Back to Journals » Journal of Blood Medicine » Volume 7
Hormonal and echocardiographic abnormalities in adult patients with sickle-cell anemia in Bahrain
Authors Garadah TS ![]() , Jaradet AA, Alalawi ME, Hassan AB
, Jaradet AA, Alalawi ME, Hassan AB ![]()
Received 11 October 2016
Accepted for publication 10 November 2016
Published 13 December 2016 Volume 2016:7 Pages 283—289
DOI https://doi.org/10.2147/JBM.S124426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
Taysir S Garadah,1,2 Ahmed A Jaradat,3 Mohammed E Alalawi,1 Adla B Hassan2
1Cardiac Unit, Salmaniya Medical Complex, Ministry of Health, 2Department of Internal Medicine, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, 3Department of Family and Community Medicine, Arabian Gulf University, Manama, Bahrain
Background: Adrenal, thyroid, and parathyroid gland hormonal changes are recognized in children with homozygous (HbSS) sickle-cell anemia (SCA), but are not clear in adult patients with SCA.
Aim: To assess the metabolic and endocrine abnormalities in adult patients with SCA and evaluate left ventricular (LV) systolic and diastolic functions compared with patients with no SCA and further study the relationship between serum levels of cortisol, free thyroxine (T4), and testosterone with serum ferritin.
Materials and methods: The study was conducted on 82 patients with adult HbSS SCA compared with a sex- and age-matched control group. The serum levels of cortisol, parathyroid hormone (PTH), testosterone, thyroid-stimulating hormone (TSH), and free T4 were compared. Blood levels of hemoglobin, reticulocyte count, lactate dehydrogenase (LDH), calcium, alkaline phosphatase (ALP), vitamin D3, and ferritin were also compared. Pulsed Doppler echo was performed to evaluate the LV mass, wall thickness, and cavity dimensions with diastolic filling velocities of early (E) and atria (A) waves. Biometric data were analyzed as mean ± standard deviation between the two groups. Multiple regression analysis was performed between serum levels of ferritin as independent variable and testosterone, cortisol, and thyroid hormones.
Results: A total of 82 adult patients with HbSS SCA were enrolled who had a mean age of 21±5.7 years, with 51 males (62%). Patients with SCA compared with the control group had significantly lower hemoglobin, body mass index, cortisol, vitamin D3, testosterone, and T4. Furthermore, there were significantly high levels of reticulocyte count, PTH, TSH, ferritin, LDH, ALP, and uric acid. The incidence of subclinical hypothyroidism and adrenal insufficiency was 7% and 4.8%, respectively, with hypogonadism 9.8% and vitamin D3 deficiency 61%. There were inverse relationships between ferritin as independent variable and serum levels of testosterone, T4, and cortisol, with regression coefficients of –0.49 (P<0.001), –0.33 (P<0.001), and –0.11 (P<0.92), respectively.
Conclusion: Patients with adult SCA had a high prevalence of in vivo hypoadrenialism (4.8%), hypogonadism (9.8%), and hypothyroidism (7%). There were significant inverse relationships between serum ferritin as independent variable and cortisol, testosterone, and T4. Pulsed Doppler echocardiography showed increased LV mass, with a restrictive LV diastolic pattern suggestive of diastolic dysfunction.
