Back to Journals » Clinical Ophthalmology » Volume 13
Hospital-Based Ocular Trauma: Factors, Treatment, And Impact Outcome
Authors Ababneh LT ![]() , Mohidat H, Abdelnabi H, Kana’an MF
, Mohidat H, Abdelnabi H, Kana’an MF ![]() , Tashtush NA
, Tashtush NA ![]() , El-Mulki OS, Aleshawi AJ
, El-Mulki OS, Aleshawi AJ
Received 16 July 2019
Accepted for publication 9 October 2019
Published 31 October 2019 Volume 2019:13 Pages 2119—2126
DOI https://doi.org/10.2147/OPTH.S223379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Laila T Ababneh,1 Hasan Mohidat,1 Heba Abdelnabi,1 Mohammed F Kana’an,2 Nour A Tashtush,2 Omar S El-Mulki,1 Abdelwahab J Aleshawi2
1Department of Special Surgery, Division of Ophthalmology, Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan; 2Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan
Correspondence: Laila T Ababneh
Department of Special Surgery, Division of Ophthalmology, Faculty of Medicine, Jordan University of Science and Technology, P. O. Box: 3030, Irbid 22110, Jordan
Tel +962799770699
Fax +962 2 7201064
Email [email protected]
Background: Specific morbidities as blindness is a serious complication that commonly results from patients with ocular traumas and can significantly impair the patient’s social and occupational abilities. This study is conducted due to the current lack of data on ocular injuries in developing countries and places near war regions and aims to investigate and evaluate the impact of ocular trauma.
Material and methods: After Institutional Review Board approval was obtained, we retrospectively identified 112 patients who were admitted due to eye trauma from January 2015 until October 2018. Information about demographics, diagnostic modalities, prognostic impact, and treatment interventions were retrieved, analyzed.
Results: One-hundred and twelve patients were included in the study. The majority of patients were males. The mean age for patients was 22.2. Road traffic accident (RTA) constituted the most common cause of trauma (60.7%). Gunshots and blast injuries were observed in 12.5% of patients. Workplace injuries were infrequent (8.1%). The gunshot was significantly associated with injury to two or more eyeball structures while the RTA was significantly related to one eyeball structure injury. RTA was associated with intact globe while gunshot was significantly associated with ruptured globes. The mean duration of admission was 8.1 days. Associated truncal injury is the most important independent factor affecting the duration of admission.
Conclusion: Majority of trauma cases occurred in young males involved in RTAs. The location of Jordan near the Syrian war increases the appearance of gunshot ocular trauma in specific and ocular trauma in general. Educating the public is essential if we wish to prevent eye injuries.
Keywords: eyeball, lens, globe, gunshot, road traffic accident
Introduction
Ocular trauma is a preventable public health problem. Eye injuries are the main cause of monocular visual disability and non-congenital unilateral blindness.1,2 Eye trauma constitutes 7% of all bodily injuries and 10–15% of all eye diseases.3 Specific morbidities as blindness is a serious complication that commonly results from ocular traumas and can significantly impair the patient’s social and occupational abilities.3 Although eye trauma causes immense economic and social burden, it is often overlooked by health officials and simple effective procedural improvements may not be realized.4,5
This study is motivated by the current lack of data on ocular injuries in Jordan and the Middle Eastern region and foreseeing a great benefit in uplifting and creating a safer environment for the inhabitants in a region complains of many wars as well as further providing different databases over time. This study focuses on types of ocular trauma and their outputs among different age groups. The mechanism of trauma is also analyzed to determine risky objects or hazardous modifiable habits. Outputs of trauma on different ocular structures and its association with corresponding mechanisms are also discussed. Treatment modalities and procedures were noted along with prognoses.
Materials And Methods
This study was conducted at King Abdullah University Hospital, a tertiary care center that is affiliated with the Jordan University of Science and Technology, located in northern Jordan. After obtaining the Institutional Review Board approval, we retrospectively identified those patients who were admitted due to ophthalmic trauma between January 2015 and October 2018. The following information were obtained: demographics (age, sex, date and season of admission), causes and objects of trauma, medical status of patients, associated body injury, site of involvement, mechanism of injury, and detailed eye parts involvement. In addition, imaging modalities with findings, and management interventions were retrieved.
