Back to Journals » Patient Preference and Adherence » Volume 19
How Does Indonesian Chronic Disease Patient Adhere to Their Treatment? A Cross-Sectional Analysis of 11,408 Subjects
Authors Pradipta IS ![]() , Aprilio K
, Aprilio K ![]() , Ningsih YF
, Ningsih YF ![]() , Pratama MAA, Gatera VA
, Pratama MAA, Gatera VA ![]() , Alfian SD
, Alfian SD ![]() , Iskandarsyah A
, Iskandarsyah A ![]() , Abdulah R
, Abdulah R
Received 5 November 2024
Accepted for publication 3 January 2025
Published 22 January 2025 Volume 2025:19 Pages 173—184
DOI https://doi.org/10.2147/PPA.S503601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ivan Surya Pradipta,1,2,* Kevin Aprilio,1,2,* Yozi Fiedya Ningsih,1,2 Mochammad Andhika Aji Pratama,2 Vesara Ardhe Gatera,3 Sofa Dewi Alfian,1,2 Aulia Iskandarsyah,4 Rizky Abdulah1,2
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 2Drug Utilization and Pharmacoepidemiology Research Group, Center of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 3Department of Pharmaceutical Biology, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 4Department of Clinical Psychology, Faculty of Psychology, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia
*These authors contributed equally to this work
Correspondence: Ivan Surya Pradipta, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jalan Ir. Soekarno KM 21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Background: Chronic disease has become an increasing burden in Indonesia, increasing the importance of treatment adherence to control the disease prognosis. Therefore, we aim to determine the prevalence and characteristics of nonadherence in Indonesian chronic disease population.
Methods: We identified 11,408 adult subjects with chronic diseases from the fifth Indonesian Family Life Survey. We defined treatment nonadherence as the outcome variable and characteristics related to the World Health Organization Multidimensional Adherence Model as exposure variables. We used descriptive and multivariable analyses to analyze factors related to treatment nonadherence.
Results: We identified that 57% (95% CI 56.1– 57.9) of chronic disease patients were nonadherent to their treatment. Treatment nonadherence was notable in subjects with liver disease (61.8%), tuberculosis (59.8%), digestive diseases (57.9%), other lung diseases (56.8%), psychiatric diseases (51.6%), asthma (51.2%), and hypertension (50%). Treatment nonadherence was associated with socioeconomic-related factors of being aged 15– 65 years, living in rural areas, having history of formal education, and having a household size of 2– 6 people. Furthermore, in patient- and condition-related factors, positive perceptions of their health condition, missing 0– 7 days of their regular activity in the last month, being ex- and non-smokers, having no depression symptoms, and having only one chronic disease were associated with treatment nonadherence.
Conclusion: Treatment nonadherence for chronic diseases in Indonesia was found to be prevalent. Further consideration of characteristics associated with treatment nonadherence should be given to ensure optimal control of chronic diseases.
Keywords: chronic diseases, adherence, socioeconomic factors, patient-related factors, condition-related factors
Introduction
Chronic diseases have become a leading issue in healthcare in terms of morbidity and mortality globally.1 They can cause disturbances in physical and social functioning, quality of life, and the economic sustainability of the healthcare system.2,3 The impact is most notable in lower-middle-income countries (LMICs).1 Out of the 41 million deaths due to non-communicable diseases in 2019, 77% occurred in LMICs.1 These data are predicted to increase to 52 million by 2030, with 42 million occurring in LMICs.4
Indonesia is an LMIC that has a high burden of chronic diseases.5 Data demonstrated that chronic diseases caused 69.9% of lost disability-adjusted life years.6 Chronic diseases constitute the most significant proportion of the causes of death in Indonesia at 76%.7 The increased prevalence of chronic diseases in adolescents has further disrupted the quality of life and individual productivity and could affect economic aspects in the future.8 Other than that, chronic diseases compose the largest cost absorber in the national health insurance system, contributing to around 60% of its spending.8,9 The data highlighted that chronic diseases increase the healthcare burden and utilization of health services and medication in Indonesia.9
Treatment adherence is paramount in managing chronic diseases.10 It is defined as a process in which patients follow agreed-upon recommendations for prescribed treatment from a healthcare provider.10 As part of treatment adherence, regular medication is required for patients with chronic diseases that involve several phases, ie, the initiation, implementation, and continuation phases.11,12 In previous studies, treatment nonadherence was high among several types of chronic disease patients in Indonesia. A low level of treatment adherence was identified among 93.6% of hypertension patients, while 71% of diabetes mellitus (DM) patients did not receive regular treatments.13,14 In breast cancer patients, 21 of 50 cancer patients postponed the treatment after receiving the diagnosis, which led to treatment nonadherence.15 Several factors could explain this phenomenon, such as socioeconomic, health system/care team, therapy, condition, and patient-related factors.10
Problems related to treatment nonadherence among chronic diseases were identified in previous studies. Long duration and accessibility to health facilities are reported in chronic disease patients.16–18 Another study showed that being elderly, having depressive symptoms, and having low satisfaction with healthcare services were associated with low adherence to hypertension treatment.19 In diabetes mellitus (DM) patients, a study demonstrated that not having insurance coverage and older ages were associated with low awareness of DM treatment.20 Problems described in the previous studies highlighted that treatment nonadherence can worsen diseases, leading to disability, increased healthcare costs, and mortality.21,22
Therefore, current Indonesia’s national health insurance program—provided by Badan Penyelenggara Jaminan Sosial Kesehatan, or BPJS Kesehatan—has devised PROLANIS (Program Penanggulangan Penyakit Kronis) to mitigate the growing number of chronic disease patients in Indonesia.23 Despite the growing participant number of BPJS Kesehatan of up to 90.24% in 2022,24 studies of PROLANIS implementation indicated the program’s inadequacy in managing chronic diseases.25–27 This issue is worsened by the low coverage of private health insurance in Indonesia of only 33.4%,28 which all affects patients’ access to treatment.29
Analysis of dimensions to treatment adherence remains low in Indonesia, despite being known to affect treatment outcome of chronic disease patients.10 Identifying the prevalence and factors associated with treatment nonadherence in various chronic diseases can provide a comprehensive picture of the treatment nonadherence situation for developing strategies to control chronic diseases in Indonesia.10 We, therefore, seek to identify the prevalence of treatment nonadherence and analyze its characteristics in chronic disease patients in Indonesia.
