Back to Journals » Psychology Research and Behavior Management » Volume 15
Homework in Cognitive Behavioral Supervision: Theoretical Background and Clinical Application
Authors Prasko J ![]() , Krone I
, Krone I ![]() , Burkauskas J, Vanek J
, Burkauskas J, Vanek J ![]() , Abeltina M, Juskiene A, Sollar T
, Abeltina M, Juskiene A, Sollar T ![]() , Bite I, Slepecky M, Ociskova M
, Bite I, Slepecky M, Ociskova M ![]()
Received 18 July 2022
Accepted for publication 5 December 2022
Published 22 December 2022 Volume 2022:15 Pages 3809—3824
DOI https://doi.org/10.2147/PRBM.S382246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Jan Prasko,1– 4 Ilona Krone,5 Julius Burkauskas,6 Jakub Vanek,1 Marija Abeltina,7 Alicja Juskiene,6 Tomas Sollar,2 Ieva Bite,7 Milos Slepecky,2 Marie Ociskova1,4
1Department of Psychiatry, University Hospital Olomouc, Faculty of Medicine, Palacky University in Olomouc, Olomouc, The Czech Republic; 2Department of Psychology Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University in Nitra, Nitra, The Slovak Republic; 3Department of Psychotherapy, Institute for Postgraduate Training in Health Care, Prague, The Czech Republic; 4Jessenia Inc. - Rehabilitation Hospital Beroun, Akeso Holding, Beroun, The Czech Republic; 5Riga`s Stradins University, Riga, Latvia; 6Laboratory of Behavioral Medicine, Neuroscience Institute, Lithuanian University of Health Sciences, Kaunas, Lithuania; 7University of Latvia, Latvian Association of CBT, Riga, Latvia
Correspondence: Jan Prasko, Department of Psychiatry, Faculty of Medicine and Dentistry, Palacky University Olomouc, University Hospital, I. P. Pavlova 6, Olomouc, 77520, The Czech Republic, Tel +420 603 414 930, Email [email protected]
Abstract: The homework aims to generalize the patient’s knowledge and encourage practicing skills learned during therapy sessions. Encouraging and facilitating homework is an important part of supervisees in their supervision, and problems with using homework in therapy are a common supervision agenda. Supervisees are encouraged to conceptualize the patient’s lack of homework and promote awareness of their own beliefs and responses to non-cooperation. The supervision focuses on homework twice – first as a part of the supervised therapy and second as a part of the supervision itself. Homework assigned in supervision usually deals with mapping problems, monitoring certain behaviors (mostly communication with the patient), or implementing new behaviors in therapy.
Keywords: supervision, cognitive behavioral therapy, homework, self-reflection
Introduction
The development of competent clinical supervision is crucial to effectively training new CBT therapists and supervisors and maintaining high therapy standards throughout their careers.1 Clinical supervision is a basis for CBT training, but there are only a few empirical evaluations on the effect of supervision on therapists’ competencies. Wilson et al2 in their systematic review and meta-analysis, synthesized the experience and impact of supervision for trainee therapists from 15 qualitative studies. Although supervision leads to feelings of distress and self-doubts, it can effectively support supervisees in personal and professional development. It could similarly harm supervisees’ well-being, clinical work and clients’ experiences. Alfonsson et al3 published a study to evaluate the effects of standardized supervision on rater-assessed competency in six CBT therapists under protocol-based clinical supervision. This is one of the first investigations showing that supervision affects cognitive behavioral competencies. Although several works have studied the effectiveness of supervision on the therapist’s competence and for the therapist’s work with patients in qualitative studies,3–7 there is still a lack of studies that dealt with the importance of homework in supervision.
Homework is a vital element of cognitive behavioral therapy (CBT) which distinguishes it from many other psychotherapeutic approaches.8–10 Patients usually participate in therapy by completing homework assignments and taking responsibility for their course.
Assigning and discussing homework is one of the basic competencies of a cognitive-behavioral therapist and a supervisor in the context of counselling, psychology, therapy, and social work. The manuscript aims to refer to homework in several settings: homework in therapy, supervision of homework in therapy, using the homework by the supervisor for the supervisee, and homework in the training of supervisors.
Homework in Therapy
While specific recommendations for the practical usage of homework have been clearly articulated since the early days of CBT,11,12 practitioners state that they do not follow these recommendations.13–15 For example, many physicians admit that they forget homework or do not focus on standard specifications when, where, how often, and how long the task should last. Often reported non-cooperation in homework assignments may be due to the practice recommendations being too strict or because students think the amount of homework they can assign is limited.16
The Sense of Homework in the Therapy
Patients verify methods and skills they learned during the session in real situations and the natural environment.9,17 Through homework, patients also test hypotheses that emerged during the session with the therapist (for example, “If I went out on the street alone, I would be so weak that I would pass out or lose control completely”). Homework help that the important part of the therapy takes place between sessions and allows the patients to become independent and manage their problems even after the end of therapy.10,18 Patients learn how to raise hypotheses and test them in real-life situations. Through completing homework persistently during the therapy, patients gain skills on how to plan their activities and gain new skills, and they also collect a rich source of therapeutic diaries. The investigations advocate that adding homework to CBT increases its efficacy and that patients who constantly complete homework have better outcomes. The outcomes of four meta-analyses highlight the value of homework in CBT:
- Kazantzis et al10 inspected 14 studies that compared results for patients allocated to CBT without or with homework. The average patient in the homework group reported better results than about 70% of controls.
- Outcomes from 16 studies17 and an updated analysis of 23 studies19 discovered that higher compliance led to better treatment results among patients who received homework projects during therapy.
- Kazantzis et al20 studied the relationships between quantity (15 studies) and quality (3 studies) of the homework to treatment results. The effect sizes were medium to large, and these effects remained fairly constant in a 12-month follow-up.