The included group comprised patients who were admitted either directly by the ophthalmic team due to the necessity to undergo ophthalmic surgery or admitted by other departmental staff and the ophthalmic team was consulted. The causes of trauma were categorized into occupational traumas, road traffic accident (RTA), gunshots, home hazards, violence, blasts and falling down. The medical status was assigned as free if the patient did not complain of diabetes, hypertension, ischemic heart disease and neurological disorders. The associated body injuries were blocked into head and neck injury, trunk injury, and limbs injury. The site of involvement was either right eye or left eye or both. The mechanisms for which traumatic injury attributed were blunt injury, sharp or chemical injury. Length of admission was measured from the day of admission to the day of discharge.
Detailed description for each part of the eye was retrieved. Bony orbit, orbital soft tissues and extraocular muscles, the eyelids and ocular adnexa and eyeball components (both anterior and posterior segments) were studied and reviewed. First, the eyeball involvement was studied in a general point of view and categorized into (no involvement, one structure involved, two or more structures involved). Diagnostic modalities with its findings were investigated and categorized into hematoma, foreign body, vitreous hemorrhage, ruptured globe and fractures. Different methods of interventions were utilized. Conservative therapy by cold compressor, medical therapy, surgical interventions as primary globe repair or combined surgeries of intraocular foreign body removal and retinal detachment repair and other procedures were utilized.
Setting
The ophthalmic team who was responsible for admission consisted of consultant ophthalmologists and senior residents who follow the same guidelines. The surgical interventions were performed by well-trained consultant ophthalmologists with the same surgical and anesthetic guidelines. The imaging modalities were generated and investigated by a consultant radiologist. Every case received prompt management within the first 24 hrs with the application of proper prophylactic measures.
Statistical Analysis
Data were entered into a spreadsheet. Statistical analyses were performed using IBM SPSS Statistics Software (v.21), 2012. Data were presented as frequency distributions for categorical variables and mean ± standard error of the mean for continuous variables. Data were tested at a significance level of 0.05%. Pearson χ2 test was used to investigate the significance of the association between categorical variables, while student’s t-test and ANOVA were applied to examine the significance level for continuous normally distributed variables. The normality of the distribution of data was tested using the Kolmogorov–Smirnov test. Kruskal–Walis and Mann–Whitney tests were applied for the abnormally distributed continuous variable. If a significant (P<0.05) relationship was found, then a posthoc residual analysis for categorical variables and a Fisher’s least significant difference test for continuous variables were applied to determine the exact significance between groups for each variable. Multiple linear and multiple logistic regression analyses were utilized to study the multiple effects of different variables.
Results
Demographics And Patients’ Characteristics
Out of 1103 traumatic cases during the study period, one-hundred and twelve patients (10.5%) were included in the study. The majority of patients were males. Eighty-five males (75.9%) and 27 (24.1%) females were included. The mean age for patients was 22.2. The youngest patient was 8 months and the oldest was 97 years. Most of the traumatic events happened within Summer. About 38.4% of patients admitted in Summer followed by Spring (22.3%), Winter (21.4%) and Autumn (17.9%). The seasons were measured according to the standard measurement in the Northern Hemisphere. Table 1 summarizes the general characteristics of the studied sample.
 |
Table 1 General Demographic And Patients’ Characteristics |
RTA constituted the most common cause of trauma as 68 (60.7%) patients involved. Falling down from buildings from different heights was the traumatic event in 15 patients. Gunshots and blast injuries were observed in 8% and 4.5% of patients, respectively. Occupational and home hazards were detected in 9 patients (three occupational and six at home) and most of these patients suffered from sharp injuries. Eighteen patients suffered from bilateral ocular injuries, 51 patients complained of right eye injury and 43 of the left. Blunt trauma as a mechanism was found in 81 patients, 30 as a sharp trauma and one chemical trauma. Associated head and neck injuries were detected in 84 (75.0%) of patients. Moreover, associated trunk and limbs injuries were present in 28 and 18 of patients, respectively. Only 8 patients were not medically free before the trauma. No complicating infections as endophthalmitis were reported. Also, Table 2 summarizes differences between causes of trauma.
