Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Hydroxychloroquine and risk of development of cancers: a nationwide population-based cohort study
Authors Mao IC ![]() , Lin CY
, Lin CY ![]() , Wu CL
, Wu CL ![]() , Kor CT
, Kor CT ![]() , Chang CC
, Chang CC ![]()
Received 28 May 2018
Accepted for publication 27 June 2018
Published 20 August 2018 Volume 2018:14 Pages 1435—1443
DOI https://doi.org/10.2147/TCRM.S175581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
I-Chieh Mao,1 Ching-Yeh Lin,2 Chia-Lin Wu,3,4 Chew-Teng Kor,5,6 Chia-Chu Chang3,7–9
1Division of Critical Care, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan; 2Division of Hematology and Oncology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan; 3Division of Nephrology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan; 4Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan; 5Internal Medicine Research Center, Changhua Christian Hospital, Changhua, Taiwan; 6Graduate Institute of Statistics and Information Science, National Changhua University of Education, Changhua, Taiwan; 7Department of Internal Medicine, Kuang Tien General Hospital, Taichung, Taiwan; 8School of Medicine, Chung-Shan Medical University, Taichung, Taiwan; 9Department of Nutrition, Hungkuang University, Taichung, Taiwan
Background: Hydroxychloroquine (HCQ), one of the disease-modifying antirheumatic drugs, may lead to an inhibition of autophagy. Autophagy, an intracellular self-defense mechanism for the lysosomal degradation of cytoplasmic components such as damaged organelles, plays a role in protecting against neoplasm growth but is also vital for cancer cells due to an increased intracellular metabolic waste.
Methods: Taiwan National Health Insurance Database was subjected to analysis to investigate the effect of HCQ exposure on cancer risk in patients with autoimmune diseases. Cancer incidence between patients with or without at least 12-month HCQ use was compared by propensity score-matched landmark analysis. A total of 100,000 participants were enrolled, including 7,662 patients who were diagnosed with autoimmune diseases between January 1, 2000, and December 31, 2012.
Results: After propensity score matching, HCQ user and nonuser groups consist of 1,933 patients with a mean follow-up time of 7.82 and 6.7 years, respectively. During the follow-up period, 93 HCQ users and 77 HCQ nonusers developed cancers. Meanwhile, Kaplan–Meier estimates showed no difference in the overall incidence of cancer between HCQ users and nonusers.
Conclusion: This propensity score-matched study of Taiwanese patients with autoimmune diseases suggested that HCQ exposure did not increase the cancer risk.
Keywords: hydroxychloroquine, autophagy, cancer, autoimmune diseases, propensity score
Introduction
Hydroxychloroquine (HCQ) is a 4-aminoquinoline agent that has been used for >50 years to prevent or to treat malarial infections and later also to treat autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis.1 Recently, HCQ has been demonstrated to have anticancer effects by inhibiting autophagy pathway in some cancer types, such as breast cancer,2 glioblastoma, lung cancer, multiple myeloma, pancreatic cancer, melanoma, hepatocellular carcinoma, and bladder cancer.1,3–5
Autophagy is an evolutionarily conserved, intracellular self-defense mechanism for the lysosomal degradation of cytoplasmic components.6 Damaged organelles and protein aggregates are sequestered into autophagic vesicles (also known as autophagosomes) that are subsequently degraded through fusion with lysosomes, which makes autophagy critical for the cellular remodeling7 and maintenance of intracellular homeostasis.8 In some stress conditions, such as infection, apoptosis, and cancer behaviors, autophagy is additionally upregulated to response difficult environmental disturbance.5 Therefore, autophagy plays an essential role in cell development, differentiation, normal growth, and immunity. In line with this notion, defected autophagy has been shown to involve in some clinical disorders, including infectious,9 neurodegenerative,10 and neoplastic11 diseases.