Therapists strategically create homework to reduce patients’ psychopathology and encourage them to practice skills learned during therapy sessions; nevertheless, non-adherence (between 20% and 50%) remains one of the most cited reasons for decreased CBT efficacy.21 Several reasons for non-adherence to homework might be pointed out –the therapist does not regularly discuss homework with the patient, the patient no longer considers it important and stop doing it.9,22 Discussing homework also allows the therapist to strengthen the patient’s belief in their ability to achieve certain goals.23 The fact that the patient has completed the assignment must be properly acknowledged, and then therapists discuss the quality of homework separately.24 Good questions might be, “How did you do your homework? Were there any difficulties in fulfilling them? What kind?” Furthermore: “How can you handle these problems next time? What did you learn while completing your homework? Can it help you cope with other issues?”
How to Increase the Effectiveness of Homework in the Therapy
Homework is the most effective, and it is most likely to succeed if:19,25
- Follows logically from the topics discussed during the session and uses the methods that the patient learned during the session;
- they are clearly and concretely defined, so it is easy to determine whether or to what extent the patient has been successful in fulfilling them (eg, “Leaving the house alone for at least 30 minutes every day”, not “Starting to go out alone”);
- the patient clearly understands their meaning (“To verify your belief that you will faint on the street” or “See for yourself whether your anxiety will continue to rise, remain the same or subside after a certain time”), and they believe they can achieve the goals;
- homework is formulated so that failure is impossible because, in any case, the patient will learn something useful that will help them in therapy;
- the therapist anticipates and discusses obstacles that could hinder the fulfilment of homework and plans procedures to overcome them.
An important aspect of CBT is the patient’s independence.10,18 Homework is typically determined by consensus. To increase the likelihood that the patient will complete the homework, the patient and the therapist should document their assignments in writing. Additionally, it is very convenient for the patient to record the homework, typically pre-prepared.24 These records serve as a basis for discussing homework in the next session and also allow the therapist to assess the changes achieved during therapy (“A month ago, you were able to go out alone for only half an hour and your anxiety level previously reached level ‘9’, while now you were alone outside for more than an hour and your anxiety do not exceed ‘5’ rated subjectively”).
Because the goal of therapy is to help the patient experience success, the patient’s assigned homework must be feasible.18,26 On the other hand, patients should improve their ability to cope with problems and unpleasant conditions during therapy, they need to exert significant effort to overcome certain unpleasant feelings and emotions.19,20
Even if therapists follow all these rules, they will unavoidably find that sometimes the patient does not complete assigned homework.20,23 In this case, it is required to find out why this happened:
- whether the patient understood what the task was and what it meant
- whether mastering this exercise is important and motivated
- whether unforeseen circumstances prevented them from fulfilling it
- whether the assigned exercise was not very demanding for them in their current mental state
Therefore, therapists do not consider the non-fulfilment of homework a priori as a manifestation of resistance or lack of moral qualities on the patient’s part, then as a problem that must be solved together.
However, if, despite a thorough discussion of homework and agreement on its completion, the patient repeatedly does not even attempt to complete it, does not bring records and fails to justify non-compliance, it is necessary to return to the problem analysis and goal-setting. We need to clarify with the patient whether the problem they are currently dealing with in therapy is really the most important for them, whether the goal they seek to achieve is sufficiently desirable, and whether the therapist offers to achieve is acceptable.9,20
Most practicing CBT therapists report that they use homework and consider homework important for many problems14 and believe in the role of homework in improving therapeutic outcomes.24,27 Encouraging and facilitating homework is a basic skill of a CBT therapist; therefore, it is an important part of supervision.19,20,26 Homework needs to be carefully assigned and discussed (Box 1).
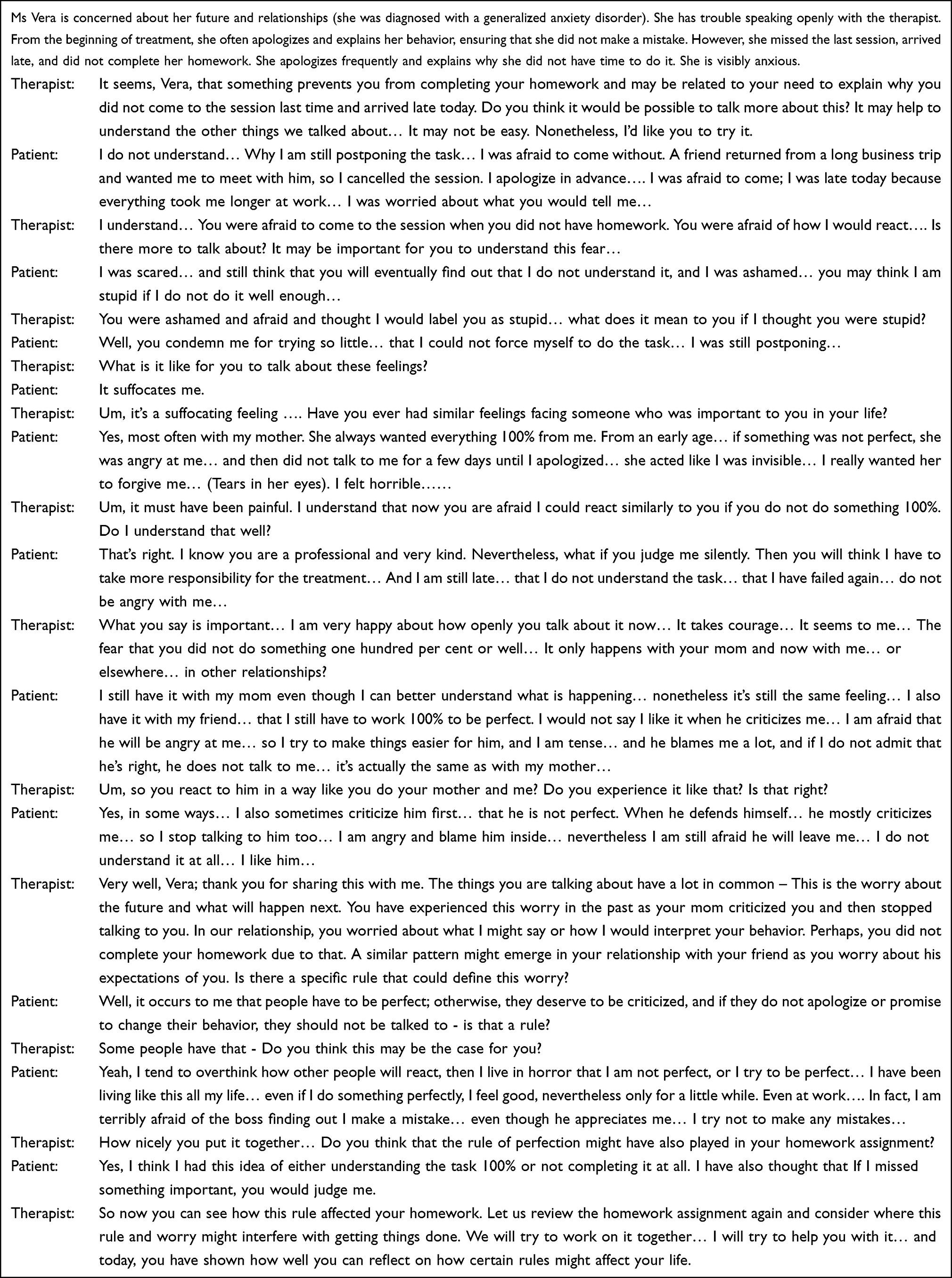 |
Box 1 Case Vignette – Discussion About Not Completing Homework with an Anxious Patient |
Kazantzis et al28 advise examining the therapeutic relationship, which significantly impacts therapy adherence, to better comprehend non-cooperation with homework assignments. Data illustrating the therapist’s homework competence and the therapy outcome29,30 show that the therapist is primarily responsible for their patients’ adhering to or failing to do homework. CBT therapists exhibit many interrelated automatic thoughts, assumptions, and behaviors during sessions that affect homework use in therapy.8,15 In training, common negative attitudes for therapists include: “Homework will make patients feel like school and resent!” “They will feel too controlled and limited!”; “Homework will increase some ps’ sense of vulnerability!”; or “Homework will be even more stressful for stressed patients!” Another widespread belief is that the “structure” of CBT, whose homework is important, reduces spontaneity and worsens the therapeutic relationship.15