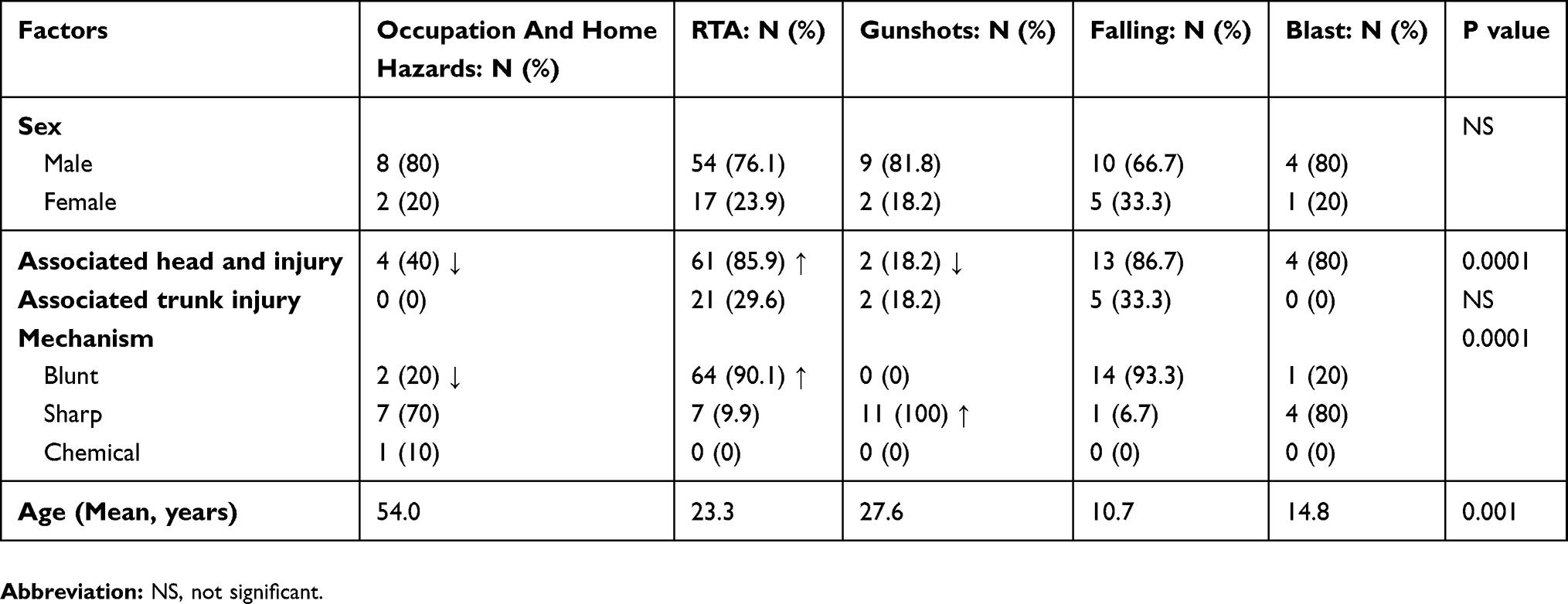 |
Table 2 Analysis Of Causes Of Trauma |
Impact Of Trauma
Ocular Part Involvement
The eyeball structures were spared in 45 of the patients, one structure involvement was detected in 32 patients and two or more structures were involved in 35 patients (Table 3). Corneal abrasions were detected in 24 patients and corneal laceration in 12 patients. Sclera was injured in 14 patients and subconjunctival hemorrhage was observed in 38 patients. Hyphema was revealed in 12 patients. The lenses were dislocated in 3 patients and cataract was evident in 10 patients. Relative Afferent Pupillary Defect was found in 15 patients and Iridodialysis in 3 patients. In addition, vitreous hemorrhage occurred in 10 patients and retinal detachment was disclosed in 4 patients.
