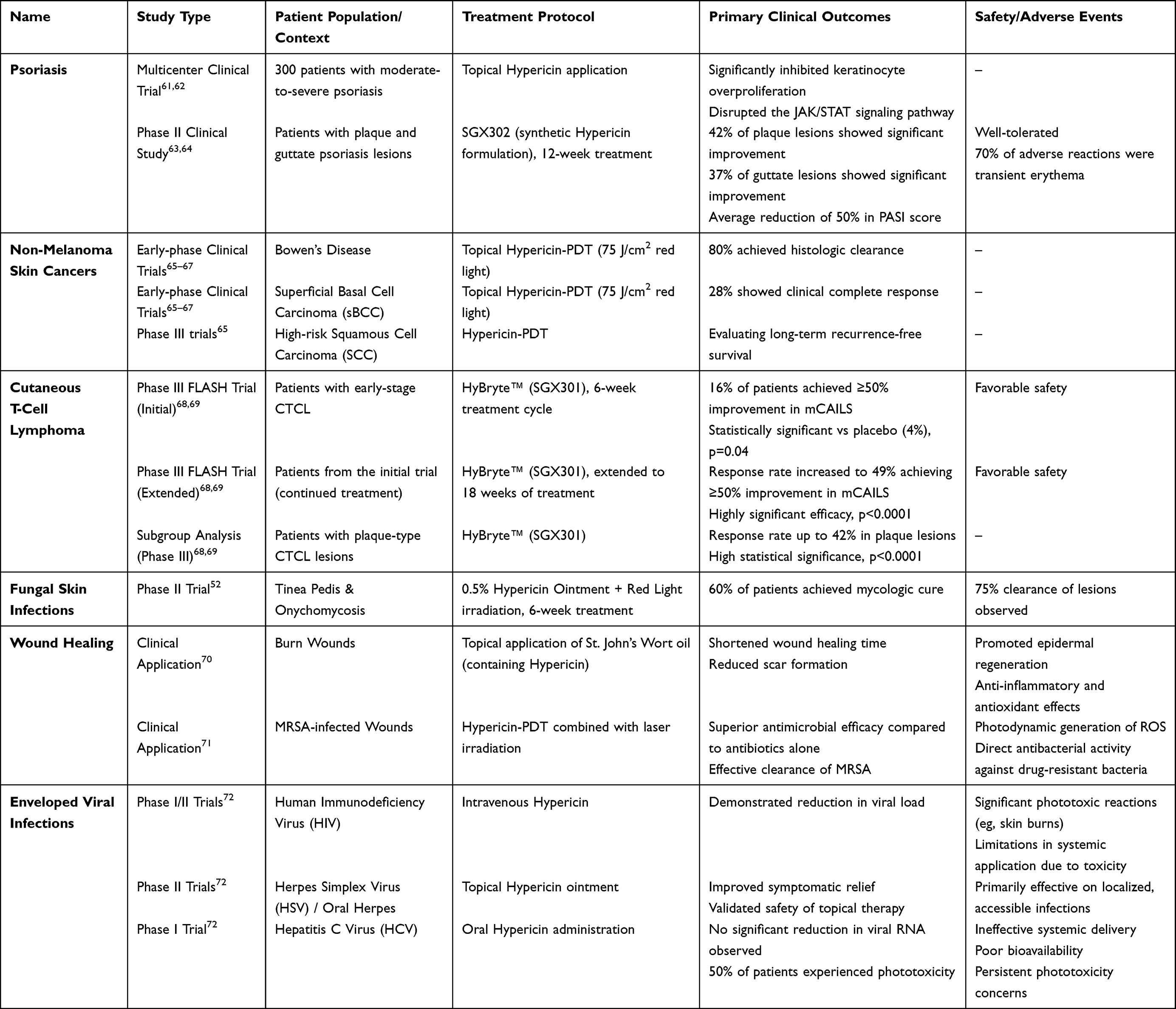 |
Table 1 Clinical Study Results of Hypericin-Based Therapies Across Multiple Disease Indications |
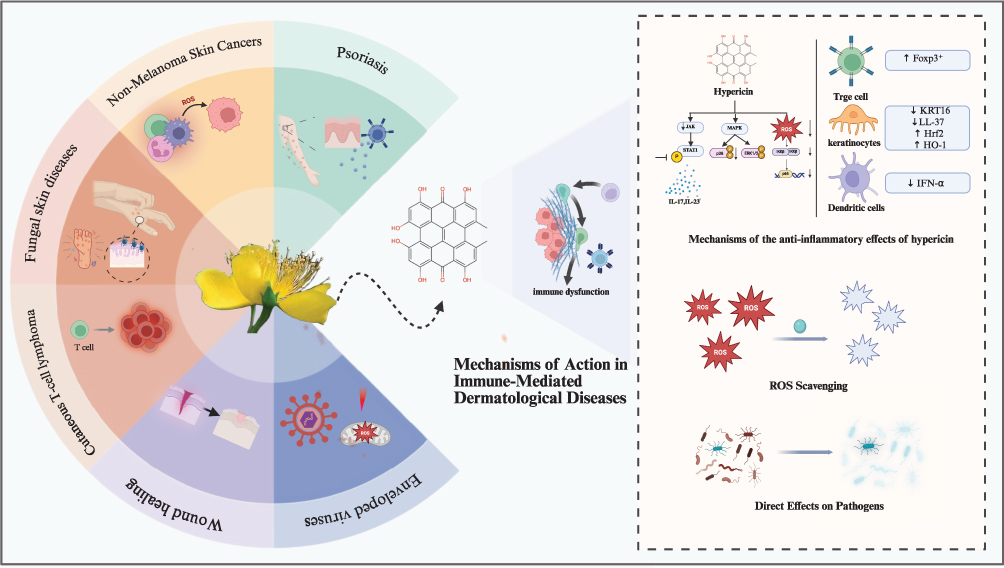 |
Figure 3 Mechanisms of Hypericin in Treating Dermatological Conditions. This schematic illustrates the proposed antiviral, anti-inflammatory, and antitumor mechanisms of Hypericin, a primary bioactive compound in St. John’s Wort, and its potential application in treating conditions like psoriasis, cutaneous T-cell lymphoma, and non-melanoma skin cancers. Figure created with BioRender.com. |
Psoriasis
Psoriasis is a chronic, inflammatory skin disease characterized by hyperproliferation of keratinocytes and dysregulation of the immune system, manifesting as silvery scales and erythematous plaques along with significant inflammation.73 Hypericin, a natural photosensitizer, has emerged as a promising agent in the treatment of psoriasis in recent years, with its therapeutic potential largely attributed to the selective targeting and immunomodulatory properties of PDT.
Preclinical studies suggest that hypericin and its derivative hyperforin can mitigate imiquimod (IMQ)-induced psoriasis-like inflammation in murine models by downregulating IL-17A-producing γδ T cells and associated cytokines.74 Specifically, hyperforin modulates MAPK/STAT3 signaling pathways, resulting in reduced epidermal thickening and lower pathological scores associated with skin lesions while inhibiting CD3+ T cell infiltration. This reduction in inflammatory cytokines, such as IL-1β, IL-6, and IL-23, contributes to improved clinical outcomes. Moreover, Hypericin directly inhibits the overproliferation of keratinocytes and improves abnormal epidermal differentiation by blocking the PKC and JNK1/p38 MAPK signaling pathways.60
The clinical efficacy of hypericin in treating psoriasis has been supported by various studies. A multicenter clinical trial involving 300 patients with moderate-to-severe psoriasis demonstrated that topical hypericin significantly inhibited keratinocyte overproliferation and disrupted the JAK/STAT signaling pathway, critical in inflammation and abnormal keratinocyte proliferation.61,62,75 Furthermore, SGX302, a synthetic Hypericin formulation developed by Soligenix, showed promising results in a Phase II study. After 12 weeks of treatment, 42% of plaque lesions and 37% of guttate lesions exhibited significant improvement, with an average reduction of 50% in the PASI score. The treatment was well tolerated, with 70% of adverse reactions being only transient erythema. Its efficacy is comparable to that of biologics (eg, IL-17 monoclonal antibodies), but it avoids the risks of systemic immunosuppression and infection.63,64 Compared with traditional therapies, Hypericin-PDT offers multiple advantages: its targets cover the key pathological links in psoriasis (T cells and keratinocytes), and it does not require DNA damage (unlike PUVA) or pose long-term carcinogenic risks.76
Recent studies have also explored the potential of Hypericin in combination therapies. For example, when used in conjunction with JAK inhibitors or glycyrrhizic acid nanoparticles, Hypericin can enhance anti-inflammatory effects and reduce dose-dependent side effects.77,78 Although currently reliant on professional phototherapy devices, the development of portable home-based devices (such as Soligenix’s “real-world” approach) is under trial, with the treatment frequency potentially reduced to twice a week. Future directions include optimizing the delivery systems for photosensitizers (eg, lipid nanoparticles) to improve skin penetration and expanding its indications to psoriasis with concomitant fungal infections, leveraging Hypericin’s broad-spectrum antimicrobial properties to achieve dual regulation.77,78
These advancements indicate that Hypericin-PDT is evolving from an adjunctive therapy to a first-line topical treatment option. It offers more precise and safer personalized choices for the management of psoriasis.
Non-Melanoma Skin Cancers - Photodynamic Therapy
Non-melanoma skin cancers (NMSC), which primarily include basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), result from the uncontrolled proliferation of skin cells, often triggered by DNA damage due to ultraviolet (UV) radiation.79,80 This damage leads to mutations in oncogenes and tumor suppressor genes, facilitating tumor development that may invade locally or metastasize. Hypericin demonstrates remarkable tumor-selective cytotoxicity in NMSC through PDT.
