Back to Journals » International Journal of Women's Health » Volume 18
Human Papillomavirus-Induced Keratinizing Squamous Cell Carcinoma in Ovarian Cystic Teratoma: A Case Report and Literature Review
Authors Zhang H, Feng J, Guo Q, Liu J, Zhan P ![]()
Received 28 September 2025
Accepted for publication 30 December 2025
Published 8 January 2026 Volume 2026:18 570899
DOI https://doi.org/10.2147/IJWH.S570899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Hanrui Zhang,1 Jia Feng,2 Qian Guo,1 Jinbo Liu,2 Ping Zhan1
1Department of Gynecology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China; 2Department of Laboratory Medicine, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China
Correspondence: Ping Zhan, Email [email protected]
Abstract: Ovarian mature cystic teratoma (MCT), the most common ovarian tumor, undergoes malignant transformation only in a small proportion of cases, most frequently into squamous cell carcinoma. However, malignant transformation into squamous cell carcinoma associated with human papillomavirus (HPV) infection is exceptionally rare. Here, we reported a 43-year-old premenopausal woman who presented with an abdominal mass. CT examination suggested an ovarian MCT, and then the patient underwent surgical resection. Histopathological analysis confirmed a diagnosis of MCT-derived keratinizing squamous cell carcinoma, with HPV types 16 and 59 infections being detected through preoperative cervical cancer screening. According to the 2014 FIGO staging system, the patient was diagnosed as stage IC. The surgery was successful, and adjuvant chemotherapy with the BEP regimen was planned. Notably, malignant transformation of MCT is uncommon, and HPV-related squamous cell carcinoma arising from an ovarian teratoma is scarcely documented. This case highlights the importance of considering malignant transformation in clinical practice, particularly through early assessment based on patient age, tumor size, and tumor marker levels, to ensure timely diagnosis and intervention.
Keywords: mature cystic teratoma, malignant transformation, squamous cell carcinoma, human papillomavirus
Introduction
Ovarian mature cystic teratomas (MCTs) are widely known as germ cell-derived neoplasms capable of multilineage differentiation.1 Although generally benign, these tumors exhibit malignant transformation in approximately 1–2% of instances, most frequently into squamous cell carcinoma (SCC), which accounts for approximately 80% of all malignant transformations, then followed by adenocarcinoma.2 Usually, MCTs are readily identifiable by conventional imaging modalities such as ultrasonography, CT, or MRI. Nevertheless, the preoperative detection of malignant change still remains difficult due to the frequent absence of specific clinical indicators.
Regrettably, a significant proportion of cases are identified at an advanced disease stage, which is associated with less favorable outcomes compared to earlier detection. Definitive diagnosis relies on postoperative histopathological and immunohistochemical evaluation, without universally established treatment protocol. However, early-stage malignant transformation might be accompanied by clinically silent, mild abdominal pain, distension, and a palpable mass. According to aggregated case literature previously, the mean age at diagnosis for malignant transformation is approximately 51.3 years.3
Therefore, postmenopausal women diagnosed with teratomas warrant heightened vigilance for potential malignant transformation. The oncogenic role of high-risk human papillomavirus (HR-HPV), particularly genotypes 16 and 18, is well-established in the pathogenesis of squamous cell carcinomas at various anatomical sites.4 Recent evidence suggests that HPV may reach ovarian tissues through an ascending route via the reproductive tract, potentially acting upon the squamous epithelial components present in MCT ectodermal elements. Herein, we present a case documenting human papillomavirus infection-related ovarian MCT squamous cell carcinoma malignant transformation.