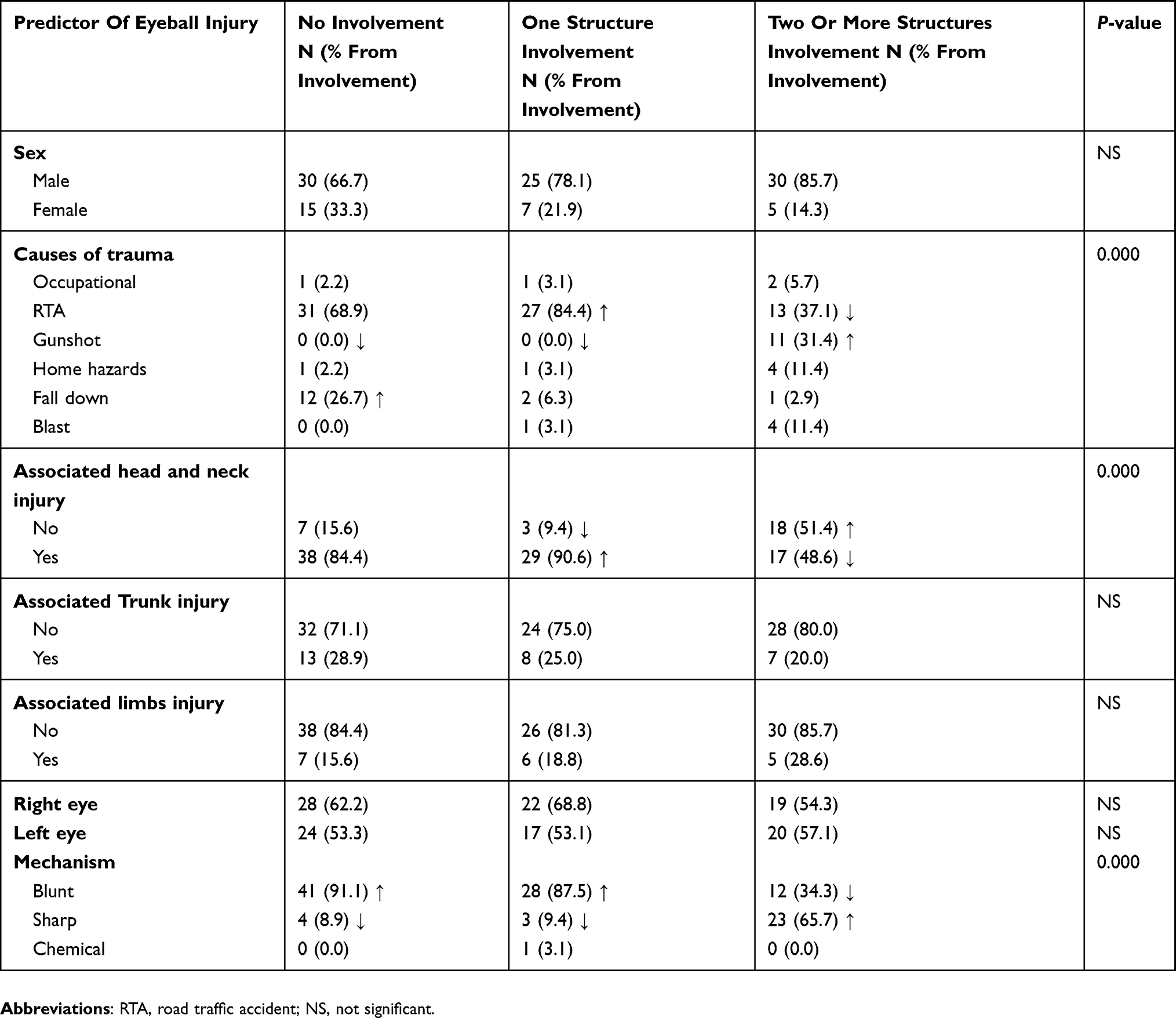 |
Table 3 Impact Of Trauma Of Eyeball Structures |
The gunshot as a causative trauma was associated significantly with two or more eyeball structures injury while the RTA was associated significantly related to one eyeball structure injury (P-value < 0.05). Falls were associated with no eyeball structure involvement. Specifically, 12 patients who fell did not experience any eyeball injury; P-value < 0.05. Interestingly, the presence of coexistent head and neck injury was associated with one eyeball structure involvement while it was not in the case of two or more structures. Trunk and limbs injuries did not reveal any association with eyeball injuries. In addition, the mechanism of injury was associated significantly with eyeball involvement as follows; the blunt injury was associated significantly with one structure involvement and sharp injury was associated with two or more (P-value < 0.05). It is known for this study that the gunshot injury attributed to the trauma through a sharp mechanism while RTA and falling down through blunt injury (P-value < 0.05). The age, sex and season did not contribute to eyeball injury. Patients who experienced two or more eyeball structures injury underwent more surgical intervention. After performing multiple logistic regression, the causative trauma is the most single important factor attributed to the eyeball injury; patients who had gunshot trauma were at a 14.5-fold to have two or more eyeball structure injured and patients who had RTA were at 16.1-fold less risk to have two or more structure involvement.