Keywords: endocrine disorders, metabolic disorders, sickle-cell anemia, echocardiogram
Introduction
Sickle-cell anemia (SCA) is a hemolytic anemia, characterized by abnormal hemoglobin production of heterozygous (HbAS) or homozygous (HbSS) autosomal-recessive inheritance. Recurrent episodes of hemolytic anemia, vaso-occlusive crises with the entrapment of red blood cells (RBCs) in the microvasculature system cause hypoperfusion infarction, leading to acute or chronic tissue ischemia, and multiorgan dysfunctions due to intermittent small-vascular obstructions.1,2
Endocrine and metabolic dysfunctions are uncommon complications in patients with blood transfusion-dependent blood disorders, such as HbSS SCA, but may be common in β-thalassemia major (β-TM). The endocrine dysfunction may lead to growth retardation and delayed puberty.3 Blood transfusion and RBC destruction leads to iron overload with disruptions of tissue vitalization during vaso-occlusive crisis and inflammatory mediators that mostly cause the metabolic and endocrine dysfunction.4 Adult patients with SCA in the second and third decade of life are expected to have had delayed puberty, short stature, and low weight compared with normal people due to endocrine dysfunction, namely hypoadrenal, hypothyroid, and hypogonadal dysfunction.5
Iron deposition affects adversely the structure and function of myocardium, kidney, liver, parathyroid, thyroid, and adrenal gland.6 In previous reports, patient blood disorders showed variable prevalence of adrenal and thyroid insufficiency in the range of 1%–35%, depending on the age of the study population, duration of blood transfusions, the level of serum ferritin, and the dose of iron-chelating agent.7–9
Myocardial involvement in SCA shows variable abnormalities depending on the patient’s disease severity and age.10 Left ventricular (LV) diastolic function on pulsed Doppler echocardiography showed abnormal diastolic dysfunction that had been classified into three patterns – abnormal relaxation, pseudonormal, and restrictive – depending on the ratio of LV early diastolic velocity (E wave) and late filling (A wave), in addition to deceleration time (DT) of the E wave.11 The restrictive pattern is characterized by high E-wave velocity, a diminished A wave, short DT, and a very high E:A ratio >1.8, while the abnormal relaxation pattern had a high A wave and diminished E wave, prolonged DT, and E:A <1.12,13
In this current study, we aimed: 1) to determine the frequency and risk factors of metabolic and endocrine abnormalities in growth development, puberty, thyroid, adrenal, and bone metabolism in adult patients with SCA; 2) to study the relationships of serum levels of cortisol, free thyroxine (T4), and testosterone with serum ferritin; and 3) to study LV systolic and diastolic functions compared with patients with no SCA.
Materials and methods
The study included 82 patients with adult HbSS SCA. The study was conducted over 12 months from January 2013 to January 2014. Patients’ selection was consecutive from those patients who are on regular follow-up in the hematology clinic at Salmaniya Medical Complex (SMC) in Bahrain. Another 82 healthy individuals with no SCA were also evaluated.
Patient selection for the control group was from those who were referred for assessment of blood disorder but proved to be healthy and negative for blood tests of SCA and other blood disorders, such as thalassemia and G6PD deficiency. Constitutional approval from Salmaniya Medical Complex Ethics Committee was obtained for the study, and every patient signed a consent form before enrollment.
Inclusion/exclusion criteria
Each adult (>12–45 years) patient with steady-state SCA had blood samples withdrawn for metabolic and hormonal assays at the end of third week prior to any blood transfusion. Echocardiography was performed for myocardial function assessment. Blood tests were made for hemoglobin electrophoresis and for solubility screening test for sickling. Patients were defined to be in a steady state if they had no history of blood transfusion during the last 4 months, no history of intercurrent illness, such as infection or inflammation, during the last 4 weeks, and no treatment with medications, such as antibiotics, that may have affected the blood counts during the last 3 weeks. Patients were excluded if they had advanced heart failure, severe liver disease, renal failure with creatinine clearance <30% of normal, had had a blood transfusion within 3 weeks prior to study entry, or had had a vaso-occlusive crisis within the last 4 weeks.
Clinical and biochemical variables
Each patient in the study had a recorded history of onset of menarche, appearance of secondary sexual character, current medications, including the use of hydroxyurea or deferoxamine, and frequency of blood transfusions. Clinical and hematological data and clinical examination of blood pressure, heart rate, presence or absence of pubic and auxiliary hair, breast development in females, and presence of cardiac murmurs on cardiovascular auscultation were also recorded.
Height and weight were recorded, along with calculated body mass index (BMI) and body surface area. Blood samples were taken for levels of hemoglobin, reticulocyte count, serum ferritin, morning cortisol hormone, parathyroid hormone (PTH), thyroid-stimulating hormone (TSH), free T4, corrected calcium, vitamin D3, uric acid, ALP, LDH, potassium, sodium, and estimated glomerular filtration rate. The corrected calcium level was obtained by an increase in calcium by 0.1 mmol/L for each 5 g reduction of albumin below 40 gm/L.