Literature Search Methodology
A comprehensive literature search was conducted using PubMed, Web of Science, Embase, and Google Scholar databases from inception to April 2025. The search terms included: (“mature cystic teratoma” OR “dermoid cyst” OR “ovarian teratoma”) AND (“squamous cell carcinoma” OR “malignant transformation”) AND (“human papillomavirus” OR “HPV”). Inclusion criteria were: (1) cases of squamous cell carcinoma arising from ovarian MCT with HPV detection; (2) English or Chinese language; (3) full-text availability. Exclusion criteria were: (1) reviews without original case data; (2) cases without HPV analysis; (3) duplicate publications. The initial search identified 156 articles; after screening and applying criteria, 12 relevant cases were included in this review.
Case Presentation
In May 2025, a 43-year-old premenopausal woman was evaluated in gynecology for a 15-day history of hypogastric pain. Her review of systems was unremarkable for vaginal bleeding, gastrointestinal or urinary symptoms, anorexia, or weight loss. Pelvic examination revealed cervical atrophy and a large, well-defined but relatively fixed pelvic mass, which was tender with rebound tenderness on palpation.
The levels of serum tumor marker were briefly described as below: CA125 36.1 U/mL (normal range <35.0), CEA 21.78 ng/mL (normal range 0–6), SCCA 66.9 ng/mL (normal range 0–2.5), CA199 969 IU/mL (normal range 0–28). Abdominal ultrasound revealed a heterogeneous mass measuring 17.5×24×11 cm with multiple cystic components in the pelvic cavity (Figure 1A). Abdominal and pelvic contrast-enhanced CT confirmed a 17×8 cm mass showing contrast uptake and ascites, along with multiple round intraperitoneal fatty density lesions (Figure 1B).
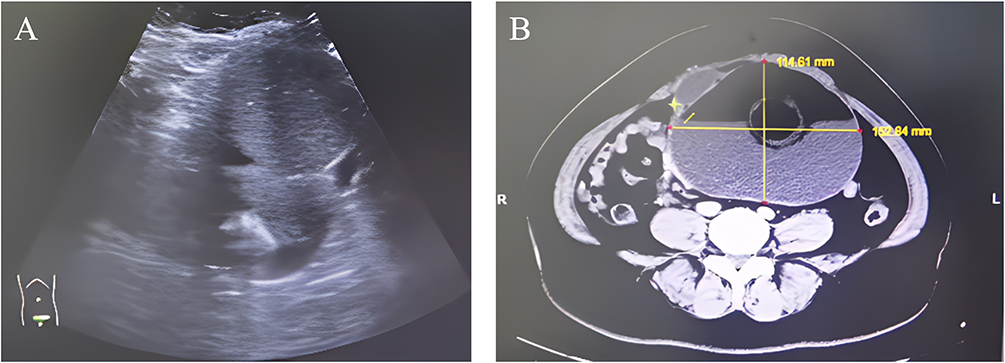 |
Figure 1 Imaging examination results. (A) Transvaginal ultrasound examination: abdominopelvic heterogeneous mass measuring 17.5×24×11 cm with multiple cystic components; (B) Enhanced abdominal CT examination: irregular low-density pelvic lesion with visible fat-fluid levels and contrast enhancement. |
Preoperative cervical cancer screening showed HPV 16 and 59 positive, TCT revealed HSIL, and cervical biopsy showed CIN III. The patient first underwent cervical LEEP procedure, with pathology showing high-grade squamous intraepithelial lesion with extensive glandular involvement and positive margins (Figure 2A). Subsequently, cervical cold knife conization was performed, with postoperative pathology showing CIN 2 and negative margins (Figure 2B). HPV typing in this case was based on preoperative cervical cancer screening results; HPV DNA testing was not performed on the ovarian tumor tissue.
