Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
How do general practitioners implement decision-making regarding COPD patients with exacerbations? An international focus group study
Authors Laue J, Melbye H ![]() , Halvorsen PA, Andreeva EA, Godycki-Cwirko M, Wollny A, Francis NA, Spigt M, Kung K, Risør MB
, Halvorsen PA, Andreeva EA, Godycki-Cwirko M, Wollny A, Francis NA, Spigt M, Kung K, Risør MB
Received 3 August 2016
Accepted for publication 20 October 2016
Published 8 December 2016 Volume 2016:11(1) Pages 3109—3119
DOI https://doi.org/10.2147/COPD.S118856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Johanna Laue,1 Hasse Melbye,1 Peder A Halvorsen,1 Elena A Andreeva,2 Maciek Godycki-Cwirko,3 Anja Wollny,4 Nick A Francis,5 Mark Spigt,6 Kenny Kung,7 Mette Bech Risør1
1Department of Community Medicine, General Practice Research Unit, University of Tromsø – The Arctic University of Norway, Tromsø, Norway; 2Department of Family Medicine, Northern State Medical University, Arkhangelsk, Russia; 3Department of Family and Community Medicine, Medical University of Lodz, Lodz, Poland; 4Institute of General Practice, University Medical Center Rostock, Rostock, Germany; 5Cochrane Institute of Primary Care and Public Health, School of Medicine, Cardiff University, Cardiff, UK; 6CAPHRI School for Public Health and Primary Care, Maastricht University, Maastricht, the Netherlands; 7The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong
Purpose: To explore the decision-making of general practitioners (GPs) concerning treatment with antibiotics and/or oral corticosteroids and hospitalization for COPD patients with exacerbations.
Methods: Thematic analysis of seven focus groups with 53 GPs from urban and rural areas in Norway, Germany, Wales, Poland, Russia, the Netherlands, and Hong Kong.
Results: Four main themes were identified. 1) Dealing with medical uncertainty: the GPs aimed to make clear medical decisions and avoid unnecessary prescriptions and hospitalizations, yet this was challenged by uncertainty regarding the severity of the exacerbations and concerns about overlooking comorbidities. 2) Knowing the patient: contextual knowledge about the individual patient provided a supplementary framework to biomedical knowledge, allowing for more differentiated decision-making. 3) Balancing the patients’ perspective: the GPs considered patients’ experiential knowledge about their own body and illness as valuable in assisting their decision-making, yet felt that dealing with disagreements between their own and their patients’ perceptions concerning the need for treatment or hospitalization could be difficult. 4) Outpatient support and collaboration: both formal and informal caregivers and organizational aspects of the health systems influenced the decision-making, particularly in terms of mitigating potentially severe consequences of “wrong decisions” and concerning the negotiation of responsibilities.
Conclusion: Fear of overlooking severe comorbidity and of further deteriorating symptoms emerged as a main driver of GPs’ management decisions. GPs consider a holistic understanding of illness and the patients’ own judgment crucial to making reasonable decisions under medical uncertainty. Moreover, GPs’ decisions depend on the availability and reliability of other formal and informal carers, and the health care systems’ organizational and cultural code of conduct. Strengthening the collaboration between GPs, other outpatient care facilities and the patients’ social network can ensure ongoing monitoring and prompt intervention if necessary and may help to improve primary care for COPD patients with exacerbations.
Keywords: COPD exacerbation, antibiotics, oral corticosteroids, hospitalization, primary care, decision-making
Introduction
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) account for the accelerated decline of lung function, loss of health-related quality of life, high morbidity, mortality, and health costs.1 It is estimated that hospitalizations due to COPD exacerbations account for 50%–75% of total health costs in the US and Europe.2 A key policy objective in many countries is to reduce costly hospitalizations, which can be achieved by prevention of exacerbations and early and optimal therapy in primary care.3 Due to their role as gatekeepers to secondary care in many countries, general practitioner (GP)s’ initial assessment and decision-making are key to determine the most appropriate treatment and in terms of treatment setting (primary or secondary care).4 Even though >80% of AECOPD can be managed in an outpatient setting, high hospitalization rates compose a major concern in COPD care.5 Current outpatient treatments are typically short courses of antibiotics and/or oral corticosteroids.5 There are great variations in prescribing, with antibiotics being usually prescribed more often than oral corticosteroids. Clinical findings, such as purulent sputum, chest findings, high C-reactive protein (CRP) and lung function impairment, as well as the exacerbation’s severity and number of previous exacerbations have been found to be predictors of treatment with antibiotics and oral corticosteroids.6–12 However, the therapeutic benefit from antibiotics and oral corticosteroids for outpatients is inconclusive13,14 and the symptom-based treatment criteria in COPD guidelines might be little helpful for GPs to base their treatment decisions on.15 Indeed, GPs can find the management of patients with AECOPD challenging, mostly due to the clinical complexity of multiple comorbidities and the patients’ social context.16 Moreover, as in other illness contexts, their prescribing and hospitalization decisions may be complicated or influenced by time constraints, aspects of the patient–physician relationship, availability of resources, and organization of health care systems.17–19 However, there is a lack of more specific insights into the GPs’ perspective on decision-making regarding COPD patients with exacerbations. Therefore, this study aimed to explore GPs’ accounts for their decision-making about treatment with antibiotics and/or oral corticosteroids and hospitalization for COPD patients with exacerbations.