Interestingly, the effect of autophagy is a double-edged sword12 for cancer cells. As a tumor suppressor, autophagy prevents the accumulation of damaged proteins and organelles.6 As a tumor promotor, autophagy facilitates tumor growth and aggressiveness by surviving microenvironmental stress.6 Cancer cells rely and are even more dependent on autophagy due to increased metabolic and biosynthetic demands imposed by deregulated proliferation.13
No doubt, autoimmune diseases, representing chronic inflammation status, have a clear association with cancer.14 Whether administration of HCQ, which leads to the inhibition of autophagy in patients with autoimmune diseases, increases the risk of cancer development is not clearly described. It is important to eliminate this doubt to ensure the safety of HCQ use in such high-risk population. Our study aimed to clarify whether HCQ use is associated with increased risk of cancers. In this retrospective study involving a large-scale nationwide cohort, we evaluated the effect of HCQ exposure on the development of cancers in patients with autoimmune diseases.
Methods
Data source
Data were retrieved from the Taiwan’s National Health Insurance Research Database (NHIRD), which includes all claims data from the National Health Insurance program.15 These claims include demographic data, ambulatory care, record of clinic visits, hospital admissions, dental services, prescriptions, and disease status. The National Health Insurance program, which was started in Taiwan in March 1995, covers >99% of the total population or ~23 million people. Researchers can apply for specific dataset such as cancer or catastrophic illness dataset and longitudinal dataset containing a random sample of 1 million NHI enrollees. Diagnostic codes for identifying diseases were based on ICD, Ninth Revision, Clinical Modification (ICD-9-CM). The drug prescriptions were managed according to Anatomical Therapeutic Chemical (ATC) codes defined by World Health Organization (WHO). Defined daily dose (DDD) was used to measure the medication consumption, and it is 516 mg for HCQ defined by WHO. Because anonymized and encrypted secondary data were analyzed, informed consent was exempt in this study. Ethics approval was obtained from the Institutional Review Board of the Changhua Christian Hospital (approval number 180604).
Study population
Patients with autoimmune diseases were identified by using ICD-9-CM code 710.2 for Sjögren’s syndrome, 696.0–696.1 for psoriasis, 714.0 for rheumatoid arthritis, 700 for systemic lupus erythematosus, 710.1 for scleroderma, and 710.4 for polymyositis. Cancer events were identified from the Registry of Catastrophic Illness Patient Database, which is a subset of the NHIRD, by excluding patients with the history of cancer before the index date, aged <18 years, and survived or being followed for <1 year. If the patients are diagnosed with a new cancer within 1 year, we assumed that the cancer may precede than the autoimmune diseases and may not be related to the use of HCQ. Exposure to HCQ (HCQ user) was defined as a pharmacological treatment of HCQ given within 12 months after the diagnosis of systemic autoimmune diseases. The index date on which the 12 months after diagnosis was defined as the index date to ensure that each patient had enough observation window for HCQ exposure. In addition, the index date was set-up at 366 days following the diagnosis of autoimmune diseases to avoid immortal time bias. The aim of this propensity score-matched study is to investigate the effect of HCQ on cancer incidence. Propensity score was calculated by logistic regression models to indicate the conditional probability of receiving HCQ and then adjusted by age, gender, autoimmune diseases, socioeconomic factors, medications, and comorbidities. Eventually, HCQ-exposed patients and nonexposed patients were matched at a ratio of 1–1.