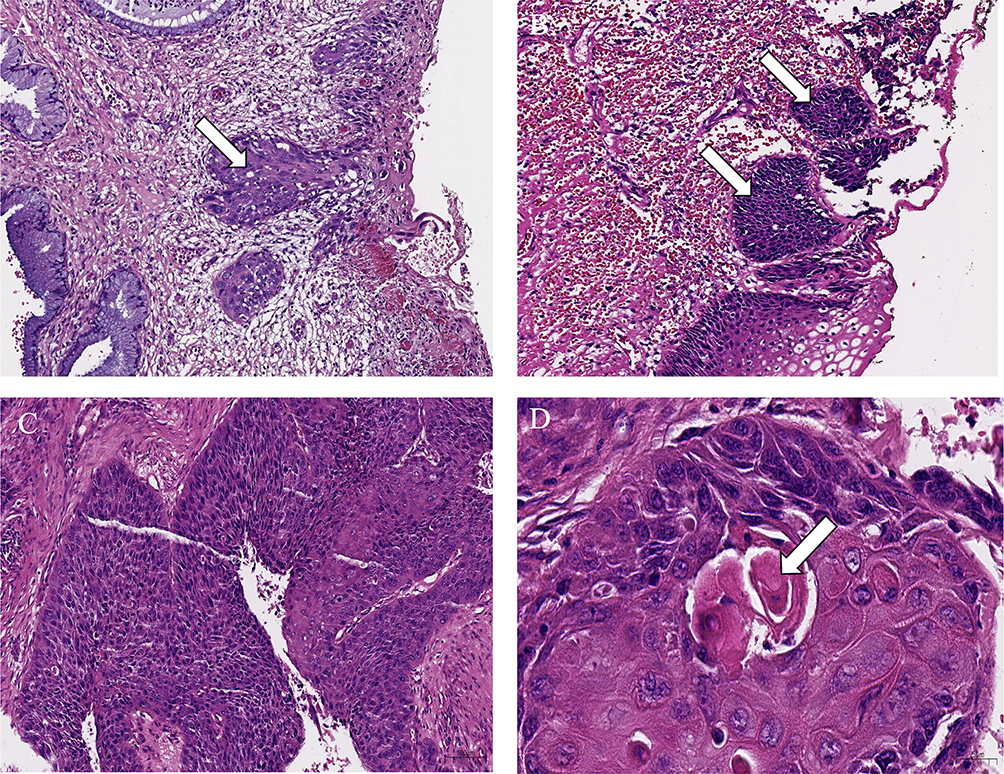 |
Figure 2 Histopathological examination results. (A) Cervical cone biopsy tissue: high-grade squamous intraepithelial lesion (HSIL, CIN 3), arrows indicate high-grade squamous intraepithelial lesion; (B) Cervical cold knife conization tissue: high-grade squamous intraepithelial lesion (CIN 2), arrows indicate high-grade squamous intraepithelial lesion; (C and D) Ovarian cystic teratoma: keratinizing squamous cell carcinoma (10× and 40×), arrows indicate keratin pearl formation. HPV types 16 and 59 were identified through preoperative cervical screening; direct HPV testing on ovarian tumor tissue was not performed. |
Following diagnosis of ovarian teratoma, surgical treatment was implemented. Then, the intraoperative exploration of the peritoneal cavity revealed a moderate amount of peritoneal fluid and numerous hair structures. A right-ovary generated mass, approximately 17×18 cm in size, was visible with surface rupture. The cyst contained multiple well-defined fatty lesions and matted hair with smooth surface. Multiple enlarged bilateral pelvic lymph nodes and para-aortic lymph nodes in a beaded pattern were observed.
Intraoperative frozen section examination showed cystic teratoma with epithelial atypia and mitotic figures. Based on the postoperative histopathological findings (Figure 2C and D), surgery revealed malignant transformation within mature cystic teratoma. The gross appearance of the resected ovarian mass is shown in Figure 3A and B, demonstrating an irregular cystic-solid mass approximately 17 cm in diameter with surface rupture and areas of hemorrhage. The patient subsequently underwent a comprehensive surgical staging procedure, including total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic/para-aortic lymphadenectomy. Histopathological assessment of the resected uterus, omentum, and lymph nodes confirmed the absence of malignant involvement.