PTH, TSH, free T4, cortisol, and testosterone levels were analyzed using chemiluminescence immunoassay (Medsinglong Medical Equipment, Guangzhou, China). The normal range for different hormones at SMC is as follows: PTH 1–6.5 pmol/L, morning cortisol 190–690 nmol/L, TSH 0.2–4.5 mU/L, free T4 9–21 pmol/L, testosterone in adult males 10–30 nmol/L and adult females 0.4–3 nmol/L, and calcium 2.1–2.6 mmol/L. World Health Organization (WHO), defined vitamin D3 level in serum as insufficient if serum level <20 ng/mL (50 nmol/L) and deficient if level <30 nmol/L.14
Echocardiography
Each patient in the study had an echocardiography examination by 2.5–5 MHz transducer, with an HP E33. The echocardiography tests were performed by a technologist who was blinded to the clinical condition of the patient. Data were reported as an average of at least five cardiac cycles. Another technician analyzed the data blindly, and the data were taken as an average of the two readings. All measurements were conducted according to the recommendations of the American Society of Echocardiography.15
Each patient had echocardiographic measurements of M-mode, 2-D echo, and LV diastolic filling velocity. M-mode echo parameters, including LV septal wall thickness, posterior LV-wall thickness, mid-LV-cavity dimension in the systole and diastole, and LV ejection-fraction percentage (LVEF%) were measured using the apical biplane-modified Simpson’s rule.16 Pulsed Doppler sectors were obtained in the apical view while patients were in the partial left lateral decubitus position during the end of expiration. LV mass was measured using a formula from Devereux et al.17
Statistical analysis
All data were entered and analyzed using SPSS version 20. Data are presented as mean ± standard deviation. The Mann–Whitney U test was used to analyze the differences between the blood levels of different hormones and metabolic markers and echo variables of M mode and pulsed Doppler in the control and SCA groups. Correlations were assessed among serum levels of testosterone, cortisol, and free T4 as dependent variables and ferritin as the independent variable. Differences between patients’ data were considered statistically significant at a probability value of <0.05.
Results
A total of 82 patients with adult SCA were enrolled, with mean age 21.2±5.7 (12–45) years and 51 (62%) males. They were compared with an age- and sex-matched control group with no SCA. Medication of patients with SCA (n=82) was as follows: two patients were using deferoxamine mesylate intravenous infusion as a chelating agent for blood ferritin level >1,000 μg/L; use of oral hydroxyurea at dose of 15mg/kg daily was noted in 25 patients; and frequency of blood transfusion was once monthly in 56 patients, with the rest receiving transfusions during vaso-occlusive crises.
The demographic and biochemical data of all SCA patients and the healthy control group are summarized in Table 1. The SCA patients matched the control group in age and sex, with a higher preponderance of males of 62% in both groups. SCA patients had significantly lower body surface area and BMI compared with control patients of 1.19±0.01 versus 1.53±0.03 (P<0.01) and 20.2±1.5 versus 26.4±2.7 (P<0.001), respectively. Also, there were significantly lower hemoglobin levels and estimated glomerular filtration rates. The mean difference between the serum level of potassium and sodium was of no statistical significance. There were significantly higher reticulocyte percentage and LDH in SCA patients compared with control group. Table 2 shows the hemodynamic parameters of patients with SCA. Patients with SCA had significantly higher heart rate and diastolic blood pressure compared with the control group, but had no difference in systolic blood pressure. Table 3 shows the hormonal and metabolite levels in SCA patients compared with the control group. Serum ferritin and uric acid levels were significantly higher in the SCA group compared with the control group: 537.87±141.1 versus 220±56 μg/L (P<0.01) and 490.6±141.1 versus 275.09±79.5 (P<0.001), respectively. There were only eight patients with ferritin above 1,000 ng/ml and ten patients with hyperuricemia of >420 μmol/L.