Methods
Study Design and Setting
We conducted a cross-sectional study using the nationwide database of the fifth Indonesian Family Life Survey (IFLS-5; https://www.rand.org/well-being/social-and-behavioral-policy/data/FLS/IFLS.html). IFLS itself is a longitudinal project that, to date, has been conducted five times since its inception in 1993. IFLS-5, as its fifth wave, was fielded in late 2014 and early 2015.30 The national survey collected individual, household, and community data using multistage stratified sampling.30
The IFLS-5 data were collected from households living in 13 out of 27 Indonesian provinces, which represented approximately 80% of the Indonesian population.31 IFLS-5 employed stratified sampling on each of the provinces and its juridical subdivisions. This sampling strategy was employed to optimize population representation in terms of the cultural and socioeconomic diversity and cost-effectiveness of the survey, given Indonesian demographical and geographical characteristics.31
Random households were sampled from the resulting 321 enumeration areas (EAs) spread across the 13 provinces, with an oversampling for urban EAs and EAs in the smaller provinces to facilitate geographic and demographic comparisons. 20 and 30 households from urban and rural EAs respectively were sampled.31 The IFLS-5 collected sociodemographic, economic, and health status characteristics through a previously validated questionnaire to confirm its reliability and validity.31
Institutional Review Boards of the RAND Corporation in the United States and Universitas Gadjah Mada in Indonesia provided the ethical approval for the IFLS-5.31 Written informed consent was obtained from all subjects prior to the survey process.31 Therefore, additional ethical approval is not mandatory for this current study, noting the previous ethical approval of the IFLS-5 study and the anonymized nature of the data. We followed the guidelines outlined by Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) to provide a transparent and systematic report.32
Participants and Study Size
The IFLS-5 recorded subject’s self-report of diagnosis chronic diseases to the following classifications: hypertension, diabetes, tuberculosis, asthma, other lung diseases, cardiovascular diseases, liver diseases, stroke, cancers, arthritis, dyslipidemia, prostate diseases, kidney diseases, digestive diseases, psychiatric diseases, and memory-related diseases. These conditions were determined by the following question: “Has a doctor/paramedic/nurse/midwife ever told you that you had [types of chronic disease]?” (Book IIIB/CD05). Subjects who reported diagnosis to any of the diseases were classified as chronic disease patients.31
To obtain a representative association between subjects’ characteristics and treatment adherence, we excluded subjects aged < 15 years measured with a different instrument in the IFLS-5 (Book V). Therefore, we included all subjects aged > 15 years who reported receiving formal diagnosis of chronic disease. Subjects with missing data were further excluded from our analysis.
Variables and Measurement
Exposure Variables
The potential variables were selected from the IFLS-5 questionnaire based on the Multidimensional Adherence Model by the World Health Organization (WHO) in relation to individual patient conditions.10 Three dimensions were included for analysis: socioeconomic-, disease-, and patient-related conditions. These variables are further described as operational definitions in Table S1.31
Socioeconomic Factors
Socioeconomic factors are composed of information on sociodemographic characteristics, such as sex (male and female), age group (15 to 65 years and > 65 years), education (unschooled and schooled), ethnicity (Javanese and non-Javanese), geographical residence (Java and non-Java), demographical residence (urban and rural), household size (1, 2 to 6, and > 6 person), health insurance (insured and noninsured), and annual income (not working, < 12 to 14, 40 to 100, and > 100 million rupiah).
Patient-Related Factors
Patient-related factors were used to analyze the perception and expectation of subjects toward their health conditions, which were acquired to gain information about previous, present, and prospective health conditions. Data were yielded using three questions: (1) “In general, how is your health?” (2) “During the last 4 weeks, how many days of your primary daily activities did you miss due to poor health?” (3) “How do you expect your health to be in next year?”.31 Responses for (1) were classified into unhealthy and healthy. For (2), responses were classified into 0 to 7 days and > 7 days. Lastly, responses to (3) were classified into worse and about the same/better.
Disease-Related Factors
The condition-related factors included smoking behavior, depression symptoms, and the number of morbidities. Smoking behavior was categorized into ex-, non-, and active smokers. Depressive symptoms were assessed using the Centers for Epidemiologic Studies Depression Scale,33 where scores > 9 were classified as having depressive symptoms.33 Multimorbidity was categorized based on the number of chronic diseases reported by the subject.
Outcome Variables
The study outcome was determined by identifying treatment nonadherence by analyzing the treatment behavior of subjects, which were classified based on the available data in IFLS-5 as adherent and nonadherent subjects. This criterion was identified by the following survey question: “Are you now taking the following treatments to treat [types of chronic diseases] and its complications?” (Book III/CD09).31 Owing to the dependence of formal diagnosis in determining the subject’s chronic disease status, we assumed prescription to be an inherent part of the clinical process and subsequently classified those who reported receiving no treatment for their chronic diseases as nonadherent subjects. Therefore, in accordance with the IFLS-5 database,31 this study defined nonadherence as interruptions to treatment regimen within the persistence phase.11
Data Analysis
Descriptive analysis was used to summarize subjects’ characteristics, chronic disease proportions, and prevalence of treatment nonadherence. A chi-square test was performed to analyze the bivariate association between the exposure and outcome variables. A subsequent multivariable analysis included associated exposure variables with a p-value of < 0.25. The multivariable logistic regression with an entry method was used to identify factors associated with treatment adherence, with a p-value of < 0.05 as the threshold for association. The odds ratio (OR) with a 95% confidence interval (95% CI) was used to assess the magnitude of association between the exposure and outcome variables in the multivariable analysis. A Hosmer–Lemeshow test was used to validate the multivariable test result based on the goodness-of-fit statistics of the resulting R2 value.34 All statistical analyses were conducted using SPSS® Statistics version 22.35
Results
Participant Characteristics
In summary, 11,419 subjects with chronic diseases were included for further analysis, but we excluded 11 due to missing information. The final number of subjects for further analysis was 11,408. Figure 1 provides a flow diagram of the subjects.
