Back to Journals » Open Access Emergency Medicine » Volume 14
How Should We Approach Syncope in the Emergency Department? Current Perspectives
Authors Canakci ME ![]() , Sevik OE, Acar N
, Sevik OE, Acar N ![]()
Received 21 November 2021
Accepted for publication 10 February 2022
Published 27 June 2022 Volume 2022:14 Pages 299—309
DOI https://doi.org/10.2147/OAEM.S247023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Mustafa Emin Canakci, Omer Erdem Sevik, Nurdan Acar
Emergency Department, Eskisehir Osmangazi University, Eskisehir, Turkey
Correspondence: Mustafa Emin Canakci, Emergency Department, Eskisehir Osmangazi University, Prof. Dr. Nabi Avcı Boulevard, No: 4, Meselik, Odunpazarı, Eskisehir, 26040, Turkey, Tel +902222392979 – 5607, Email [email protected]
Abstract: Syncope is a clinical picture that can affect all age groups and has an important place in admissions to the emergency department. There is an important diagnostic challenge in cases where there are different clinical presentations and patients cannot express the situation clearly. Although the emergency department facilities for the diagnosis of syncope are limited, the diagnosis of many patients can be differentiated from life-threatening conditions with a detailed history and physical examination. High-risk patients should be identified and directed for definitive treatment by emergency medicine physicians. This review contains information about the management of the syncope patient in the emergency department.
Keywords: syncope, emergency department, high risk
Background
Syncope is a clinical syndrome that is defined as a transient loss of consciousness (TLOC) that has a rapid onset, occurs for a short period of time, and a full recovery expectancy after the episode with or without underlying specific conditions.1 It is a symptom that could be observed in various diseases on a scale from benign to malignant. Syncope, for the most time, occurs after inadequate cerebral perfusion.1 There are also other conditions in which TLOC could be observed with preserved cerebral perfusion (eg, hypoglycemia, seizures). While the loss of postural tonus is typical after syncope, it should be noted that there are other life-threatening conditions in which loss of postural tonus is also present and, in this paper, they are mentioned as “malignant syncope”. These malignant syncopes can also be defined as conditions that have a high potential for morbidity and mortality in short term without proper intervention. Syncope is self-limited and typically occurs for a very brief period (usually 8–10 seconds).
Syncope is not an uncommon reason for admission to the Emergency Department (ED) which accounts for 0.6–3% of visits annually around the world.2–4 It is observed in men and women roughly equally.5,6 Incidence increases as patients get older with the most significant increase in the 6th decade of life.5
Below are the most frequent conditions that can present themselves with TLOC in the Emergency Department.
- Reflex syncope (sometimes called “vasovagal syncope” or “neurocardiogenic syncope”)
- Orthostatic syncope
- Myocardial infarctions and cardiac arrhythmias
- Pulmonary embolism
- Structural cardiopulmonary diseases
- Epilepsy, seizures
- Hypoglycemia
- Hemorrhagic events leading to shock
- Postural orthostatic tachycardia syndrome
- Adenosine sensitive syncope
- Transient ischemic attack.
It should be noted that myocardial infarctions, cardiac arrhythmias, pulmonary embolism and hemorrhagic events are not the direct cause but rather predispose patients to have malignant syncope due to their negative effects on hemodynamic stability.
Syncope can be classified into three groups as reflex, orthostatic and cardiac syncope according to the cause.
Syncope can also be classified by pathophysiology. This classification centers around cerebral hypoperfusion due to low blood pressure. Mechanisms that result in falls in both cardiac output and peripheral resistance may cause syncope or malignant syncope. Most of the time, pathophysiology of the conditions overlaps.1
Three main causes of low total peripheral resistance are decreased reflex activity, functional and structural impairment of the autonomic nervous system (ANS). Decreased reflex activity causes vasodilation and is called “vasodepressor type”. ANS impairment works mainly when patients get to an upright position from a sitting or supine stance causing insufficient vasoconstriction. Cardiac output is affected by four primary causes. These are reflex bradycardia (cardioinhibitory reflex), arrhythmia, structural disease (including pulmonary embolism), and pulmonary hypertension (PHT). Arrhythmia, structural diseases, and PHT are classified as ‘cardiovascular causes’ altogether.1
We aimed to develop a methodological approach in the Emergency Department for syncope patients. This methodological approach covers syncope reasons to evaluate and differentiate between benign and malignant conditions.
History and Patient Characteristics
When caring for syncope patients in ED, caring clinicians must be aware that patient characteristics are as important as event history. Syncope in the elderly is important. Because presentation in this age group is challenging and often recognition is the first step to optimizing management and care of these patients. To start with, syncope in the older patient is under-recognized, especially in emergency department because the presentation can be atypical.7 Also, as age is an independent risk factor for various individual cardiovascular and neurological diseases, an older patient with syncope is at more risk for malignant causes of syncope than a younger one. Elder patients might also have several illnesses in their past medical history which might contribute to their pre-test possibility due to the cumulative risk of those conditions.