In addition, there is some scientific support for these views of therapists’ attitudes toward homework concerning the therapeutic process.31 The result of these attitudes is either a complete avoidance of homework assignments in a way that is not effective and consequently maintains these beliefs.8 For example, common behaviors require supervision, such as rapidly discussing directions at the end of a session, neglecting to repeat homework, or failing to justify while designing homework.9 The CBT Homework Project proposed a practice model29 that emphasizes the importance of therapist beliefs, therapist empowerment, cognitive conceptualization, and the therapeutic relationship in enhancing homework practice.23
Theoretical and empirical support for homework assignments in CBT leads most practicing CBT therapists to at least accept in principle that regular and systematic homework assignments will benefit their patients.8 As a result, CBT therapists favour assigning homework in therapy. However, many beginning therapists encounter problems when they start designing homework (ie, selecting tasks and discussing them with the patient), assigning homework (ie, collaborating on practical aspects of completing homework), and repeating homework in sessions.32 Incorporating homework into therapy is often superficial, hasty, poorly done, or forgotten.16 Therefore, problems with using homework in therapy are a common supervision agenda of practicing CBT therapists.
Personal Training and Self-Reflection of the Therapist as a Supervision Intervention
CBT training students are encouraged to conceptualize the patient’s lack of homework and promote awareness of their own beliefs and responses to non-cooperation in the CBT conceptual framework.8 Suppose the therapist fails to develop this awareness. In that case, errors in clinical judgment may occur, adversely affecting the therapeutic relationship and course of therapy.33 Self-exercise (practicing CBT techniques and interventions as a therapist) and self-reflection (ie, process reflection) are concepts developed by Bennett-Levy et al,34 to operationalize a useful understanding of own processes in working with patients. CBT training students are asked to become accustomed to using self-exercise and self-reflection. In a few qualitative studies, self-exercise and self-reflection have proven to improve the therapist’s self-concept, ie, self-confidence, perceived competence in one’s abilities and belief in the effectiveness of the CBT model.34–36 Calvert et al37 study checked the use of meta-communication in supervision from supervisees’ perspectives using the Metacommunication in Supervision Questionnaire (MSQ). There were differences in the reported frequency with which the different types of meta-communication were used. It appears that meta-communication around difficult or uncomfortable feelings in the supervisory relationship occurs less often than other components of meta-communication.1
Below are examples of self-exercise and self-reflective exercises. The following self-assessment is developed to shape thinking before a preliminary meeting with a supervisor. Earlier knowledge has shown that supervisees and supervisors do not always share common ideas about supervision. Therefore, the supervisee could finish this self-assessment as a homework exercise before supervision. A supervisee might want to identify conversation matters that may enable a supervisor to better comprehend their requirements and needs.
Before Starting
Questions Regarding Previous and Desired Experience in Supervision
What background information do you think your supervisor requires to understand you at the start? (This may include a curriculum vitae noting appropriate previous experience). What would be the best method to convey these details? Is there any distinction between what you desire from this placement and what you feel you need? What background details about this placement and this supervisor do you have? How does this make you feel? Exists any more information that you need? What do you want and expect your supervisor to concentrate on during supervision? What roles do you want your supervisor to play with respect to you and your work? What supervisory media do you want to experience (for example, taped, “live”, or reported)? What do you intend to do about your feelings? Consider how you feel about your supervisor evaluating your work at the end of the positioning process.
More Specific Questions
- What specific activities during supervision do you recall as being helpful?
- What conditions would be most convenient for you?
- What would you personally anticipate getting from being supervised?
- However, what would you want to receive from supervision prepared that will not be on offer?
- What could you do about this?
Several possible tough issues can appear in supervision. The following list includes concerns the supervisee might consider (Table 1).