Methods
Design and methodological considerations
This study is inspired by a naturalistic approach to decision-making, according to which decision-making under “everyday life” conditions – that are situated in a particular context and are often affected by contingencies – cannot be predicted or improved by formal models and normative rules.20,21 It addresses the disparity between idealized standards of care and variations in care that are not always meeting these standards,22 and draws on the understanding that GPs’ management decisions – even though sometimes appearing “irrational” or “inappropriate” from a biomedical, economical, or public health perspective – are rational in the process of caring for a particular patient in a particular situation.23
The study forms part of a cross-national grounded theory study using focus group discussions (FGDs).16 FGD can be particularly useful in exploring “what people think, how they think, and why they think that way”,24 which is why this method should be suitable for identifying reasoning patterns that shape GPs’ decision-making. The group interaction characteristic of this interview form can stimulate and unravel opinions, which are less accessible in individual interviews, and gives the participants the opportunity to define themselves related to what is relevant or important within the topic of interest.24 Contrary to the study of Risør et al,16 we based our study on the FGDs with GPs only. The results of this study indicate that there are differences in how GPs and pulmonary physicians approach decision-making. Overall, GPs typically deal with less severely ill patients than pulmonary specialists, and treatment with antibiotics and/or oral corticosteroids may often be less necessary for COPD patients in primary care.13,14 Therefore, we considered it important to explore the GPs’ perspective in particular.
Sampling and material
The overall study design and data collection is described comprehensively in a previously published paper.16 Briefly, this study is based on seven FGDs with a total of 53 GPs in six European countries (the Netherlands, Russia, Norway, Germany, Poland, and Wales) and China (Hong Kong), which were sampled purposefully through personal contacts of the researchers and professional networks in each country. The sample aimed for and covered urban and rural practices (Table 1). The FGDs were conducted in native language in March 2011. Moderators were head researchers from each country’s network (a professor or doctor in family medicine), except for one case that was moderated by a PhD student and an epidemiologist. All moderators underwent training in the FGD method. The same interview guide, collaboratively developed by the initiators of the overall research project PEXACO,16 was used in all FGDs. Topics comprised assessment and medication, hospitalization, use of guidelines, challenging or difficult situations, most important problem, self-treatment, smoking cessation, and improvement of clinical practice (some topics served as data for other studies).16,25 The interview guide included two patient cases to prompt discussions on the first two topics (Supplementary material). The FGDs were transcribed verbatim from audio recordings by local researchers and translated into English. The research team maintained communication throughout the whole research process to resolve any issues concerning the interpretation of country-specific content in the FGDs.
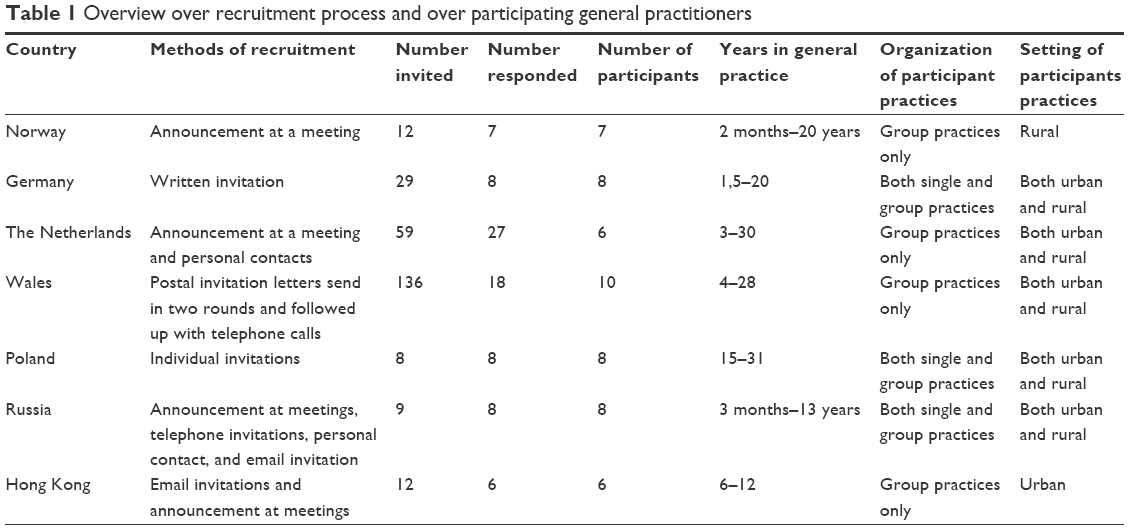 | Table 1 Overview over recruitment process and over participating general practitioners |
Ethical approval was obtained from the appropriate bodies in the participating countries (Norway: Regional Ethical Committee, Norwegian Social Science Data Services; Germany: Ethical guidelines of the University of Rostock, according to these guidelines ethical approval is not needed for interviews with professionals; the Netherlands: Ethical review board of Maastricht University Hospital/Maastricht University; Wales: South East Wales Research Ethics Committee Panel C; Poland: Bioethical Commission of Medical University of Lodz; Russia: Ethics review board of the Northern State Medical University, Arkhangelsk; Hong Kong: Chinese University of Hong Kong). The participants gave written informed consent and received a financial reimbursement (funded by the PEXACO project) for participation. Before the transcriptions were distributed in the research group, identifiers were removed.
Analysis
We employed thematic analysis as described by Braun and Clarke,26 which offers a stepwise method for analyzing qualitative data. Thematic analysis in this version is independent of specific theoretical frameworks and may be used flexibly and actively addressing the chosen design of a project, while still providing a sound methodological and theoretical approach. Apart from our overall interpretive framework and assumption that data is situated and relational, we depart from a data-driven, inductive, and semantic approach to the analysis without applying specific theories but still interpreting patterns and their broader meanings in relation to theory or relevant literature.26 NVivo 10 data analysis software27 and Mindjet MindManager Professional28 were used as tools to organize the transcripts, codes, memos, and relationships between them, and to visualize our findings. First, all transcripts were read by JL and MBR, and then initially coded by JL. Subsequently, codes were organized and developed to preliminary themes and subthemes, comprising the role of clinical findings and their interpretation, medical uncertainty, and decision-making as a collaborative process. Their further development into final themes was based on literature reading, ongoing reflections, and discussions between JL, MBR, and HM. During the whole data analysis, codes and themes were constantly tested by moving between the data, codes, and visual theme maps to ensure that they represented the meanings found in the data. Any disagreements were resolved through discussions between the authors.