Patients’ hetero-anamnesis also gives valuable clues about the etiology of the episode, especially in patients with post-syncope confusion who might not be aware of the situation to its full extent. For example, lateral tongue bites and urinary incontinence might direct the diagnosis more to epileptic convulsion while pallor and sweaty appearance might suggest hemodynamic instability or cardiac events.
A comprehensive history by the patient and/or witnesses (if any) might give valuable information about the etiology of the syncope. The following questions should be asked:
- Duration of the episode
- Frequency of the episodes (if more than one)
- Existence of any triggers
- Position in which syncope has occurred
- Any accompanying symptoms (eg, chest pain, dyspnea, headache)
- Medical history and history of any inherited cardiac or neurovascular disorders in the family
- Use of any prescribed or recreational drugs.
Duration and Frequency of the Episode
Less frequent episodes usually point towards non-life-threatening disorders, whereas frequent ones especially if they are new-onset should raise clinical suspicion for more malignant disorders. However, low frequency should not be taken as a low-risk indicator in and on itself and it should be taken into consideration in concurrence with other features of the patient’s medical history. Patients with no significant clinical disorder with prolonged syncope durations might have psychogenic underlying causes.
Existence of Any Triggers
When obtaining the history from the patient; circumstances surrounding the episode should be asked as they could reveal specific triggers. Situations that should be evaluated in this area include:
- Whether syncope has occurred during or after exercise. (Syncope during exercise would raise suspicion for cardiac conduction disorders, whereas syncope after exercise is a benign situation)
- During or after urination, defecation, sneezing or coughing. (Syncope that is triggered by those is most likely benign vasovagal)
- Syncope after standing for a long time (mostly benign)
- Syncope triggered by emotional stress (mostly psychogenic).
Position in Which Syncope Has Occurred
Syncope during standing is associated with more benign conditions. If syncope occurred after standing up from a supine position, clinician should be suspicious of orthostatic causes. If syncope occurred during supine position, more serious illnesses like cardiac arrhythmias should be considered as the cause.
Any Accompanying Symptoms
Any symptoms that patients are complaining about before, during, or after the syncope should be evaluated carefully as they could reveal disorders that are malignant causes of syncope. Benign syncope patients might have prodromal symptoms before the episodes.1 These symptoms include light-headedness, visual impairments, palpitations, and nausea.
Medical History and History of Any Inherited Cardiac or Neurovascular Disorders in the Family
Any condition in patient’s medical history (eg, epilepsy) that can result in malignant syncope should be evaluated and ruled in or out as the reason. Family history of structural cardiac diseases (eg, Hypertrophic Cardiomyopathy, Brugada Syndrome) or neurovascular disorders should also be evaluated especially in relatively younger patients.8,9
Initial Evaluation
Like any other patient, management of the syncope patient starts with A, B, C (Airway, Breathing, Circulation). Patients (or relatives) might declare if they had a complete recovery or not. Patients might be hypoxic, and there might be perfusion disorders due to malignant arrhythmias. Thus, it is important to take every patient into the circle of security and cardiac monitorization. In any case, syncope, by definition, is a situation that a full recovery is expected. Thus, if decrease in the consciousness level is still ongoing, caring physician must be alert for malignant syncope.
Patient’s vital parameters with orthostatic readings must be obtained firstly. If there is an anomaly in those, evaluation should be focused on but not limited to those. Hypoxemia, hypotension, or tachycardia could be present in benign syncope as well as other malignant conditions.10
If the patient is hypoxic, differential diagnosis includes but is not limited to pulmonary embolism, tension pneumothorax, pericardial tamponade, acute coronary syndromes, and pneumonia. In unstable patients, treatment for the underlying cause should start immediately with appropriate intervention (eg, needle thoracotomy, pericardiocentesis, fibrinolytic agents, and cardiac catheterization). In tachycardic patients, ventricular or supraventricular arrhythmias might be present and intervention should start according to the guidelines in the earliest possibility.11 If the patient has low blood pressure readings, he/she should be evaluated for fluid status and should be intervened. In hypertensive patients, a search for hypertensive emergencies should start and antihypertensive agents should be started in the presence of said emergencies.12
Blood glucose must be obtained at the start of the evaluation. If there is hypoglycemia, it should be corrected before ordering any further diagnostic tests. The mainstream treatment for hypoglycemia is 25g of intravenous dextrose not exceeding 10% concentration from a peripheral line. This equals to 250 milliliters of 10% dextrose or 500 milliliters of 5% dextrose. In hyperglycemic patients, treatment is not initiated as rapidly as hypoglycemia, but these patients should be evaluated carefully for hyperosmotic-hyperglycemic state and diabetic ketoacidosis.