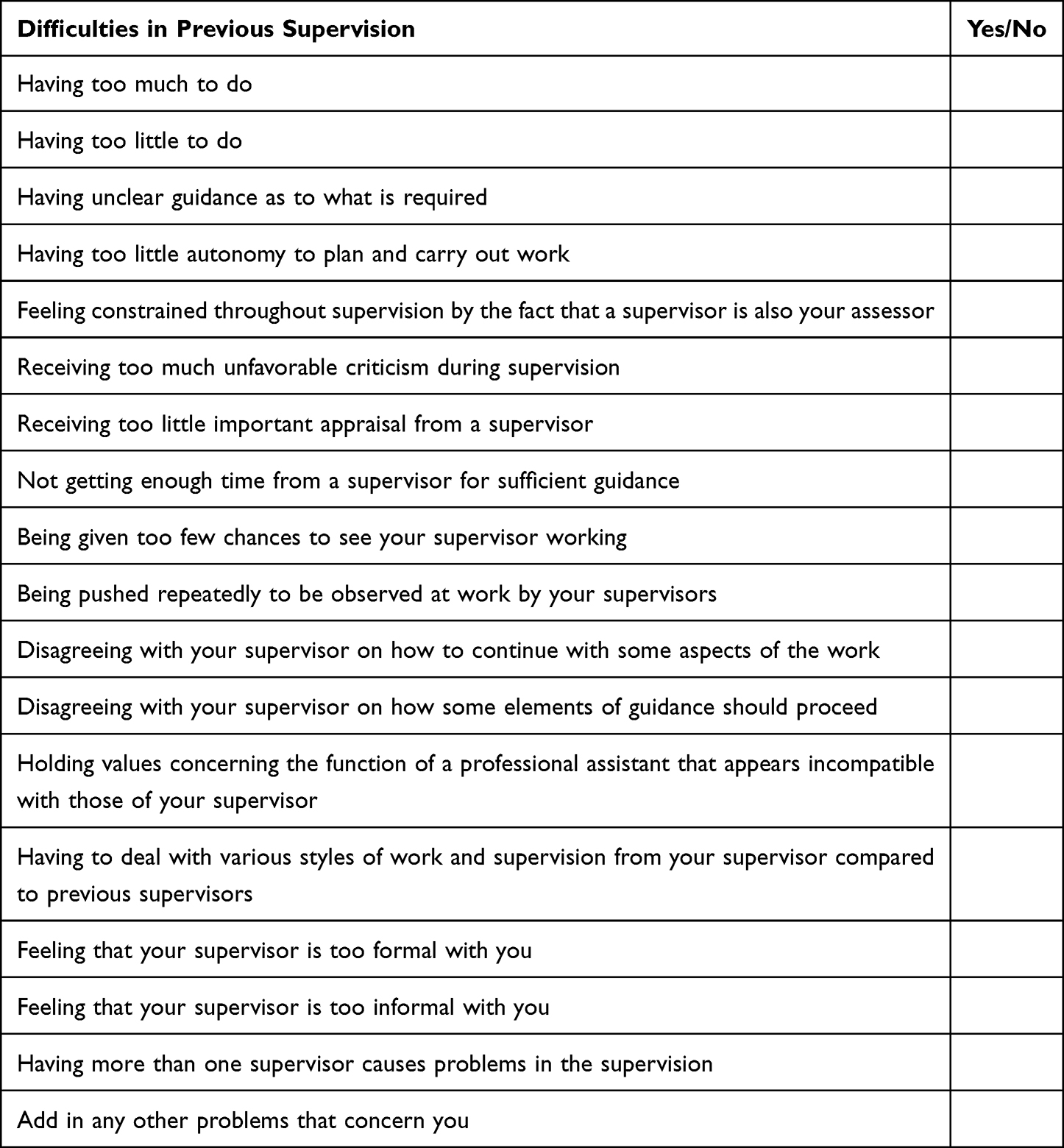 |
Table 1 Difficulties in Previous Supervisions (Adapted According to Scaife 201938) |
In the next step:
- Recognize the two issues which seem to be the most important ones for you.
- What steps can be taken now to minimize the chances that these two concerns will seriously disrupt your cooperation?
Reflection on the Strengths
What are the top three strengths you want your supervisor to uncover as you enter this supervisory relationship?
List 3 points for your development that may or might not be obvious to your supervisor.
Reflection on Difficulties
Therapists regularly discover face-to-face contact with people labelled by society as coming from a specific sub-group.
Which sub-groups make you feel uneasy for whatever reason? Do you want to address this during supervision?38
Examples of Self-Assessment in the Supervision Process
Exploring Sources of Stress from Clinical Work
Check all that resonate for you.39
❑ Perfectionism ❑ Fear of failure ❑ Self-doubt ❑ Need for approval ❑ Emotional depletion ❑ Unhealthy lifestyle
Which of them seems to have the greatest impact on your stress levels?
What supervisor has most regularly identified as weak points in your clinical work?
Processing Mistakes
When mistakes are processed in ways that lead to reflection, flexibility, and adjustments in how you function, it can result in learning and growth.
Consider a patient you are now working with (or have recently worked with) with whom you have experienced a therapeutic failure.
Answer the following questions while keeping this experience in mind:
- What are the signs of a therapeutic failure? How can you be certain that what you are doing is not beneficial on some level? What benefits might your patient derive from failure? When did things begin to deteriorate? Which initiatives have been most effective so far, and which have been least effective? How have you been careless?
- Examine your intervention choices as well as how they were carried out:
- What concerns or considerations did you overlook? What is impeding your ability to be more effective? How has your empathy and compassion for this individual been harmed? How can you use this experience to help you grow?
Reflection of Therapeutics Mastery Skills
Favorite Techniques
- Explain three things you have put off in your career or life because they appear risky—you have something to lose and gain.
- Which therapeutic strategies or interventions stimulate you the most?
- What would you call your “hidden weapon”?
- What kind of patients or presenting difficulties interest you the most?
- What would it take to incorporate more of the pleasure and satisfaction you receive when applying the strategies mentioned earlier into other aspects of your work?39
The following examples from clinical supervision demonstrate how self-exercise and self-reflection can help participants understand their belief system’s impact on homework in CBT.
