Back to Journals » International Medical Case Reports Journal » Volume 19
Human Coenurosis Caused by Taenia multiceps Mimicking a Thyroglossal Duct Cyst in a Child: A Case Report
Received 5 February 2026
Accepted for publication 20 April 2026
Published 25 April 2026 Volume 2026:19 601445
DOI https://doi.org/10.2147/IMCRJ.S601445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Charles Malisaba Posite,1,2 Henry Wabinga1,3
1Department of Pathology, Kampala International University Western Campus, Ishaka, Uganda; 2Department of Pathology, Université Catholique du Graben, Butembo, Democratic Republic of the Congo; 3Department of Pathology, Multisystem Laboratory, Kampala, Uganda
Correspondence: Charles Malisaba Posite, Kampala International University Western Campus, Ishaka, Uganda, Email [email protected]
Background: Coenurosis is a rare zoonotic parasitic infection in humans, caused by the larval stage (coenurus) of Multiceps multiceps, typically acquired through ingestion of ova shed in the feces of infected canids. While the central nervous system is the most commonly affected site, extracranial involvement, particularly in the head and neck region, is exceedingly uncommon. In pediatric patients, such presentations may closely mimic congenital cystic lesions, leading to potential delays in diagnosis and management.
Case Presentation: We present the case of a 4-year-old male from the pastoralist Karamoja region of Northeastern Uganda who presented with a painless, slow-growing midline cystic neck mass of unspecified duration. The mass was mobile, located in the subcutaneous plane superficial to the strap muscles, and lacked communication with the deeper neck structures or oral cavity. Initially presumed to be a thyroglossal duct cyst, the lesion was managed via total surgical excision through a transverse neck incision. Histopathological examination revealed a thin-walled cyst containing multiple protoscolices with characteristic hooklets, consistent with a coenurus cyst caused by Multiceps multiceps. The patient’s postoperative recovery was uneventful.
Conclusion: This case, the first of its kind reported in Uganda, demonstrates that Multiceps multiceps can clinically mimic a thyroglossal duct cyst. It underscores the necessity of histopathologic evaluation for all pediatric neck masses in endemic regions. Definitive management requires a high index of suspicion for multi-organ involvement, necessitating postoperative systemic anthelmintics and screening for occult central nervous system or ocular disease to ensure comprehensive care.
Keywords: Multiceps multiceps, Taenia multiceps, coenurosis, thyroglossal duct cyst, case report
Introduction
Cystic neck lesions in pediatric patients encompass a wide differential diagnosis, often comprising slow-growing congenital anomalies such as thyroglossal duct cysts, dermoid cysts, branchial cleft anomalies, and lymphatic malformations.1 The gradual progression of these lesions often leads clinicians to favor a benign developmental etiology. Parasitic infections are rarely considered, particularly in non-endemic areas. However, cestode infections, especially those involving Multiceps multiceps, must remain a diagnostic consideration in endemic regions or in patients with relevant exposure history.2,3
Multiceps multiceps, often referred to as Taenia multiceps, is a cestode parasite that causes coenurosis, a zoonotic infection predominantly impacting intermediate hosts like cows, sheep, and goats. Humans are accidental intermediate hosts and acquire the infection through ingestion of Multiceps multiceps eggs excreted by canids like dogs, foxes, and coyotes that are the definitive hosts. In humans, the larval form (coenurus) typically localizes in the central nervous system, but rare presentations in subcutaneous tissue, muscles, or other extracranial sites have been documented.4,5
Neck involvement is exceptionally uncommon. To our knowledge, reports of Multiceps multiceps presenting as a midline cystic neck mass in children are exceptionally scarce. The clinical similarity to benign congenital cysts can obscure timely diagnosis and appropriate management. Accurate identification relies on a combination of imaging, histopathology, and sometimes serology or molecular methods. Early recognition is essential to prevent complications and guide surgical and antiparasitic treatment strategies.6,7 We present a case of human coenurosis mimicking a thyroglossal duct cyst in a 4-year-old male.