The eyelid was lacerated in 24 patients and developed hematoma in 59 patients. The presence of the latter complication was associated significantly with RTA as a causative event and presented more significantly in association with head and neck injuries as well as blunt trauma rather than sharp which was more significantly contributed to laceration to it (P-value < 0.05).
Orbital walls were spared in 63 of the cases. Blowout fractures of the orbital floor were detected in 10 patients, roof in 12 patients, lateral surface in 13, medial surface in 2 patients and combined two or more surfaces in 12 patients. Falls, as a causative event, was associated with combined orbital injuries while gunshots were not (P-value < 0.05). Head and neck injuries were significantly associated with combined orbital injuries. The sharp mechanism injury was associated with no orbital injury and blunt trauma associated with blowout and roof injuries.
The globe was intact in 91 patients. In contrast, it was ruptured in 37 cases constituting 33% of the overall population. The anterior segment was injured in 6 patients, the posterior segment in 1 patient and both segments in 13 patients. RTA was associated with an intact globe while gunshot was associated significantly with ruptured globes. The co-existence of head and neck injury associated significantly and negatively with the presence of globe injury. A sharp mechanism was associated significantly with globe involvement. The presence of globe injury increased significantly the chance to have two or more eyeball structures involvement.
Duration Of Admission
The mean for the duration of admission was 8.1 days. The shortest duration was one day and the longest was 50 days. No factor was associated significantly with the length of duration except for the presence of trunk injury. Results showed that the co-existence of trunk injury increased the duration of admission (mean rank for the presence of truncal injury 49 versus 36 for the absence; P-value = 0.024).
Diagnosis And Treatment
Computed tomography (CT) was the most diagnostic tool utilized. The most findings in RTA and falls were hematoma and fractures. The most common finding in gunshot was the ruptured globe. The most sensitive finding for eyeball involvement was a ruptured globe (in 92.9% of patients who had two or more eyeball structure damaged).
Most patients experienced RTA underwent observational and medical management. However, most patients with gunshots underwent surgical and interventional management. Different surgical and interventional approaches were performed such as; orbital reconstruction, eyelid repair, globe repair, cataract extraction, intraocular foreign body removal and vitrectomy for retinal detachment repair.