A full physical examination with special emphasis on neurological and cardiovascular examinations must be done. Confusion can be present in benign syncope patients as well as some other diseases (eg, post-ictal state after a seizure, stroke, hypoglycemia, diabetic ketoacidosis). Lung auscultation could reveal pneumothorax and pneumonia. Cardiac auscultation could reveal pericardial rubbing and murmurs especially in the aortic site in patients with thoracic aortic aneurysm, aortic dissection, or aortic stenosis. Tenderness or pulsatile mass in the abdomen is a sign of abdominal aortic aneurysm rupture and could potentially cause loss of consciousness and hemorrhagic shock. Rectal examination is also warranted for the presence of hematochezia or melena as they could be the reason for syncope as well. The head, thorax, abdomen, and extremities should be examined for the signs of trauma. Trauma could potentially happen before or after the loss of consciousness.13
Diagnosis
Diagnostic tests should be ordered after the initial evaluation and patient stabilization. An ECG is essential to rule out ST-segment elevated myocardial infarction (STEMI), Mobitz Type 2 atrioventricular block, and 3rd degree atrioventricular block. Other diagnostic tests such as laboratory, chest x-ray, and computerized tomography should only be obtained on selected cases in selected conditions.
ECG
An ECG is a “must do” diagnostic test that any syncope patient should undergo. Apart from obvious malignant syncope reasons such as ventricular tachycardia, ventricular fibrillation, and STEMI, which clinician should be on alert for during patients’ course of stay, ECG can reveal subtle but important findings. Rhythm strip of emergency medical services should also be obtained if available and possible as those measurements might show transient cardiac arrhythmias. Second- or third-degree blocks can also be diagnosed with ECG. In third-degree heart block, there is complete absence of AV conduction, with none of the supraventricular impulses conducted to the ventricles. Mobitz type 2 AV block in which there are intermittent non-conducted P waves without progressive prolongation of the PR interval. These atrioventricular conduction disorders may present with syncope to the ED (Figure 1). Bifascicular block is another ECG abnormality that can cause syncope which presents with RBBB with left anterior fascicular block, manifested as left-axis deviation or RBBB and left posterior fascicular block (LPFB), manifested as right-axis deviation in the absence of other causes.14