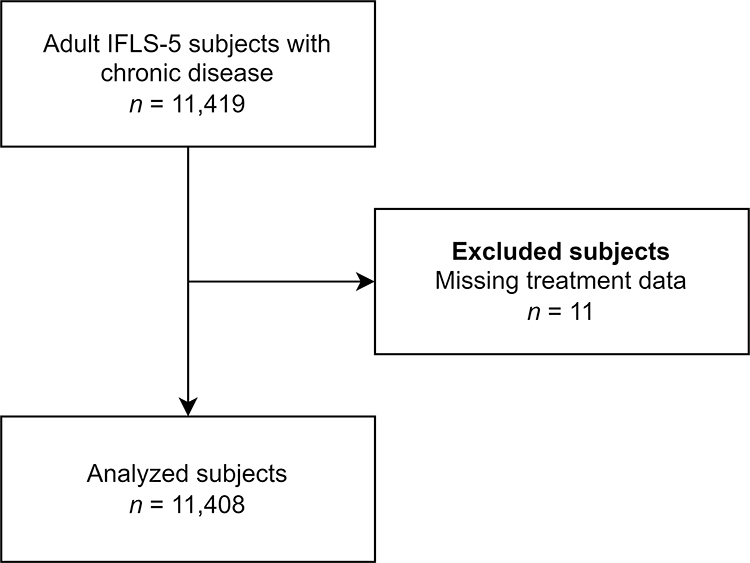 |
Figure 1 Flow Diagram of Subjects. |
Most of the included subjects were female (59.3%), aged 15 to 65 years (87.9%), and had a formal education background or were schooled (93.2%). Among the subjects, 35.1% were not working and 56.2% had an income of < 12 to 60 million rupiah per year. We found that 82.8% expected their health to be the same or better, 64.6% perceived they had a health condition, and 69.2% had one chronic disease. Missing data were identified in some variables with an acceptable percentage (< 10%).36 Hence, no specific approach was taken to manage the missing data. Table 1 depicts the characteristics of the subjects and the missing data.
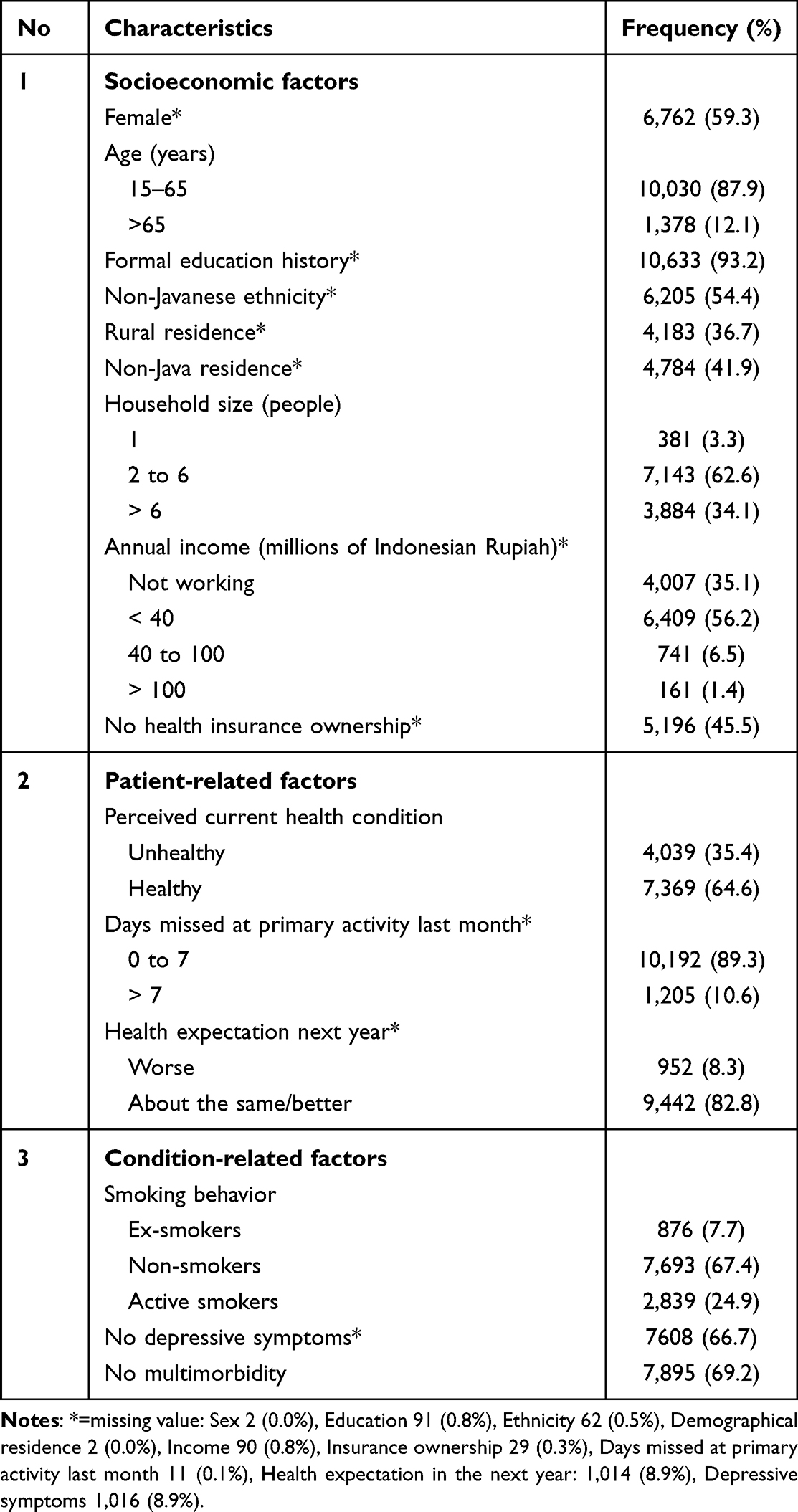 |
Table 1 Characteristic of Respondents with Chronic Diseases (n = 11,408) |
As illustrated in Figure 2, digestive diseases exhibited the highest prevalence (38.4%; 95% CI 37.5–39.3), followed by hypertension (36.9%; 95% CI 36–37.8), arthritis (15.2%; 95% CI 14.5–15.9), dyslipidemia (12.2%; 95% CI 11.6–12.8), asthma (8.8%; 95% CI 8.3–9.3), and diabetes (6.8%; 95% CI 6.3–7.3), whereas the lowest prevalence was noted for memory-related diseases (0.8%; 95% CI 0.6–0.9). Among these figures, 57% of all chronic disease patients were found to be nonadherent, with the highest proportion of nonadherence in liver diseases (61.8%) and the lowest in stroke (26.8%).