Results
We identified four main themes in the GPs’ accounts for their decision-making: dealing with medical uncertainty, knowing the patient, balancing the patients’ perspective, and outpatient support and collaboration.
Dealing with medical uncertainty
The GPs emphasized that, in order to make a medically accountable decision, sufficient clinical information, for example, medical history and clinical investigation was necessary.
History is important, obviously, if you have got increased breathlessness, increased sputum production, particularly, if its mucopurulent, if they are feeling unwell, and then you would want to do an examination and then you can see if they have got any signs of respiratory distress above what they normally have and if there are any signs of pneumonia, any signs of infection, and then treat appropriately. That’s the sort of way I would manage it. [GP, Wales]
In terms of antibiotics, colored sputum, fever, and high CRP levels appeared particularly relevant. For oral corticosteroids, the GPs emphasized (severe) dyspnea and certain lungs sounds (“wheezing,” “whirring,” or “whimpering”). Particularly important regarding hospitalization were clinical findings such as cyanosis, edema, or low oxygen saturation, but also the impression that a patient was seriously ill.
But we can look at it in 2–3 days. If he will be evidently short of breath, with cyanosis, with symptoms of such a serious exacerbation, then there is no joking, he will go to the hospital. [GP, Poland]
Yet, even though decision-making seemed straightforward in the presence of certain symptoms and clinical findings, the discussions revealed that these theoretically decisive signs could lose their diagnostic relevance in the context of chronic and comorbid illness.
I think it’s difficult because a lot of these patients do have chronic [illness], their sputum is chronically um – there is all sorts of bacteria – it is difficult to be guided by things such as sputum culture because it’s often going to come back as positive whether or not it’s acute […]. [GP, Wales]
Indeed, GPs seemed considerably concerned that symptoms and clinical signs were often diffuse, and some GPs’ mentioned that limited access to diagnostic tests such as blood gas analysis, CRP, or pulse oximetry also reduced the possibility of making a certain diagnosis.
Overall, making medically “correct” decisions was challenging when those in need of antibiotics, oral corticosteroids, or hospitalizations could not be identified with certainty based on symptoms, clinical findings, or diagnostic tests. This could make it difficult to balance the benefits and harms of a management option.
See if we knew if it was bacterial or you knew that it wasn’t bacterial then you wouldn’t have to start the antibiotics and start worrying about the warfarin and that it is going to mess up the diabetes and all the rest of it. So, if you did have some diagnostic certainty it would not create all these other problems and exacerbate their other conditions. [GP, Wales]
Even though there were some concerns related to unnecessary prescribing, such as pharmacological interactions and eventually an increased workload, the GPs’ overall attitude to treatment was rather precautionary. Such a “better safe than sorry” approach seemed associated with their understanding that COPD patients tend to be vulnerable due to advanced age and comorbidities, and, consequently, at high risk for infections and further deterioration. This added a certain sense of urgency to the decision-making.
Usually, we should be concerned whether there is an infective component when we prescribe steroids. Usually, chronic COPD patients are weak and if we prescribe steroids for them, will it be easy for them to get infections and often I will prescribe antibiotics as daily practice. [GP, Hong Kong]
In addition to such rather rational risk assessment, there was a clear emotional component in the GPs’ narrations. Particularly, worries about having overlooked a severe illness, mostly heart diseases, could be worrisome and were associated with unpleasant feelings of regret subsequent to having been too restrictive with treatment or hospitalization.
I would say that, well, the worst cases I remember are the ones when I didn’t send the people to the hospital – when I couldn’t stop thinking about these patients and was like “Oooh, how is it going with them?”, I experienced sometimes that I had too high a threshold for hospitalizing people, […]. [GP, Norway]
Both such memories from individual cases and the rather analytical, epidemiological contemplation of risk factors associated with COPD seemed to contribute to an understanding of COPD patients as vulnerable patients. In the light of diagnostic and prognostic uncertainty, the GPs’ decision-making for a patient belonging to this patient group seemed characterized by an overall sense of alertness and precaution to take any risks regarding treatment and hospitalization.
Knowing the patient
Since deciphering the biomedical meaning of symptoms and clinical findings could be difficult, the GPs emphasized that knowing their patients was essential for reasonable decisions.
I just wanted to say. Now we talk a lot, but if you know him, then you know whether he already had something like this in the past? Do you have the case history, is he compliant? Does he take his medication? Or not? [GP, Germany]
Such knowledge acquired through their role as family doctors, comprised both clinical and more personal aspects. In terms of clinical knowledge, familiarity with a patient’s appearance during a stable state and previous exacerbations helped the GPs for instance to make initial, intuitive judgments regarding their patients’ overall condition, and to determine the direction of the further assessment.
It’s easier in a face to face consultation, you can judge it much better. Especially when you know them and if they walk the corridor to your room you can tell how good or bad they are. [GP, Wales]
Such initial judgments were particularly relevant regarding hospitalizations, as they could either increase or decrease the perceived risk of further deterioration, eventually triggering immediate hospitalization. It could also create a sense of comfort that they were able to manage the patient in an outpatient setting. Moreover, knowing the patient’s medical history, comorbidities, and maintenance treatment, as well as the outcome of previous treatment for a similar condition, and how effectively, could reduce uncertainty and enable straightforward decision-making.