Hypericin’s lipophilic nature enables preferential accumulation in cancer cell organelles, such as mitochondria and endoplasmic reticulum, particularly in BCC and SCC. Upon activation by visible light (580–600 nm), hypericin generates ROS via dual mechanisms: Type I reactions produce free radicals (eg, superoxide anions, O2-), while Type II reactions generate singlet oxygen (1O2), a potent cytotoxic agent.6,7,60 With a 1O2 quantum yield exceeding 0.7, hypericin-PDT achieves over 50% apoptosis rates in SCC-25 and MUG-Mel2 cells while sparing HaCaT.7 In an animal subcutaneous tumor model, Hypericin-PDT significantly reduced the size of subcutaneous HK1 tumors, and the mechanisms involved include (a) direct killing of tumor cells by disrupting the cell membrane system or mitochondria, and (b) indirect killing of tumor cells by disrupting the vascular system.81–83
Preclinical studies also highlight its anti-angiogenic effects, disrupting tumor vasculature to suppress growth.65 Compared to conventional photosensitizers like 5-aminolevulinic acid (ALA), hypericin exhibits 10-fold higher phototoxicity in vitro and reduced post-treatment photosensitivity, making it ideal for superficial NMSC lesions such as Bowen’s disease and superficial BCC.6,66
Clinical trials underscore hypericin’s potential as a non-invasive NMSC treatment. Early-phase studies revealed 80% histologic clearance in Bowen’s disease and 28% clinical complete response in superficial BCC after topical hypericin-PDT (75 J/cm2 red light).65–67 However, nodular BCC showed partial responses, emphasizing the need for optimized delivery systems. To overcome hypericin’s poor skin penetration, researchers developed advanced nanocarriers. For instance, hollow microneedles combined with lipid nanocapsules (Donnelly et al) boosted intratumoral drug concentrations while minimizing systemic exposure. Similarly, Pluronic® F127 nanoparticles functionalized with folate ligands improved tumor targeting in SCC models, enhancing PDT efficacy.76,84 Emerging combination strategies—such as hypericin-PDT paired with anti-angiogenic agents or immune checkpoint inhibitors (eg, PD-1 blockers)—have shown synergistic tumor regression in preclinical models. Ongoing Phase III trials are evaluating hypericin-PDT for high-risk SCC, focusing on long-term recurrence-free survival.65
Cutaneous T-Cell Lymphoma
CTCL is a rare and complex form of non-Hodgkin’s lymphoma primarily affecting the skin. It is characterized by the malignant proliferation of skin-homing T cells, which exhibit immunological abnormalities, cytogenetic irregularities, and resistance to apoptosis.85 Research indicates that malignant T cells in CTCL can disseminate and establish secondary lesions throughout the skin, resulting in independent parallel subclonal evolution at various anatomical sites. The clinical manifestations of CTCL may include patches, plaques, and tumors, often accompanied by debilitating symptoms such as pruritus and pain, which adversely affect patients’ quality of life.86
Preclinical studies have shown that Hypericin has potent photodynamic killing effects on CTCL malignant T cells in vitro. Upon activation by visible light, Hypericin generates ROS, which directly disrupts mitochondrial function and activates the caspase apoptotic pathway, inducing malignant cell death (half-maximal inhibitory concentration, IC50, as low as 0.34 μM).49 Its targeting properties stem from the preferential uptake of Hypericin by malignant T cells and remains effective against chemoresistant cells. In addition, Hypericin reverses the immunosuppressive microenvironment by inhibiting the JAK-STAT and NF-κB pathways and down-regulating Th2-type cytokines (eg, IL-4, IL-13), providing a theoretical basis for clinical treatment. In animal models of CTCL, local application of Hypericin combined with visible light significantly inhibited tumor growth (>70% reduction in volume) and demonstrated unique advantages: on the one hand, Hypericin selectively enriched in skin lesions (penetration depth of 2–3 mm), which is particularly suitable for plaque-type CTCL; on the other hand, its systemic absorption is extremely low (blood concentration <0.05 ng/mL) and did not cause hepato-renal toxicity or hepato-kidney toxicity.76 On the other hand, it has a very low systemic absorption (blood concentration <0.05 ng/mL) and does not pose a risk of liver or kidney toxicity or DNA damage.87 Hypericin was also found to reduce intra-lesional regulatory T cells (Treg) and promote CD8+ T cell infiltration, suggesting that its efficacy is enhanced by remodeling the immune microenvironment.76 Experiments in combination with PD-1 inhibitors further showed synergistic anti-tumor effects, laying the foundation for clinical combination therapies.
In terms of clinical translation, HyBryte™ (SGX301), a synthetic version of Hypericin, established its efficacy and safety through multiple pivotal trials. The Phase III FLASH trial demonstrated that a significantly higher proportion of patients with early-stage CTCL improved by ≥50% on the lesion severity index (mCAILS) after 6 weeks of treatment than in the placebo group (16% vs 4%, p=0.04), and the response rate was further increased to 49% with the extension of the treatment period to 18 weeks (p<0.0001).68,69 Notably, Hypericin demonstrated greater penetration and efficacy in traditionally refractory plaque lesions (plaque lesions), with response rates of up to 42% (p<0.0001), which may be related to its superior depth of visible light penetration compared to UV therapy. In terms of safety, no systemic absorption or serious adverse effects were detected in any of the trials, with only a slightly higher incidence of localized skin irritation (16.4%), and there was no risk of DNA damage or secondary malignancy, an advantage that makes it an ideal choice for long-term treatment.88
Fungal Skin Diseases
Fungal skin diseases, also known as dermatomycoses, are primarily caused by the invasion and proliferation of fungi within the keratinized layers of the skin.89,90 These infections often stem from dermatophytes, yeasts, or non-dermatophyte molds that invade the stratum corneum, where they enzymatically break down proteins and lipids to derive necessary nutrients. The resulting immune response to this invasion is characterized by inflammation and can lead to significant tissue damage, particularly in individuals with immunosuppression or compromised skin barriers, such as those with diabetes or dermatological disorders.
Hypericin generates ROS through PDT, destroying fungal cell membranes, proteins and nucleic acids, and inhibiting the activity of key enzymes such as tyrosine kinase, creating a multi-targeted antifungal effect91,92(Figure 2). In vitro studies show that its minimum inhibitory concentration (MIC) against dermatophytes (eg, Trichophyton rubrum, Microsporum canis) is as low as 0.18–46.9 μg/mL, and under light-activated conditions (wavelength of 600–800 nm, light dose of 6–37 J/cm2), its bactericidal rate can reach more than 99.9%.91,93 In addition, Hypericin is also highly effective against Malassezia furfur and Candida albicans, and its combination with antibiotics further reduces the MIC value and enhances the synergistic fungicidal effect.52,91,93 These data provide a solid basis for its broad-spectrum antifungal potential, especially against the main causative agents of superficial fungal infections.92
In animal models, Hypericin has demonstrated significant therapeutic potential and safety. For example, in a white rat skin wound model, a 0.5% Hypericin-containing ointment combined with visible light irradiation (5 J/cm2) reduced the wound area by 97% and inhibited the spread of fungal infections; in a guinea pig model of Trichophyton mentagrophytes infection, Hypericin-PDT treatment reduced the diameter of the lesion by 70%, with a fungal turnaround rate of over 80%.92 In a hamster model of cutaneous leishmaniasis (caused by fungus-like protozoa), twice-weekly application of 0.5% Hypericin cream, combined with low-dose light (5 J/cm2), resulted in complete healing of the lesions within 3 weeks, and histopathology showed a significant decrease in the levels of inflammatory factors (eg, TNF-α, IL-6). This model not only verified the antifungal effect but also revealed the immunomodulatory effect of Hypericin. For the rabbit vaginal mucosa model of Candida albicans infection, Hypericin-PDT (0.625 μM, 37 J/cm2) treatment resulted in a 3 log reduction in fungal load and no mucosal irritation was observed.92 Safety assessment showed no significant damage to skin cells at light doses ≤37 J/cm2, and no hepato- or nephrotoxicity or phototoxicity reactions were detected in long-term application (12 weeks), providing an important basis for its clinical translation.92
While clinical studies of Hypericin-PDT are currently focused on CTCL and psoriasis (eg, the Phase III trial of HyBryte™ demonstrated lesion clearance rates of over 50%), its direct application in fungal dermatoses is beginning to show signs of promise.93 A Phase II trial initially demonstrated that the use of 0.5% Hypericin ointment in combination with red light in the treatment of tinea pedis and onychomycosis, with 60% of patients achieving mycologic cure criteria after 6 weeks; case reports showed 75% clearance of refractory cutaneous candidiasis.52 However, insufficient penetration (relying on nanocarriers to increase local concentration) and standardization of light parameters (eg, adjusting the depth of red light penetration for nail beds) remain major challenges.76 Future directions include advancing phase III trials for drug-resistant S. dermatitidis and S. marcescens infections, developing home-use portable phototherapy devices (eg, Soligenix’s “real-world” trial), and combining traditional antifungal drugs (eg, terbinafine) to enhance synergistic effects.94 With its multi-mechanism action, low risk of resistance, and policy support (FDA orphan drug status), Hypericin has the potential to become a novel option for the treatment of fungal dermatoses, particularly in cases of complicated infections and chronic relapses.
Wound Healing
Wound healing is a multifaceted biological process that consists of four interrelated phases: hemostasis, inflammation, proliferation, and remodeling.95 During the hemostasis phase, platelets aggregate at the site of injury to form a clot, effectively preventing excessive blood loss. This is followed by the inflammation phase, wherein leukocytes are recruited to eliminate pathogens and debris, while releasing growth factors and cytokines that create a conducive environment for subsequent tissue repair. The proliferation phase is marked by the migration and proliferation of fibroblasts and keratinocytes, which are essential for the formation of granulation tissue. These cells synthesize collagen and extracellular matrix components, facilitating the reconstruction of new tissue. Finally, during the remodeling phase, the newly deposited collagen undergoes reorganization and maturation to enhance the strength and functional integrity of the healed tissue.96
Hypericin (Hypericin), as one of the main active ingredients of Onychomycetes, exhibits multi-targeted therapeutic potential in the field of wound healing. Its mechanism of action includes promoting angiogenesis and collagen deposition through the up-regulation of vascular endothelial growth factor (VEGF) and transforming growth factor-β1 (TGF-β1), accelerating the formation of granulation tissue and regeneration of epithelium;70,97,98 meanwhile, it can alleviate the inflammatory response through the inhibition of pro-inflammatory factors (eg, TNF-α, IL-6) and cyclo-oxygenase-2 (COX-2) and protect the function of mitochondria and increase the survival of fibroblasts under the condition of oxidative stress improve fibroblast survival.99 In addition, the photodynamic activity of Hypericin generates ROS, which effectively kills drug-resistant bacteria (eg, MRSA) and enveloped viruses, providing dual protection for infected wounds.71,98
In a rat burn model, topical application of Hypericin significantly shortened the healing time and promoted epidermal regeneration;98 in a diabetic ulcer model, it improved the microenvironment of chronic wounds through the upregulation of antioxidant genes (SOD1, GPX1) and the inhibition of matrix metalloproteinases (MMP2/9);9 PDT combined with laser irradiation in MRSA-infected mice demonstrated efficient in MRSA-infected mice.71 In vitro experiments further revealed that Hypericin promotes the proliferation and migration of fibroblasts by activating the TGF-β signaling pathway, and protects normal cells by regulating apoptosis-related pathways.70
In terms of clinical application, the topical application of traditional St. John’s wort oil can shorten the healing time of burns and reduce scarring;70 and the antimicrobial efficacy of the combination dressing of Hypericin-PDT was superior to that of antibiotics for MRSA-infected wounds.71 In terms of safety, the incidence of phototoxicity (eg, erythema, pruritus) is low (5–16%) and can be controlled by light-avoidance management; however, high doses of intravenous injection may cause elevated liver enzymes, and caution should be exercised in breastfeeding applications.100,101 Hypericin shows some promise in trauma therapy due to its multi-targeted effects (pro-healing, anti-inflammatory, antibacterial) and low toxicity.