Supervision of Homework in Therapy
Supervision is classically mandatory for students in cognitive behavioral training and plays a crucial part in therapist development.2 The typical structure of continuous supervision of one patient includes discussing questionnaires or scales used to measure the severity of the problem (like the Beck depression inventory), homework, events in therapy since the last session, and then discussing the agenda of the current supervision meeting (what will be done in the session, which problem will be addressed), work on a selected issue or problems, homework assignment, session summary and its evaluation by the supervisor. The supervision focuses on homework twice – first as a part of the supervised therapy and second as a part of the supervision itself (Box 2).
 |
Box 2 Case Vignette – Discussion About Patient´s Homework During Supervision |
Whether and how the patient completes homework is a common supervisory issue (Box 3). The therapist often complains that the patient refuses to do homework or rarely does it.8,16
 |
Box 3 Case Vignette –Discussion of Setting Homework During Supervision |
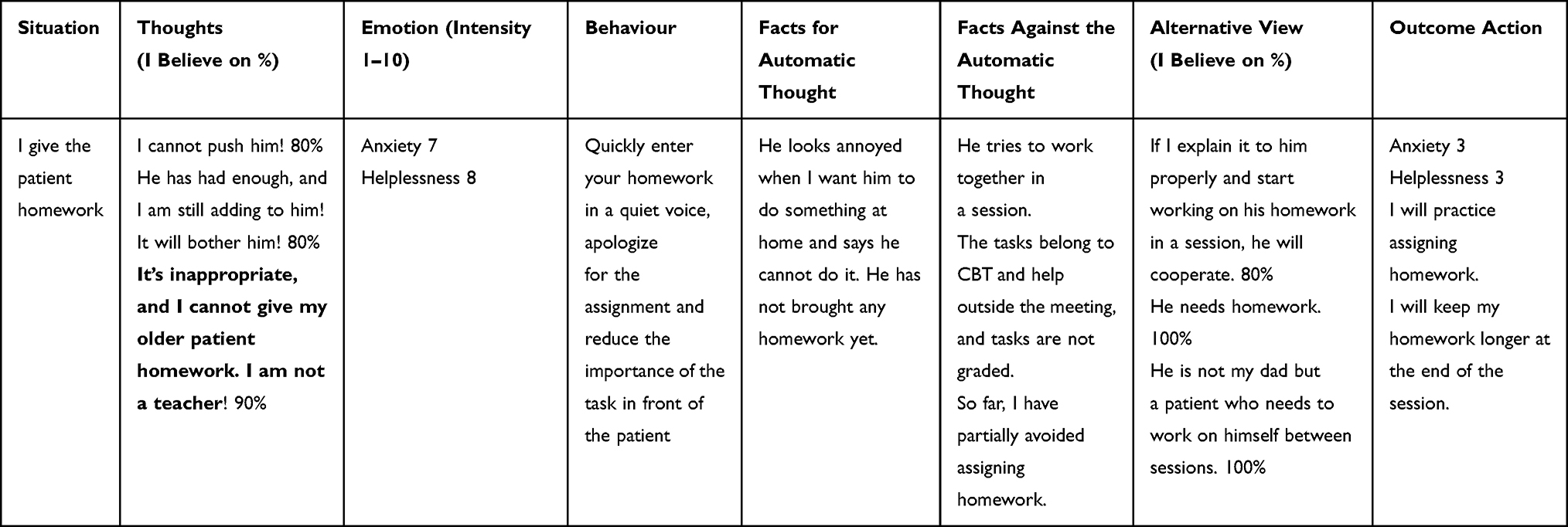 |
Table 2 Recording of Paul’s Automatic Thoughts |
 |
Figure 1 The picture describes the vicious circle of countertransference reaction, where automatic thoughts lead to developing negative emotions, bodily reactions and behaviors. Any vicious circle components can alert the therapists that their countertransference reaction is taking place. |
Homework in Supervision
Homework assignments are a common part of supervisory work. These may involve the patient’s management (eg noticing on their recording how often the therapist strengthens the patient and how and if it is rare to clarify where reinforcement would be appropriate), working on oneself (eg clarifying experiences and attitudes that lead to countertransference in a particular patient, awareness of which other patients may also occur) and theoretical study (the supervisor may advise the therapist to read a professional text that can help better understand and work with the patient).40
The supervisor helps define a specific engagement, discusses specific therapeutic methods, touches on what methods the therapist has used and what else they may consider the role, for the most part, the implementation of strategies whose ability to use in therapy under supervision will be planned, as part of homework.
Homework assigned in supervision usually deals with mapping problems (supplementing the conceptualization of the case, evaluation, vicious circle of the problem with the patient, etc.), monitoring certain behaviors (mostly communication with the patient), or implementing new, behaviors in therapy (usually using therapeutic strategies).12 Homework teaches the supervisee to work on self-reflection outside the supervision meetings.41 Discussing the homework properly at the beginning of the session is important. The mentioned home exercises usually concern the work with the supervised case report of the patient. The basic questions concern homework results, discussing the obstacles in solving them and what the supervisee learned in homework.8 The discussion gives the supervisor case management information and can point to important practice moments.
Homework Assignment
Before the end of the session, the supervisor and the supervisee agree on a homework assignment. It is optimal when homework arises from a problem addressed in the session’s main part.8 At the beginning of supervision, proposals for homework assignments usually come from the supervisor and are discussed and recorded in writing.40 During supervision, the supervisee creates homework assignments, and the content is discussed with the supervisee.
The Meaning of Homework
Homework must make sense for the supervisee; otherwise, he will have no motivation to do it. However, it is also important to make sense of the patient or patients and develop the therapist’s skills and competencies. It is desirable to discuss the meaning of homework in supervision.
Possible Difficulties When Completing Homework
It is advantageous to discuss the anticipated difficulties in completing homework. This has the advantage that the supervisee can prepare for possible difficulties, consider overcoming them and consult with the supervisor. Discussing difficulties helps the supervisee model and later develops the skill to discuss the patient’s homework difficulties.