Previous history, that is, the last exacerbation was very severe and required hospitalization. […] These patients – we know them and, naturally, refer to hospital. [GP, Russia]
In terms of personal knowledge, the GPs emphasized that knowledge about their patients’ help-seeking behavior, their ways to present symptoms, and whether a patient was predisposed to anxiety was helpful to judge the “real” severity of symptoms and necessity for treatment.
The first thing is whether the patient is known to me, […]. How often has he been in the practice and does he tend to be a hypochondriac? [GP, Germany]
Overall, we found that the GPs’ knowledge about a particular patient could serve as a frame of reference, adding a certain sense of security and confidence to the GPs’ assessment and decisions.
Balancing the patients’ perspective
The GPs’ knowledge about their patients also seemed important in assessing whether they could rely on the patients’ own judgment about the necessity for treatment and hospitalization.
I believe that patients are rather good at assessing that themselves. Not all of them of course, but severe and long-term COPD patients know when something is really wrong. [GP, the Netherlands]
Many of the GPs’ stories indicated that they favored active involvement of patients in the decision-making, being aware of the patients’ experiential knowledge from having lived with COPD. Knowledge about the previous effectiveness of treatments and hospitalizations were seen as particularly valuable. Similarly, the GPs knew that patients’ opinions did not necessarily reflect a biomedical need, but also the need for relieving anxiety and meeting challenges in the patients’ social life.
I think the other thing is why the patient wants antibiotics this time, he may have had other exacerbations through the year and managed them himself, maybe this time he wants to be treated as he’s going on holidays next week or he’s been keeping his wife awake and she’s fed up of his coughs, maybe find out why this time he feels he’s bad enough to want antibiotics. [GP, Wales]
Consequently, there could be discrepancies between the GPs’ and patients’ judgments, which the GPs had to balance. When the GPs considered treatment or hospitalization unnecessary but the patient insisted, the GPs had to decide whether to make efforts to convince the patients about their position or to give into the patients’ requests. While the GPs seemed most critical regarding the patients’ opinion about antibiotic treatment, they seemed to largely acknowledge the patients’ preferences regarding the safe surroundings of a hospital.
If she is a worried lady and self-wants to be in a hospital I would set the threshold even lower I suppose. [GP, Norway]
However, more challenging for the GPs were contrary situations, in which the GP would prefer medical treatment or hospitalization, but the patients refused.
And it all comes down to the patient’s consent, when he says: you won’t get me into a hospital, I can’t do anything. [GP, Germany]
According to the GPs, patients might be afraid to take oral corticosteroids or did not want to be treated in hospital. Lack of patients’ consent to treatment or referral to the hospital seemed particularly challenging for the GPs, as it could increase their worries. In such situations, but also, in general, possibilities to sharing responsibility emerged as important aspects of the GPs decision-making.
Outpatient support and collaboration
The GPs’ emphasized repeatedly that the patients’ social context, as well as infrastructural and organizational aspects, were highly relevant to their management decisions. Considering that the GPs often wished to manage patients in an outpatient setting but could be worried about further deteriorations, reliable outpatient support emerged as one of the most important aspects in this regard.
Sometimes, indeed, the hospitalization is not connected with the condition of the patient, not for purely medical reasons, but really for social factors. Could the patient reach the day care hospital, whether it is possible to organize at home and if the doctor and nurse are busy […] Many factors affect hospitalization. [GP, Russia]
“Social factors”, as this GP described them, could be home support by family members, specialized nurse teams, or day care institutions, which could ensure that patients took their medications correctly and were monitored by family members or health care professionals. In addition to reliable home support, social and infrastructural circumstances sufficient to ensure that patients could reach any sort of emergency care institution, if needed, seemed crucial to whether the GPs considered hospitalization as necessary or not.
Moderator: Ok, then if a patient is at risk when treated at home, is there any options in your management other than hospitalization?
GP1: In Hong Kong? […]. If the case is so risky, […] I cannot think of any [other option].
GP2: In Hong Kong, there is no community nurse support.
GP4: It seems that CNS [Community Nursing Service] does not cover COPD cases unless they have poor drug compliance.
Moderator: Then, all of you can only think of hospitalization?
GP3: Actually, we can see whether NGOs [non-governmental organizations] could help, but if the patients are not members of these NGOs, there will not be services available for them. [Hong Kong]
Overall, having such “insurances” to reduce the risk of severe outcomes seemed to raise the GPs’ readiness to assume the risk and try outpatient management in the first place, which could be particularly important when dealing with patients whose care belonged somewhere between their own and the hospitals’ responsibility. Depending on the health care systems’ organization, GPs could even create their own “insurances,” such as giving patients a “standby” referral they could redeem when their condition worsened.
However, a reliable outpatient network could not always make for up the GPs’ worries caused by uncertainty regarding the underlying cause of symptoms and appropriate treatment. In this regard, referring to hospitalizations could not always serve pure therapeutic, but also diagnostic purposes.
I think from that worry, from that worry I think if they have a co-existing infection possibly maybe pneumonia, I’d be admitting them. I think if they need a chest X-ray they need it then, as opposed to going next Monday, […]. [GP, Wales]
Referring to diagnostics, however, could also serve the purpose of transferring responsibility to secondary care, when feeling that a patient’s condition was too severe to keep responsibility but lacking a “good” biomedical reason to justify hospitalization.
[…], […] sometimes we try […] we don’t write: ‘for hospitalization’, but only ‘for diagnostic evaluation in the Admission Room’. Sometimes, they ‘buy’ such things […] [GP, Russia]
This citation indicates that implementing a certain decision that involved other actors within the health care system, depends, at least partly, on these actors’ acceptance. In fact, some GPs shared their experiences with not finding acceptance for their referrals, which forced them to remain responsible for patients even though this could be outside their own comfort zone.