 | Table 1 Demographic characteristics of SCA patients (n=82) and the control group (n=82) Notes: Data presented as mean ± standard deviation; P<0.05 considered statistically significant. Abbreviations: BSA, body surface area; eGFR, estimated glomerular filtration rate; LDH, lactate dehydrogenase; RBCs, red blood cells; SCA, sickle-cell anemia. |
 | Table 2 Hemodynamic parameters in SCA patients and the control group Note: Data presented as mean ± standard deviation. Abbreviation: SCA, sickle-cell anemia. |
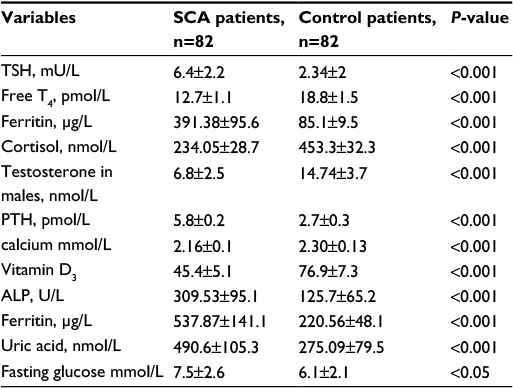 | Table 3 Hormonal and metabolic variables in SCA patients (n=82) and the control group (n=82) Notes: Data presented as mean ± standard deviation; P<0.05 considered statistically significant. Abbreviations: ALP, alkaline phosphatase; PTH, parathyroid hormone; SCA, sickle-cell anemia; T4, thyroxine; TSH, thyroid-stimulating hormone. |
The mean serum level of cortisol was low in SCA compared with the control group, but only four (4.8%) patients had morning cortisol of <190 nmol/L. PTH was significantly high compared with control; however, vitamin D3 was <50 nmol/L in 48 (58%) patients in the SCA group, but 15 (18%) patients in the control group. A further 34 patients with SCA had a normal vitamin level D3 >50 nmol/L, and among those PTH was lower than normal (<1 pmol/L) in three (8.8%) patients only. Furthermore, serum calcium levels were significantly low in the SCA group (2.16 vs 2.3 mmol/L, P<0.01). Mean free T4 was low (12.7 vs 18.8 pmol/L, P<0.001) and patients with T4 <9 pmol/L numbered six (7%). Testosterone levels in males with SCA were 8.8 versus 14.7 nmol/L (P<0.001), with a serum level <10 nmol/L detected in five of 51 (9.8%) patients.
In this study, there were 21 (41%) male patients with a history of delayed onset of puberty by 2–3 years compared with two (2%) males in the control group, and similarly breast development and menarche were both delayed by 2–3 years in 12 (38%) females. There were 21 (41%) male patients who gave a history of delayed onset of puberty of age 14–16 years (2–3 years delayed) compared with males in the control group of 12–13 years. Delayed breast development and age of menarche to 15 years was observed in 12 (38%) females. ALP was significantly higher in the SCA group (309.53 versus 125.7, P<0.01) than the control group.
The serum level of uric acid was significantly higher in the SCA group, with more than ten (12%) patients with uric acid above 420 nmol/L. The mean level of fasting sugar in the SCA group showed significantly higher mean of 7.5 vs 6.1 mmol/L compared with controls, but only 13 (15.8%) patients had serum levels above 7 mmol/l in the SCA group compared with eleven (13.4%) in the control group. Multiple regression analysis between ferritin levels as the independent variable in relation to other dependent variables, such as cortisol, free T4, and testosterone hormones, showed inverse relationships with serum ferritin, with coefficients of –0.49 (P<0.001) for testosterone, –0.33 (P<0.001) for free T4, and –0.11 (P=0.92) for cortisol level.