The Impact of the Therapist’s Belief System
In some therapists, there can be reasons for a more complex level of conceptualization.42 That is important when the therapist repeats certain mistakes even though they have repeatedly discussed them with the supervisor. At a directly accessible level, the situation with the patient can be described using a vicious circle. The deeper “hidden” level refers to the core beliefs and conditional rules activated in a specific situation with the patient.40,43 A supervisor can use the “falling arrow” technique to map core beliefs and conditional assumptions.43
One such way is the Therapeutic Belief System (TBS).44 TBS is a theoretical model useful for understanding the specific beliefs, assumptions, and behaviors that therapists and patients commonly experience that could potentially affect the course of therapy. In line with the cognitive model, TBS provides a framework for identifying therapists’ and patients’ beliefs about themselves, each other, the treatment process, the emotions these beliefs can evoke, and typical behavioral reactions. For example, a therapist may see a patient as an “aggressor”, a “helpless victim”, or a “collaborator”. The participant’s own beliefs may supplement these beliefs about himself, such as “victim”, “co-worker”, “carer”, or “rescuer”. Homework assignments may be perceived by both the therapist and the patient as “hopeless”, “productive”, or simply maintaining the status quo and lead to a different emotional and behavioral response.8 Thus, TBS can be introduced into supervision to guide the supervisee to consider whether he or she identifies with any of the therapists’ typical beliefs and behaviors outlined in the model. A simple awareness of such patterns can be a useful orientation when considering the role of attitudes and beliefs in integrating homework (Box 4).
 |
Box 4 Case Vignette – Discussion About Supervisee Homework |
The scheme broadly refers to mental structures that integrate and give meaning to events.45 Schemes can be positive, negative or neutral. In CBT as a treatment for psychological disorders, we focus on dysfunctional patterns often associated with specific diagnostic presentations (for example, emotional vulnerability patterns are common in anxiety disorders). Schema is generally defined as a ubiquitous topic of cognitive functions, emotions, physiological feelings about oneself, and relations with others.33
Therapists’ schemes run in specific therapies and do not usually signal mental health problems.8 Therapists’ schemes are influenced by the following factors: training experiences, such as supervision and training phase, therapy model, peer group, clinical experience, and personal experience.13,40 Once identified, the therapist’s scheme can be used in supervision as a starting point to discuss some of the practitioner’s views that may interfere with therapy.8 Completing structured questionnaires can identify participants’ schemes, basic beliefs, and assumptions. Some examples of useful questionnaires are the Dysfunctional Attitudes Scale,46 the Personal Faith Questionnaire,47 the Young Schema Questionnaire48 and the Therapists’ Schema Questionnaire.49 Leahy’s Therapists’ Scheme Questionnaire is a relatively straightforward screening technique for identifying therapeutic patterns that could affect a therapeutic relationship. It consists of 46 assumptions related to the 14 most common therapeutic regimens.
Certain schemes are particularly common in CBT supervisees. These include “demanding standards”, “excessive self-sacrifice”, and “special superior person”.49 Training therapists who identify with the “demanding standards” scheme have a somewhat obsessive, perfectionist, and controlling approach to therapy. These therapists usually have high expectations for keeping a patient’s homework and may not realize that non-compliance with homework is often part of the learning process. Therapists may expect that there is a “right” way to complete a homework assignment, leading to feelings of frustration when assignments produce different results. This may signify insecurity and a notion that if things break from the planned structure, the therapist will be exposed as “incompetent”. Many therapists identify with the “excessive self-sacrifice” pattern, the most commonly observed pattern in both novice and experienced therapists.33 Leahy49 proposes that these therapists overstate the importance of their patient relationships. They may fear leaving or feel guilty that they are or feel better than the patient. As a result, the therapist may engage in therapy-defeating behaviors, such as making the homework assignment to the patient’s various needs, having difficulty with appropriate assertiveness in discussing persistent patient non-cooperation, and having a tendency to avoid techniques. Such as exposure or opening of painful memories for fear that the patient will be upset.
Novice therapists who identify with the “special superior person” scheme see the therapeutic situation as an opportunity to achieve excellent results and have high-performance expectations. There may be a tendency for the patient to idealize or, conversely, to devalue or distance himself from patients who do not improve or do their homework. The presence of a “special superior” scheme can be seen as overcompensation in response to “demanding standards” and “excessive self-sacrifice”, which have the thematic connotations of “not being good enough”. The supervision session sets the supervisee in a situation where the supervisor supervises homework through videotaped therapeutic sessions utilizing a cognitive therapy scale (CTS).50 Feelings of superiority and exceptionality can, in some cases, be a way of dealing with the feelings of inferiority that they experience, that their use of homework is judged in this way.
In addition to recognizing the general responses to the scheme that most training students encounter, the supervisor should help the supervisor become aware of his or her idiosyncratic beliefs and coping styles, which some patients may trigger (Box 5). The supervisor should encourage the supervisee to pay special attention to the “overlapping patterns” in which the therapist’s scheme and the patient’s scheme overlap, leading to the over-identification of the therapist with the patient.33
 |
Box 5 Case Vignette – The Supervisor Advises the Therapist to Work with Core Beliefs and Conditional Rules |
Homework in Supervisor Training
For supervisors, their supervisors’ training is important. An important part of this training is the practice of self-reflection, which should be requested directly in the meeting and as homework. It can be a task to capture situations in supervision in which they do not feel comfortable using the vicious circle, cognitive restructuring of automatic negative thoughts in these situations, capturing thoughts, emotions, bodily sensations and behaviors in situations where they are aware that they are experiencing countertransference reactions to the supervised therapist. It is also important that in their homework, they reflect on their concentration level during supervision sessions and consider what supervision skills they have used or what they have learned for the next session. A typical complex homework in supervision training is a video recording of supervision sessions and their analysis. The recorded supervision and analysis are then analyzed in the next supervision training meeting.