Discussion
Main findings
The GPs aimed to make accurate medical decisions and avoid unnecessary prescriptions/hospitalizations, yet worries about having overlooked a severe underlying illness seem to fuel “better safe than sorry” decisions. Under medical uncertainty, “knowing the patient” provided a supplementary framework to make sense of the clinical picture and to make more differentiated judgments. The GPs considered patients’ experiential knowledge about their own body and illness as valuable, yet disagreements between their own and the patients’ perceptions could be difficult to deal with. Both formal and informal caregivers, as well as organizational and infrastructural aspects of the health systems, influenced the decision-making, particularly in terms of providing an “insurance” to reduce the risk of severe consequences of “wrong decisions” and concerning the negotiation of responsibilities.
Discussion of main findings
Role of symptoms and signs
Quantitative investigations on GPs’ prescribing behavior for AECOPD (and other respiratory diseases) have shown that symptoms and signs such as colored sputum, severe dyspnea, and CRP testing are associated with treatment decisions for antibiotics and/or oral corticosteroids.29–32 Our findings confirm that GPs consider these clinical cues relevant to their decision-making, yet also show that GPs cannot always rely on their presence and significance. Indeed, as Mueller and Tamm stated, “observational studies might overestimate the diagnostic value of a marker.”33 In the context of chronic illness and comorbidity, differentiating a “pure” AECOPD from other somatic diseases such as pneumonia or heart disease34 and from anxiety35 is probably particularly challenging in a primary care setting.
Responses to medical uncertainty
Uncertainty due to inconclusive clinical findings refers not only to a lack of information but also to emotional responses, which may be highly influential in decision-making.36,37 We found that worries/fear about overlooking a severe illness were quite dominant emotions in the GPs’ narrations, which related to rather categorical precautionary prescribing and hospitalization. From a psychological perspective, such “action rather than inaction”38 may compose a strategy to deal with uncertainty through avoiding unpleasant feelings and pondering after the decision is made.39,40 GPs may also experience “prescribing against the evidence,” such as prescribing antibiotics without proof of bacterial infection, as uncomfortable. Yet such rather abstract risks seemed less relevant to the GPs’ decision-making18 than more concrete risks, whose consequences may not only affect the patient but also the GPs themselves.41 Therefore, it may not surprise that having an “insurance” seemed related to more risk tolerance and motivation to remain responsible for a patient.
Holistic understanding of illness
Precautionary decision-making may be regarded as a stress response to uncertainty.42,43 Drawing on this concept, Evans and Trotter suggested that clinicians with a holistic, biopsychosocial understanding of illness had fewer stress reactions to uncertainty than those with the biomedical understanding that symptoms always have a detectable biomedical cause.44 Also, Fairhurst and May suggested that clinician’s knowledge about their patients’ “behavior and cognition” is related to patient-centered consultation styles and positive consultation experiences.45 Comparably, our results indicate that a holistic interpretative framework based on “knowing the patient” is helpful for GPs to make more differentiated and confident treatment decisions. Yet, GPs may not always have this specific knowledge about their patients.46 Recognizing “contextual red flags,” which may address relevant contextual issues, under the consultation has been suggested important to achieve health benefits for patients.47,48
Involving patients
Adapting care plans to the individual’s contextual circumstances would include acknowledging patients’ own opinions about symptoms and the most appropriate treatment options. Involving patients in treatment decisions is a key concept of the shared decision-making model, which is frequently promoted in chronic care policies.49,50 This may, however, primarily relate to chronic care situations and not so much to acute medical situations, which COPD exacerbations after all are.51 Moreover, our findings suggest that the patients’ expertise seemed most valuable to GPs when feeling unsure themselves. Otherwise, patients’ opinions could be “downgraded” to “preferences”, sometimes difficult to deal with. Therefore, GPs’ motivations to involve patients in the decision-making may, at least partly, be a strategy to deal with uncertainty rather than reflect implementation of a care concept.52 This may be important to consider for the implementation of care strategies and policies. A variety of factors influence patient involvement in decision-making, including the patients’ motivation to be involved and their expectations of the consultation.53–56 Importantly, in terms of prescribing antibiotics, the clinicians’ perception of the patients’ expectations seems to strongly predict prescribing.57–60 Addressing patients’ expectations – rather than teaching them about the uselessness of antibiotics on viruses – seem critical in reducing unnecessary use of antibiotics.61–63
Support from other caregivers and collaboration
According to our findings, not only GPs and patients but also patients’ family members, other health care professionals as well as organizational and infrastructural factors play a part in shaping decisions. The influence of social, health care systems, and infrastructural factors on clinical decision-making has been described previously, and depending on national and local circumstances, such factors may be limiting or enabling to GPs’ practice.64,65 Yet, explanations for these statistical relationships are rare. Our findings suggest that such contextual factors’ can affect GPs’ overall risk assessment, for example, in providing what we called “security network” or “insurance.” Both professional outpatient care services, such as specialist nurses providing home visits, and family members could embody such an “insurance.” Thus, more important than the type of service or the “title” of actors seems their function to bear some of the responsibility and to attenuate consequences of “wrong” decision. This finding strengthens the importance of community-based care services, such as ambulant nursing services in COPD care,66 but also of informal caregivers. Cooperation between informal caregivers and health care professionals can be challenged by different perspectives on a conditions’ severity and unclear areas of responsibility.67,68 Our findings indicate that GPs can face similar challenges in cooperation with other health care professionals. For instance, when hospital doctors base their judgments on stricter biomedical criteria than GPs.69 Due to not speaking “the same language,”69 referral decisions based on a holistic evaluation might not match with criteria from more biomedical oriented guidelines applied in specialist care.