Enveloped Viruses
Enveloped viruses, including prominent pathogens such as influenza virus, human immunodeficiency virus (HIV), and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), possess a lipid bilayer acquired from the host cell membrane during viral assembly.102,103 This lipid envelope facilitates viral entry into host cells through membrane fusion, subsequently initiating a complex replication cycle. This cycle entails the release of viral RNA or DNA, transcription and translation of viral genes, and the assembly and release of new virions.104 Notably, the viral envelope plays a pivotal role in evading host immune responses, providing a shield against neutralizing antibodies and allowing for persistent infections.
Hypericin shows a unique potential in the treatment of enveloped viral diseases thanks to its photosensitizing properties and multi-targeted mechanism of action. Its antiviral activity is mainly mediated by photodynamic inactivation (PDI): activated by visible light (590 nm), Hypericin generates ROS such as 1O2, which destroys the lipid layer of the viral envelope and the capsid proteins, eg, in the case of HIV it prevents viral exfoliation by cross-linking the capsid protein p24.105,106 In addition, Hypericin can directly bind to viral glycoproteins (eg, Spike protein of SARS-CoV-2 or gB/gD of HSV-1), interfering with the membrane fusion process between the virus and the host cell, and in vitro experiments have shown that pre-treatment of HSV-1 particles reduces infectivity by up to 90%. In addition to physical disruption, Hypericin targets key viral enzyme activities, such as inhibiting the alkaline nuclease (AN) of HSV-1 to block DNA processing (EC50 of 2.59–2.94 μM), and hinders viral outgrowth by interfering with the PKC signaling pathway of the host cell, which in HIV mouse models significantly reduced viral load.6,72,106
Hypericin showed broad-spectrum antiviral effects in experimental studies against different enveloped viruses. In vitro experiments on HIV showed that its photodynamic effect could inhibit reverse transcriptase activity (IC50 of 0.3 μM), while on herpesvirus (HSV-1), it could block the infection at multiple stages of adsorption, penetration and replication, resulting in the retention of the nucleocapsid in the cell nucleus.106 In the field of coronaviruses, Hypericum extract and purified Hypericin were effective against SARS-CoV-2 Alpha, Beta, and Delta variants (EC50 of 10–15 μg/mL) by a mechanism related to the inhibition of Spike protein function.107 In addition, studies on influenza virus (disruption of hemagglutinin), dengue virus (inhibition of E-protein expression), and infectious bronchitis virus (IBV) have confirmed its role in apoptosis and immunomodulation through ROS induction.6,108
Despite the promising experimental studies, Hypericin’s clinical application still faces multiple challenges. Early phase I/II trials in HIV (1990s) found that intravenous administration reduced viral load, but phototoxic reactions (eg, skin burns) limited systemic application; subsequent phase II trials that shifted to topical administration (eg, oral herpes ointment) demonstrated improved symptomatic relief, validating the safety of topical therapy.72 In a phase I trial in hepatitis C (HCV), oral Hypericin did not significantly reduce viral RNA and 50% of patients experienced phototoxicity, suggesting limitations in systemic delivery. There is a lack of formal clinical trial data in the area of COVID-19, although preliminary studies support its potential for adjuvant therapy.72
There is a lack of formal clinical trial data in the area of COVID-19, although preliminary studies support its potential for adjuvant therapy. The central bottleneck is the light-dependent limitation: light is required to activate the activity, and precise light control is difficult during systemic administration, which can lead to side effects. In addition, Hypericin binds to serum albumin resulting in lower free concentrations, and poor aqueous solubility (dependent on DMSO or NaOH solubilization) further limits bioavailability.109 Although its multi-targeting mechanism may delay resistance, sustained efficacy against rapidly mutating strains such as Omicron needs to be verified.
Mechanisms of Action in Immune-Mediated Dermatological Diseases
Anti-Inflammatory Effects
Hypericin anti-inflammatory mechanism involves multi-pathway regulation. Basic research has shown that Hypericin acts by inhibiting the expression of key inflammatory mediators. For example, in a lipopolysaccharide (LPS)-stimulated RAW 264.7 macrophage model, Hypericin significantly reduced nitric oxide (NO) levels and inhibited the gene expression of inducible nitric oxide synthase (iNOS), COX-2, and pro-inflammatory cytokines (eg, TNF-α, IL-1β, and IL-6).99 Further studies revealed that this inhibitory effect may be associated with the blockade of the NF-κB signaling pathway, which reduces the transcription of downstream inflammatory factors. In addition, Hypericin has been shown to inhibit 12-lipoxygenase (12-LOX) and protein kinase C (PKC), both of which exacerbate inflammation by promoting leukotriene and ROS production in the inflammatory cascade.110,111 Molecular modeling studies further revealed that Hypericin may interfere with the JAK-STAT signaling pathway by binding to the ATP-binding site of Janus kinase (JAK1), thereby inhibiting the inflammatory response.21 These multi-target mechanisms of action provide a theoretical basis for the broad-spectrum anti-inflammatory activity of Hypericin.
Several preclinical experiments validated the anti-inflammatory potential of Hypericin. In the LPS-induced macrophage inflammation model, Hypericin inhibited NO production in a concentration-dependent manner (IC50 = 5 μM) without significant cytotoxicity.99 In addition, Hypericin treatment significantly reduced iNOS and COX-2 protein levels and was also confirmed by qRT-PCR that it could down-regulate the mRNA expression of TNF-α, IL-1β and IL-6. It is worth noting that the photosensitizing properties of Hypericin may affect its mode of action: in the absence of light, its anti-inflammatory activity is mainly achieved through enzyme inhibition; whereas, when light activation occurs, the generated 1O2 can further disrupt the membrane structure of inflammatory cells and enhance the anti-inflammatory effect112 (Figure 4).
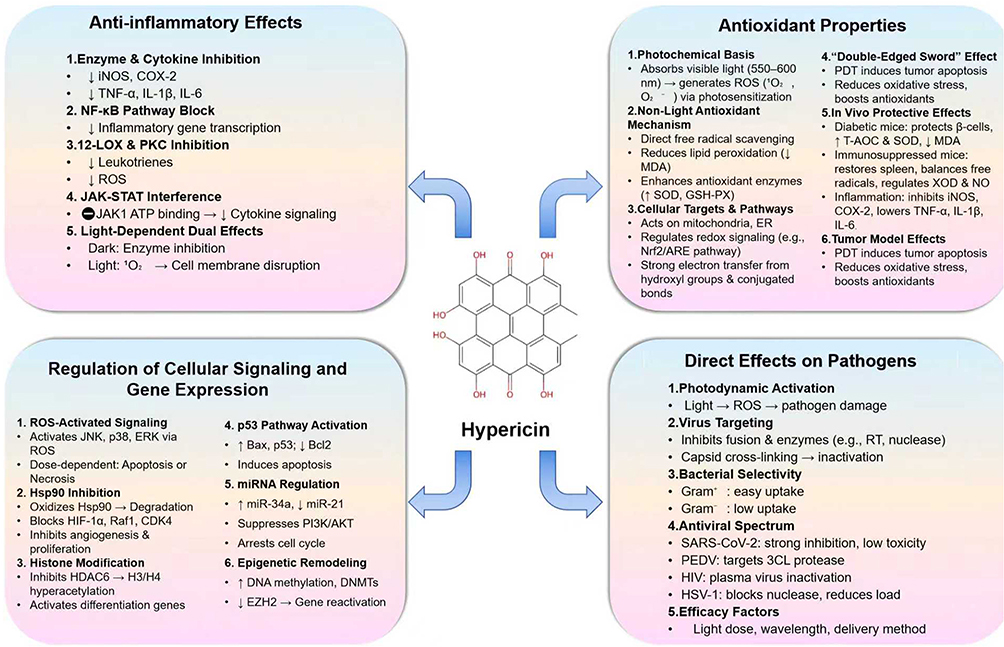 |
Figure 4 Mechanisms of Action in Immune-Mediated Dermatological Diseases. The diagram illustrates the pleiotropic pharmacological mechanisms of Hypericin, which underpin its therapeutic potential. These actions are categorized into four primary domains: (1) Anti-inflammatory Effects, (2) Antioxidant Properties, (3) Regulation of Cellular Signaling and Gene Expression, and (4) Direct Effects on Pathogens. Symbols: ↑: Induction/Activation; ↓: Inhibition/Suppression; →: Leads to/Promotes. |
Antioxidant Properties
The antioxidant activity of Hypericin is closely related to its unique photochemical properties. As a naphthalene dianthrone compound, Hypericin absorbs visible light (maximum absorption peak located at 550–600 nm) under light illumination and generates ROS, including 1O2 and O2- through photosensitization, which then triggers an oxidative stress response.60,113 However, its antioxidant mechanism under non-light conditions is characterized by its direct scavenging capacity for free radicals. For example, Hypericin can reduce the production of oxidation products such as malondialdehyde (MDA) and up-regulate the activities of endogenous antioxidant enzymes such as superoxide dismutase (SOD) and glutathione peroxidase (GSH-PX) by inhibiting lipid peroxidation.114,115 It was also found that Hypericin can target mitochondria, endoplasmic reticulum and other organelles, and enhance cellular antioxidant defense by regulating redox signaling pathways (eg, Nrf2/ARE pathway).114 In addition, the multiple hydroxyl groups and the conjugated double bond system in its structure endow it with a strong electron transfer capacity, which can directly neutralize free radicals.116 It is worth noting that the antioxidant effects of Hypericin have a “double-edged sword” character: in PDT, it induces apoptosis in cancer cells through ROS generation, while in non-photo-irradiated conditions, it protects normal cells by scavenging free radicals.117 For example, in melanoma cells, Hypericin-PDT significantly increased the level of the lipid peroxidation product TBARS while inhibiting GSH-PX activity; however, in normal hepatocytes, it attenuated oxidative damage by increasing SOD activity.117 This selective effect makes it potentially applicable in antioxidant therapy.
In animal models, Hypericin demonstrated protective effects against a variety of oxidative stress-related diseases. For example, in high-fat-high-sugar (HFHS)-induced diabetic mice, Hypericin protects pancreatic islet β-cells from glycolipotoxic damage by elevating the total antioxidant capacity (T-AOC) and SOD activity of pancreatic tissues, and significantly decreasing MDA levels.114 In an immunosuppressed mouse model, Hypericin not only restored spleen index, but also ameliorated oxidative damage to immune function by regulating xanthine oxidase (XOD) and NO levels and balancing the free radical generation and scavenging system. In inflammation models, Hypericin indirectly reduces inflammation-related oxidative stress by inhibiting the expression of iNOS and COX-2 and reducing the release of pro-inflammatory cytokines (TNF-α, IL-1β, IL-6).99 In addition, its photodynamic properties exhibited dual regulation in tumor models: on the one hand, it induced apoptosis in cancer cells via ROS, and on the other hand, it suppressed oxidative imbalance in the tumor microenvironment by activating anti-angiogenesis and immune response.60 For example, in the RIF-1 mouse tumor model, Hypericin-PDT reduced hypoxia-induced ROS overproduction by disrupting the tumor vascular system while enhancing local antioxidant enzyme activities118 (Figure 4).