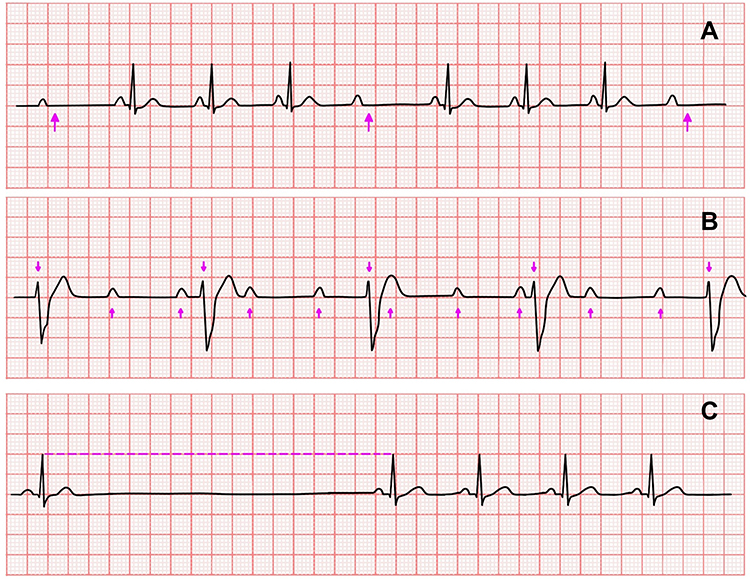 |
Figure 1 (A) Mobitz type 2 AV Block. There is intermittent non-conducted P waves without progressive prolongation of the PR interval. (pink arrow: p wave not followed by a QRS complex). (B) Third degree AV Block. ECG demonstrates complete AV dissociation, with independent atrial and ventricular rates (arrows pointing up: atrial activity; arrows pointing down: ventricular activity). (C) Sinus pause. |
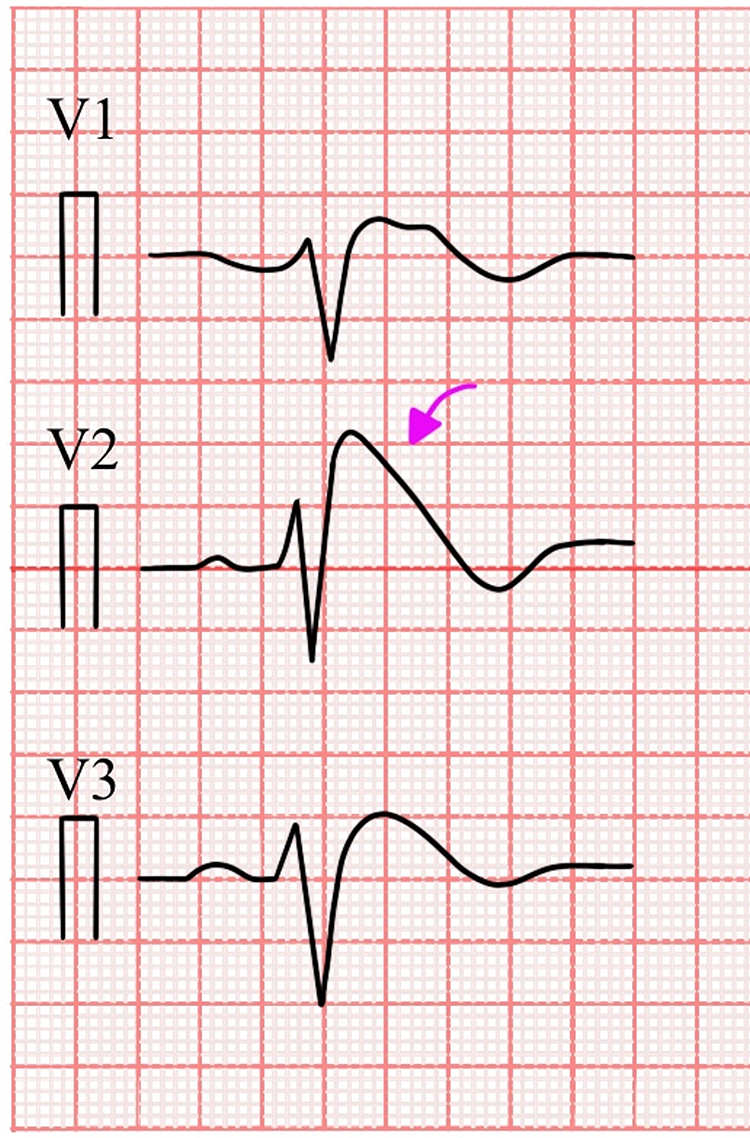 |
Figure 2 Brugada type 1 (pink arrow: Coved type ST-segment elevation in V2). |
 |
Figure 3 (A) Wolff-Parkinson-White (WPW) syndrome (pink arrow: Delta wave). (B) Long QT interval. (pink arrow: QT interval). |
Pulmonary embolism also has a specific pattern in ECG. This usually can be detected in more severe cases. Thus, ECG cannot be used to rule out pulmonary embolism but can be used as an adjunctive for diagnosis. ECG demonstrates right ventricular strain findings. These are sinus tachycardia, S1Q3T3 pattern (S wave in D1, Q wave in D3, and inverted T wave in D3), right bundle branch block (RBBB) and inverted T waves in V1-V4.15
Sinus node dysfunction is defined with these ECG features: sinus bradycardia, sinus pause, and inadequate heart rate response to activity. While asymptomatic patients (these patients are susceptible to bradycardia and relevant symptoms) sinus pauses lesser than three seconds might not require specific treatment, patients with persistent fall in the heart rate (≤50 bpm) and with sinus pauses more than three seconds do.1 Symptoms due to low cardiac output and end-organ hypoperfusion are also another indication for treatment. Patients with relatively milder degrees of sinus bradycardia might also benefit from the treatment in the absence of other causes of malignant syncope.16 These patients should be referred to syncope clinics for 24-hour Holter monitorization. ICDs are useful in symptomatic sinus pauses without any apparent underlying condition.1 While relatively a benign condition, reflex syncope patients might have intermittent sinus pauses, and these ECG findings might not present themselves in the first obtained ECG strip. ECG monitorization of these patients in the ED is important to “catch” the sinus pause and differentiate between benign and malignant syncope.