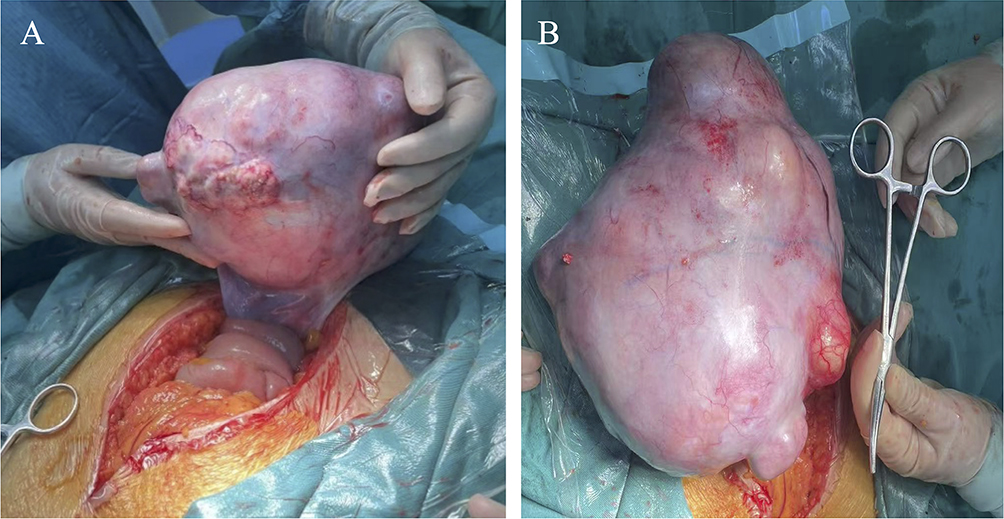 |
Figure 3 Surgical exploration findings. (A) Irregular cystic-solid mass approximately 17 cm in diameter showing smooth anterior surface with focal areas of surface irregularity and vascular engorgement; the tumor demonstrates areas of hemorrhage and surface rupture. (B) The same ovarian mass viewed from a different angle, displaying the characteristic appearance of the tumor with visible surface vasculature and areas of capsular breach; surgical instruments shown for scale reference. |
The operation was successful, and the patient recovered smoothly after operation. The patient was discharged 7 days after operation. According to the 2014 FIGO staging system, the woman was eventually diagnosed as stage IC. At present, the patient recovered well and planned to undergo BEP chemotherapy.
Discussion
Malignant transformation of ovarian MCTs is not a very common event, with the underlying pathogenic mechanism remaining incompletely elucidated. Existing evidence suggests that HPV infection may potentially drive the malignant progression of mature teratomas toward squamous cell carcinoma. Advanced age and increased tumor size constitute established risk factors for this transformation. Notably, the present case involved a premenopausal patient with a large tumor, aligning with these risk profiles.
The coexistence of cervical HPV infection and ovarian MCT malignant transformation in this case raises important questions about potential causal relationships. High-risk HPV subtypes, especially HPV-16 and −59, demonstrate distinct oncogenic profiles that may influence the pattern of malignant transformation. HPV 16 was considered as playing an important role during the squamous cell carcinoma development across multiple anatomical sites, showing remarkable ability to immortalize keratinocytes and induce squamous differentiation patterns.4,5 This viral preference for squamous cell carcinoma induction is particularly relevant when considering that 80% of MCT malignant transformations originate from ectodermal tissues containing squamous epithelium.6
HPV 59, identified in this case alongside HPV 16, belongs to the established high-risk oncogenic HPV group.7 While HPV 59 is recognized as oncogenic and capable of causing cervical cancer, its specific role in ovarian teratoma malignant transformation requires further investigation, as current research primarily focuses on HPV 16 and 18 in extragenital malignancies.8
The temporal sequence observed in this case—concurrent cervical HPV infection with subsequent ovarian MCT squamous cell carcinoma—suggests potential mechanisms by which cervical HPV infection might promote ovarian teratoma malignant transformation. Recent studies demonstrate that HPV can spread through an ascending route via the reproductive tract, with viral particles migrating from the cervix through the endometrium and fallopian tubes to reach the ovaries.9,10 This ascending infection pathway has been documented in various pelvic inflammatory conditions and may facilitate HPV access to ovarian tissues.11,12 Once HPV reaches the ovary, it could theoretically act upon the squamous epithelial components present in MCT ectodermal elements, potentially accelerating malignant transformation processes.13,14
The preoperative assessment of malignant potential poses a significant diagnostic challenge. Notably, ruptured tumors presenting with features such as ascites and fatty-density nodules on CT or MRI can be misinterpreted as benign mature cystic teratomas. In such contexts, elevated CA125 and SCCA in serum may serve as valuable biomarkers suggestive of transformation to squamous cell carcinoma.15 In the reported patient, who presented with abdominal pain, both elevated tumor markers and ascites were observed, consisting with tumor indicators.