Regulation of Cellular Signaling and Gene Expression
Hypericin regulates cell signaling pathways through multiple pathways, and its core mechanism involves ROS-mediated kinase activation and inhibition. Studies have shown that Hypericin generates ROS in response to light, which activates the JNK, p38 MAPK and ERK signaling pathways through Type I and Type II photodynamic responses, thereby inducing apoptosis or necrosis, depending on the concentration and light dose.60,118 For example, high doses of Hypericin led directly to cell necrosis via ROS, whereas intermediate doses achieved programmed death via activation of pro-survival or pro-apoptotic signaling.60,119,120 In addition, Hypericin’s targeting of Hsp90 is particularly critical: it selectively binds to and oxidizes Hsp90, inducing its polyubiquitination and degradation, thereby disrupting Hsp90’s interactions with a variety of client proteins (eg, HIF-1α, Raf1, and CDK4), and inhibiting tumor angiogenesis and cell proliferation.121 This process also leads to hyperacetylation of histones H3 and H4 by inhibiting HDAC6 activity, which in turn relaxes chromatin structure and activates the expression of differentiation-related genes, ultimately inducing differentiation of glioblastoma cells.122
Hypericin exerts anti-tumor effects through epigenetic modifications and regulation of key gene expression. In hepatocellular carcinoma cells Huh7, Hypericin significantly up-regulated the mRNA expression of pro-apoptotic genes Bax and p53, while down-regulating the anti-apoptotic gene Bcl2, and the accumulation of p53 protein was verified by immunocytochemistry, which indicated that it relied on the p53 pathway to induce apoptosis.123 In breast cancer cells MCF7, Hypericin regulated the expression of its target genes PTEN, TP53, BCL2 and CDK4 by up-regulating miR34a and down-regulating miR21, inhibiting the PI3K/AKT signaling pathway and promoting cell cycle arrest.124–126 In addition, Hypericin can remodel the epigenetic features of tumor cells and suppress the malignant phenotype by increasing genome-wide DNA methylation levels (eg, 5-methylcytosine) and upregulating DNA methyltransferases (DNMT1, DNMT3a/b).16,122 In glioblastoma, this epigenetic regulation further leads to repression of the expression of EZH2, a component of the multi-combs repressive complex, and unsilencing of differentiation genes122 (Figure 4).
Direct Effects on Pathogens
The core mechanism of Hypericin’s action against pathogens relies on photodynamic effects. Hypericin enters the excited state by efficiently absorbing light energy and generates large amounts of ROS. These ROS directly damage cell membranes or viral envelope structures by oxidatively damaging key biomolecules of the pathogen (eg, lipids, proteins, and nucleic acids).127 For enveloped viruses (eg, HIV, HSV-1), Hypericin blocks viral replication by interfering with the fusion process between the virus and the host cell through photoactivation and by inhibiting the activity of viral enzymes (eg, reverse transcriptase, HSV-1 alkaline nuclease).106,127,128 In addition, Hypericin cross-links with viral capsid proteins, leading to viral inactivation.128 In bacteria, its action is selective: as Gram-positive bacteria (eg, Staphylococcus aureus) lack an outer membrane barrier, Hypericin penetrates efficiently and accumulates intracellularly, whereas Gram-negative bacteria (eg, Escherichia coli) have a significantly lower uptake rate due to the barrier of the outer membrane polysaccharide layer.91
Preclinical and clinical studies have shown that Hypericin has broad-spectrum inhibitory potential against a wide range of viruses. In in vitro experiments, Hypericin (IC50 = 1.11 pmol/mL) significantly inhibited the infectivity of SARS-CoV-2 pseudoviruses and real viruses with very low cytotoxicity (CC50 > 100 μg/mL), demonstrating a high selectivity index.107 Against α-coronaviruses (eg, porcine epidemic diarrhea virus PEDV), Hypericin inhibits viral replication by targeting the 3CL protease (a key viral replicative enzyme), and molecular docking assays confirm its high-affinity binding to the enzyme active site.129 In HIV treatment, Hypericin’s photodynamic therapy inactivates viral particles in plasma and inhibits syncytium formation, providing a new strategy for blood product safety.127,128 In addition, clinical trials against HSV-1 have demonstrated that Hypericin blocks viral nuclease activity, resulting in retention of the nucleocapsid in the host cell nucleus and significant reduction of viral load (>99%).106 Notably, the antiviral effect of Hypericin is dependent on the optimization of photoactivation conditions (wavelength, dose) and route of administration (Figure 4).
Comparative Analysis with Other Immunomodulators
Comparison with Synthetic Immunosuppressants
As a natural photosensitizer, Hypericin’s mechanism of action is mainly dependent on the generation of ROS in PDT, and selectively kills aberrant cells by targeting the activation of mitochondrial apoptotic pathway, showing significant inhibition of malignant T-cell proliferation, especially in CTCL and psoriasis models, and also showing potential for precision therapy due to optimization of topical penetration (eg, co-menthol pro-permeability) and low toxicity to normal tissues, showing potential for precision therapy.60,74,130 In contrast, synthetic immunosuppressants (eg, glucocorticoids, tacrolimus, methotrexate) achieve broad immunosuppression through systemic blockade of immune responses (eg, inhibition of pro-inflammatory factor transcription, disruption of T-cell signaling, or DNA synthesis); however, their multi-targeted effects may lead to systemic side effects such as myelosuppression and liver and renal toxicity, and lack of lesion-specificity, which predispose to elevated infection risk.131–133 The core difference between the two lies in the mode of action: Hypericin relies on light-activated local targeting, whereas synthetic drugs are based on systemic immunosuppression, presenting the challenge of balancing efficacy and safety.
In clinical trials, phase III/II studies of Hypericin-PDT (eg, HyBryte) in early-stage CTCLand psoriasis have shown significantly better disease remission rates than placebo (95% CI 2.0–11.5 for complete remission rate), and the safety profile is highlighted by predominantly localized irritation (<17% incidence) with no risk of systemic accumulation.68 In contrast, synthetic immunosuppressants (eg, the JAK inhibitors tofacitib and mertiomacrophenol ester), although effective in a wide range of indications such as atopic dermatitis and lupus erythematosus, require vigilance against serious systemic risks such as thrombosis and infections (eg, black box warning).134 Topical formulations (eg, tacrolimus ointment) reduce systemic exposure, but long-term safety needs to be verified. Overall, Hypericin is more suitable for precision treatment of limited skin lesions, whereas synthetic drugs are indispensable in severe or systemic dermatoses, but side effects need to be strictly monitored. Future studies may need to explore nanocarrier delivery of Hypericin to break through the limitations of light penetration depth and combine it with synthetic drugs to achieve synergistic effects.
Comparison with Other Natural Products
Hypericin mechanism of action contrasts with other natural products in multiple dimensions. Among the anti-inflammatory mechanisms, Hypericin significantly reduces the inflammatory response by inhibiting PKC and regulating the expression of various cytokines, including increasing anti-inflammatory cytokines like IL-4 and IL-10.6,52 Curcumin acts by blocking the NF-κB pathway and inhibiting COX-2 enzyme activity, which helps reduce the production of pro-inflammatory cytokines and mediators.135 As for antioxidant activity, Hypericin scavenges free radicals by generating ROS through photoactivation. However, this process is only effective when specific wavelengths of light are used. In contrast, mangiferin and lutein exhibit more direct antioxidant effects: mangiferin neutralizes free radicals and complexes metal ions, thereby reducing oxidative stress, while lutein protects skin lipids and collagen by absorbing UV light.136,137 Regarding antimicrobial properties, Hypericin demonstrates a photo-oxidative effect against viruses (eg, HIV, HSV) and bacteria under specific light conditions.105,106,138 In contrast, Tea Tree Oil and honey rely on the natural antimicrobial activities of monoterpenes (eg, terpinen-4-ol) and peroxidases.105,106,138 Among anti-cancer mechanisms, Hypericin’s PDT achieves targeted killing by inducing apoptosis (activation of Caspase-3/9) and destroying tumor vasculature.119,139,140 Resveratrol and green tea extract (EGCG) work by inhibiting tumor cell proliferation signals (eg, the PI3K/Akt pathway) and inducing autophagy.141–143 Additionally, Hypericin’s modulation of the dopamine system (eg, inhibition of dopamine β-hydroxylase) may indirectly affect cutaneous neurogenic inflammation, a mechanism that is rare among other natural products.60,144
In terms of clinical efficacy, Hypericin showed significant results in PDT for CTCL, with a 49% lesion remission rate in a phase III clinical trial and no serious adverse effects.68 In contrast, curcumin showed dose-dependent inflammation-reducing effects in eczema and psoriasis, but was limited by low bioavailability and required nanocarrier technology to enhance efficacy.135,145–147 Clinical data on resveratrol in anti-photo-aging and hyperpigmentation are mainly based on topical formulations, and stability issues remain a bottleneck for dissemination.148
In conclusion, Hypericin has unique advantages in terms of targeting and mechanistic complexity, especially in the field of PDT, but its application scenarios are relatively limited, while other natural products (eg, curcumin, resveratrol) are more generalizable in the management of generalized skin diseases by virtue of their multiplexed effects and low toxicity.