Discussion
This article is designed as an overview of views and experiences. Its important element is work samples. This is also a limitation of this article. Assignment of homework in supervision and therapist and supervisor training lacks scientific information about its effectiveness. Nevertheless, assigning homework is an important part of cognitive behavioral therapy. We know quite well about its meaning in prescribing for patients. Less is known about their meaning and effectiveness in supervision. The supervisee encounters problems completing homework assignments for her patients that she brings to the supervisee. Why the patient does not complete the homework may be his problem, but his therapist may also have a part in it his requirements, which include how the homework is assigned, its suitability for the given patient, timing, and complexity. Homework can also belong to the training of supervisors and the supervision of supervision. Here, we do not know any research evidence about their effectiveness in using the most important part of supervision, the patient; however, they are experienced by supervisors and supervisees as useful and meaningful.
Homework in supervision and supervision requires further reflection on their meaning and subsequent research, which should examine their significance for the supervisee’s competence (supervisee) and the ultimate impact on the patient himself.
Conclusion
Homework presents one of the cornerstones of cognitive-behavioral therapy, CB supervision and the training of CBT supervisors. If applied consistently and collaboratively, homework enhances therapeutic outcomes and increases the patient’s self-confidence. Setting and maintaining a fruitful working alliance for homework can be challenging – issues with homework present one of the common reasons to seek a supervisory consultation. Supervision then focuses on examining the specific case and experienced problems, factors in the interaction between the therapist and their patient, and the therapist’s automatic thoughts, schemas, and behaviors that might maintain the issue. There are several ways to address this topic in supervision. Homework is usually part of supervision because of its usefulness. The supervised therapist may be given similar tasks as the patient receives in therapy: to describe the automatic thoughts that occur to him while guiding the patient, to test them and look for a more rational response, to conduct behavioral experiments, to clarify the core beliefs and conditioned assumptions that influence the formation of the therapeutic relationship, experiments with adequate communication with the patient and others. A therapist’s self-experience through practice can help them improve their therapeutic work.
Acknowledgments
This paper was supported by the research grant VEGA no. APVV-15-0502 Psychological, psychophysiological and anthropometric correlates of cardiovascular diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Newman CF. Training cognitive behavioral therapy supervisors: didactics, simulated practice, and “meta-supervision”. J Cogn Psychother. 2013;27(1):5–18. doi:10.1891/0889-8391.27.1.5
2. Wilson HM, Davies JS, Weatherhead S. Trainee therapists’ experiences of supervision during training: a meta-synthesis. Clin Psychol Psychother. 2016;23(4):340–351. doi:10.1002/cpp.1957
3. Alfonsson S, Lundgren T, Andersson G. Clinical supervision in cognitive behavior therapy improves therapists’ competence: a single-case experimental pilot study. Cogn Behav Ther. 2020;49(5):425–438. doi:10.1080/16506073.2020.1737571
4. Coren S, Farber BA. A qualitative investigation of the nature of “informal supervision” among therapists in training. Psychother Res. 2019;29(5):679–690. doi:10.1080/10503307.2017.1408974
5. Odyniec P, Probst T, Margraf J, Willutzki U. Psychotherapist trainees’ professional self-doubt and negative personal reaction: changes during cognitive behavioral therapy and association with patient progress. Psychother Res. 2019;29(1):123–138. doi:10.1080/10503307.2017.1315464
6. Probst T, Jakob M, Kaufmann YM, Müller-Neng JMB, Bohus M, Weck F. Patients’ and therapists’ experiences of general change mechanisms during bug-in-The-eye and delayed video-based supervised cognitive-behavioral therapy. A randomized controlled trial. J Clin Psychol. 2018;74(4):509–522. doi:10.1002/jclp.22519
7. Weck F, Jakob M, Neng JM, Höfling V, Grikscheit F, Bohus M. The effects of bug-in-The-eye supervision on therapeutic alliance and therapist competence in cognitive-behavioral therapy: a randomized controlled trial. Clin Psychol Psychother. 2016;23(5):386–396. doi:10.1002/cpp.1968
8. Haarhoff B, Kazantzis N. How to supervise the use of homework in cognitive behavior therapy: the role of trainee therapist beliefs. Cogn Behav Pract. 2007;14:325–332. doi:10.1016/j.cbpra.2006.08.004
9. Hollon SD, Beck AT. Cognitive and cognitive-behavioral therapies. In: Bergin AE, Garfield SL, editors. Handbook of Psychotherapy and Behavior Change.
10. Kazantzis N, Whittington C, Dattilio F. Meta‐analysis of homework effects in cognitive and behavioral therapy: a replication and extension. Clin Psychol. 2010;17(2):144–156.
11. Beck AT, Rush JA, Shaw BF, Emery G. Cognitive Therapy of Depression. New York: The Guilford Press; 1979.
12. Shelton JL, Levy RL. Behavioral Assignments and Treatment Compliance: A Handbook of Clinical Strategies. Champaign, IL: Research Press; 1981.
13. Kazantzis N, Busch R, Ronan KR, Merrick PL. Using homework assignments in psychotherapy: differences by theoretical orientation and professional training? Behav Cognitive Psychother. 2006;35:121–128. doi:10.1017/S1352465806003328
14. Kazantzis N, Deane FP. Psychologists’ use of homework assignments in clinical practice. Prof Psychol Res Pr. 1999;30:581–585. doi:10.1037/0735-7028.30.6.581
15. Whisman MA, Jacobson NS. Brief behavioral marital therapy. In: Wells RA, Giannetti VJ, editors. Handbook of Brief Psychotherapies. New York: Plenum; 1990:325–349.
16. Kazantzis N, Deane FP, Ronan KR. Assessing compliance with homework assignments: review and recommendations for clinical practice. J Clin Psychol. 2004;60:627–641. doi:10.1002/jclp.10239
17. Kazantzis N, Deane FP, Ronan KR. Homework assignments in cognitive and behavioral therapy: a meta‐analysis. Clin Psychol. 2000;7(2):189–202.
18. Persons JB, Davidson J, Tompkins MA. Essential Components of Cognitive-Behavior Therapy for Depression. Washington, DC: American Psychological Association; 2000.