Discussion
Because of the delicacy and the features of ocular tissues, any trauma that would not be harmful elsewhere in the body is a serious one in the eye. Direct ocular trauma results in different degrees of damage and often loss of the eye.6,7 The prime idea to figure out the impact of ocular and orbital trauma as this study guided was to correlate the cause and object of the trauma along with the mechanism which significantly affects the ocular structure and function. RTA was the cause of 60.7% of the cases while the second one was falling down from different heights 13.4%. This was similar to the previous study of ocular injuries in polytrauma patients in the UK that declared that RTA had the prevalence of 56% and falling down 28%.8 Another study in the USA of all hospital-based ocular emergencies declared that RTA recorded 17.4% of the cases (the first) and falling down 14.4% (the second).9 Gunshots and blast injuries recorded 8% (9 cases) and 3.5% (5 cases) respectively.9 However, in UK study, two cases were recorded gunshot.8 These results are in line with the globe rupture recorded cases in our study 9.82% (11/112 cases) while in the UK study the prevalence was 6% (11/222 cases).8
Patients who got the trauma in their working sites during doing their daily duties were 3 (2.7%) of total cases while who were hit by blunt or sharp objects indoors were 6 (5.4%) This means that home hazards prevalence is the double of occupational trauma, this insists the importance of spreading awareness about supervision of children play areas and available toys for each age group. Blunt ocular trauma records the highest prevalence in many studies, Georgouli et al reported the incidence of 64% of blunt trauma and Oner et al reported 48%. In this study, the blunt trauma was detected in 72.3%.10,11
All ages were revealed to be susceptible to ocular trauma. However, the mean age was found to be 22.2, which was clinically less than most other studies by at least 10 years.12–14 Only one study reported a similar mean age by Soliman and Macky.15 This confined and attributed to the prevalence of young age groups and early commencing to work in our country and in Egypt. Most of the reported cases were males 75.9% which is similar to previous studies where 80% and 74% of the cases were males.10,11
Head and neck trauma was the most frequent associated body trauma with ocular trauma recorded in 75% of cases, while in Soni et al study it was 94% of the patients.10 Eyelid hematoma and subconjunctival hemorrhage were the most common findings in the examination with 52.7% and 33.9%, respectively. Soni et al study revealed comparable percentages of 46% and 23%.10 The lens was the affected part in 10 cases (8.9%) as cataract and 3 cases (2.7) as lens dislocation, all cases needed surgical intervention for cataract or lens extraction with or without intraocular lens implantation. The most recorded posterior segment involvement was vitreous hemorrhage in 10 cases (8.9%) managed either by observation or surgical vitrectomy according to other posterior segment injuries.
The number of the recorded cases was dramatically increased comparing 2015/2016 to 2017/2018; 21 cases in 2015, 20 in 2016, 37 in 2017, and 34 in 2018, which is explained by the increasing incidence of RTAs during the last 3 years and the refugees of the Syrian war during 2017 specifically. Regarding the RTAs in Jordan and according to the Public Security Department in Jordan, Jordan faces 150,398 accidents in 2018 with 571 deaths and 16,203 injuries, 150,226 accidents in 2017 with 685 deaths and 16,246 injuries, 144,521 accidents in 2016 with 750 deaths and 17,435 injuries and 111,057 accidents in 2015 with 608 deaths and 16,139 injuries.16 These findings reveal two important points: the high prevalence of RTAs in Jordan. Also, it reveals that the impact of RTA is restricted to the survivors as the fatality of RTAs is high.
Although it was complicated to properly measure the visual acuity at presentation, comparing the visual acuity at presentation with that of discharge did not reveal any significant deterioration. On the contrary, there were improvements in some cases. Those with deterioration were due to complications like development of cataract or retinal detachment.
According to the revised classification of ocular trauma by Shukla et al,17 this study had 68 cases caused by RTA, 4 caused by industrial events, 16 caused by assault events and 21 caused by daily activity events.
Out study is not without limitations, in this study, we cannot depend on the visual acuity as a final outcome for patients as the general status of most traumatic patients was not allowed to transfer patient to do proper tests. In addition, many patients had improvement of vision on follow-up. This was not included in the study, due to inadequate follow-up of the majority of patients. Moreover, because of lacking proper documentation of other important variables, like profession, location, drug or alcohol we could not identify these as risk factors for eye trauma. Another point is that the impact of RTA is restricted to the survivors only.
Conclusion
We can conclude from our study that the majority of ocular traumas occurred because of RTAs. Also, males are more prone to ocular injuries because they are more involved at work and in streets. The location of Jordan near the Syrian war increases the appearance of gunshot ocular trauma in specific and ocular trauma in general. Most patients of ocular trauma are polytraumatic whom circumstances necessitate more diagnostic, medical and surgical interventions. Educating the public is essential if we wish to prevent eye injuries. Also, improving the good and secure workplaces is of crucial importance. This study hopes to lift the community’s quality of life and agitate social and legislative associations towards preventative measures for ocular traumas to control new incidences of ocular trauma.