Outcome measures and relevant variables
The catastrophic illness registry was used to identify cancer cases (ICD-9-CM codes 140–208). Major comorbid diseases diagnosed before the index date were defined as baseline comorbidities based on claims data. These comorbidities included hypertension, diabetes mellitus (DM), hyperlipidemia, coronary artery disease (CAD), congestive heart failure (CHF), stroke, chronic obstructive pulmonary disease (COPD), and alcohol-related diseases (alcoholism, alcoholic liver disease, and alcoholic gastritis). Charlson’s comorbidity index score was used to quantify baseline comorbidities.16
Statistical analysis
Demographic and clinical characteristics in the HCQ user and HCQ nonuser cohorts were summarized using proportions and mean ± SD. Chi square tests and Student’s t-tests were used to compare the distributions of discrete and continuous variables, respectively. Cox’s proportional hazard models were used to estimate the relative risk of developing cancers in the HCQ user cohort compared with that in the HCQ nonuser cohort. Confounders, including age, gender, type of autoimmune diseases, and propensity score, were adjusted in multivariate Cox’s analysis with competing risks (Fine–Gray subdistribution hazards models) of death to estimate adjusted hazard ratios (aHRs). To determine the dose–response relation, we estimated the risk of cancer according to the cumulative DDD (cDDD) during the 1-year exposure period (DDD 1–142 or >142 mg) and the prescribed daily dose (≤200, 201–400, or >400 mg) compared with HCQ nonuser. Cumulative incidence of cancers was calculated using the Kaplan–Meier estimation and compared using Log-rank tests. To assess the reliability of our results, five sensitivity analyses were performed to ascertain our results. First of all, clinical variables (demographics, comorbidities, and long-term medications) were adjusted in multivariable Cox proportional hazard model. Second, we evaluated misclassification bias by defining HCQ use at intervals 90, 150, and 180 days after the initial diagnosis of autoimmune diseases. Third, an as-treat model for patients who discontinued HCQ use was censored. Fourth, we evaluated the patients who were followed up for >7 and 10 years due to the evolutionary time to tumor. Fifth, we removed patients with other immunosuppressants in order to minimize potential effects on unbalanced covariate after propensity score matched. All statistical analyses were performed using the SAS 9.4 software (SAS Institute Inc., Cary, NC, USA). Two-tailed P-values <0.05 were considered statistically significant.
Results
Through the subject selection process shown in Figure 1, a total of 100,000 participants were enrolled to include 7,662 patients diagnosed with autoimmune diseases between January 1, 2000, and December 31, 2013. During this process, 1,112 patients were excluded and 6,541 patients were eligible for subsequent analysis, including 3,408 HCQ users and 3,133 HCQ nonusers. After propensity score matching, 1,993 subjects were assigned to each group. Variables included in the propensity score calculation did not significantly differ between HCQ user and nonuser after matching, which confirms the success of matching (Table 1).
 | Figure 1 Flow chart for subject selection process. |
 | Table 1 Demographics and clinical characteristics of the study population |
Table 1 shows the baseline characteristics of study population to reveal a similar age distribution in both cohorts, with a mean age of 50.95±13.66 and 50.96±13.69 years in HCQ user and nonuser groups, respectively. With female (84.35%) accounting for the majority, all patients were diagnosed with autoimmune diseases, including rheumatoid arthritis (55.09%), Sjögren’s syndrome (36.13%), systemic lupus erythematosus (7.98%), scleroderma (0.4%), psoriasis (0.35%), and polymyositis (0.05%). Most of the population were from northern Taiwan without significant difference regarding monthly income. The comorbidities, including hypertension, hyperlipidemia, DM, COPD, and alcohol-related diseases, are similar between HCQ user and HCQ nonuser groups. However, HCQ users still have a significantly higher rate of taking other immunosuppressants, such as methotrexate, leflunomide, sulfasalazine, and azathioprine. The mean follow-up duration is 7.82 and 6.7 years, respectively, in HCQ nonuser and user groups.
Results in Figures 2–4 revealed the relationship between cancer risk and HCQ and dose–response of HCQ. Kaplan–Meier curve showed no significant different cumulative incidence of cancer between HCQ user and nonuser (Log rank test P-value =0.927) (Figure 2). The incidence of cancer was not significantly increased in the larger cumulative daily dose of HCQ group (Figure 3, P=0.958). In Figure 4, our results suggested that prescribed daily dose did not affect the incidence of cancer significantly. In extended Cox proportional hazards models (Table 2), confounding factors, including age, gender, type of autoimmune diseases, and propensity score, were adjusted and the aHRs of cancer were 1.027 (95% CI: 0.76–1.39) in the HCQ user group, 1.088 (95% CI: 0.68–1.75) in the group with prescribed daily dose ≤200 mg, 1.051 (95% CI: 0.71–1.57) in the group with prescribed daily dose 201–400 mg, and 0.986 (95% CI: 0.63–1.55) in the group with prescribed daily dose >400 mg. For cDDDs, the hazard ratio was 1.077 (95% CI: 0.77–1.50) in 1–142 cDDDs’ group and 0.933 (95% CI: 0.58–1.50) in >142 cDDDs’ group. Therefore, HCQ did not showed significant increase in cancer risk. Similar to that from primary analyses, results from the subgroup analysis (Table 3) demonstrated that there was no significant difference in the risk of cancer between HCQ user and nonuser across different ages, genders, comorbidities, and autoimmune diseases. Moreover, none of these subgroups significantly interacted with HCQ treatment (all interactions P>0.05). As shown in Table 4, there was no difference in risk for specific cancers between two cohorts, in both unadjusted and adjusted models.