Case Presentation
From a histopathological perspective, we present the case of a 4-year-old male from the Karamoja region in northeastern Uganda, who presented to Matany Hospital with a painless, slow-growing midline neck swelling of unspecified duration. The Karamoja region is a semi-arid area where pastoralism is the primary livelihood, facilitating frequent contact between domestic dogs, livestock, and children. The attending medical doctor had the impression of a thyroglossal cyst and underwent surgical excision of the cystic mass. The mass was mobile, located in the subcutaneous plane, superficial to the strap muscles, and was removed via a standard transverse neck incision without communication to deeper neck structures or the oral cavity. Nonetheless, radiologic imaging was unavailable at the time of pathologic evaluation. However, the patient’s postoperative recovery was uneventful.
Pathological Findings
Gross Finding
The Multisystem Histopathology Laboratory received fragments of tissue weighing 5 grams, brown in color, and firm in consistency. All the fragments were processed using basic histological techniques and stained with hematoxylin and eosin.
Microscopic Finding
Histological examination revealed cestodes with multiple protoscolices containing hooklets (Figure 1) consistent with Multiceps multiceps.
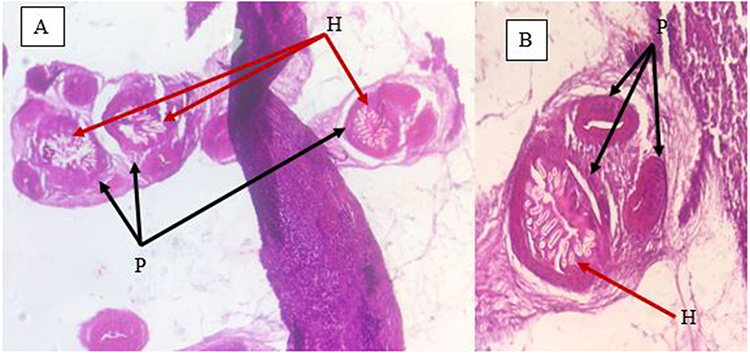 |
Figure 1 Hematoxylin and Eosin-stained sections (A-×100 and B-×200) show multiple protoscolices (black arrows) with visible hooklets (red arrows). |
Discussion
Coenurosis in humans is a rare parasitic infection caused by the larval stage (coenurus) of Taenia multiceps, a cestode primarily found in canids, including dogs, foxes, and coyotes. Human infection is accidental and occurs via fecal-oral transmission after ingestion of ova shed in the feces of definitive hosts. Once ingested, the larvae penetrate the intestinal wall and migrate to various tissues, most commonly the central nervous system, where they form coenurus cysts.2,3,5,8
Subcutaneous or extracranial manifestations are few, and cervical involvement is particularly unusual. To date, very few cases of coenurosis presenting as a cystic neck lesion have been documented in the literature, especially in pediatric patients.3,5,9 This case report presents a child with a midline cystic swelling in the neck, which on histology was diagnosed as Multiceps multiceps. To our knowledge, this is the first reported instance of a midline neck coenurus cyst clinically mimicking a thyroglossal duct cyst in a child in Uganda. We present it in a histopathological perspective.
The differential diagnosis of midline neck masses in children generally encompasses congenital defects, including thyroglossal duct cysts, dermoid cysts, and lymphangiomas. Infectious and neoplastic causes are considered less frequently unless clinical features are atypical.1,5 Parasitic infections are often overlooked, particularly in non-endemic areas. However, in regions where humans live in close proximity to infected livestock and dogs, as in many rural African and South Asian settings, parasitic causes must be considered.3,5 In the Karamoja region, domestic dogs commonly coexist with humans, contributing to close and sustained human-canine interaction that may facilitate the zoonotic transmission of parasitic infections.
The clinical characteristics were indistinguishable from those of a benign congenital cyst. Definitive diagnosis was achieved only through histopathological examination, which revealed the presence of multiple protoscolices with hooklets (rostellar hooks) within a cystic structure-hallmarks of a coenurus cyst.3,5,6
The management of this case requires considerations beyond simple surgical excision. Because the initial clinical suspicion was a congenital cyst, the surgery was likely performed without scolicidal agents, such as hypertonic saline, which increases the risk of local recurrence if the cyst wall was compromised. Therefore, the initiation of systemic albendazole therapy is essential to target any residual viable parasitic tissue.5,7
Furthermore, given the predilection of Multiceps multiceps for the CNS and the eyes, a comprehensive post-surgical follow-up protocol is mandatory.3,5,9 We recommend that such patients undergo a baseline neurological assessment and, where resources permit, cranial Computed Tomography or Magnetic Resonance Imaging to rule out asymptomatic neurocoenurosis. An ophthalmologic fundoscopic exam should also be performed to exclude intraocular involvement. While logistical constraints often hinder follow-up in resource-limited settings, the risk of neurocoenurosis makes screening a priority.