Strengths and limitations
The study’s cross-cultural design allowed us to look at common issues despite different health care systems and cultural contexts, and we argue that our findings have uncovered overall aspects relevant to more than just one particular setting. Yet, we acknowledge that our focus on common views produced in a focus group setting does not allow for specifying differences between countries and the role of particular health systems and cultural aspects, so the direct applicability of our findings in specific settings may be limited. Moreover, the GPs in our sample had different backgrounds in terms of clinical experience, gender, and workplace, all of which may have affected the results. More experienced GPs may for instance tolerate more uncertainty,70,71 may therefore be less worried than inexperienced GPs, and might therefore refrain to a larger extent from precautionary decisions. Female GPs may tolerate less uncertainty than male GPs,71 but may practice being more patient-centered and spend more time on patients,72 perhaps enabling female GPs to better deal with uncertainty. GPs in high-frequented practices may be more likely to prescribe antibiotics as this is least time consuming73 and GPs who practice in urban areas with better access to specialists may refer more patients than those in rural areas. However, this may reflect other differences between urban and rural practices.74 Knowing this, we still maintained a focus on common views and themes cutting across the sample as is often done in FGD analyses, and while no immediate implications emerged, we did not explore specifically for variations linked to the sample and we may have missed, eg, the influence of experiences on practice routines. This could be interesting to elaborate in further studies. In terms of recruitment, the fact that some participants knew each other might have created a safe setting for in-depth discussions, but may also have composed a barrier to critical and open-minded comments about daily practice. There were considerable differences in response rates across the countries (Table 1), which may be due to different recruitment methods. Participating GPs may be above-average be interested in this particular topic, and in general interested in reflective activities on clinical practice. The different moderators were trained in the research method and used the same interview guide; however, different moderation styles and different settings put emphasis on different topics in the discussions. Even though the research group members discussed the meaning of phrases when in doubt, using translated transcripts for data analysis always carries the risk that phrases/ideas do not reflect their actual meaning. Finally, it has to be kept in mind that studying decision-making with FGDs can only tell us something about how decisions are thought to be made, not how they are made in the actual consultations.24
Conclusion
Fear of overlooking severe illness and of further deteriorating symptoms emerged as a main driver of GPs’ decision-making regarding the management of patients with COPD exacerbations. Individual coping styles may partly explain variations in prescribing and high hospitalization rates. Yet, the perceived availability and reliability of other formal and informal carers to share responsibility with, and a functioning local infrastructure to ensure transportation to professional care is important for GPs to refrain from a “better safe than sorry” approach to decision-making. Other types of knowledge than biomedical knowledge, such as experiential knowledge of patients and GPs’ personal knowledge about a patient, should be acknowledged as valid conceptual resource for decision-making. Overall, our findings suggest that multiple stakeholders are involved in the management of COPD exacerbations, and that their approach to decision-making may not always be compatible with each other and with care goals of policy makers. This study suggests a collaborative approach to COPD management across all care sectors. Fruitful collaboration requires communication to address mismatches in perceived “appropriateness” of a decision, and clear areas of responsibilities between GPs, other health care professionals, patients, and their social network. This could be helpful to reduce hospitalization rates and unnecessary use of medications, and at the same time ensure monitoring of patients and prompt intervention if necessary.
Disclosure
The authors report no conflicts of interest in this work.
References
Anzueto A. Impact of exacerbations on COPD. Eur Respir Rev. 2010;19(116):113–118. | ||
Toy EL, Gallagher KF, Stanley EL, Swensen AR, Duh MH. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: a review. COPD. 2010;7(3):214–228. | ||
Wilkinson TM, Donaldson GC, Hurst JR, Seemungal TA, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;169(12):1298–1303. | ||
Allan J, Gay B, Crebolder H, et al. eds. The European definition of General Practice/Family Medicine. WHO Europe Office, Barcelona, Spain WONCA Europe; 2011. | ||
Global Strategy for the diagnosis, management, and prevention of COPD: Revised 2016. Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Available from: http://www.goldcopd.org. Accessed August 2016. | ||
Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662–665. | ||
Andre M, Vernby A, Odenholt I, et al. [General practitioners prescribed less antibiotics but used the CRP test more. Diagnosis-prescription studies in 2000–2005]. Lakartidningen. 2008;105(41):2851–2854. Sweden. | ||
de Vries M, Berendsen AJ, Bosveld HE, Kerstjens HA, van der Molen T. COPD exacerbations in general practice: variability in oral prednisolone courses. BMC Fam Pract. 2012;13(1):1–7. | ||
Murio C, Soler X, Perez M, Calero G, Ruiz-Manzano J. Acute exacerbation of chronic obstructive pulmonary disease in primary care setting in Spain: the EPOCAP study. Ther Adv Respir Dis. 2010;4(4):215–223. | ||