 | Figure 2 Kaplan–Meier curves for cumulative incidence of cancer, HCQ nonuser and user. |
 | Figure 3 Kaplan–Meier curves for cumulative incidence of cancer with various cDDDs of HCQ. |
 | Figure 4 Kaplan–Meier curves for cumulative incidence of cancer with various prescribed daily dose of HCQ. |
 | Table 2 Incidences and hazard ratios of cancer in hydroxychloroquine users compared with nonusers |
 | Table 3 Results of subgroup analysis for cancer incidence of HCQ users and nonusers stratified by various confounders |
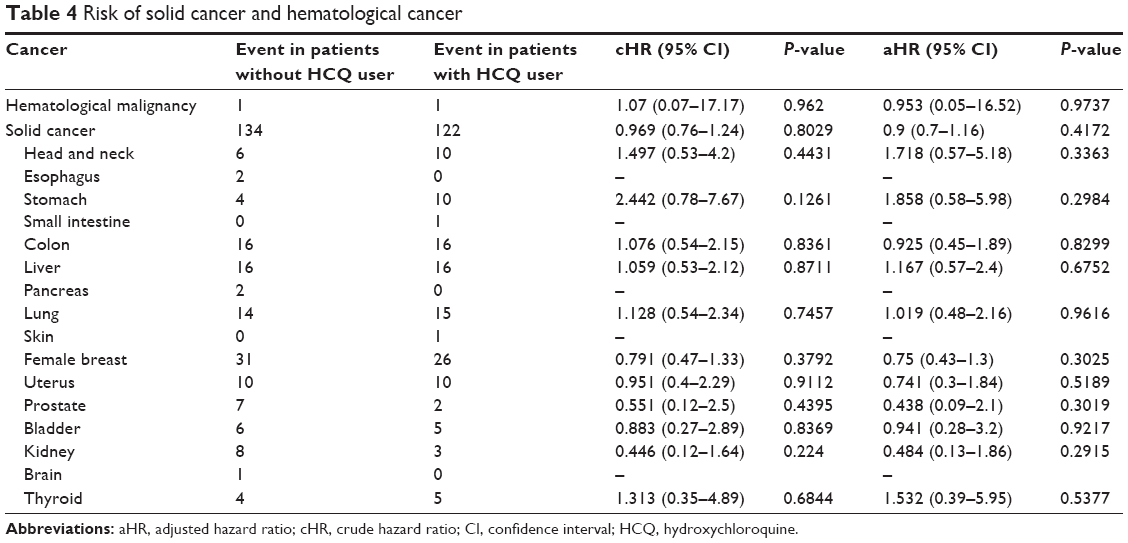 | Table 4 Risk of solid cancer and hematological cancer |
Regarding the reliability of our main results, results of five steps of sensitivity analyses shown in Table 5 have showed consistence with those of our primary analyses.
 | Table 5 Results of sensitivity analyses |
Discussion
This is the first population-based study to investigate the effects of HCQ on the incidence of malignancy in patients with autoimmune diseases. Our evidence suggests that HCQ use is not associated with an increased risk of cancers in patients with autoimmune diseases. After adjustment for cancer risk factors and covariates including age, gender, and autoimmune types, HCQ still does not increase the risk in patients with autoimmune diseases both in hematological and solid malignancies (Table 4).