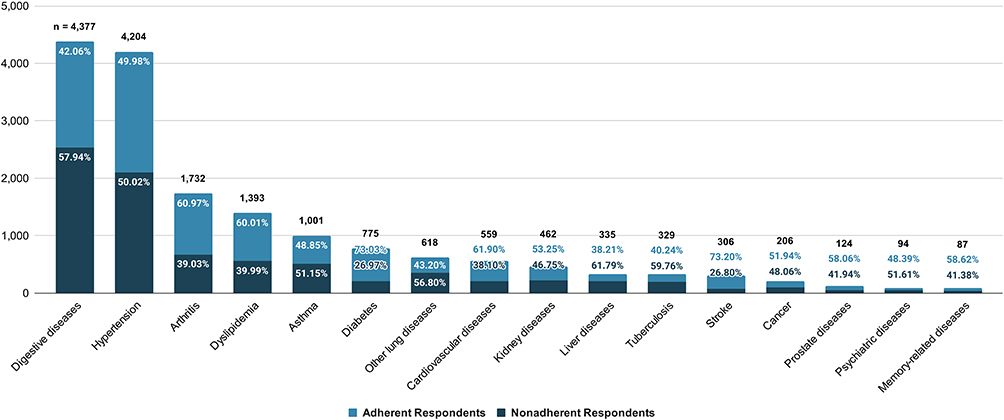 |
Figure 2 Proportion of Treatment Nonadherence across Chronic Diseases. |
Factors to Treatment Nonadherence
During the bivariate analysis, various factors, including sex, age, education, residential site, household size, income, health insurance, health condition, smoking behavior, depressive symptoms, and the number of morbidities, were found to have a p-value of ≤ 0.25. Consequently, these factors were incorporated into the multivariable model.
The results pointed to ten characteristics that are significantly associated with treatment nonadherence, such as age 15 to 65 years (OR 1.64; 95% CI 1.39–1.94; p < 0.001), schooled (OR 1.52; 95% CI 1.23–1.88; p < 0.001), living in rural areas (OR 1.12; 95% CI 1.03–1.23; p = 0.010), household size of 2–6 people (OR 1.11; 95% CI 1.02–1.22; p = 0.019), healthy condition (OR 1.57; 95% CI 1.43–1.73; p < 0.001), missed 0 to 7 days of regular activities in the last month (OR 1.61; 95% CI 1.38–1.89; p < 0.001), expecting health to be the same or better (OR 1.29; 95% CI 1.11–1.50; p = 0.001), nonsmoker (OR 1.41; 95% CI 1.16–1.70; p < 0.001), active smoker (OR 1.62; 95% CI 1.35–1.94; p < 0.001), without depressive symptoms (OR 1.11; 95% CI 1.01–1.22; p = 0.038), and without multimorbidity (OR 2.93; 95% CI 2.67–3.21; p < 0.001). Table 2 presents the bivariate and multivariable analyses.
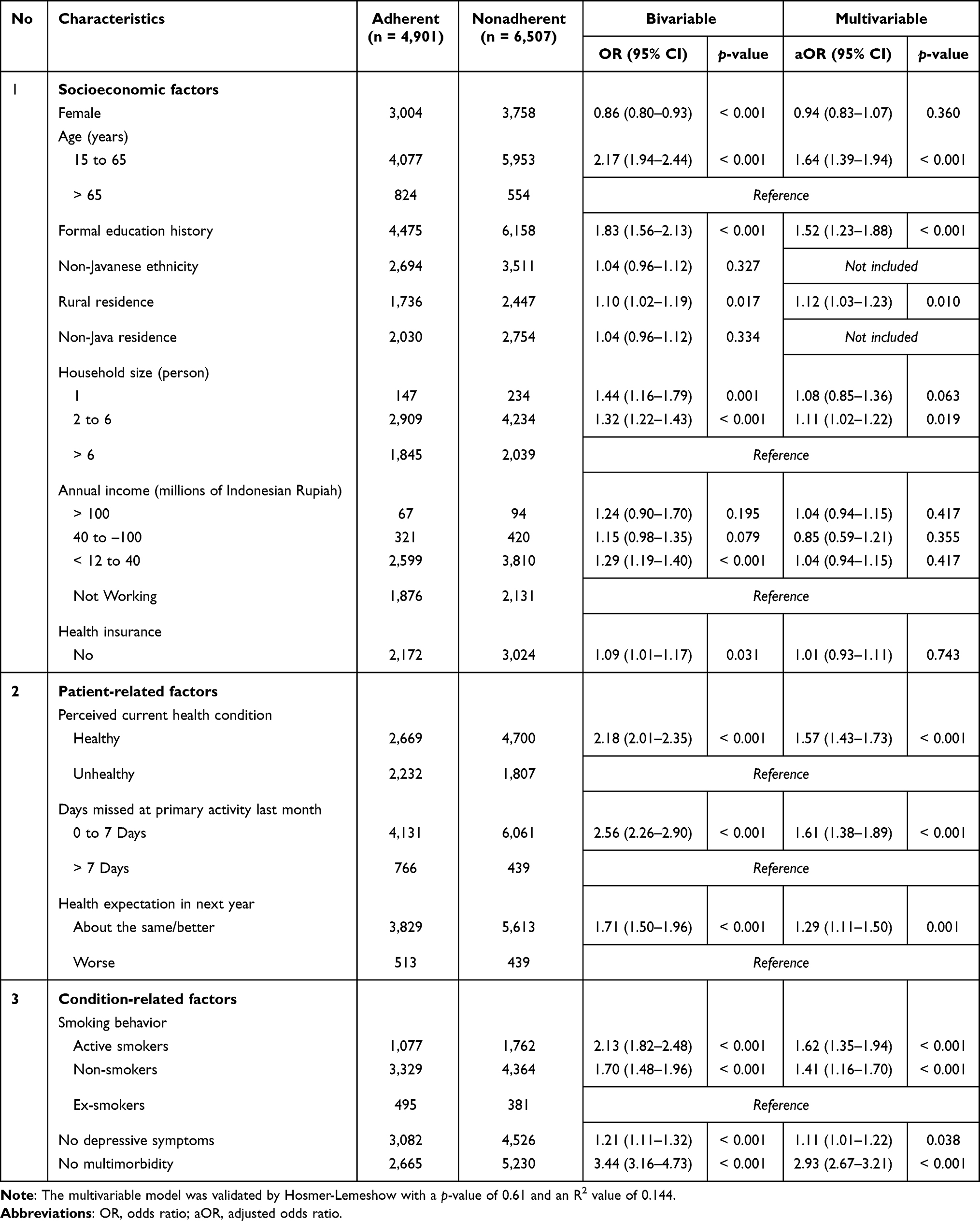 |
Table 2 Characteristics Associated with Nonadherence (n = 11,408) |
Discussion
This study demonstrated that cardiovascular problems and hypertension had the highest prevalence rates among chronic diseases. We also identified that nonadherence to treatment was high and was observed in all chronic diseases. The highest proportion of nonadherence was noted in subjects with liver, tuberculosis, and digestive problems. The socioeconomic characteristics of nonadherent subjects were identified in the group aged 15 to 65 years, had a formal education background, lived in rural areas, and had a household size of 2 to 6 people. In the patient- and condition-related factors, subjects with a positive perception of their health condition who missed 0 to 7 days of regular activities in the last month, ex- and nonsmokers, without depression symptoms, and with only one chronic disease were identified as the associated characteristics for treatment nonadherence.