Salwan AA, Spigt M, Laue J, Melbye H. Predictors of treatment with antibiotics and systemic corticosteroids for acute exacerbations of asthma and chronic obstructive pulmonary disease in primary care. BMC Fam Pract. 2015;16(1):1–10. | ||
Decramer M, Bartsch P, Pauwels R, Yernault JC. Management of COPD according to guidelines. A national survey among Belgian physicians. Monaldi Arch Chest Dis. 2003;59(1):62–80. | ||
Miravitlles M, Mayordomo C, Artes M, Sanchez-Agudo L, Nicolau F, Segu JL. Treatment of chronic obstructive pulmonary disease and its exacerbations in general practice for EOLO Group. Estudio observacional de la limitacion obstructiva al Flujo aEreo. Respir Med. 1999;93(3):173–179. | ||
Vollenweider DJ, Jarrett H, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257. | ||
Walters JA, Gibson PG, Wood-Baker R, Hannay M, Walters EH. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2009;1:CD001288. | ||
Laue J, Reierth E, Melbye H. When should acute exacerbations of COPD be treated with systemic corticosteroids and antibiotics in primary care: a systematic review of current COPD guidelines. NPJ Prim Care Respir Med. 2015;25:15002. | ||
Risør MB, Spigt M, Iversen R, et al. The complexity of managing COPD exacerbations: a grounded theory study of European general practice. BMJ Open. 2013;3(12):e003861. | ||
Horwood J, Cabral C, Hay AD, Ingram J. Primary care clinician antibiotic prescribing decisions in consultations for children with RTIs: a qualitative interview study. Br J Gen Pract. 2016;66(644):e207–e213. | ||
Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N. Understanding the culture of prescribing: qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ. 1998;317(7159):637–642. | ||
Wennberg JE. Time to tackle unwarranted variations in practice. BMJ. 2011;342(26):687–690. | ||
Patel VL, Kaufman DR, Arocha JF. Emerging paradigms of cognition in medical decision-making. J Biomed Inform. 2002;35(1):52–75. | ||
Lipshitz R, Klein G, Orasanu J, Salas E. Taking stock of naturalistic decision making. J Behav Decis Mak. 2001;14(5):331–352. | ||
Falzer PR. Cognitive schema and naturalistic decision-making in evidence-based practices. J Biomed Inform. 2004;37(2):86–98. | ||
Petursson P. GPs’ reasons for “non-pharmacological” prescribing of antibiotics. A phenomenological study. Scand J Prim Health Care. 2005;23(2):120–125. | ||
Kitzinger J. Qualitative research. Introducing focus groups. BMJ. 1995;311(7000):299–302. | ||
Davies F, Risør MB, Melbye H, et al. Primary and secondary care clinicians’ views on self-treatment of COPD exacerbations: a multinational qualitative study. Patient Educ Couns. 2014;96(2):256–263. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
NVivo qualitative data analysis software; QSR International Pty Ltd. version 10, 2012 [computer program]. Accessed June 2016. | ||
Mindjet Mindmanager. Available from: https://www.mindjet.com/mindmanager/. Accessed November 2015. | ||
Llor C, Bjerrum L, Munck A, et al. Predictors for antibiotic prescribing in patients with exacerbations of COPD in general practice. Ther Adv Respir Dis. 2013;7(3):131–137. | ||
Hopstaken RM, Butler CC, Muris JW, et al. Do clinical findings in lower respiratory tract infection help general practitioners prescribe antibiotics appropriately? An observational cohort study in general practice. Fam Pract. 2006;23(2):180–187. | ||
Hopstaken RM, Stobberingh EE, Knottnerus JA, et al. Clinical items not helpful in differentiating viral from bacterial lower respiratory tract infections in general practice. J Clin Epidemiol. 2005;58(2):175–183. | ||
Fischer T, Fischer S, Kochen MM, Hummers-Pradier E. Influence of patient symptoms and physical findings on general practitioners’ treatment of respiratory tract infections: a direct observation study. BMC Fam Pract. 2005;6(1):6. | ||
Mueller B, Tamm M. Biomarkers in acute exacerbation of chronic obstructive pulmonary disease: among the blind, the one-eyed is king. Am J Respir Crit Care Med. 2006;174(8):848–849. | ||
Cavailles A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. | ||
Halpin D, Hyland M, Blake S, et al. Understanding fear and anxiety in patients at the time of an exacerbation of chronic obstructive pulmonary disease: a qualitative study. JRSM Open. 2015;6(12):2054270415614543. | ||
Slovic P, Finucane ML, Peters E, MacGregor DG. Risk as analysis and risk as feelings: some thoughts about affect, reason, risk, and rationality. Risk Anal. 2004;24(2):311–322. | ||
Loewenstein GF, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychol Bull. 2001;127(2):267–286. | ||
Berger L, Bleichrodt H, Eeckhoudt L. Treatment decisions under ambiguity. J Health Econ. 2013;32(3):559–569. | ||
Sorum PC, Mullet E, Shim J, Bonnin-Scaon S, Chasseigne G, Cogneau J. Avoidance of anticipated regret: the ordering of prostate-specific antigen tests. Med Decis Making. 2004;24(2):149–159. | ||
Djulbegovic M, Beckstead J, Elqayam S, et al. Thinking styles and regret in physicians. PLoS One. 2015;10(8):e0134038. | ||
Heath I. Role of fear in overdiagnosis and overtreatment – an essay by iona Heath. BMJ. 2014;349:g6123. | ||
Gerrity MS, White KP, DeVellis RF, Dittus RS. Physicians’ reactions to uncertainty: Refining the constructs and scales. Motiv Emot. 1995;19(3):175–191. | ||
Gerrity MS, DeVellis RF, Earp JA. Physicians’ reactions to uncertainty in patient care. A new measure and new insights. Med Care. 1990;28(8):724–736. | ||
Evans L, Trotter DR. Epistemology and uncertainty in primary care: an exploratory study. Fam Med. 2009;41(5):319–326. | ||
Fairhurst K, May C. Knowing patients and knowledge about patients: evidence of modes of reasoning in the consultation? Fam Pract. 2001;18(5):501–505. | ||
Mjølstad BP, Kirkengen AL, Getz L, Hetlevik I. What do GPs actually know about their patients as persons? Eur J Pers Cent Healthc. 2013;1(1):149–160. | ||