Supraventricular tachycardias (SVTs) are tachycardias that are originated from or above the His-bundle. The most typical presentation in the absence of P waves with regular QRS complexes is atrioventricular nodal re-entrant tachycardia.17 In patients with SVT, while uncommon, syncopal episodes could be observed. These patients typically complain about palpitations, light-headedness, or shortness of breath before the event. Current guidelines recommend vagal stimulations and adenosine for both differential diagnosis and treatment. In syncope patients who do not have a clear cause for syncope and who have typical complaints of SVTs but no documented ECG referral to a syncope clinic for 24-hour Holter monitorization or implantable loop recorders might be beneficial to diagnose the presence of SVTs and to differentiate between its various forms.18
Brugada syndrome is an inherited cardiac disease that can cause ventricular arrhythmias. Three types of Brugada pattern are defined and type 1 carries the high risk for malignant syncope.1,19 Only type 1 has definite diagnostic criteria for the disease. It can be detected on ECG with ST-segment elevation followed by a convex descension in V1-3 leads followed by an inverted T wave (Figure 2).19 In patients with silent ECGs with a positive family history of the disease, a sodium channel blocking agent is used to induce the Brugada pattern.20 Thus, sodium channel blocking agents in patients who present to the ED with syncope should be avoided. ICDs are recommended for treatment.1
Atrial fibrillation with pre-excitation might result in rapid ventricular contractions which can evolve into ventricular fibrillation. It is a potentially lethal ECG finding which can also cause malignant syncope.21 Optimal ventricular rate in AF is determined as lesser than 110 bpm. In the ED, type of intervention depends on the patient’s hemodynamic stability as a first step. In unstable patients, electrical cardioversion is the choice of treatment, whereas in stable patients ß-blockers or calcium channel blockers are recommended.22 The most common ventricular pre-excitation syndrome, Wolff-Parkinson-White syndrome, has following ECG characteristics: A delta wave, short P-R interval, wide QRS complex with repolarization abnormalities (Figure 3).23 However, in the absence of anterograde conducting accessory pathway, ECG characteristics of WPW might not be observed. It can be diagnosed in the electrophysiological study.
Left ventricular hypertrophy is a structural cardiac disease that can lead to left ventricular outflow tract obstruction resulting in syncope. While it may be seen in patients with uncontrolled hypertension in the chronic setting, in patients with valvular diseases, hypertrophic cardiomyopathy which is an inherited disease might also be responsible for an increase in left ventricular mass. Regardless of the etiology, high QRS amplitudes in various leads are observed in ECG. The Romhilt-Estes score is one of the many scores that can be used to diagnose left ventricular hypertrophy in ECG.24
Epsilon wave is another ECG anomaly that can be seen in arrhythmogenic right ventricular cardiomyopathy. It is a rare disease that affects relatively younger patients. It may result in ventricular arrhythmias and can be life threatening.25,26
Repolarization abnormalities in the myocardium are also another reason for syncope. It presents itself in ECG with long QT interval and T wave abnormalities. The normal QT interval should be lesser than 460 milliseconds.1 It should be noted that QT interval is affected by heart rate and a corrected QT interval should be used to make clinical decisions. Long QT syndrome might be hereditary or acquired. Drugs and hypocalcemia are the most common causes for acquired long QT syndrome. Long QT interval is associated with syncope and sudden cardiac death due to Torsades de Pointes, a special form of ventricular arrhythmia that is detected in ECG.27 Some psychoactive drugs to treat psychiatric conditions as well as drugs to treat certain cardiovascular disorders are associated with long QT syndrome.28 As the risk for drug-induced long QT syndrome is greater in female or older patients who use multiple drugs, those patients should be careful.29 This classification is important because while certain antiarrhythmic drugs, left ventricular denervation, and ICDs are used in congenital long QT syndrome, the treatment for acquired long QT syndrome depends on the underlying cause.30 Patients with congenital long QT syndrome should be monitored intensively and be consulted with interventional cardiologists in the ED.
Point-of-Care Ultrasonography (POCUS)
POCUS is an easy to use and readily available tool in most EDs, and it is widely used in various conditions.31 Lack of ionizing radiation and allowing for repeated bedside examinations makes it feasible to use in EDs. It provides a rapid assessment of various life threatening conditions.32
There is no one decided protocol of POCUS for syncope but Rapid Ultrasound for Shock and Hypotension (RUSH) protocol for hypotensive patients might also be suitable for syncope patients as it focuses on areas that would also be the cause for syncope.
This protocol includes:
- Bedside echocardiography (apical four chamber view, parasternal long and short axis views)
- Acute Coronary Syndromes
- Pericardial tamponade
- Evaluation of right ventricles for pulmonary embolism
- Thoracic aortic aneurysm and dissection
- 2nd or 3rd degree AV blocks (These disorders are primarily diagnosed with ECG but POCUS can be used in patients with indefinite ECG readings).33
- Hypertrophic or dilated cardiomyopathies
- Prosthetic valve disfunction
- Pulmonary views for each lung
- Pneumothorax
- Fluid overload in congestive heart failure
- Pneumonia
- Free fluid in the abdomen
- Morrison’s pouch (including hemothorax view)
- Splenorenal pouch (including hemothorax view)
- Evaluation of abdominal aorta
- Six-point compression examination for deep vein thrombosis
- Ectopic pregnancy search (in women of childbearing age).