The study demonstrated that 57% of patients with chronic diseases were nonadherent to treatment. This result was relatively consistent with that of the WHO report, which estimated that the adherence rate to long-term therapy for chronic diseases in LMICs was around 50%.10 Compared with high-income countries, the cases of pharmacological nonadherence in Spain and Japan were lower than those in Indonesia (48.8% and 17.7%, respectively).37,38 Similarly, a high nonadherence rate was found in Ghana (55.5%).39 This could be due to an inadequate healthcare system and inequality in access to healthcare in LMICs.4,10 Other than that, human resources, the availability of infrastructure and medical equipment, and medicines are still challenges in Indonesia.40 Despite the wide range of nonadherence rates across the countries, the main concern is that nonadherence remains a significant problem in the treatment of chronic diseases.41
The current study demonstrated that subjects aged 15 to 65 years are more likely to be nonadherent to treatment compared with those aged > 65 years. This result may be attributed to the lower severity of chronic diseases among younger patients compared to older ones.42 This finding leads to the increased potential of treatment nonadherence at a younger age due to the lower severity of diseases.42 This notion was also supported by the study finding that the group with a positive perception of their health condition and fewer days missing regular activities was less adherent to treatment than its comparators (Table 2).
The association between education status and nonadherence is inconsistent across other studies. Although previous studies demonstrated that high levels of education exerted a positive relationship with adherence,43,44 the current study found that subjects with formal educational backgrounds are significantly associated with treatment nonadherence. Nevertheless, our finding was supported by a previous study that reported low adherence among patients with high levels of education.45 However, another study found no significant association between adherence and health literature due to education levels.46 These different findings highlight the need for further studies to explain the association between education status and nonadherence to treatment.
The current study further identified that living in rural areas was associated with treatment nonadherence, which can be explained by issues with access to qualified healthcare services. This finding was supported by previous studies that stated that long distances from healthcare facilities and affordable medication influence treatment nonadherence.47–49
Regarding household size, previous studies demonstrated that having more family members and friends could provide social support for treatment adherence.41,50,51 In contrast, the current study found that having two to six family members was associated with treatment nonadherence compared with a household size of more than six. We inferred that the number of family members should not directly influence behavior toward adherence. Theoretically, the essential factors related to the household size that led to nonadherence were the lack of support from family members, irregular supervision, conflicts, low levels of education of parents, and family beliefs about the nature of illnesses.50,51
Importantly, we identified that the self-assessment of health conditions was associated with treatment nonadherence, especially for subjects who perceived themselves as healthy. This study underlined the link between adherence and the feeling of poor health conditions, which is in line with a systematic review that proposed that several factors can influence treatment nonadherence, such as asymptomatic diseases, clinical improvement, symptom reduction, and feeling better, whereas disease severity positively influenced adherence.50
Consistent with other studies, the current study found that subjects who smoked had the highest probability of treatment nonadherence. Previous studies identified that active smokers were more likely to be nonadherent to treatments for hypertension, asthma, and renal transplantation.41,50 However, in another group, we identified that nonsmokers are more likely to be nonadherent than ex-smokers. A possible explanation is that ex-smokers may have ceased smoking due to their chronic condition; hence, this group displays higher levels of awareness about their health conditions and treatment than nonsmokers. This result implies that nonsmokers are more likely to be nonadherent than ex-smokers.
In contrast with other studies, we analyzed that subjects without depressive symptoms and with only one chronic disease were associated with treatment nonadherence. In previous studies, depression and multimorbidity status were reported as factors that influence nonadherence to treatment.41,50,52 These conflicting results may be due to these groups’ health awareness levels. The positive effect of multimorbidity on adherence may be associated with the perception of the disease, such as a person with multi-comorbidities may perceive more severe conditions compared with a person with only a single disease.45,52,53 This tendency may also occur in those with depressive symptoms. The perception of severity can lead to high levels of health awareness and treatment adherence. However, these differences give room for further investigation of such issues. Hence, further studies are required to analyze these associations.