Advantages and Disadvantages of Hypericin as a Foundational Treatment
Hypericin, a core component of PDT, has demonstrated multi-dimensional benefits in the treatment of skin diseases. Basic research has confirmed that its photoactivation generates ROS and single-linear oxygen species, which achieve multi-targeted anti-tumor effects by destroying key tumor cell molecules, activating apoptotic pathways (eg, caspase-9/3), inhibiting pro-oncogenic signals (PKC/EGFR), and interfering with metabolic enzyme activities (eg, succinate dehydrogenase), and selectively accumulates due to the high permeability of tumor tissues, with low systemic toxicity (LD50 significantly higher than therapeutic doses).13,76 Meanwhile, its light-dependent antiviral mechanism disrupts the envelope viral structure and down-regulates pro-inflammatory factors such as IL-6, providing a new strategy for infectious and inflammatory skin diseases.13 In clinical application, the phase III trial (FLASH trial) showed its remission rate of up to 49% in early-stage CTCL, which was significantly better than that of the placebo group, and the 0.5% gel in combination with light promoted lesion healing in a model of leishmaniasis, which was both non-invasive (localized erythema/pruritus only) and safe (no blood levels detected), which was significantly superior to conventional chemotherapy in terms of DNA damage Risk.130
Despite its potential, Hypericin faces multiple limitations. At the basic level, its poor water solubility (easily aggregated into inactive molecules) and high molecular weight (504 Da) lead to low transdermal efficiency, which needs to be improved by nanocarriers; light-dependent therapeutic efficacy (550–600 nm wavelength) reduces the systemic toxicity, but triggers the risk of photosensitization, and it may weaken the efficacy of cisplatin and other chemotherapeutic drugs through the up-regulation of drug-resistant proteins, such as MRP1.54,149,150 In clinical practice, the complete remission rate of BCC and SCC varies among individuals, and the efficacy is affected by the size of the lesion, the light parameters and the frequency of administration, which requires the optimization of individualized regimens; about 16.4% of patients experienced pain or erythema at the treatment site, and multiple light exposure (twice a week) may reduce compliance.67,130,151 In addition, most of the existing studies focus on CTCL and infectious dermatoses, and there is a lack of data on common inflammatory diseases such as atopic dermatitis, and breakthroughs are still needed in the exploration of mechanisms and expansion of indications.
Conclusion and Future Prospects
Unresolved Issues and Areas for Further Research
There are still multiple bottlenecks in the use of Hypericin in the treatment of skin diseases. The balance between the risk of phototoxicity and the therapeutic window is the core challenge: its potent photosensitizing properties may damage healthy tissues while killing lesion cells, for example, its enhanced permeability significantly increases phototoxicity risks. Critically, available clinical data show only 33% of sun-damaged actinic keratosis lesions achieved complete response to HY-PDT, suggesting inadequate drug accumulation in deeper tissue layers and limited therapeutic efficacy.6,152 Inefficient drug delivery further constrains application, as Hypericin’s hydrophobicity (water solubility <0.1 mg/mL) and large molecular weight (504 Da) make it difficult to penetrate the epidermis, and it is particularly ineffective against thick plaques or deep-seated tumors.130,150,153 In addition, long-term safety and resistance mechanisms are unknown. Although phase III trials have shown that adverse effects are mild to moderate (eg, local irritation), the carcinogenic risk (eg, melanoma) and potential effects on the immune system (eg, T-cell suppression) under repeated light exposure need to be verified, and it is inconclusive whether resistance is related to autophagy pathway activation.68
Potential for Developing Novel Hypericin-Based Therapies
Hypericin, a natural photosensitizer extracted from Hypericum perforatum, shows great promise in the treatment of skin diseases due to its photodynamic effect. To break through the limitations of Hypericin’s low water solubility and poor photostability, novel delivery technologies have become the focus of research.154,155 Nanocarriers (eg, PLA nanoparticles, liposomes, and Pluronic® micelles) can significantly enhance their cellular uptake and tumor targeting. For instance, folic acid-modified nanoparticles increased phototoxicity 3-fold in melanoma treatment.84 Combination therapies (eg, with doxorubicin or immunomodulators) amplify ROS killing through synergistic effects, and graphene oxide-loaded systems have achieved a 60% increase in tumor inhibition in mitochondrial targeting.13,155 Future directions focus on two-photon activation systems (penetration depth up to 5 mm), bionic delivery (exosome carriers) and smart response formulations (pH/photorelease) to optimize topical slow-release treatments for chronic inflammatory skin diseases such as psoriasis.
Conclusion
Hypericin, the principal photosensitiser of Hypericum perforatum (St. John’s wort), unites anticancer, antimicrobial and neuroprotective activities in one molecule. Pre-clinical and early-phase studies confirm that light-activated hypericin selectively induces tumour-cell apoptosis and eradicates multidrug-resistant microbes, providing a clinically scalable option for patients with CTCL, severe acne or chronic fungal infections who fail standard care. Its translation to first-line therapy is nevertheless blocked by poor water solubility, limited skin penetration, a narrow phototoxic window and a lack of long-term safety data. Future work should prioritise: 1) nano-carriers, micro-emulsions or liposomes to enhance lesion accumulation while reducing systemic exposure; 2) PDT-plus-immunomodulation regimens (eg, anti-PD-1, CTLA-4) to amplify tumour immunogenicity; 3) large-scale, multicentre, randomised trials to establish optimal light-dose parameters, dosing frequency and late-onset adverse events. Moreover, efficacy in pigmented or immune-privileged sites and safety in children and immunosuppressed individuals remain undefined and demand systematic investigation. Synergising formulation innovation with evidence-based research will advance hypericin from bench-top photosensitiser to a precision dermatologic modality, equipping clinicians with a safe, effective and economical tool for the most challenging skin diseases.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China under Grant number 82374453 and 82074434.
Disclosure
The authors declare no competing interest.
References
1. Laforet K, Woodbury GM, Sibbald RG. Wound bed preparation and complementary and alternative medicine. Adv Skin Wound Care. 2011;24(5):226–21. doi:10.1097/01.ASW.0000397896.10380.5a
2. Yi J, Yang X, Zheng L, et al. Photoactivation of hypericin decreases the viability of RINm5F insulinoma cells through reduction in JNK/ERK phosphorylation and elevation of caspase-9/caspase-3 cleavage and Bax-to-Bcl-2 ratio. Biosci Rep. 2015;35(3):e00195. doi:10.1042/BSR20150028
3. Menegazzi M, Masiello P, Novelli M. Anti-tumor activity of Hypericum perforatum L. and hyperforin through modulation of inflammatory signaling, ROS generation and proton dynamics. Antioxidants. 2020;10(1):18.
4. Schempp CM, Müller KA, Winghofer B, Schöpf E, Simon JC. Johanniskraut (Hypericum perforatum L.) Eine Pflanze mit Relevanz für die Dermatologie: eine Pflanze mit Relevanz für die Dermatologie. Der Hautarzt. 2002;53(5):316–321. doi:10.1007/s00105-001-0317-5
5. Rook AH, Wood GS, Duvic M, et al. A phase II placebo-controlled study of photodynamic therapy with topical hypericin and visible light irradiation in the treatment of cutaneous T-cell lymphoma and psoriasis. J Am Acad Dermatol. 2010;63(6):984–990. doi:10.1016/j.jaad.2010.02.039
6. Wölfle U, Seelinger G, Schempp CM. Topical application of St. John’s wort (Hypericum perforatum). Planta Med. 2014;80(02/03):109–120. doi:10.1055/s-0033-1351019
7. Woźniak M, Nowak-Perlak M. Hypericin-based photodynamic therapy displays higher selectivity and phototoxicity towards melanoma and squamous cell cancer compared to normal keratinocytes in vitro. Int J Mol Sci. 2023;24(23):16897. doi:10.3390/ijms242316897
8. Galinari CB, Conrado PCV, Arita GS, et al. Nanoencapsulated hypericin in P-123 associated with photodynamic therapy for the treatment of dermatophytosis. J Photochem Photobiol B Biol. 2021;215:112103. doi:10.1016/j.jphotobiol.2020.112103
9. Anastasiou IA, Sarantis P, Eleftheriadou I, et al. Effects of hypericin on cultured primary normal human dermal fibroblasts under increased oxidative stress. Int J Low Extrem Wounds. 2023:15347346231212332. doi:10.1177/15347346231212332
10. Farasati Far B, Gouranmohit G, Naimi Jamal MR, et al. The potential role of Hypericum perforatum in wound healing: a literature review on the phytochemicals, pharmacological approaches, and mechanistic perspectives. Phytother Res. 2024;38(7):3271–3295. doi:10.1002/ptr.8204
11. Kapinus EI, Falk H, Tran HT. Spectroscopic investigation of the molecular structure of hypericin and its salts. Monatshefte Fuèr Chemie. 1999;130(5):623–635.
12. Lavie G, Mazur Y, Lavie D, Meruelo D. The chemical and biological properties of hypericin—a compound with a broad spectrum of biological activities. Med Res Rev. 1995;15(2):111–119. doi:10.1002/med.2610150203
13. Wu J, Zhang J, Xia C, et al. Hypericin: a natural anthraquinone as promising therapeutic agent. Phytomedicine. 2023;111:154654. doi:10.1016/j.phymed.2023.154654
14. Barnes J, Anderson LA, Phillipson JD. St John’s wort (Hypericum perforatum L.): a review of its chemistry, pharmacology and clinical properties. J Pharm Pharmacol. 2001;53(5):583–600. doi:10.1211/0022357011775910
15. Butterweck V. Mechanism of action of St John’s wort in depression: what is known? CNS Drugs. 2003;17:539–562.
16. Lei C, Li N, Chen J, Wang Q. Hypericin ameliorates depression-like behaviors via neurotrophin signaling pathway mediating m6a epitranscriptome modification. Molecules. 2023;28(9):3859. doi:10.3390/molecules28093859
17. Galeotti N. Hypericum perforatum (St John’s wort) beyond depression: a therapeutic perspective for pain conditions. J Ethnopharmacol. 2017;200:136–146.
18. Hudson JB, Lopez-Bazzocchi I, Towers G. Antiviral activities of hypericin. Antiviral Res. 1991;15(2):101–112. doi:10.1016/0166-3542(91)90028-P
19. Sytar O, Švedienė J, Ložienė K, et al. Antifungal properties of hypericin, hypericin tetrasulphonic acid and fagopyrin on pathogenic fungi and spoilage yeasts. Pharm Biol. 2016;54(12):3121–3125. doi:10.1080/13880209.2016.1211716
20. Schempp CM, Pelz K, Wittmer A, Schöpf E, Simon JC. Antibacterial activity of hyperforin from St John’s wort, against multiresistant Staphylococcus aureus and gram-positive bacteria. Lancet. 1999;353(9170):2129. doi:10.1016/S0140-6736(99)00214-7
21. Dellafiora L, Galaverna G, Cruciani G, Dall Asta C, Bruni R. On the mechanism of action of anti-inflammatory activity of hypericin: an in silico study pointing to the relevance of Janus kinases inhibition. Molecules. 2018;23(12):3058.
22. Caldeira GI, Gouveia LP, Serrano R, Silva OD. Hypericum genus as a natural source for biologically active compounds. Plants. 2022;11(19):2509.
23. Liebes L, Mazur Y, Freeman D, et al. A method for the quantitation of hypericin, an antiviral agent, in biological fluids by high-performance liquid chromatography. Anal Biochem. 1991;195(1):77–85. doi:10.1016/0003-2697(91)90298-8
24. Smelcerovic A, Spiteller M, Zuehlke S. Comparison of methods for the exhaustive extraction of hypericins, flavonoids, and hyperforin from Hypericum perforatum L. J Agric Food Chem. 2006;54(7):2750–2753. doi:10.1021/jf0527246
25. Alahmad A, Alghoraibi I, Zein R, et al. Identification of major constituents of Hypericum perforatum L. extracts in Syria by development of a rapid, simple, and reproducible HPLC-ESI-Q-TOF MS analysis and their antioxidant activities. ACS Omega. 2022;7(16):13475–13493. doi:10.1021/acsomega.1c06335
26. Da Silva RP, Rocha-Santos TA, Duarte AC. Supercritical fluid extraction of bioactive compounds. TrAC Trends Anal Chem. 2016;76:40–51.