The epidemiological context of the Karamoja region cannot be overstated. The close-knit interaction between humans and canids in pastoralist communities creates a high-risk environment for the ingestion of Multiceps multiceps ova. Addressing this requires a “One Health” approach, combining pediatric clinical vigilance with veterinary public health measures, such as the routine deworming of domestic dogs and education on the proper disposal of infected livestock offal to break the parasite’s life cycle.5,7,10
Limitations
This report is limited by its retrospective histopathological nature and the constraints of a resource-limited setting. The lack of preoperative imaging and specific intraoperative data reflects challenges in clinical-pathological correlation. These gaps underscore the necessity for standardized postoperative protocols and heightened clinical vigilance for rare zoonoses in endemic regions.
Conclusion
This case represents an exceptionally rare presentation of Multiceps multiceps infection as a midline cystic neck lesion in a pediatric patient. Definitive management extends beyond the operating theater; it necessitates a high index of suspicion for multi-organ involvement and a robust follow-up strategy including anthelmintic therapy and CNS staging. Public health interventions, particularly in pastoralist regions like Karamoja, remain the cornerstone for preventing further pediatric morbidity from this neglected zoonosis.
Ethics Approval
Institutional review board approval was not required for a single anonymized case report according to local institutional policy.
Consent for Publication
Written informed consent was obtained from the patient’s mother for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, took part in drafting and reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Jackson DL. Evaluation and management of pediatric neck masses an otolaryngology perspective. Physician Assist Clin. 2018;3:245–4. doi:10.1016/j.cpha.2017.12.003
2. Ing MB, Schantz PM, Turner JA. Human coenurosis in north america: case reports and review. Clin Infect Dis. 1998;27:519–523. doi:10.1086/514716
3. Nhlonzi GB, Mwazha A. Clinicopathological review of human coenurosis in Kwazulu- Natal, South Africa: a retrospective single center study. Iran J Parasitol. 2022;17:62–69. doi:10.18502/ijpa.v17i1.9017
4. Abbas I, El-Alfy E-S, Saleh S, Tamponi C, Varcasia A. Global epidemiology and molecular biology of Taenia multiceps: a comparative meta-analysis and in silico analysis study. Parasitology. 2022;49:1607–1622. doi:10.1017/S0031182022001123
5. Varcasia A, Tamponi C, Ahmed F, et al. Taenia multiceps coenurosis: a review. Parasit Vectors. 2022;15:1–18. doi:10.1186/s13071-022-05210-0
6. Alex CE, Hébert J, Boabaid F, Ambrose D, Howerth EW. Pathology in Practice. JAVMA. 2017;250:393–395. doi:10.2460/javma.250.4.393
7. Abbas I, Tamponi C, Madau G, Cavallo L, Varcasia A, Scala A. Treatment and management of coenurosis by Taenia multiceps: field data from outbreaks in endemic regions and literature review. Parasit Vectors. 2024:1–17. doi:10.1186/s13071-024-06430-2
8. Wilson VCLC, Wayte DM, Addae RO. Human coenurosis-the first reported case from Ghana. Trans R Sov Trop Med Hyg. 1972;66:611–623. doi:10.1016/0035-9203(72)90307-0
9. Ali SM, Reddy PS, Venugopal S, Chhabra M, Mahadevan A. Cerebral coenurosis masquerading as malignancy: a rare case report from India. J Neurosci Rural Pr. 2019;10:367–370. doi:10.4103/jnrp.jnrp
10. El OJ, Shelef I, Cagnano E. Taenia multiceps: a rare human cestode infection in Israel. Vet Ital. 2015;44:621–631.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.