Laboratory
Choice of bloodwork depends on the findings of initial evaluation, physical examination, ECG, and POCUS findings. There is not one single test to be ordered in all syncope patients. Complete blood count can be ordered to rule in or out anemia as low hemoglobin and hematocrit levels could predispose patients to have orthostatic syncope due to volume depletion. Venous blood gas analysis would reveal certain intoxications such as carbon monoxide and it would be useful to get a quick glance at patient’s electrolytes and acid-base status. Any patient with ECG abnormalities (newly developed) or high-risk factors in history or physical examination for acute coronary syndromes should undergo cardiac testing. D-dimer testing might be suitable in patients with suspected pulmonary embolism according to the risk stratification with scoring systems such as Wells criteria or Geneva Score. Women of childbearing age should be tested for pregnancy as an addition to other bloodwork.
Computerized Tomography (CT)
Computerized tomography is a diagnostic modality that uses ionizing radiation. Current literature suggests that computerized tomography is overused unnecessarily in syncope patients.34–36
Most of these patients have no abnormalities in their CT scans.37 Thus, in syncope patients, there is no indication of routine CT scan. This modality should be reserved for patients with neurological deficits before or after the episode as they would suggest a central nervous system disorder for the cause of the syncope. In syncope patients with head trauma, patients should be asked and examined for high energy yielding trauma, which can have a high risk of intracranial hemorrhages. There are scoring systems that can guide a clinician’s deciding pathway (NEXUS head trauma score, Canadian CT Head Score to name a few).
CT is also useful for differential diagnosis of the syncope with clinical findings of certain conditions. It is readily available in most EDs worldwide and has huge diagnostic value in potentially life-threatening conditions, such as pulmonary embolism and aortic dissection. These scans of thorax and abdomen should be used according to their respective guidelines.
Chest X-Ray
Chest x-ray is a radiographic modality that can successfully diagnose various diseases that could cause syncope such as pneumothorax, pneumonia, congestion due to heart failure. It also gives clues for some conditions such as pulmonary embolism (Hampton’s hump), thoracic aorta aneurysm, and dissection (calcium sign).38,39
There are conflicting studies on whether syncope patients should get chest x-ray routinely in their admission. A study published in 2006 by Wong et al suggests chest x-rays have modest diagnostic utility in syncope patients, but it fails to rationalize routine chest x-rays as of now.40 It might be useful in rural settings with limited diagnostic resources to rule out mentioned reasons for syncope. Since most of the chest x-rays of syncope patients are normal, cost-effectiveness and radiation exposure should be kept in mind when ordering this diagnostic tool and should be limited to selected patients.
Treatment
There is no “one fits all” treatment for syncope patients. Treatment should be guided by diagnosis and those diagnoses’ respective guidelines. Patients with life-threatening cardiac arrhythmias or acute coronary syndromes should be consulted from ED to get an implantable cardiac defibrillator or coronary angiography. Pulmonary embolism patients and stroke patients should be evaluated for the necessity of fibrinolytic treatment and/or anticoagulation or other treatment modalities. Patients who have orthostatic syncope due to dehydration or acute bleeding should get volume replacement therapy according to the cause. For reflex syncope patients, education and referral to a syncope unit might be suitable as it might reoccur during their lifetime.
Risk Stratification
Risk stratification for syncope patients should be done with event history, past medical history, physical examination findings, ECG features, and POCUS. This assessment provides guidance for further testing, treatment as well as disposition.
For this purpose, the San Francisco Syncope Rule can also be used. It predicts major outcomes at 7 days in patients with syncope. History of congestive heart failure, hematocrit level below 30, ECG abnormalities, dyspnea, and systolic blood pressure below 90 mmHg at admission are the components of the score. If any of these parameters are disrupted patient is not considered low risk and safe discharge is not recommended. A meta-analysis by Serrano et al puts San Francisco Syncope Rule’s sensitivity level at 86% and specificity at 49%.41
Conclusion
Syncope is a symptom of various diseases. ED management of syncope should primarily focus to distinguish between benign causes and underlying malignant conditions. Low-risk patients can safely be discharged from the ED. Patients who have neither low- nor high-risk features can be classified as moderate risk. For these patients, prolonged observation of ED might be appropriate. Any patient who has high-risk features should undergo diagnostic testing and get treatment for their specific underlying condition. It should not be forgotten that patients may have overlapping conditions and treatment should be directed for every individual condition.
Step-by-Step Approach
We offer the following step-by-step approach to syncope patients in the ED:
- Stabilize the patient. Start with A, B, and C and correct the defects in those if you find any.
- Get a bedside glucose reading simultaneously with history taking.
- Obtain a comprehensive history from the patient and witnesses to get a clue about the nature of the syncope. Specifically ask for symptoms of diseases that can cause malignant syncope.