27. Riera E, Blanco A, García J, et al. High-power ultrasonic system for the enhancement of mass transfer in supercritical CO2 extraction processes. Physics Procedia. 2010;3(1):141–146. doi:10.1016/j.phpro.2010.01.020
28. Cao X, Wang Q, Li Y, et al. Isolation and purification of series bioactive components from Hypericum perforatum L. by counter-current chromatography. J Chromatogr B. 2011;879(7–8):480–488. doi:10.1016/j.jchromb.2011.01.007
29. Gonçalves RS, César GB, Barbosa PM, et al. Optimized protocol for multigram preparation of emodin anthrone, a precursor in the hypericin synthesis. Nat Prod Res. 2019;33(8):1196–1199. doi:10.1080/14786419.2018.1457661
30. Huang L, Zeng-Hui W, Shi-Lin C. Hypericin: chemical synthesis and biosynthesis. Chin J Nat Med. 2014;12(2):81–88. doi:10.1016/S1875-5364(14)60014-5
31. Xu M, Yang B, Dong J, et al. Enhancing hypericin production of Hypericum perforatum cell suspension culture by ozone exposure. Biotechnol Prog. 2011;27(4):1101–1106.
32. Cai F, Li Y, Zhang M, et al. Combination of integrated expanded bed adsorption chromatography and countercurrent chromatography for the direct extraction and purification of pseudohypericin and hypericin from St. John’s wort (Hypericum perforatum L.). J Sep Sci. 2015;38(15):2588–2596. doi:10.1002/jssc.201500260
33. Kerb R, Brockmöller J, Staffeldt B, Ploch M, Roots I. Single-dose and steady-state pharmacokinetics of hypericin and pseudohypericin. Antimicrob Agents Chemother. 1996;40(9):2087–2093. doi:10.1128/AAC.40.9.2087
34. Peng Z, Lu J, Liu K, et al. Hypericin as a promising natural bioactive naphthodianthrone: a review of its pharmacology, pharmacokinetics, toxicity, and safety. Phytother Res. 2023;37(12):5639–5656. doi:10.1002/ptr.8011
35. Schulz H, Schürer M, Bässler D, Weiser D. Investigation of pharmacokinetic data of hypericin, pseudohypericin, hyperforin and the flavonoids quercetin and isorhamnetin revealed from single and multiple oral dose studies with a hypericum extract containing tablet in healthy male volunteers. Arzneimittelforschung. 2005;55(10):561–568. doi:10.1055/s-0031-1296905
36. Wurglics M, Schubert-Zsilavecz M. Hypericum perforatum: a ‘modern’herbal antidepressant: pharmacokinetics of active ingredients. Clin Pharmacokinet. 2006;45:449–468.
37. Caccia S, Gobbi M. St. John’s wort components and the brain: uptake, concentrations reached and the mechanisms underlying pharmacological effects. Curr Drug Metab. 2009;10(9):1055–1065. doi:10.2174/138920009790711878
38. Silva SM, Martinho A, Moreno I, et al. Effects of Hypericum perforatum extract and its main bioactive compounds on the cytotoxicity and expression of CYP1A2 and CYP2D6 in hepatic cells. Life Sci. 2016;144:30–36.
39. Mohagheghzadeh A, Badr P, Mohagheghzadeh A, Hemmati S. Hypericum perforatum L. and the underlying molecular mechanisms for its choleretic, cholagogue, and regenerative properties. Pharmaceuticals. 2023;16(6):887.
40. Cona MM, Feng Y, Verbruggen A, Oyen R, Ni Y. Improved clearance of radioiodinated hypericin as a targeted anticancer agent by using a duodenal drainage catheter in rats. Exp Biol Med. 2013;238(12):1437–1449.
41. Chrubasik-Hausmann S, Vlachojannis J, McLachlan AJ. Understanding drug interactions with St John’s wort (Hypericum perforatum L.): impact of hyperforin content. J Pharm Pharmacol. 2019;71(1):129–138. doi:10.1111/jphp.12858
42. Nobakht SZ, Akaberi M, Mohammadpour AH, Moghadam AT, Emami SA. Hypericum perforatum: traditional uses, clinical trials, and drug interactions. Iran J Basic Med Sci. 2022;25(9):1045.
43. Russo E, Scicchitano F, Whalley BJ, et al. Hypericum perforatum: pharmacokinetic, mechanism of action, tolerability, and clinical drug–drug interactions. Phytother Res. 2014;28(5):643–655. doi:10.1002/ptr.5050
44. Meruelo D, Lavie G, Lavie D. Therapeutic agents with dramatic antiretroviral activity and little toxicity at effective doses: aromatic polycyclic diones hypericin and pseudohypericin. Proc Natl Acad Sci. 1988;85(14):5230–5234. doi:10.1073/pnas.85.14.5230
45. Abma E, Peremans K, De Vos F, et al. Biodistribution and tolerance of intravenous iodine‐131‐labelled hypericin in healthy dogs. Vet Comp Oncol. 2018;16(3):318–323. doi:10.1111/vco.12381
46. Mannel M. Drug interactions with St John’s wort: mechanisms and clinical implications. Drug Saf. 2004;27:773–797. doi:10.2165/00002018-200427110-00003
47. Chan LY, Chiu P, Lau T. A study of hypericin-induced teratogenicity during organogenesis using a whole rat embryo culture model. Fertil Steril. 2001;76(5):1073–1074. doi:10.1016/S0015-0282(01)02730-3
48. Capasso R, Borrelli F, Montanaro V, et al. Effects of the antidepressant St. John’ s wort (Hypericum perforatum) on rat and human vas deferens contractility. J Urol. 2005;173(6):2194–2197. doi:10.1097/01.ju.0000158132.31157.01
49. Fox FE, Niu Z, Tobia A, Rook AH. Photoactivated hypericin is an anti-proliferative agent that induces a high rate of apoptotic death of normal, transformed, and malignant T lymphocytes: implications for the treatment of cutaneous lymphoproliferative and inflammatory disorders. J Invest Dermatol. 1998;111(2):327–332. doi:10.1046/j.1523-1747.1998.00278.x
50. Xie L, Jiang N, Liu Y, et al. Thermo-responsive hydrogel loading hypericin induces pro-inflammatory response against Trichinella spiralis infection via toll-like receptor 3 activation. Phytomedicine. 2025;136:156284. doi:10.1016/j.phymed.2024.156284
51. Larisch P, Verwanger T, Linecker M, Krammer B. The interrelation between a pro-inflammatory milieu and fluorescence diagnosis or photodynamic therapy of human skin cell lines. Photodiagnosis Photodyn Ther. 2014;11(2):91–103. doi:10.1016/j.pdpdt.2014.01.002
52. Krupka-Olek M, Bożek A, Czuba ZP, et al. Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures. Pharmaceutics. 2024;16(6):696. doi:10.3390/pharmaceutics16060696
53. Nowak-Perlak M, Woźniak M, Ziółkowski P. Hypericin-a natural photosensitizer in photodynamic therapy on skin cancer cells. Photodiagnosis Photodyn Ther. 2024;46:104170. doi:10.1016/j.pdpdt.2024.104170
54. Schmitt LA, Liu Y, Murphy PA, et al. Reduction in hypericin-induced phototoxicity by Hypericum perforatum extracts and pure compounds. J Photochem Photobiol B Biol. 2006;85(2):118–130. doi:10.1016/j.jphotobiol.2006.06.001
55. Zivari Ghader T, Shokouhi B, Kosari Nasab M, et al. Hypericum perforatum callus extract‐loaded composite hydrogel with diverse bioactivities for enhanced wound healing and fibrosis prevention. Small. 2024;20(52):2407112. doi:10.1002/smll.202407112
56. Hu X, Wu P, Zhao Y, et al. Enhancing the photodynamic efficacy of hypericin in antitumor treatment by inhibiting the cell integration stress response. Chem Eng J. 2025;505:159141. doi:10.1016/j.cej.2024.159141
57. Liang C, Liu X, Yu J, et al. Hypericin photoactivation induces triple-negative breast cancer cells pyroptosis by targeting the ROS/CALR/Caspase-3/GSDME pathway. J Adv Res. 2025;77:669–688. doi:10.1016/j.jare.2025.01.042
58. Galanou MC, Theodossiou TA, Tsiourvas D, Sideratou Z, Paleos CM. Interactive transport, subcellular relocation and enhanced phototoxicity of hypericin encapsulated in guanidinylated liposomes via molecular recognition. Photochem Photobiol. 2008;84(5):1073–1083. doi:10.1111/j.1751-1097.2008.00392.x
59. Zhang Q, Li Z, Li Y, et al. Hypericin-photodynamic therapy induces human umbilical vein endothelial cell apoptosis. Sci Rep. 2015;5(1):18398. doi:10.1038/srep18398
60. Karioti A, Bilia AR. Hypericins as potential leads for new therapeutics. Int J Mol Sci. 2010;11(2):562–594. doi:10.3390/ijms11020562
61. Mansouri P, Mirafzal S, Najafizadeh P, et al. The impact of topical Saint John’s Wort (Hypericum perforatum) treatment on tissue tumor necrosis factor-alpha levels in plaque-type psoriasis: a pilot study. J Postgrad Med. 2017;63(4):215–220. doi:10.4103/0022-3859.201423
62. Najafizadeh P, Hashemian F, Mansouri P, et al. The evaluation of the clinical effect of topical St Johns wort (Hypericum perforatum L.) in plaque type psoriasis vulgaris: a pilot study. Australas J Dermatol. 2012;53(2):131–135. doi:10.1111/j.1440-0960.2012.00877.x
63. Garg T, Rath G, Goyal A. Ancient and advanced approaches for the treatment of an inflammatory autoimmune disease− psoriasis. Crit Rev Ther Drug Carrier Syst. 2014;31(4):331–364. doi:10.1615/CritRevTherDrugCarrierSyst.2014010122
64. Almutawa F, Thalib L, Hekman D, et al. Efficacy of localized phototherapy and photodynamic therapy for psoriasis: a systematic review and meta‐analysis. Photodermatol Photoimmunol Photomed. 2015;31(1):5–14. doi:10.1111/phpp.12092
65. Abd-El-Azim H, Tekko IA, Ali A, et al. Hollow microneedle assisted intradermal delivery of hypericin lipid nanocapsules with light enabled photodynamic therapy against skin cancer. J Control Release. 2022;348:849–869. doi:10.1016/j.jconrel.2022.06.027
66. Kacerovská D, Pizinger K, Majer F, Šmíd F. Photodynamic therapy of nonmelanoma skin cancer with topical Hypericum perforatum extract—a pilot study. Photochem Photobiol. 2008;84(3):779–785. doi:10.1111/j.1751-1097.2007.00260.x
67. Alecu M, Ursaciuc C, Halalau F, et al. Photodynamic treatment of basal cell carcinoma and squamous cell carcinoma with hypericin. Anticancer Res. 1998;18(6B):4651–4654.