Table 4 shows the echocardiographic results in both groups. The M-mode measurements in the SCA group showed significantly thicker LV interventricular septa and posterior walls. Further, the LV-cavity dimensions at the end of the systole and diastole were not dilated to any significant extent compared the with control group. LV mass was significantly higher in the SCA group compared with the control group (105.4±5.9 vs 83.3±4.8, respectively; P<0.01).
 | Table 4 Echocardiographic variables of M-mode and pulsed Doppler of LV in SCA patients (n=82) and controls (n=82) Notes: Data presented as mean ± standard deviation; P<0.05 considered statistically significant. Abbreviations: DT, deceleration time; E, early; A, atrial; IVS, interventricular septum; LVEDD, left ventricle end-diastolic dimension; LVESD, left ventricle end-systole dimensions; LVEF, left ventricle ejection fraction; PW, posterior wall; SCA, sickle-cell anemia. |
LVEF% in the systole was normal (56.9 ±5.5 vs 58.4±4.2, P<0.28). Left atrial area was significantly larger in the SCA group compared with the control group. In SCA patients, pulsed Doppler velocities of the LV in the diastole showed a restrictive pattern in 48 (59%) patients versus 23 (28%) in the control group; 20 (24%) patients had an abnormal relaxation pattern versus nine (11%) in the control group, and 14 (17%) patients had pseudonormal filling versus none in the control group. In the control group, there were 50 (61%) patients who had a normal LV diastolic filling pattern. In patients with SCA, mild mitral regurgitation was observed in eight and three had mild aortic regurgitation, with none in the control group.
Discussion
In this study, adult patients with steady-state SCA compared with a control group showed a significant increment in heart rate and lower diastolic blood pressure. Also, hemoglobin was lower with higher reticulocyte percentage and higher LDH. These findings may be explained by chronic anemia status and chronic RBC hemolysis.18,19
Endocrine dysfunction in iron-overload subjects was reported by Fung et al20 to be higher in thalssemia patient compared with SCA, where ratio of DM was 13% vs 2%, hypogonadism of 40% vs 4%, hypothyrodism 10 vs 2%, and growth failure of 33 vs 7%, respectively. Multivariate analysis indicated that endocrinopathy was more likely in β-TM than SCA (odds ratio 9.4, P<0.001), with duration of chronic transfusion a significant predictor (odds ratio 1.4 per 10 years of transfusion, P=0.04).20 The duration of disease requiring transfusion therapy and more than eight transfusions per year are predictors of iron overload. Therefore, SCA patients are at greater risk of endocrine dysfunction.21
The incidence of in vivo adrenal insufficiency in this study was 4.8% with morning cortisol of <190 nmol/L. In one report by Osifo et al, the mean plasma cortisol level in HbSS steady-state SCA patients was significantly lower than patients with no SCA; however, only 8% of SCA patients had plasma cortisol below the normal range.22 In another report, basal plasma cortisol levels were lower in children with the HbSS genotype compared with those of other genotypes.4 Iron overload-induced endocrinopathy with vaso-occlusion and ischemia have been considered potential causes of adrenal insufficiency in SCA patients, but the normal potassium level in adult SCA patients in this study may suggest that adrenal insufficiency is secondary to hypothalamic–pituitary–adrenal axis dysfunction, rather than primary adrenal disease.
In vivo thyroid dysfunction in this study showed 7% incidence of hypothyroidism, with low free T4 and high TSH levels. These biochemical findings are in keeping with previous reports on the development of hypothyroidism in patients with SCA.23,24 Male patients with HbSS SCA have significantly lower endogenous T3 and higher TSH levels than those without.9
Hypogonadism is one of the most prevalent endocrinopathies in subjects with SCA. Male patients with SCA frequently present with eunuchoid body habitus, absent or diminished secondary sexual characteristics, and small testicles. Biochemical studies have demonstrated low levels of testosterone and dihydrotestosterone and variable levels of follicle-stimulating hormone and luteinizing hormone.25,26
In the current study, there were 21 of 51 (41%) male patients who gave a history of delayed onset of puberty to age of 14–16 years (2–3 years delayed) compared with males in the control group (puberty onset at 12–13 years). Delayed breast development and menarche to age of 15 years was observed in 12 of 31 (38%) females. Testosterone levels <6 nmol/L were observed in 9.8% of male patients with SCA. This is in agreement with other studies where puberty has been found to have been delayed approximately 2 years in both boys and girls with SCA, resulting in delayed onset of puberty to the early and mid-teen years of adolescent patients with SCA, and also delayed onset of puberty, breast development, and menarche by 2–3 years.20,27