Strengths and Limitations
This study has several strengths. First, it is based on the IFLS survey, a large population-based study representing 83% of the Indonesian population. Second, we followed the STROBE guidelines in reporting for a systematic and transparent report.32 Third, we analyzed various types of chronic diseases to provide a comprehensive picture of chronic diseases in Indonesia. Fourth, we followed the conceptual framework of the WHO for data analysis that considers several strong determinants related to treatment nonadherence.10
Alternatively, several limitations should be acknowledged. First, the use of secondary data in this study limits the number of exposure factors potentially associated with the study outcome and the definitional settings of each variable. As such, our study did not include nonadherence on the initiation and implementation step of treatment regimen. Second, the self-reported questionnaires for measuring nonadherence may be prone to social desirability bias. Third, the cross-sectional design may limit the evaluation of causal relationships between the exposure and the outcome variables among subjects, as both were examined simultaneously.54
Implication for Policy and Practice
The findings echo the urgent need to reduce the prevalence of treatment nonadherence by improving adherence rates to treatments for chronic diseases. In general, the study highlights two significant points. First, chronic diseases influence all dimensions of people’s lives in Indonesia. Second, the majority of people with chronic diseases overlook the role of treatment in controlling chronic diseases, particularly NCDs. Given the threat posed by chronic diseases to public health and the economic development of countries,55 a comprehensive strategy with a high-level framework-based approach that would better serve a broad range of chronic conditions is needed to overcome these problems. Preventive interventions should be developed in the form of policies, structural, and behavioral strategies.56
From the results of our study, it was found that most of the predictors indicated that non-adherence to treatment was characterized by self-perceptions that they were in good health, causing them to think about not taking treatment and vice versa. The process of increasing patient’s treatment adherence must then shift their perception of illnesses, acting as a basis of their subsequent behavior.21 As patient’s belief is primarily determined by their knowledge, doctors, nurses, and pharmacists should provide an extensive information of their disease prognosis and treatment to improve their medication adherence.21 However, this practice is rarely carried out in Indonesia.57,58 Consequently, we emphasize the importance of counseling the patients as the first fundamental step to tackling the problem and empowering patients’ self-management.
Noting the multitude of factors influencing patient’s adherence, interventions for improving treatment adherence should be personalized according to patient’s needs.10,50,59,60 This notion underlines the need for collaborative healthcare practices among medical doctors, nurses, and pharmacists to manage individual problems of nonadherence among patients with chronic diseases. However, the involvement of healthcare professionals in patient education is still lacking due to limited knowledge, limited human resources, time constraints, and the burden of administration.57
Therefore, we also highlight the importance of accessibility to qualified health services to provide patients the knowledge needed in managing their chronic diseases and treatments.61 Healthcare professional should engage in managing patient’s treatment adherence.21 Hence, it is necessary to educate and train healthcare professionals and adjust their workload and number to improve the management of chronic diseases.
Conclusion
Treatment nonadherence among patients with chronic diseases continues to be a challenge in Indonesia. The high rate of treatment nonadherence among chronic disease patients emphasized the need for a patient-centered care in adherence management. Considerable attention should be given to younger patients aged with a lower severity of the chronic disease, living in a rural areas, having positive health perception, and are active or nonsmokers. No one-size-fits-all intervention exists; thus, targeted and tailored interventions should be developed to improve treatment nonadherence. In efforts to improve adherence management, further studies need to develop and utilize a more comprehensive assessment instruments in gathering further data on medication nonadherence subtypes and its associated factors.
Data Sharing Statement
The IFLS-5 dataset analyzed for this study can be found at https://www.rand.org/well-being/social-and-behavioral-policy/data/FLS/IFLS/access.html.
Ethical Statements
No ethical approval is needed in this study since this is a database study using a public database with anonymous data. However, all activities followed the ethical principles in the Declaration of Helsinki. The fifth Indonesian Family Life Survey has obtained ethical approval from the Institutional Review Boards of RAND Corporation in the United States and Universitas Gadjah Mada in Indonesia. Consent for participation was handled by the conducting parties.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by internal funding from Universitas Padjadjaran. The funder had neither role nor influence in the development and analysis of this study. The IFLS-5 project received funding from the National Institute of Aging (NIA), grant 2R01 AG26676; the National Institute for Child Health and Human Development (NICHD), grant 2R01 HD050764-05A1; World Bank, Indonesia and GRM International; and the Department of Foreign Affairs and Trade, Government of Australia.
Disclosure
All authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
REFERENCE
1. World Health Organization. Noncommunicable diseases. 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
2. Bernell S, Howard SW. Use your words carefully: what is a chronic disease? Front Public Health. 2016;4. doi:10.3389/fpubh.2016.00159
3. Bloom DE, Cafiero ET, Jané-Llopis E, et al. The global economic burden of non-communicable diseases. World Economic Forum; 2011. Available from: https://www3.weforum.org/docs/WEF_Harvard_HE_GlobalEconomicBurdenNonCommunicableDiseases_2011.pdf.
4. Arokiasamy P, Uttamacharya, Kowal P, et al. Chronic noncommunicable diseases in 6 low- and middle-income countries: findings From wave 1 of the World Health Organization’s Study on Global Ageing and Adult Health (SAGE). American Journal of Epidemiology. 2017;185(6):414–428. doi:10.1093/aje/kww125
5. Mboi N, Murty Surbakti I, Trihandini I, et al. On the road to universal health care in Indonesia, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392(10147):581–591. doi:10.1016/S0140-6736(18)30595-6
6. Ditjen Pencegahan dan Pengendalian Penyakit. Rencana Aksi Program Tahun 2020–2024. Kementerian Kesehatan Republik Indonesia; 2020. Indonesian. Available from: https://e-renggar.kemkes.go.id/file_performance/1-029017-2tahunan-218.pdf.
7. The World Bank. Cause of death, by non-communicable diseases (% of total) – Indonesia; 2019. Available from: https://data.worldbank.org/indicator/SH.DTH.NCOM.ZS?end=2019&locations=ID&start=2000&view=chart.
8. Kementerian Kesehatan Republik Indonesia. Penyakit Tidak Menular Kini Ancam Usia Muda; 2020. Indonesian. Available from: https://www.kemkes.go.id/article/view/20070400003/penyakit-tidak-menular-kini-ancam-usia-muda.html.
9. Marthias T, Anindya K, Ng N, et al. Impact of non-communicable disease multimorbidity on health service use, catastrophic health expenditure and productivity loss in Indonesia: a population-based panel data analysis study. BMJ Open. 2021;11(2):e041870. doi:10.1136/bmjopen-2020-041870
10. Sabaté E, World Health Organization, eds.. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
11. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Brit J Clinical Pharma. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
12. Alfian SD. Adherence to Antihypertensive or Antihyperlipidemic Co-Medications in Diabetes: Patterns, Predictors, and Intervention. University of Groningen; 2020. doi:10.33612/diss.135922731.