68. Kim EJ, Mangold AR, DeSimone JA, et al. Efficacy and safety of topical hypericin photodynamic therapy for early-stage cutaneous T-cell lymphoma (Mycosis fungoides): the FLASH Phase 3 randomized clinical trial. JAMA Dermatol. 2022;158(9):1031–1039. doi:10.1001/jamadermatol.2022.2749
69. Liu W, Wang H, Yeh Y, Wong T. An update on recent advances of photodynamic therapy for primary cutaneous lymphomas. Pharmaceutics. 2023;15(5):1328. doi:10.3390/pharmaceutics15051328
70. Nayak SB, Isik K, Marshall JR. Wound-healing potential of oil of hypercium perforatum in excision wounds of male sprague dawley rats. Adv Wound Care. 2017;6(12):401–406. doi:10.1089/wound.2017.0746
71. Chan BCL, Dharmaratne P, Wang B, et al. Hypericin and pheophorbide a mediated photodynamic therapy fighting MRSA wound infections: a translational study from in vitro to in vivo. Pharmaceutics. 2021;13(9):1399. doi:10.3390/pharmaceutics13091399
72. Waqar MA, Riaz T, Zaman M, et al. Origin, synthesis and various mechanisms of hypericin as antidepressant, photosensitizer and antiviral: hypericin as antidepressant, photosensitizer and antiviral. Pak J Health Sci. 2022:07–12. doi:10.54393/pjhs.v3i06.321
73. Zhou X, Chen Y, Cui L, Shi Y, Guo C. Advances in the pathogenesis of psoriasis: from keratinocyte perspective. Cell Death Dis. 2022;13(1):81. doi:10.1038/s41419-022-04523-3
74. Zhang S, Zhang J, Yu J, et al. Hyperforin ameliorates imiquimod-induced psoriasis-like murine skin inflammation by modulating IL-17A–producing Γδ T cells. Front Immunol. 2021;12:635076. doi:10.3389/fimmu.2021.635076
75. Haag SF, Tscherch K, Arndt S, et al. Enhancement of skin radical scavenging activity and stratum corneum lipids after the application of a hyperforin-rich cream. Eur J Pharm Biopharm. 2014;86(2):227–233. doi:10.1016/j.ejpb.2013.06.016
76. Mazur A, Koziorowska K, Dynarowicz K, Aebisher D, Bartusik-Aebisher D. Use of Hypericin in Clinical Trials of Photodynamic Therapy. 2024.
77. Su L, Zhu Y, Li X, et al. Topical adhesive spatio-temporal nanosystem co-delivering chlorin e6 and HMGB1 inhibitor glycyrrhizic acid for in situ psoriasis chemo-phototherapy. Acta Pharm Sin B. 2025;15:1126–1142. doi:10.1016/j.apsb.2024.12.020
78. Gallardo-Villagrán M. New anti-inflammatory and pro-apoptotic photosensitizers against arthritis and synovial sarcoma. 2022.
79. Khan NH, Mir M, Qian L, et al. Skin cancer biology and barriers to treatment: recent applications of polymeric micro/nanostructures. J Adv Res. 2022;36:223–247. doi:10.1016/j.jare.2021.06.014
80. Edwards SJ, Mavranezouli I, Osei-Assibey G, et al. VivaScope® 1500 and 3000 systems for detecting and monitoring skin lesions: a systematic review and economic evaluation. Health Technol Assess. 2016;20(58):1–260. doi:10.3310/hta20940
81. Theodossiou TA, Hothersall JS, De Witte PA, Pantos A, Agostinis P. The multifaceted photocytotoxic profile of hypericin. Mol Pharm. 2009;6(6):1775–1789. doi:10.1021/mp900166q
82. Peng Q, Moan J, Nesland JM. Correlation of subcellular and intratumoral photosensitizer localization with ultrastructural features after photodynamic therapy. Ultrastruct Pathol. 1996;20(2):109–129. doi:10.3109/01913129609016306
83. Wang K, Yu B, Pathak JL. An update in clinical utilization of photodynamic therapy for lung cancer. J Cancer. 2021;12(4):1154. doi:10.7150/jca.51537
84. de Morais FAP, De Oliveira ACV, Balbinot RB, et al. Multifunctional nanoparticles as high-efficient targeted hypericin system for theranostic melanoma. Polymers. 2022;15(1):179. doi:10.3390/polym15010179
85. Pulitzer M. Cutaneous T-cell lymphoma. Clin Lab Med. 2017;37(3):527–546. doi:10.1016/j.cll.2017.06.006
86. Beltraminelli H. Cutaneous T‐cell lymphoma—Focus on some problems, and some solutions. Hematol Oncol. 2023;41:20–24. doi:10.1002/hon.3147
87. Alexander Savino CV, Rumage A, Pullion C, et al. Compatibility study of topical 0.25% hypericin (HyBryteTM) application in subjects with mycosis fungoides: results of the HPN‐CTCL‐02 study. JEADV Clin Pract. 2024;3(4):1109–1118. doi:10.1002/jvc2.442
88. HyBryte™ Cutaneous T-Cell Lymphoma Treatment (CTCL) - Soligenix. 2025.
89. Guégan S, Lanternier F, Rouzaud C, Dupin N, Lortholary O. Fungal skin and soft tissue infections. Curr Opin Infect Dis. 2016;29(2):124–130. doi:10.1097/QCO.0000000000000252
90. Weitzman I, Summerbell RC. The dermatophytes. Clin Microbiol Rev. 1995;8(2):240–259. doi:10.1128/CMR.8.2.240
91. Yow CM, Tang HM, Chu ES, Huang Z. Hypericin‐mediated photodynamic antimicrobial effect on clinically isolated pathogens. Photochem Photobiol. 2012;88(3):626–632. doi:10.1111/j.1751-1097.2012.01085.x
92. Lazzara S, Carrubba A, Napoli E. Variability of hypericins and hyperforin in Hypericum species from the Sicilian flora. Chem Biodivers. 2020;17(1):e1900596. doi:10.1002/cbdv.201900596
93. Silva AR, Taofiq O, Ferreira IC, Barros L. Hypericum genus cosmeceutical application–A decade comprehensive review on its multifunctional biological properties. Ind Crops Prod. 2021;159:113053. doi:10.1016/j.indcrop.2020.113053
94. Montoya A, Daza A, Muñoz D, et al. Development of a novel formulation with hypericin to treat cutaneous leishmaniasis based on photodynamic therapy in in vitro and in vivo studies. Antimicrob Agents Chemother. 2015;59(9):5804–5813. doi:10.1128/AAC.00545-15
95. Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res. 2009;37(5):1528–1542. doi:10.1177/147323000903700531
96. Sorg H, Tilkorn DJ, Hager S, Hauser J, Mirastschijski U. Skin wound healing: an update on the current knowledge and concepts. Eur Surg Res. 2017;58(1–2):81–94. doi:10.1159/000454919
97. Süntar IP, Akkol EK, Yılmazer D, et al. Investigations on the in vivo wound healing potential of Hypericum perforatum L. J Ethnopharmacol. 2010;127(2):468–477. doi:10.1016/j.jep.2009.10.011
98. Sayar H, Gergerlioglu N, Seringec N, et al. Comparison of efficacy of topical phenytoin with hypericin in second-degree burn wound healing: an experimental study in rats. Med Sci Monit Basic Res. 2014;20:36. doi:10.12659/MSMBR.890337
99. Mahendrakumar M, Seeni S, Perinbam K. Hypericin, an anthraquinone derivative of Hypericum hookerianum wight and Arn.(Hypericaceae) of Palni Hills, South India, exhibits anti-inflammatory property in lipopolysaccharide—stimulated raw 264.7 macrophages. Pharmacogn Mag. 2018;14(56).
100. Quave CL. Wound healing with botanicals: a review and future perspectives. Curr Dermatol Rep. 2018;7:287–295. doi:10.1007/s13671-018-0247-4
101. Choudhary N, Collignon TE, Tewari D, Bishayee A. Hypericin and its anticancer effects: from mechanism of action to potential therapeutic application. Phytomedicine. 2022;105:154356. doi:10.1016/j.phymed.2022.154356
102. Wigginton KR, Boehm AB. Environmental engineers and scientists have important roles to play in stemming outbreaks and pandemics caused by enveloped viruses. 2020.
103. Connolly SA, Jardetzky TS, Longnecker R. The structural basis of herpesvirus entry. Nat Rev Microbiol. 2021;19(2):110–121. doi:10.1038/s41579-020-00448-w
104. Darlix J, de Rocquigny H, Mély Y. The multiple roles of the nucleocapsid in retroviral RNA conversion into proviral DNA by reverse transcriptase. Biochem Soc Trans. 2016;44(5):1427–1440. doi:10.1042/BST20160101-T
105. Miskovsky P. Hypericin-a new antiviral and antitumor photosensitizer: mechanism of action and interaction with biological macromolecules. Curr Drug Targets. 2002;3(1):55–84. doi:10.2174/1389450023348091
106. Cao K, Zhang Y, Yao Q, et al. Hypericin blocks the function of HSV-1 alkaline nuclease and suppresses viral replication. J Ethnopharmacol. 2022;296:115524. doi:10.1016/j.jep.2022.115524
107. Mohamed FF, Anhlan D, Schöfbänker M, et al. Hypericum perforatum and its ingredients hypericin and pseudohypericin demonstrate an antiviral activity against SARS-CoV-2. Pharmaceuticals. 2022;15(5):530. doi:10.3390/ph15050530
108. Chen H, Feng R, Muhammad I, et al. Protective effects of hypericin against infectious bronchitis virus induced apoptosis and reactive oxygen species in chicken embryo kidney cells. Poultr Sci. 2019;98(12):6367–6377. doi:10.3382/ps/pez465
109. Miškovský P, Jancura D, Sánchez-Cortés S, Kocišová E, Chinsky L. Antiretrovirally active drug hypericin binds the IIA subdomain of human serum albumin: resonance Raman and surface-enhanced Raman spectroscopy study. J Am Chem Soc. 1998;120(25):6374–6379. doi:10.1021/ja974233a
110. Bezakova L, Pšenák M, Kartnig T. Effect of dianthrones and their precursors from Hypericum perforatum L. on lipoxygenase activity. 1999.