The etiology for hypogonadism in SCA is unclear, but several causes have been proposed, including primary testicular failure, hypothalamic and/or pituitary dysfunction, and constitutional delay of puberty.28 Episodes of intravascular sickling, vaso-occlusion, infarction, and hypoxia associated with chronic anemia are responsible for testicular failure in SCA.29
BMI was low in the control group (20.2 vs 26.4), with four patients below two standard deviations of 17.2 (4.8%). This is in agreement with other reports, where children with SCA had significantly decreased height, weight, and BMI when compared with healthy control subjects of comparable age, sex, and ethnicity.30,31 Reasons for decreased growth are multifactorial, with contributions from abnormal endocrine function32 and suboptimal nutrition.24
Significant hypocalcemia was observed in SCA patients, with 19% <2.1 mmol/L, and vitamin D3 was low (<50 nmol/L) in 62% of patients with SCA. These findings are in keeping with one study, where vitamin D3 deficiency was noted with high levels of PTH.9 Another report by showed patients with SCA had low calcium and vitamin D3 (below the normal range) in 14% and 12%, respectively, with PTH significantly higher (31% with values above normal range).33 A possible cause of hypocalcemia and vitamin D3 deficiency is impaired intestinal absorption of calcium and vitamin D, leading to the disturbed calcium metabolism seen in SCA.33,34
Uric acid was high in patients with SCA compared with controls, with 12 patients >420 nmol/L; however, in vivo high uric acid level was associated with clinical gouty arthritis in four patients only. In a previous report, patients with SCA showed high prevalence of hyperuricemia at the beginning of childhood. The initial event in the development of hyperuricemia is presumably increased synthesis of nucleic acids occurring as part of the erythropoietic response to hemolysis.35
Echocardiography and pulsed Doppler results in adult SCA patients showed a significant increase in LV mass with no dilation of LV, but enlarged LA and restrictive pattern of diastolic filling detected in 73% of patients with SCA. Recent studies using standard pulsed Doppler parameters have shown that diastolic dysfunction is common in children with SCA.36–38 Another study showed diastolic dysfunction to be an independent risk factor for mortality in SCA, whereby a low E:A ratio, was associated with mortality, with a risk ratio of 3.5 (95% confidence interval 1.5–8.4, P<0.001).39
Yaprak et al40 demonstrated that β-TM patients had significantly higher E-wave velocity, high E:A ratio, and lower A-wave velocity indicating a restrictive pattern in 54% in the study population. Similar findings were reported by Spirito et al,41 who demonstrated a restrictive pattern in 32 patients with β-TM where the rate of deceleration of flow velocity after the early diastolic peak (E) and the ratio between the early and late (A) peaks of flow velocity were increased (1,050±325 vs 762±193 cm/s2 and 2.7±0.7 vs 2.2±0.5, respectively; P<0.001). In this study, LVEF% was normal, indicating that SCA patients had preserved systolic function, but serum ferritin was 2.5 times higher in the SCA group compared with controls. These findings confirm previous reports that iron overload appears to mediate impaired diastolic function, leading to stiffness of the myocardial wall but with well-preserved LV systolic function with no heart failure.38,42 There were inverse linear relationships between serum ferritin as the independent variable and serum levels of cortisol, testosterone, and T4, which highlight the importance of reducing ferritin levels by chelating agents in patients with blood transfusion-dependent hemolytic anemia.
Limitations
In this study, the small number of patients invite assumptive rather than firm conclusions about metabolic abnormalities. Also, hormonal assay of pituitary gland releasing hormones was not done to help differentiate between primary and secondary endocrine dysfunctions. However, the hormonal abnormalities and echo-pulsed Doppler findings in the current study invite another larger trial including assessment of pituitary trophic hormones and releasing factors, as well as right-ventricle function.
Conclusion
Patients with adult SCA had high prevalence of subclinical hypoadrenialism of 4.8%, hypogonadism of 9.8%, and hypothyroidism of 7%. There were significant inverse relationships between serum ferritin as the independent variable and cortisol, testosterone, and T4. Pulsed Doppler echocardiography showed increased LV mass, with restrictive LV diastolic patterns suggestive of diastolic dysfunction.