13. Kaaffah S, Soewondo P, Riyadina W, Renaldi FS, Sauriasari R. Adherence to treatment and glycemic control in patients with type 2 diabetes mellitus: a 4-year follow-up PTM Bogor Cohort Study, Indonesia. PPA. 2021;15:2467–2477. doi:10.2147/PPA.S318790
14. Puspitasari IM, Azizah LN, Sinuraya RK, Alfian SD, Abdulah R. Measuring medication adherence of hypertensive patients with monotherapy treatment in a community health center by utilizing medication possession ratio. PHAR. 2022;69(2):345–350. doi:10.3897/pharmacia.69.e82330
15. Iskandarsyah A, de Klerk C, Suardi DR, Sadarjoen SS, Passchier J. Consulting a traditional healer and negative illness perceptions are associated with non-adherence to treatment in Indonesian women with breast cancer: non-adherence to treatment in Indonesian women with breast cancer. Psycho-Oncology. 2014;23(10):1118–1124. doi:10.1002/pon.3534
16. Alfian SD, Worawutputtapong P, Schuiling-Veninga CCM, et al. Pharmacy-based predictors of non-persistence with and non-adherence to statin treatment among patients on oral diabetes medication in the Netherlands. Curr Med Res Opin. 2018;34(6):1013–1019. doi:10.1080/03007995.2017.1417242
17. Pradipta IS, Idrus LR, Probandari A, et al. Barriers to optimal tuberculosis treatment services at Community Health Centers: a qualitative study from a high prevalent tuberculosis country. Front Pharmacol. 2022;13:857783. doi:10.3389/fphar.2022.857783
18. Pradipta IS, Idrus LR, Probandari A, et al. Barriers and strategies to successful tuberculosis treatment in a high-burden tuberculosis setting: a qualitative study from the patient’s perspective. BMC Public Health. 2021;21(1):1903. doi:10.1186/s12889-021-12005-y
19. Khoiry QA, Alfian SD, Abdulah R. Modifiable and non-modifiable factors associated with low awareness of hypertension treatment in Indonesia: a cross-sectional population-based national survey. Global Heart. 2022;17(1):56. doi:10.5334/gh.1143
20. Khoiry QA, Alfian SD, Abdulah R. Sociodemographic and behavioural risk factors associated with low awareness of diabetes mellitus medication in Indonesia: findings from the Indonesian Family Life Survey (IFLS-5). Front Public Health. 2023;11:1072085. doi:10.3389/fpubh.2023.1072085
21. Jüngst C, Gräber S, Simons S, Wedemeyer H, Lammert F. Medication adherence among patients with chronic diseases: a survey-based study in pharmacies. QJM. 2019;112(7):505–512. doi:10.1093/qjmed/hcz058
22. Raghupathi W, Raghupathi V. An empirical study of chronic diseases in the United States: a visual analytics approach to public health. IJERPH. 2018;15(3):431. doi:10.3390/ijerph15030431
23. World Health Organization, Organisation for Economic Cooperation and Development, Nappoe SA, Djasri H, Kurniawan MF. Chronic Disease Management Programme (PROLANIS) in Indonesia: case study. World Health Organization; 2023. https://iris.who.int/handle/10665/373226.
24. Dewan Jaminan Sosial Nasional, Badan Penyelenggara Jaminan Sosial Kesehatan, United States Agency for International Development. Statistik JKN 2016-2021. Dewan Jaminan Sosial Nasional; 2022. Available from: https://djsn.go.id/files/dokumen/Dokumen%20Kajian/202212131425Buku%20Statistik%20JKN%202016-2021.pdf.
25. Rachmawati S, Prihhastuti-Puspitasari H, Zairina E. The implementation of a chronic disease management program (Prolanis) in Indonesia: a literature review. J Basic Clin Physiol Pharmacol. 2019;30(6):20190350. doi:10.1515/jbcpp-2019-0350
26. Alkaff FF, Sukmajaya WP, Intan RE, Salamah S. Effectivity of Indonesia Chronic Disease Management Program (PROLANIS) to control hypertension and its comorbidities at primary health care: effectivity of PROLANIS to control hypertension. Open Access Maced J Med Sci. 2020;8(E):224–227. doi:10.3889/oamjms.2020.4583
27. Alkaff FF, Illavi F, Salamah S, et al. The impact of the Indonesian Chronic Disease Management Program (PROLANIS) on metabolic control and renal function of type 2 diabetes mellitus patients in primary care setting. J Prim Care Community Health. 2021;12:215013272098440. doi:10.1177/2150132720984409
28. Standard Insights. Leading insurance owned by people in Indonesia in 2022, by type. Published online 2022. Available from: https://www-statista-com.unpad.idm.oclc.org/statistics/1338308/indonesia-popular-type-of-insurance-owned-by-people/.
29. Arviana ME, Hafidz F, Setiyaningsih H, et al. The relationship between health insurance ownership and health service utilization, out-of-pocket expenses, and catastrophic health expenditure in the Special Region of Yogyakarta in 2023. In: Sato H, El Wahed AA, Frutos R, editors. BIO Web Conf. 2024. Vol. 132:04002. doi:10.1051/bioconf/202413204002
30. Strauss J, Witoelar F, Sikoki B. User’s Guide for the Indonesia Family Life Survey, Wave 5: Volume 2. RAND Corporation; 2016. doi:10.7249/WR1143.2
31. Strauss J, Witoelar F, Sikoki B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report: Volume 1. RAND Corporation; 2016. doi:10.7249/WR1143.1
32. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
33. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. 1994;10(2):77–84. doi:10.1016/S0749-3797(18)30622-6