19. Mausbach BT, Moore R, Roesch S, Cardenas V, Patterson TL. The relationship between homework compliance and therapy outcomes: an updated meta-analysis. Cognit Ther Res. 2010;34(5):429–438. doi:10.1007/s10608-010-9297-z
20. Kazantzis N, Whittington C, Zelencich L, Kyrios M, Norton PJ, Hofmann SG. Quantity and quality of homework compliance: a meta-analysis of relations with outcome in cognitive behavior therapy. Behav Ther. 2016;47(5):755–772. doi:10.1016/j.beth.2016.05.002
21. Tang W, Kreindler D. Supporting homework compliance in cognitive behavioral therapy: essential features of mobile apps. JMIR Ment Health. 2017;4(2):e20. doi:10.2196/mental.5283
22. Freeman A, Davis DD. Cognitive therapy of depression. In: Bellack AS, Hersen M, Kazdin AE, editors. International Handbook of Behavior Modification and Therapy.
23. March P. In two minds about cognitive-behavioral therapy: talking to patients about why they do not do their homework. Br J Psychother. 1997;13:461–472. doi:10.1111/j.1752-0118.1997.tb00332.x
24. Kazantzis N, Dattilio FM, MacEwan J. In pursuit of homework adherence in behavior and cognitive behavior therapy: comment on Malouff and Schutte (2004). Behav Therap. 2005;28:179–183.
25. Fennel MJV. Depression. In: Hawton K, Salkovskis PM, Kirk J, Clark DM, editors. Cognitive Behavior Therapy for Psychiatric Problems. Oxford: Oxford University Press; 1989.
26. Thase M. Cognitive behavior therapy manual for treatment of depressed inpatients. In: Van Hasselt VB, Hersen M, editors. Sourcebook of Psychological Treatment Manuals for Adult Disorders. New York: Plenum; 1996:201–231.
27. Fehm L, Kazantzis N. Attitudes and use of homework assignments in therapy: a survey of German psychotherapists. Clin Psychol Psychother. 2004;11:332–343. doi:10.1002/cpp.419
28. Bryant MJ, Simons AD, Thase ME. Therapist skill and patient variables in homework compliance: controlling an uncontrolled variable in cognitive therapy outcome research. Cognit Ther Res. 1999;23:381–399. doi:10.1023/A:1018703901116
29. Kazantzis N, MacEwan J, Dattilio FM. A guiding model for practice. In: Kazantzis N, L’Abate L, editors. Using Homework Assignments in Cognitive Behavior Therapy. New York: Routledge; 2005b:359–407.
30. Kazantzis N. Therapist competence in cognitive and behavior therapies: review of the contemporary empirical evidence. Behav Change. 2003;20:1–12. doi:10.1375/bech.20.1.1.24845
31. Kazantzis N, Lampropoulos GL, Deane FP. A national survey of practicing psychologists’ use and attitudes towards homework in psychotherapy. J Consult Clin Psychol. 2005a;73:742–748. doi:10.1037/0022-006X.73.4.742
32. Kazantzis N, Lampropoulos GL. Reflecting on homework in psychotherapy: what can we conclude from research and experience? J Clin Psychol. 2002;58:577–585. doi:10.1002/jclp.10034
33. Young JE, Klosko JS, Weishaar ME. Schema Therapy: A Practitioner’s Guide. New York: The Guilford Press; 2003.
34. Bennett-Levy J, Turner F, Beaty T, Smith M, Paterson B, Farmer S. The value of self-practice of cognitive therapy techniques and self-reflection in the training of cognitive therapists. Behav Cognitive Psychother. 2001;29:203–220. doi:10.1017/S1352465801002077
35. Haarhoff BA, Stenhouse LM. “Practice makes perfect”: practicing cognitive behavior therapy techniques and training. Clin Psychol. 2004;14:26–30.
36. Chigwedere C, Bennett-Levy J, Fitzmaurice B, Donohoe G. Personal practice in counselling and CBT trainees: the self-perceived impact of personal therapy and self-practice/self-reflection on personal and professional development. Cogn Behav Ther. 2021;50(5):422–438. doi:10.1080/16506073.2020.1846608
37. Calvert FL, Deane FP, Grenyer BFS. Supervisee perceptions of the use of meta-communication in the supervisory relationship. Psychother Res. 2020;30(2):228–238. doi:10.1080/10503307.2018.1524169
38. Scaife J. Supervision in Clinical Practice: A Practitioner’s Guide. Routledge; 2019.
39. Kottler JA. The Therapist’s Workbook: Self-Assessment, Self-Care, and Self-Improvement Exercises for Mental Health Professionals. John Wiley & Sons; 2011.
40. L’Abate L. A Guide to Self-Help Workbooks for Clinicians and Researchers. Binghamton, NY: Haworth; 2004.
41. Bennett-Levy J. Why therapists should walk the talk: the theoretical and empirical case for personal practice in therapist training and professional development. J Behav Ther Exp Psychiatry. 2019;62:133–145. doi:10.1016/j.jbtep.2018.08.004
42. Persons JB. Cognitive Therapy in Practice: A Case Formulation Approach. New York: Norton; 1989.
43. Beck JS. Cognitive Therapy: Basics and Beyond. New York: The Guilford Press; 1995.
44. Rudd M, Joiner T. Countertransference and the therapeutic relationship: a cognitive perspective. J Cognitive Psychother. 1997;11:231–249. doi:10.1891/0889-8391.11.4.231
45. Beck AT, Freeman A, Davis DD. Cognitive Therapy of Personality Disorders.
46. Weissman AN, Beck AT. Development and validation of the Dysfunctional Attitude Scale: a preliminary investigation.
47. Beck AT, Beck JS. The personality belief questionnaire. In: Unpublished Assessment Instrument. Bala Cynwyd, PA: The Beck Institute for Cognitive Therapy and Research; 1991.
48. Young JE, Brown G. Young Schema Questionnaire.
49. Leahy RL. Overcoming Resistance in Cognitive Therapy. New York: The Guilford Press; 2001.
50. Young J, Beck AT. Cognitive therapy scale: rating manual. (Available from the Beck Institute for Cognitive Therapy and Research, GSB Building, One Belmont Avenue, Suite 700, Bala 1980. Cynwyd, PA 19004-1610); 1980.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.