The main pathogenic factor for cervical cancer is oncogenic HPV, primarily HPV 16 and HPV 18.16 Chiang et al discovered that HR-HPV infection may be a cause inducing mature ovarian teratoma transformation to squamous cell carcinoma.5 Vergote et al reported no invasive cervical carcinoma in ovarian squamous cell carcinoma cases; they speculated that ovarian squamous cell carcinoma might be a new lesion arising from HR-HPV infected ovarian epithelium.17
The molecular mechanisms by which HPV promotes malignant transformation involve the viral E6 and E7 oncoproteins, which block the regular cell cycle by intercepting tumor suppressor p53 and pRb, respectively.18 In the context of ovarian MCT, these oncogenic proteins could act specifically on squamous epithelial cells within teratoma tissues, leading to uncontrolled proliferation and eventual malignant transformation. This mechanism would explain why HPV-associated ovarian teratoma transformations predominantly manifest as squamous cell carcinomas rather than other histological types.19,20
Cooke et al conducted the first systematic genomic evaluation of ovarian squamous cell carcinoma arising in MCT and suggested that future treatment for MCT-SCC patients might involve immune checkpoint inhibitors.19 Tamura et al found through whole-gene analysis that APOBEC gene mutation frequency was closely related to HPV infection, suggesting that HPV infection might participate in gene mutations in MCT-SCC.21
On account of the rarity of malignant transformation in MCTs, standardized therapeutic protocol still unestablished, and the optimal management strategy remains undefined. Current practice is guided by disease stage: following comprehensive surgical staging, patients with stage IA disease may be candidates for conservative management, whereas those with advanced-stage disease should undergo optimal cytoreductive surgery to enhance survival.22 At present, combination therapy integrating cytoreductive surgery and adjuvant chemotherapy forms the mainstay of treatment.
Recently, immunotherapy has also shown promising prospects in MCT-SCC. PD-1 inhibitors such as pembrolizumab have achieved significant efficacy in HPV-related malignant tumors.23 Hackethal et al’s systematic review showed that early-stage cases could achieve 5-year survival rates above 75%, while advanced cases had poorer prognosis.24 Patient prognosis was affected by the type, volume, marker levels, and pathological stage of tumor.
This study has several limitations that should be acknowledged. First, due to the rarity of this disease, a standardized therapeutic protocol and optimal management strategy remain unestablished, and our treatment approach was based on current best practices rather than evidence from large-scale trials. Second, the low incidence of malignant transformation and lack of specific diagnostic criteria create inherent diagnostic challenges, where symptoms often mimic benign complications such as rupture or torsion. Third, most of the current studies on HPV-related malignant tumors outside the genital tract focus on HPV 16 and 18. We first reported ovarian teratomas infected with cervical HPV 16 and 59 at the same time, and the specific carcinogenic effects need further study. Fourth, as a single case report, the generalizability of our findings is limited, and larger cohort studies are needed to establish definitive causal relationships between cervical HPV infection and ovarian teratoma malignant transformation. Finally, the temporal sequence of HPV infection and malignant transformation cannot be definitively established in retrospective analysis.