- Get an ECG to rule in or out any cardiac pathology.
- Assess for the trauma.
- Do a full physical exam with rectal digital exam.
- Perform POCUS to rule in or out syncope causes.
- Order laboratory testing guided by history and physical exam.
- Order imaging techniques guided by history, physical exam, and POCUS.
- Start the treatment guided by the diagnosis.
- Evaluate the patient for hospitalization or disposition according to risk stratification.
- If you decide on disposition, re-do the physical exam before discharge. Do not forget: By nature, patients might be asymptomatic after the episode and occult findings might reveal themselves later.
- Educate the patient about the syncope. Mention symptoms of life-threatening diseases and advise the patient to re-admit to the ED if he/she experiences any of them. Refer patient to syncope clinic.
Acknowledgments
We thank Mumin Murat Yazici, MD for the illustrations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brignole M, Moya A, de Lange FJ, et al. 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883–1948. doi:10.1093/eurheartj/ehy037
2. Thiruganasambandamoorthy V, Hess EP, Turko E, Perry JJ, Wells GA, Stiell IG. Outcomes in Canadian emergency department syncope patients – are we doing a good job? J Emerg Med. 2013;44(2):321–328. doi:10.1016/j.jemermed.2012.06.028
3. Probst MA, Kanzaria HK, Gbedemah M, Richardson LD, Sun BC. National trends in resource utilization associated with ED visits for syncope. Am J Emerg Med. 2015;33(8):998–1001. doi:10.1016/j.ajem.2015.04.030
4. Greve Y, Geier F, Popp S, et al. The prevalence and prognostic significance of near syncope and syncope: a prospective study of 395 cases in an emergency department (the SPEED study). Dtsch Arzteblatt Int. 2014;111(12):197–204. doi:10.3238/arztebl.2014.0197
5. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878–885. doi:10.1056/NEJMoa012407
6. Ruwald MH, Hansen ML, Lamberts M, et al. The relation between age, sex, comorbidity, and pharmacotherapy and the risk of syncope: a Danish nationwide study. Eur Eur Pacing Arrhythm Card. 2012;14(10):1506–1514. doi:10.1093/europace/eus154
7. O’ Brien H, Anne Kenny R. Syncope in the elderly. Eur Cardiol. 2014;9(1):28–36. doi:10.15420/ecr.2014.9.1.28
8. Veselka J, Anavekar NS, Charron P. Hypertrophic obstructive cardiomyopathy. Lancet Lond Engl. 2017;389(10075):1253–1267. doi:10.1016/S0140-6736(16)31321-6
9. Mascia G, Della Bona R, Ameri P, Canepa M, Porto I, Brignole M. Brugada syndrome and syncope: a systematic review. J Cardiovasc Electrophysiol. 2020;31(12):3334–3338. doi:10.1111/jce.14787
10. Brignole M, Moya A, de Lange FJ, et al. Practical instructions for the 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):e43–e80. doi:10.1093/eurheartj/ehy071
11. Soar J, Böttiger BW, Carli P, et al. European resuscitation council guidelines 2021: adult advanced life support. Resuscitation. 2021;161:115–151. doi:10.1016/j.resuscitation.2021.02.010
12. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
13. Auer J. Syncope and trauma. Are syncope-related traumatic injuries the key to find the specific cause of the symptom? Eur Heart J. 2008;29(5):576–578. doi:10.1093/eurheartj/ehm637
14. Rivera-López R, Cabrera-Ramos M, Jordán-Martinez L, et al. Syncope and bifascicular block in the absence of structural heart disease. Sci Rep. 2020;10(1):8139. doi:10.1038/s41598-020-65088-9
15. Shopp JD, Stewart LK, Emmett TW, Kline JA. Findings from 12-lead electrocardiography that predict circulatory shock from pulmonary embolism: systematic review and meta-analysis. Acad Emerg Med off J Soc Acad Emerg Med. 2015;22(10):1127–1137. doi:10.1111/acem.12769
16. Doundoulakis I, Gatzoulis KA, Arsenos P, et al. Permanent pacemaker implantation in unexplained syncope patients with borderline sinus bradycardia and electrophysiology study-proven sinus node disease. J Arrhythmia. 2021;37(1):189–195. doi:10.1002/joa3.12460
17. Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(5):655–720. doi:10.1093/eurheartj/ehz467
18. Soulaidopoulos S, Arsenos P, Doundoulakis I, et al. Syncope associated with supraventricular tachycardia: diagnostic role of implantable loop recorders. Ann Noninvasive Electrocardiol. 2021;26(5):e12850. doi:10.1111/anec.12850
19. Bayés de Luna A, Brugada J, Baranchuk A, et al. Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report. J Electrocardiol. 2012;45(5):433–442. doi:10.1016/j.jelectrocard.2012.06.004
20. Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V. Brugada syndrome: diagnosis, risk stratification and management. Arch Cardiovasc Dis. 2017;110(3):188–195. doi:10.1016/j.acvd.2016.09.009
21. Sakthivel R, Selvaraj RJ. Atrial fibrillation and preexcitation - A licence to kill. Indian Pacing Electrophysiol J. 2020;20(1):1–2. doi:10.1016/j.ipej.2020.01.001
22. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
23. Milliez P, Slama R. [Wolff-Parkinson-White syndrome]. Rev Prat. 2004;54(16):1747–1753. French.
24. Romhilt DW, Estes EH. A point-score system for the ECG diagnosis of left ventricular hypertrophy. Am Heart J. 1968;75(6):752–758. doi:10.1016/0002-8703(68)90035-5
25. Gemayel C, Pelliccia A, Thompson PD. Arrhythmogenic right ventricular cardiomyopathy. J Am Coll Cardiol. 2001;38(7):1773–1781. doi:10.1016/s0735-1097(01)01654-0
26. Corrado D, Link MS, Calkins H. Arrhythmogenic right ventricular cardiomyopathy. N Engl J Med. 2017;376(1):61–72. doi:10.1056/NEJMra1509267
27. Shah SR, Park K, Alweis R. Long QT syndrome: a comprehensive review of the literature and current evidence. Curr Probl Cardiol. 2019;44(3):92–106. doi:10.1016/j.cpcardiol.2018.04.002
28. Roden DM. Predicting drug-induced QT prolongation and torsades de pointes. J Physiol. 2016;594(9):2459–2468. doi:10.1113/JP270526
29. Trinkley KE, Page RL, Lien H, Yamanouye K, Tisdale JE. QT interval prolongation and the risk of torsades de pointes: essentials for clinicians. Curr Med Res Opin. 2013;29(12):1719–1726. doi:10.1185/03007995.2013.840568
30. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36(41):2793–2867. doi:10.1093/eurheartj/ehv316
31. Andersen CA, Holden S, Vela J, Rathleff MS, Jensen MB. Point-of-care ultrasound in general practice: a systematic review. Ann Fam Med. 2019;17(1):61–69. doi:10.1370/afm.2330
32. Bhagra A, Tierney DM, Sekiguchi H, Soni NJ. Point-of-care ultrasonography for primary care physicians and general internists. Mayo Clin Proc. 2016;91(12):1811–1827. doi:10.1016/j.mayocp.2016.08.023
33. Canakci ME, Cure R, Sevik OE, Mert KU, Acar N. Man with syncope. Ann Emerg Med. 2021;77(4):e95–e96. doi:10.1016/j.annemergmed.2020.10.011
34. Giglio P, Bednarczyk EM, Weiss K, Bakshi R. Syncope and head CT scans in the emergency department. Emerg Radiol. 2005;12(1–2):44–46. doi:10.1007/s10140-005-0434-z
35. Grossman SA, Fischer C, Bar JL, et al. The yield of head CT in syncope: a pilot study. Intern Emerg Med. 2007;2(1):46–49. doi:10.1007/s11739-007-0010-5
36. Mitsunaga MM, Yoon HC. Journal club: head CT scans in the emergency department for syncope and dizziness. AJR Am J Roentgenol. 2015;204(1):24–28. doi:10.2214/AJR.14.12993
37. Viau JA, Chaudry H, Hannigan A, Boutet M, Mukarram M, Thiruganasambandamoorthy V. The yield of computed tomography of the head among patients presenting with syncope: a systematic review. Acad Emerg Med off J Soc Acad Emerg Med. 2019;26(5):479–490. doi:10.1111/acem.13568
38. Marshall GB, Farnquist BA, MacGregor JH, Burrowes PW. Signs in thoracic imaging. J Thorac Imaging. 2006;21(1):76–90. doi:10.1097/01.rti.0000189192.70442.7a
39. Lertsuwunseri V, Chattranukulchai P, Tumkosit M, Boonyaratavej S. Calcium sign of thoracic aortic dissection in Takayasu’s arteritis. BMJ Case Rep. 2018;2018:bcr2018224313. doi:10.1136/bcr-2018-224313
40. Wong ML, Chiu D, Shapiro NI, Grossman SA. Utility of chest radiography in emergency department patients presenting with syncope. West J Emerg Med. 2016;17(6):698–701. doi:10.5811/westjem.2016.8.29897
41. Serrano LA, Hess EP, Bellolio MF, et al. Accuracy and quality of clinical decision rules for syncope in the emergency department: a systematic review and meta-analysis. Ann Emerg Med. 2010;56(4):362–373.e1. doi:10.1016/j.annemergmed.2010.05.013
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.