Disclosure
The authors report no conflicts of interest in this work.
References
Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376(9757):2018–2031. | ||
Smiley D, Dagogo-Jack S, Umpierrez G. Therapy insight: metabolic and endocrine disorders in sickle cell disease. Nat Clin Pract Endocrinol Metab. 2008;4(2):102–109. | ||
Chatterjee R, Katz M. Reversible hypogonadotrophic hypogonadism in sexually infantile male thalassaemic patients with transfusional iron overload. Clin Endocrinol (Oxf). 2000;53(1):33–42. | ||
el-Hazmi MA, Bahakim HM, al-Fawaz I. Endocrine functions in sickle cell anaemia patients. J Trop Pediatr. 1992;38(6):307–313. | ||
Toumba M, Sergis A, Kanaris C, Skordis N. Endocrine complications in patients with thalassaemia major. Pediatr Endocrinol Rev. 2007;5(2):642–648. | ||
el-Hazmi MA, Warsy AS, al-Fawaz I. Iron-endocrine pattern in patients with β-thalassaemia. J Trop Pediatr. 1994;40(4):219–224. | ||
Elsedfy HH, El Kholy M, Tarif R, Hamed A, Elalfy M. Adrenal function in thalassemia major adolescents. Pediatr Endocrinol Rev. 2011;8 Suppl 2:295–299. | ||
Kwan EY, Lee AC, Li AM, et al. A cross-sectional study of growth, puberty and endocrine function in patients with thalassaemia major in Hong Kong. J Paediatr Child Health. 1995;31(2):83–87. | ||
Ozen S, Unal S, Erçetin N, Taşdelen B. Frequency and risk factors of endocrine complications in Turkish children and adolescents with sickle cell anemia. Turk J Haematol. 2013;30(1):25–31. | ||
Gladwin MT, Sachdev V. Cardiovascular abnormalities in sickle cell disease. J Am Coll Cardiol. 2012;59(13):1123–1133. | ||
Nishimura RA, Schwartz RS, Tajik AJ, Holmes DR Jr. Noninvasive measurement of rate of left ventricular relaxation by Doppler echocardiography: validation with simultaneous cardiac catheterization. Circulation. 1993;88(1):146–155. | ||
Aessopos A, Deftereos S, Tsironi M, et al. Predictive echo-Doppler indices of left ventricular impairment in B-thalassemic patients. Ann Hematol. 2007;86(6):429–434. | ||
Choong CY, Herrmann HC, Weyman AE, Fifer MA. Preload dependence of Doppler-derived indexes of left ventricular diastolic function in humans. J Am Coll Cardiol. 1987;10(4):800–808. | ||
[No authors listed]. Prevention and management of osteoporosis. World Health Organ Tech Rep Ser. 2003;921:1–164. | ||
Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978;58(6):1072–1083. | ||
Vandenbossche JL, Kramer BL, Massie BM, Morris DL, Karliner JS. Two-dimensional echocardiographic evaluation of the size, function and shape of the left ventricle in chronic aortic regurgitation: comparison with radionuclide angiography. J Am Coll Cardiol. 1984;4(6):1195–1206. | ||
Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57(6):450–458. | ||
Ballas SK. Lactate dehydrogenase and hemolysis in sickle cell disease. Blood. 2013;121(1):243–244. | ||
Kato GJ, McGowan V, Machado RF, et al. Lactate dehydrogenase as a biomarker of hemolysis-associated nitric oxide resistance, priapism, leg ulceration, pulmonary hypertension, and death in patients with sickle cell disease. Blood. 2006;107(6):2279–2285. | ||
Fung EB, Harmatz PR, Lee PD, et al. Increased prevalence of iron-overload associated endocrinopathy in thalassaemia versus sickle-cell disease. Br J Haematol. 2006;135(4):574–582. | ||
Alustiza JM, Castiella A, De Juan MD, Emparanza JI, Artetxe J, Uranga M. Iron overload in the liver diagnostic and quantification. Eur J Radiol. 2007;61(3):499–506. | ||