111. Percifield RJ, Hawkins JS, McCoy J, Widrlechner MP, Wendel JF. Genetic diversity in Hypericum and AFLP Markers for species-specific identification of H. perforatum L. Planta Med. 2007;73(15):1614–1621. doi:10.1055/s-2007-993749
112. Li YH, Wang FS. Comparison of hypericin contents in Hypericum hubeiense and Hypericum perforatum. 2010.
113. Thomas C, MacGill RS, Miller GC, Pardini RS. Photoactivation of hypericin generates singlet oxygen in mitochondria and inhibits succinoxidase. Photochem Photobiol. 1992;55(1):47–53. doi:10.1111/j.1751-1097.1992.tb04208.x
114. Liang C, Hao F, Yao X, et al. Hypericin maintians PDX1 expression via the Erk pathway and protects islet β-cells against glucotoxicity and lipotoxicity. Int J Biol Sci. 2019;15(7):1472. doi:10.7150/ijbs.33817
115. Hadjur C, Richard MJ, Parat MO, Jardon P, Favier A. Photodynamic effects of hypericin on lipid peroxidation and antioxidant status in melanoma cells. Photochem Photobiol. 1996;64(2):375–381. doi:10.1111/j.1751-1097.1996.tb02474.x
116. Wang X, Wang L, Fekrazad R, et al. Polyphenolic natural products as photosensitizers for antimicrobial photodynamic therapy: recent advances and future prospects. Front Immunol. 2023;14:1275859. doi:10.3389/fimmu.2023.1275859
117. Kitanov GM. Hypericin and pseudohypericin in some Hypericum species. Biochem Syst Ecol. 2001;29(2):171–178. doi:10.1016/S0305-1978(00)00032-6
118. Chen B, Xu Y, Roskams T, et al. Efficacy of antitumoral photodynamic therapy with hypericin: relationship between biodistribution and photodynamic effects in the RIF‐1 mouse tumor model. Int J Cancer. 2001;93(2):275–282. doi:10.1002/ijc.1324
119. Agostinis P, Vantieghem A, Merlevede W, de Witte PA. Hypericin in cancer treatment: more light on the way. Int J Biochem Cell Biol. 2002;34(3):221–241. doi:10.1016/S1357-2725(01)00126-1
120. Gutman I, Marković Z, Solujić S, Sukdolak S. Zur Tautomerie von Hypericin. Monatshefte Für Chemie. 1998;129:481–486.
121. Barliya T, Mandel M, Livnat T, Weinberger D, Lavie G. Degradation of HIF-1alpha under hypoxia combined with induction of Hsp90 polyubiquitination in cancer cells by hypericin: a unique cancer therapy. PLoS One. 2011;6(9):e22849. doi:10.1371/journal.pone.0022849
122. Dror N, Mandel M, Lavie G. Unique anti-glioblastoma activities of hypericin are at the crossroad of biochemical and epigenetic events and culminate in tumor cell differentiation. PLoS One. 2013;8(9):e73625. doi:10.1371/journal.pone.0073625
123. Olya M, Arani HZ, Shekarriz A, et al. Hypericin exerts detrimental effect on Huh-7 as a delegacy of hepatocellular carcinoma: a P53 dependent pathway. Galen Med J. 2020;9:e1896. doi:10.31661/gmj.v9i0.1896
124. Hassin O, Oren M. Drugging p53 in cancer: one protein, many targets. Nat Rev Drug Discov. 2023;22(2):127–144. doi:10.1038/s41573-022-00571-8
125. Goel S, Bergholz JS, Zhao JJ. Targeting CDK4 and CDK6 in cancer. Nat Rev Cancer. 2022;22(6):356–372. doi:10.1038/s41568-022-00456-3
126. Hafezi S, Rahmani M. Targeting BCL-2 in cancer: advances, challenges, and perspectives. Cancers. 2021;13(6):1292. doi:10.3390/cancers13061292
127. Lenard J, Rabson A, Vanderoef R. Photodynamic inactivation of infectivity of human immunodeficiency virus and other enveloped viruses using hypericin and rose bengal: inhibition of fusion and syncytia formation. Proc Natl Acad Sci. 1993;90(1):158–162. doi:10.1073/pnas.90.1.158
128. Lavie G, Mazur Y, Lavie D, et al. Hypericin as an inactivator of infectious viruses in blood components. Transfusion. 1995;35(5):392–400. doi:10.1046/j.1537-2995.1995.35595259149.x
129. Zhang Y, Chen H, Zou M, et al. Hypericin inhibit alpha-coronavirus replication by targeting 3CL protease. Viruses. 2021;13(9):1825. doi:10.3390/v13091825
130. Jendželovská Z, Jendželovský R, Kuchárová B, Fedoročko P. Hypericin in the light and in the dark: two sides of the same coin. Front Plant Sci. 2016;7:560. doi:10.3389/fpls.2016.00560
131. Huang S. Comprehensive dermatologic drug therapy. Skinmed. 2022;20(3):240.
132. Holliday AC, Moody MN, Berlingeri-Ramos A. Methotrexate: role of treatment in skin disease. Skin Ther Lett. 2013;18(3):4–9.
133. Sehgal VN, Srivastava G, Dogra S. Tacrolimus in dermatology—pharmacokinetics, mechanism of action, drug interactions, dosages, and side effects: part I. SKINmed. 2008;7(1):27–30. doi:10.1111/j.1540-9740.2007.06485.x
134. Solimani F, Meier K, Ghoreschi K. Emerging topical and systemic JAK inhibitors in dermatology. Front Immunol. 2019;10:2847. doi:10.3389/fimmu.2019.02847
135. Kumar B, Aggarwal R, Prakash U, Sahoo PK. Emerging therapeutic potential of curcumin in the management of dermatological diseases: an extensive review of drug and pharmacological activities. Futur J Pharm Sci. 2023;9(1):42. doi:10.1186/s43094-023-00493-1
136. Pardo Andreu GL, Delgado R, Núñez Sellés AJ, Vercesi AE. Mangifera indica L. extract (Vimang®) inhibits 2‐deoxyribose damage induced by Fe (III) plus ascorbate. Phytother Res. 2006;20(2):120–124. doi:10.1002/ptr.1813
137. Lee EH, Faulhaber D, Hanson KM, et al. Dietary lutein reduces ultraviolet radiation-induced inflammation and immunosuppression. J Invest Dermatol. 2004;122(2):510–517. doi:10.1046/j.0022-202X.2004.22227.x
138. Verfaillie T, van Vliet A, Garg AD, et al. Pro-apoptotic signaling induced by photo-oxidative ER stress is amplified by Noxa, not Bim. Biochem Biophys Res Commun. 2013;438(3):500–506. doi:10.1016/j.bbrc.2013.07.107
139. Dong X, Zeng Y, Zhang Z, et al. Hypericin-mediated photodynamic therapy for the treatment of cancer: a review. J Pharm Pharmacol. 2021;73(4):425–436. doi:10.1093/jpp/rgaa018
140. Xu L, Zhang X, Cheng W, et al. Hypericin-photodynamic therapy inhibits the growth of adult T-cell leukemia cells through induction of apoptosis and suppression of viral transcription. Retrovirology. 2019;16:1–13. doi:10.1186/s12977-019-0467-0
141. Fürst R, Zündorf I. Plant‐derived anti‐inflammatory compounds: hopes and disappointments regarding the translation of preclinical knowledge into clinical progress. Mediators Inflamm. 2014;2014(1):146832. doi:10.1155/2014/146832
142. Jantan I, Ahmad W, Bukhari SNA. Plant-derived immunomodulators: an insight on their preclinical evaluation and clinical trials. Front Plant Sci. 2015;6:655. doi:10.3389/fpls.2015.00655
143. Di Sotto A, Gullì M, Percaccio E, et al. Efficacy and safety of oral green tea preparations in skin ailments: a systematic review of clinical studies. Nutrients. 2022;14(15):3149. doi:10.3390/nu14153149
144. Denke A, Schneider W, Elstner EF. Biochemical activities of extracts from Hypericum perforatum L. 2nd Communication: inhibition of metenkephaline-and tyrosine-dimerization. Arzneimittelforschung. 1999;49(02):109–114. doi:10.1055/s-0031-1300369
145. Scontre VA, Martins JC, de Melo Sette CV, et al. Curcuma longa (turmeric) for prevention of capecitabine-induced hand-foot syndrome: a pilot study. J Diet Suppl. 2018;15(5):606–612. doi:10.1080/19390211.2017.1366387
146. Mo Z, Yuan J, Guan X, Peng J. Advancements in dermatological applications of curcumin: clinical efficacy and mechanistic insights in the management of skin disorders. Clin Cosmet Invest Dermatol. 2024;17:1083–1092. doi:10.2147/CCID.S467442
147. Basu P, Dutta S, Begum R, et al. Clearance of cervical human papillomavirus infection by topical application of curcumin and curcumin containing polyherbal cream: a phase II randomized controlled study. Asian Pac J Cancer Prev. 2013;14(10):5753–5759. doi:10.7314/APJCP.2013.14.10.5753
148. Song Y, Zhang J, Zhu L, et al. Recent advances in nanodelivery systems of resveratrol and their biomedical and food applications: a review. Food Funct. 2024;15:8629–8643. doi:10.1039/D3FO03892K
149. Jürgenliemk G, Nahrstedt A. Dissolution, solubility and cooperativity of phenolic compounds from Hypericum perforatum L. in aqueous systems. Die Pharmazie. 2003;58(3):200–203.
150. Zhang J, Gao L, Hu J, et al. Hypericin: source, determination, separation, and properties. Sep Purif Rev. 2022;51(1):1–10.
151. Kiss N, Farkas K, Tosti G, et al. Photodynamic therapy with 5-aminolevulinic acid patch for the treatment of actinic keratosis. J Clin Med. 2022;11(11):3164. doi:10.3390/jcm11113164
152. Korzeniowska K, Malesza K, Pawlaczyk M. The phototoxic properties of Hypericum perforatum—Case report and review of the literature. Farm Wspólczesna. 2019;12:107–112.
153. Zhang J, Zhou X, Fu M. Integrated utilization of red radish seeds for the efficient production of seed oil and sulforaphene. Food Chem. 2016;192:541–547. doi:10.1016/j.foodchem.2015.07.051
154. Qiu C, Zhang JZ, Wu B, et al. Advanced application of nanotechnology in active constituents of Traditional Chinese Medicines. J Nanobiotechnology. 2023;21(1):456.
155. Li Y, Shen Q, Feng L, et al. A nanoscale natural drug delivery system for targeted drug delivery against ovarian cancer: action mechanism, application enlightenment and future potential. Front Immunol. 2024;15:1427573.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.