Recently, the safety issue of long-term HCQ therapy mainly focuses on retinopathy.17 To our knowledge, little attention has been paid to the safety concern regarding the effect on cancer development of HCQ. On the contrary, growing data and researches are emerging on the anticancer effects of HCQ and HCQ is mostly often administered in combination with other anticancer agents. Multiple hypotheses have been proposed on how HCQ exerts their anticancer activities. The most popular hypothesis is that the antineoplastic activity of HCQ probably stems from the direct inhibition of autophagy pathway18 to augment the efficacy of anticancer agents.19 As a tumor suppressor, HCQ inhibits autophagy to suppress the growth of established tumors, which had been illuminated in cell and mice studies.20–22 In several preclinical studies, administration of HCQ can disable autophagy pathway through the inhibition of fusion of autophagosomes with lysosomes and their degradation.23 Up to date, there are >20 ongoing trials involving HCQ on human cancer treatment on ClinicalTrials.gov.
Our study used a real-world large nationwide population-based cohort to understand whether HCQ has any effect on the incidence of cancers. The results did not support that HCQ use has any effect on cancer risk, regardless of the cDDDs or prescribed daily doses. Therefore, HCQ can safely be used as a disease-modifying antirheumatic drug for autoimmune diseases without concerns of its autophagy inhibition ability that would potentially promote the risk of cancer development. It is worth noting that in our subgroup analysis, there is a trend of decreasing incidence of cancer in elderly patients after adjusting confounding factors. Therefore, it may need more investigation to clarify if HCQ has a protective benefit of cancer development in elderly patient with autoimmune diseases.
Some possible explanations may be taken into consideration for the interpretation of our observations. First of all, patients with autoimmune diseases are already at a higher risk of cancers than general population.24 Unregulated inflammation chronically provokes cellular malignant transformation and carcinogenesis in surrounding tissues. Compared to this strong trigger factor, the contribution of the carcinogenicity of HCQ may be neglected. Second, the usual dosage of HCQ used to treat autoimmune disease patients is often <400 mg daily while the dosage of HCQ to be antineoplastic or able to inhibit autophagy is required as high as up to 1,000 mg.25 HCQ at a lower dosage may only exert limited ability for inhibiting autophagy and eventually no apparent influence on cancer development.
The strength of this study was primarily based on the use of longitudinal population-based data, which represents the general population in Taiwan. However, this study has some potential limitations. First of all, the NHIRD does not include detailed information on socioeconomic status, smoking and betel nut chewing habits, dietary patterns, family history of cancers, and relevant biochemical parameters. Second, this study is not able to clearly elucidate the different effects of high (≥1,000 mg) and low dosages of HCQ on the incidence of cancers. In such higher HCQ dose, whether there is any influence on cancer incidence in autoimmune diseases’ patient remains to be investigated. Third, propensity was used to handle confounding by indication bias in our study. There may be residual confounders that have not been considered. Results derived from a retrospective cohort study are generally of lower statistical quality than those from prospective studies because of potential biases. Finally, as the majority of Taiwan’s population is of Chinese ethnicity, the findings of this study may not be applicable to populations of other ethnic backgrounds.
Conclusion
This propensity score matching population-based retrospective cohort study revealed that Taiwanese patients with autoimmune diseases showed that HCQ had a neutral effect on cancer risk but a nonsignificant protective effect in elderly patients. HCQ is a widely and chronically used medication in autoimmune diseases and poses a potential effect of dysregulated tumor growth by inhibiting autophagy. However, the occurrence of malignancies should not be a concern according to our results.
Disclosure
The authors report no conflicts of interest in this work.