Abbreviations
RTA, road traffic accident; CT, Computed tomography.
Ethics And Patient Consent
Written informed consent was obtained from the patients for publication. Institutional approval was obtained from the Institutional Review Board at Jordan University of Science and Technology. This study was conducted in accordance with the Declaration of Helsinki.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jandeck C, Kellner U, Bornfeld N, Foerster MH. Open globe injuries in children. Graefes Arch Clin Exp Ophthalmol. 2000;238(5):420–426. doi:10.1007/s004170050373
2. May DR, Kuhn FP, Morris RE, et al. The epidemiology of serious eye injuries from the United States Eye Injury Registry. Graefes Arch Clini Exp Ophthalmol. 2000;238(2):153–157. doi:10.1007/PL00007884
3. Acar U, Tok OY, Acar DE, Burcu A, Ornek F. A new ocular trauma score in pediatric penetrating eye injuries. Eye (Lond). 2011;25(3):370–374. doi:10.1038/eye.2010.211
4. Pieramici DJ, Au Eong KG, Sternberg P
5. Thompson CG, Kumar N, Billson FA, Martin F. The etiology of perforating ocular injuries in children. Br J Ophthalmol. 2002;86(8):920–922. doi:10.1136/bjo.86.8.920
6. De Juan E, Sternberg P, Michels RG. Penetrating ocular injuries, types of injuries and visual results. Ophthalmology. 1993;90(11):1318–1322. doi:10.1016/S0161-6420(83)34387-6
7. Esmaeli B, Elner SG, Schork MA, Elner VM. Visual outcome after penetrating trauma, a clinicopathological study. Ophthalmology. 1995;102(3):393–400. doi:10.1016/s0161-6420(95)31009-3
8. Georgouli T, Pountos I, Chang BY, Giannoudis PV. Prevalence of ocular and orbital injuries in polytrauma patients. Eur J Trauma Emerg Surg. 2011;37(2):135–140. doi:10.1007/s00068-010-0029-6
9. Cheung CA, Rogers-Martel M, Golas L, Chepurny A, Martel JB, Martel JR. Hospital-based ocular emergencies: epidemiology, treatment, and visual outcomes. Am J Emerg Med. 2014;32(3):221–224. doi:10.1016/j.ajem.2013.11.015
10. Soni M, Khan IU, Jadoon Z. The pattern of ocular trauma in patients at Govt. Naseerullah Khan Babar Memorial Hospital, Peshawar (A study from 2010–2014). Ophthalmol Update. 2015;13(4):271–275.
11. Oner A, Kekec Z, Krakucuk S, Ikizceli I, Sözüer EM. Ocular Trauma in Turkey: a 2-Year Prospective Study. Adv Ther. 2006;23(2):274–283.
12. Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries: factors predictive of poor outcome. Eye. 2006;20(12):1336–1341. doi:10.1038/sj.eye.6702099
13. Rofail M, Lee GA, O’Rourke P. Prognostic indicators for open globe injury. Clin Experiment Ophthalmol. 2006;34(8):783–786. doi:10.1111/j.1442-9071.2006.01309.x
14. Smith AR, O’Hagan SB, Gole GA. Epidemiology of open and closed-globe trauma Presenting to Cairns Base Hospital, Queensland. Clin Experiment Ophthalmol. 2006;34(3):252–259. doi:10.1111/j.1442-9071.2006.01200.x
15. Soliman MM, Macky TA. Pattern of ocular trauma in Egypt. Graefes Arch Clin Exp Ophthalmol. 2008;246(2):205–212. doi:10.1007/s00417-007-0720-4
16. Public Security Directorate of Jordan, Department of Traffic. Available from: https://www.psd.gov.jo/index.php/ar/2015-03-15-10-24-05.
17. Shukla B, Agrawal R, Shukla D, Seen S. Systematic analysis of ocular trauma by a new proposed ocular trauma classification. Indian J Ophthalmol. 2017;65(8):719–722. doi:10.4103/ijo.IJO_241_17
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.