Osifo BO, Lukanmbi FA, Adekile A. Plasma cortisol in sickle cell disease. Acta Haematol. 1988;79(1):44–45. | ||
Phillips G Jr, Becker B, Keller VA, Hartman J. Hypothyroidism in adults with sickle cell anemia. Am J Med. 1992;92(5):567–570. | ||
Prasad AS. Malnutrition in sickle cell disease patients. Am J Clin Nutr. 1997;66(2):423–424. | ||
Li M, Fogarty J, Whitney KD, Stone P. Repeated testicular infarction in a patient with sickle cell disease: a possible mechanism for testicular failure. Urology. 2003;62(3):551. | ||
Modebe O, Ezeh UO. Effect of age on testicular function in adult males with sickle cell anemia. Fertil Steril. 1995;63(4):907–912. | ||
Balgir RS. Age at menarche and first conception in sickle cell hemoglobinopathy. Indian Pediatr. 1994;31(7):827–832. | ||
Taddesse A, Woldie IL, Khana P, et al. Hypogonadism in patients with sickle cell disease: central or peripheral? Acta Haematol. 2012;128(2):65–68. | ||
Abbasi AA, Prasad AS, Ortega J, Congco E, Oberleas D. Gonadal function abnormalities in sickle cell anemia: studies in adult male patients. Ann Intern Med. Nov 1976;85(5):601–605. | ||
Oerter KE, Kamp GA, Munson PJ, Nienhuis AW, Cassorla FG, Manasco PK. Multiple hormone deficiencies in children with hemochromatosis. J Clin Endocrinol Metab. 1993;76(2):357–361. | ||
Thomas PW, Singhal A, Hemmings-Kelly M, Serjeant GR. Height and weight reference curves for homozygous sickle cell disease. Arch Dis Child. 2000;82(3):204–208. | ||
Reed JD, Redding-Lallinger R, Orringer EP. Nutrition and sickle cell disease. Am J Hematol. 1987;24(4):441–455. | ||
Mohammed S, Addae S, Suleiman S, et al. Serum calcium, parathyroid hormone, and vitamin D status in children and young adults with sickle cell disease. Ann Clin Biochem. 1993;30(Pt 1):45–51. | ||
Nolan VG, Nottage KA, Cole EW, Hankins JS, Gurney JG. Prevalence of vitamin D deficiency in sickle cell disease: a systematic review. PloS One. 2015;10(3):e0119908. | ||
Reynolds MD. Gout and hyperuricemia associated with sickle-cell anemia. Semin Arthritis Rheum. 1983;12(4):404–413. | ||
Caldas MC, Meira ZA, Barbosa MM. Evaluation of 107 patients with sickle cell anemia through tissue Doppler and myocardial performance index. J Am Soc Echocardiogr. 2008;21(10):1163–1167. | ||
Hankins JS, McCarville MB, Hillenbrand CM, et al. Ventricular diastolic dysfunction in sickle cell anemia is common but not associated with myocardial iron deposition. Pediatr Blood Cancer. 2010;55(3):495–500. | ||
Gujja P, Rosing DR, Tripodi DJ, Shizukuda Y. Iron overload cardiomyopathy: better understanding of an increasing disorder. J Am Coll Cardiol. 2010;56(13):1001–1012. | ||
Sachdev V, Machado RF, Shizukuda Y, et al. Diastolic dysfunction is an independent risk factor for death in patients with sickle cell disease. J Am Coll Cardiol. 2007;49(4):472–479. | ||
Yaprak I, Akşit S, Oztürk C, Bakiler AR, Dorak C, Türker M. Left ventricular diastolic abnormalities in children with β-thalassemia major: a Doppler echocardiographic study. Turk J Pediatr. 1998;40(2):201–209. | ||
Spirito P, Lupi G, Melevendi C, Vecchio C. Restrictive diastolic abnormalities identified by Doppler echocardiography in patients with thalassemia major. Circulation. 1990;82(1):88–94. | ||
Gerry JL, Baird MG, Fortuin NJ. Evaluation of left ventricular function in patients with sickle cell anemia. Am J Med. 1976;60(7):968–972. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.