Conclusion
In summary, the malignant transformation of ovarian MCT into squamous cell carcinoma is an infrequent but serious occurrence, which is associated with a distinctly poor clinical outcome. This case highlights the potential role of concurrent cervical HPV infection in promoting ovarian teratoma malignant transformation, particularly through the oncogenic effects of high-risk HPV types 16 and 59. The preferential development of squamous cell carcinoma in HPV-associated ovarian teratoma transformations supports the hypothesis that viral oncoproteins specifically target squamous epithelial elements within teratoma tissues. Future research should investigate the mechanistic pathways by which cervical HPV infection influences ovarian teratoma malignant transformation and explore targeted therapeutic approaches based on HPV status. The low incidence of malignant transformation in ovarian MCTs, combined with the lack of specific diagnostic criteria, often creates a diagnostic dilemma. Presenting symptoms such as abdominal pain and ascites can mimic complications of benign ovarian tumors, including torsion or rupture, Thus, heightened recognition of this potential diagnosis is essential and warrants more extensive clinical study.
Abbreviations
MCT, mature cystic teratoma; SCC, squamous cell carcinoma; HPV, human papillomavirus; HR-HPV, high-risk human papillomavirus; FIGO, International Federation of Gynecology and Obstetrics.
Ethical Statement
The study protocol was approved by the Ethics Committee for Clinical Trials of the Affiliated Hospital of Southwest Medical University (Approval No. KY2025417). Prior to participation, written informed consent was obtained from all potential subjects after a detailed explanation of the study. The Ethics Committee for Clinical Trials of the Affiliated Hospital of Southwest Medical University approved the publication of case details.
Acknowledgments
The authors would like to express gratitude to the doctors in the Imaging Department and Pathology Department for their assistance in the diagnosis process.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This case report involved no source of funding for any of the authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Outwater EK, Siegelman ES, Hunt JL. Ovarian teratomas: tumor types and imaging characteristics. Radiographics. 2001;21(2):475–7. doi:10.1148/radiographics.21.2.g01mr09475
2. Chen VW, Ruiz B, Killeen JL, et al. Pathology and classification of ovarian tumors. Cancer. 2003;97(10 Suppl):2631–2642. doi:10.1002/cncr.11345
3. Comerci JT, Licciardi F, Bergh PA, et al. Mature cystic teratoma: a clinicopathologic evaluation of 517 cases and review of the literature. Obstet Gynecol. 1994;84(1):22–28.
4. Ferris RL, Westra W. Oropharyngeal carcinoma with a special focus on HPV-related squamous cell carcinoma. Annu Rev Pathol. 2023;18:515–535. doi:10.1146/annurev-pathmechdis-031521-041424
5. Chiang AJ, Chen DR, Cheng JT, et al. Detection of human papillomavirus in squamous cell carcinoma arising from dermoid cysts. Taiwan J Obstet Gynecol. 2015;54(5):559–566. doi:10.1016/j.tjog.2015.08.008
6. Shi Z, Yang L, Bian C. Squamous cell carcinoma in mature cystic teratoma of the ovary induced by human papillomavirus 16 infection: a case report and literature review. Medicine. 2022;101(38):e30667. doi:10.1097/MD.0000000000030667
7. Bzhalava D, Eklund C, Dillner J. International standardization and classification of human papillomavirus types. Virology. 2015;476:341–344. doi:10.1016/j.virol.2014.12.028
8. Faridi R, Zahra A, Khan K, et al. Oncogenic potential of Human Papillomavirus (HPV) and its relation with cervical cancer. Virol J. 2011;8:269. doi:10.1186/1743-422X-8-269
9. Paradowska E, Haręża DA, Kania KD, et al. Human papillomavirus infection of the fallopian tube as a potential risk factor for epithelial ovarian cancer. Sci Rep. 2024;14(1):21602. doi:10.1038/s41598-024-72814-0
10. Bilyk OO, Pande NT, Pejovic T, et al. The frequency of human papilloma virus types 16, 18 in upper genital tract of women at high risk of developing ovarian cancer. Exp Oncol. 2014;36(2):121–124.