References
Verbaanderd C, Maes H, Schaaf MB, et al. Repurposing drugs in oncology (ReDO) – chloroquine and hydroxychloroquine as anti-cancer agents. Ecancermedicalscience. 2017;11:1–35. | ||
Cook KL, Wärri A, Soto-Pantoja DR, et al. Hydroxychloroquine inhibits autophagy to potentiate antiestrogen responsiveness in ER+ breast cancer. Clin Cancer Res. 2014;20(12):3222–3232. | ||
Lin YC, Lin JF, Wen SI, et al. Chloroquine and hydroxychloroquine inhibit bladder cancer cell growth by targeting basal autophagy and enhancing apoptosis. Kaohsiung J Med Sci. 2017;33(5):215–223. | ||
Manic G, Obrist F, Kroemer G, Vitale I, Galluzzi L. Chloroquine and hydroxychloroquine for cancer therapy. Mol Cell Oncol. 2014;1(1):e29911. | ||
Amaravadi RK, Lippincott-Schwartz J, Yin XM, et al. Principles and current strategies for targeting autophagy for cancer treatment. Clin Cancer Res. 2011;17(4):654–666. | ||
Yang ZJ, Chee CE, Huang S, Sinicrope FA. The role of autophagy in cancer: therapeutic implications. Mol Cancer Ther. 2011;10(9):1533–1541. | ||
White E. The role for autophagy in cancer. J Clin Invest. 2015;125(1):42–46. | ||
Towers CG, Thorburn A. Therapeutic targeting of autophagy. EBioMedicine. 2016;14:15–23. | ||
Deretic V, Saitoh T, Akira S. Autophagy in infection, inflammation and immunity. Nat Rev Immunol. 2017;13(10):722–737. | ||
Nixon RA. The role of autophagy in neurodegenerative disease. Nat Med. 2013;19(8):983–997. | ||
Mathew R, Karantza-Wadsworth V, White E. Role of autophagy in cancer. Nat Rev Cancer. 2007;7(12):961–967. | ||
White E, Dipaola RS. The double-edged sword of autophagy modulation in cancer. Clin Cancer Res. 2009;15(17):5308–5316. | ||
Rabinowitz JD, White E. Autophagy and metabolism. Science. 2010;330(6009):1344–1348. | ||
Giat E, Ehrenfeld M, Shoenfeld Y. Cancer and autoimmune diseases. Autoimmun Rev. 2017;16(10):1049–1057. | ||
Bureau of National Health Insurance. National Health Insurance Annual Statistical Report, 2016–2017 (bilingual). Available from: https://www.nhi.gov.tw/Resource/webdata/13767_1_National%20Health%20Insurance%20in%20Taiwan%202016-2017(bilingual).pdf | ||
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Melles RB, Marmor MF. The risk of toxic retinopathy in patients on long-term hydroxychloroquine therapy. JAMA Ophthalmol. 2014;132(12):1453–1460. | ||
Shi TT, Yu XX, Yan LJ, Xiao HT. Research progress of hydroxychloroquine and autophagy inhibitors on cancer. Cancer Chemother Pharmacol. 2017;79(2):287–294. | ||
Fang Y, Chen Y, Chung T, et al. Hydroxychloroquine and risk of cancer in patients with primary Sjögren syndrome: propensity score matched landmark analysis. Oncotarget. 2017;8(46):80461–80471. | ||
Mathew R, Karp CM, Beaudoin B, et al. Autophagy suppresses tumorigenesis through elimination of p62. Cell. 2009;137(6):1062–1075. | ||
Komatsu M, Waguri S, Koike M, et al. Homeostatic levels of p62 control cytoplasmic inclusion body formation in autophagy-deficient mice. Cell. 2007;131(6):1149–1163. | ||
Komatsu M, Waguri S, Ueno T, et al. Impairment of starvation-induced and constitutive autophagy in Atg7-deficient mice. J Cell Biol. 2005;169(3):425–434. | ||
White E. Deconvoluting the context-dependent role for autophagy in cancer. Nat Rev Cancer. 2012;12(6):401–410. | ||
K-H Y, Kuo C-F, Huang LH, Huang W-K, See L-C. Cancer risk in patients with inflammatory systemic autoimmune rheumatic diseases. Medicine. 2016;95(18):e3540. | ||
Goldberg SB, Supko JG, Neal JW, et al. A phase I study of erlotinib and hydroxychloroquine in advanced non-small-cell lung cancer. J Thorac Oncol. 2012;7(10):1602–1608. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.