34. Dodge Y. The Concise Encyclopedia of Statistics. Springer; 2010.
35. IBM Corporation. IBM SPSS Statistics for Windows. Published online 2013.
36. Madley-Dowd P, Hughes R, Tilling K, Heron J. The proportion of missing data should not be used to guide decisions on multiple imputation. J Clin Epidemiol. 2019;110:63–73. doi:10.1016/j.jclinepi.2019.02.016
37. Llorca CVY, Cortés Castell E, Ribera Casado JM, et al. Factors associated with non-adherence to drugs in patients with chronic diseases who go to pharmacies in Spain. IJERPH. 2021;18(8):4308. doi:10.3390/ijerph18084308
38. Suzuki T, Shiga T, Omori H, Tatsumi F, Nishimura K, Hagiwara N. Self-reported non-adherence to medication in Japanese patients with cardiovascular diseases. Am J Cardiovasc Drugs. 2018;18(4):311–316. doi:10.1007/s40256-018-0278-z
39. Addo B, Sencherey S, Babayara MNK. Medication noncompliance among patients with chronic diseases attending a primary health facility in a Periurban District in Ghana. Int J Chronic Dis. 2018;2018:1–10. doi:10.1155/2018/7187284
40. Wulandari RD, Laksono AD, Nantabah ZK, Rohmah N, Zuardin Z. Hospital utilization in Indonesia in 2018: do urban–rural disparities exist? BMC Health Serv Res. 2022;22(1):491. doi:10.1186/s12913-022-07896-5
41. Li SC. Factors affecting therapeutic compliance: a review from the patient’s perspective. TCRM. 2008;4:269–286. doi:10.2147/TCRM.S1458
42. Fernandez-Lazaro CI, Adams DP, Fernandez-Lazaro D, Garcia-González JM, Caballero-Garcia A, Miron-Canelo JA. Medication adherence and barriers among low-income, uninsured patients with multiple chronic conditions. Res Social Administrative Pharm. 2019;15(6):744–753. doi:10.1016/j.sapharm.2018.09.006
43. Chauke GD, Nakwafila O, Chibi B, Sartorius B, Mashamba-Thompson T. Factors influencing poor medication adherence amongst patients with chronic disease in low-and-middle-income countries: a systematic scoping review. Heliyon. 2022;8(6):e09716. doi:10.1016/j.heliyon.2022.e09716
44. Gast A, Mathes T. Medication adherence influencing factors—an (updated) overview of systematic reviews. Syst Rev. 2019;8(1):112. doi:10.1186/s13643-019-1014-8
45. AlHewiti A. Adherence to long-term therapies and beliefs about medications. Int J Fam Med. 2014;2014:1–8. doi:10.1155/2014/479596
46. Sawkin MT, Deppe SJ, Thelen J, Stoner SC, Dietz CA, Rasu RS. Health literacy and medication adherence among patients treated in a free health clinic: a pilot study. Health Services Res Manag Epidemiol. 2015;2:233339281558909. doi:10.1177/2333392815589094
47. Martin MY, Kim Y, Kratt P, et al. Medication adherence among rural, low-income hypertensive adults: a randomized trial of a multimedia community-based intervention. Am J Health Promot. 2011;25(6):372–378. doi:10.4278/ajhp.090123-QUAN-26
48. Rahmawati R, Bajorek B. Access to medicines for hypertension: a survey in rural Yogyakarta province, Indonesia. RRH. 2018. doi:10.22605/RRH4393
49. Xu J, Zhao M, Vrosgou A, et al. Barriers to medication adherence in a rural-urban dual economy: a multi-stakeholder qualitative study. BMC Health Serv Res. 2021;21(1):799. doi:10.1186/s12913-021-06789-3
50. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4. doi:10.3389/fphar.2013.00091
51. Krueger KP, Berger BA, Felkey B. Medication adherence and persistence: a comprehensive review. Adv Ther. 2005;22(4):313–356. doi:10.1007/BF02850081
52. Cheen MHH, Tan YZ, Oh LF, Wee HL, Thumboo J. Prevalence of and factors associated with primary medication non‐adherence in chronic disease: a systematic review and meta‐analysis. Int J Clin Pract. 2019;73(6):e13350. doi:10.1111/ijcp.13350
53. Pagès-Puigdemont N, Mangues MA, Masip M, et al. Patients’ perspective of medication adherence in chronic conditions: a qualitative study. Adv Ther. 2016;33(10):1740–1754. doi:10.1007/s12325-016-0394-6
54. Di Girolamo N, Mans C. Research study design. Fowler’s Zoo Wild Animal Med Curr Ther. 2019;9:59–62. doi:10.1016/B978-0-323-55228-8.00011-4
55. Schröders J, Wall S, Hakimi M, et al. How is Indonesia coping with its epidemic of chronic noncommunicable diseases? A systematic review with meta-analysis. PLoS One. 2017;12(6):e0179186. doi:10.1371/journal.pone.0179186
56. Christian H, Trapp G, Villanueva K, Pikora T. Chronic disease prevention interventions in children and young adults: a rapid review of evidence. Australian Prevention Partnership Centre; 2016. Available from: https://preventioncentre.org.au/wp-content/uploads/2021/10/1604_DoH-review_21April_final.pdf.
57. Presley B, Groot W, Pavlova M. Pharmacists’ and patients’ perceptions about the importance of pharmacist services types to improve medication adherence among patients with diabetes in Indonesia. BMC Health Serv Res. 2021;21(1):1227. doi:10.1186/s12913-021-07242-1
58. Puspitasari HP, Aslani P, Krass I. Challenges in the management of chronic noncommunicable diseases by Indonesian community pharmacists. Pharm Pract. 2015;13(3):578. doi:10.18549/PharmPract.2015.03.578
59. Alfian SD, Van Boven JFM, Abdulah R, Sukandar H, Denig P, Hak E. Effectiveness of a targeted and tailored pharmacist‐led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: a cluster randomised controlled trial. Brit J Clinical Pharma. 2021;87(4):2032–2042. doi:10.1111/bcp.14610
60. Ridho A, Alfian SD, Van Boven JFM, et al. Digital health technologies to improve medication adherence and treatment outcomes in patients with tuberculosis: systematic review of randomized controlled trials. J Med Internet Res. 2022;24(2):e33062. doi:10.2196/33062
61. Pradipta IS, Aprilio K, Febriyanti RM, et al. Traditional medicine users in a treated chronic disease population: a cross-sectional study in Indonesia. BMC Complement Med Ther. 2023;23(1):120. doi:10.1186/s12906-023-03947-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.