Weiner SJ. Contextualizing medical decisions to individualize care: Lessons from the qualitative sciences. J Gen Intern Med. 2004;19(3):281–285. | ||
Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158(8):573–579. | ||
Thompson AG. The meaning of patient involvement and participation in health care consultations: a taxonomy. Soc Sci Med. 2007;64(6):1297–1310. | ||
Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (Or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692. | ||
Watt S. Clinical decision-making in the context of chronic illness. Health Expect. 2000;3(1):6–16. | ||
Fried TR. Shared decision making – finding the sweet spot. N Engl J Med. 2016;374(2):104–106. | ||
Gravel K, Legare F, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals’ perceptions. Implement Sci. 2006;1:16. | ||
McKinstry B. Do patients wish to be involved in decision making in the consultation? A cross sectional survey with video vignettes. BMJ. 2000;321(7265):867–871. | ||
Benbassat J, Pilpel D, Tidhar M. Patients’ preferences for participation in clinical decision making: a review of published surveys.Behav Med. 1998;24(2):81–88. | ||
Levinson W, Kao A, Kuby A, Thisted RA. Not all patients want to participate in decision making. A national study of public preferences. J Gen Intern Med. 2005;20(6):531–535. | ||
Britten N, Ukoumunne O. The influence of patients’ hopes of receiving a prescription on doctors’ perceptions and the decision to prescribe: a questionnaire survey. BMJ. 1997;315(7121):1506–1510. | ||
Cockburn J, Pit S. Prescribing behaviour in clinical practice: patients’ expectations and doctors’ perceptions of patients’ expectations – a questionnaire study. BMJ. 1997;315(7107):520–523. | ||
Coenen S, Michiels B, Renard D, Denekens J, Van Royen P. Antibiotic prescribing for acute cough: the effect of perceived patient demand. Br J Gen Pract. 2006;56(524):183–190. | ||
Jakobsen KA, Melbye H, Kelly MJ, et al. Influence of CRP testing and clinical findings on antibiotic prescribing in adults presenting with acute cough in primary care. Scand J Prim Health Care. 2010;28(4):229–236. | ||
Altiner A, Brockmann S, Sielk M, Wilm S, Wegscheider K, Abholz HH. Reducing antibiotic prescriptions for acute cough by motivating GPs to change their attitudes to communication and empowering patients: a cluster-randomized intervention study. J Antimicrob Chemother. 2007;60(3):638–644. | ||
Butler CC, Kinnersley P, Prout H, Rollnick S, Edwards A, Elwyn G. Antibiotics and shared decision-making in primary care. J Antimicrob Chemother. 2001;48(3):435–440. | ||
Britten N, Stevenson FA, Barry CA, Barber N, Bradley CP. Misunderstandings in prescribing decisions in general practice: qualitative study. BMJ. 2000;320(7233):484–488. | ||
Hajjaj FM, Salek MS, Basra MK, Finlay AY. Non-clinical influences on clinical decision-making: a major challenge to evidence-based practice. J R Soc Med. 2010;103(5):178–187. | ||
Wong AW, Gan WQ, Burns J, Sin DD, van Eeden SF. Acute exacerbation of chronic obstructive pulmonary disease: influence of social factors in determining length of hospital stay and readmission rates. Can Respir J. 2008;15(7):361–364. | ||
Fletcher MJ, Dahl BH. Expanding nurse practice in COPD: is it key to providing high quality, effective and safe patient care? Prim Care Respir J. 2013;22(2):230–233. | ||
Aasbø G, Rugkåsa J, Solbrække KN, Werner A. Negotiating the care-giving role: family members’ experience during critical exacerbation of COPD in Norway. Health Soc Care Community. Epub 2016 Apr 21. | ||
Berntsen GKR, Gammon D, Steinsbekk A, et al. How do we deal with multiple goals for care within an individual patient trajectory? A document content analysis of health service research papers on goals for care. BMJ Open. 2015;5(12):e009403. | ||
Howie JG. Diagnosis – the Achilles heel? Br J Gen Pract. 1972;22(118):310–315. | ||
Nevalainen M, Kuikka L, Pitkälä K. Medical errors and uncertainty in primary health care: a comparative study of coping strategies among young and experienced GPs. Scand J Prim Health Care. 2014;32(2):84–89. | ||
Ringberg U, Fleten N, Førde OH. Examining the variation in GPs’ referral practice: a cross-sectional study of GPs’ reasons for referral. Br J Gen Pract. 2014;64(624):e426–e433. | ||
Roter DL, Hall JA. Physician gender and patient-centered communication: a critical review of empirical research. Annu Rev Public Health. 2004;25:497–519. | ||
Mousquès J, Renaud T, Scemama O. Is the “practice style” hypothesis relevant for general practitioners? An analysis of antibiotics prescription for acute rhinopharyngitis. Soc Sci Med. 2010;70(8):1176–1184. | ||
O’Donnell CA. Variation in GP referral rates: what can we learn for the literature? Fam Pract. 2000;17(6):462–471. |
Supplementary material
Patient stories
- A 60-year-old male patient with moderate COPD has called your practice and asked for medicine, due to increased coughing and shortness of breath the last week. He quit smoking a year ago. You have prescribed anticholinergics for inhalation as maintenance medication. Now he thinks a course of antibiotics might be helpful. He was treated with amoxicillin and prednisolone last winter 9 months ago, and recovered after a few weeks.
- A 70-year-old female patient, still smoking, visits your practice. She was hospitalized due to her COPD 1 year ago. She uses a combination of inhaled corticosteroids and long acting beta2 agonists, and short acting beta2 agonists on demand. She had a common cold a week ago. Now she has no fever, but breathes heavily and rather fast. She had to sit in her bed last night, and she feels somewhat exhausted. Although you hear wheezes all over her chest, you do not think the obstruction is very severe. You believe her illness is worsened by her anxiety, but consider admitting her to hospital.
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.