11. Kairys N, Roepke C. Tubo-ovarian abscess. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
12. Sibeko S, Sanderson M, Moyo S, et al. Role of the epithelium in human papillomavirus and human immunodeficiency virus infections in the female genital tract. Front Reprod Health. 2024;6:1408198. doi:10.3389/frph.2024.1408198
13. Graham SV. The human papillomavirus replication cycle, and its links to cancer progression: a comprehensive review. Clin Sci. 2017;131(17):2201–2221. doi:10.1042/CS20160786
14. Steinbach A, Riemer AB. Immune evasion mechanisms of human papillomavirus: an update. Int J Cancer. 2018;142(2):224–229. doi:10.1002/ijc.31027
15. Chen RJ, Chen KY, Chang TC, et al. Prognosis and treatment of squamous cell carcinoma from a mature cystic teratoma of the ovary. J Formos Med Assoc. 2008;107(11):857–868. doi:10.1016/S0929-6646(08)60202-8
16. Burd EM. Human papillomavirus and cervical cancer. Clin Microbiol Rev. 2003;16(1):1–17. doi:10.1128/CMR.16.1.1-17.2003
17. Verguts J, Amant F, Moerman P, et al. HPV induced ovarian squamous cell carcinoma: case report and review of the literature. Arch Gynecol Obstet. 2007;276(3):285–289. doi:10.1007/s00404-007-0333-5
18. Rahangdale L, Mungo C, O’Connor S, et al. Human papillomavirus vaccination and cervical cancer risk. BMJ. 2022;379:e070115. doi:10.1136/bmj-2022-070115
19. Cooke SL, Ennis D, Evers L, et al. The driver mutational landscape of ovarian squamous cell carcinomas arising in mature cystic teratoma. Clin Cancer Res. 2017;23(24):7633–7640. doi:10.1158/1078-0432.CCR-17-1789
20. Chiang AJ, Chen MY, Weng CS, et al. Malignant transformation of ovarian mature cystic teratoma into squamous cell carcinoma: a Taiwanese Gynecologic Oncology Group (TGOG) study. J Gynecol Oncol. 2017;28(5):e69. doi:10.3802/jgo.2017.28.e69
21. Tamura R, Nakaoka H, Yachida N, et al. Spatial genomic diversity associated with APOBEC mutagenesis in squamous cell carcinoma arising from ovarian teratoma. Cancer Sci. 2023;114(5):2145–2157. doi:10.1111/cas.15754
22. Park CH, Jung MH, Ji YI. Risk factors for malignant transformation of mature cystic teratoma. Obstet Gynecol Sci. 2015;58(6):475–480. doi:10.5468/ogs.2015.58.6.475
23. Wu M, Bennett JA, Reid P, et al. Successful treatment of squamous cell carcinoma arising from a presumed ovarian mature cystic teratoma with pembrolizumab. Gynecol Oncol Rep. 2021;37:100837. doi:10.1016/j.gore.2021.100837
24. Hackethal A, Brueggmann D, Bohlmann MK, et al. Squamous-cell carcinoma in mature cystic teratoma of the ovary: systematic review and analysis of published data. Lancet Oncol. 2008;9(12):1173–1180. doi:10.1016/S1470-2045(08)70306-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ruptured Ovarian Mature Cystic Teratoma with Adenocarcinoma Transformation: A Case Report
Xu L, Jiang J, Geng Q, Zhang Y
International Journal of Women's Health 2024, 16:2281-2285
Published Date: 21 December 2024