Back to Journals » Patient Preference and Adherence » Volume 15
Home Care Patients’ Experiences with Home Care Nurses’ Support in Medication Adherence
Authors Dijkstra NE ![]() , Vervloet M
, Vervloet M ![]() , Sino CGM, Heerdink ER
, Sino CGM, Heerdink ER ![]() , Nelissen-Vrancken M, Bleijenberg N, de Bruin M, Schoonhoven L
, Nelissen-Vrancken M, Bleijenberg N, de Bruin M, Schoonhoven L ![]()
Received 19 January 2021
Accepted for publication 9 June 2021
Published 1 September 2021 Volume 2021:15 Pages 1929—1940
DOI https://doi.org/10.2147/PPA.S302818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Nienke E Dijkstra,1,2 Marcia Vervloet,3 Carolien G M Sino,1 Eibert R Heerdink,2,4 Marjorie Nelissen-Vrancken,5 Nienke Bleijenberg,1,6 Marijn de Bruin,7 Lisette Schoonhoven6,8
1Research Group Care for the Chronically Ill, University of Applied Sciences Utrecht, Utrecht, the Netherlands; 2Research Group Innovation in Pharmaceutical Care, University of Applied Sciences Utrecht, Utrecht, the Netherlands; 3Nivel, Netherlands Institute for Health Services Research, Utrecht, the Netherlands; 4Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Utrecht, the Netherlands; 5Dutch Institute for Rational Use of Medicine, Utrecht, the Netherlands; 6Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands; 7IQ Healthcare, Radboud University Medical Centre, Nijmegen, the Netherlands; 8School of Health Sciences, Faculty of Environmental and Life Sciences, University of Southampton, Southhampton, UK
Correspondence: Nienke E Dijkstra
Research Group Proactive Care for Elderly People Living at Home, University of Applied Sciences Utrecht, Heidelberglaan 7, Utrecht, 3584 CS, the Netherlands
Tel +31 641620681
Email [email protected]
Purpose: To describe nurses’ support interventions for medication adherence, and patients’ experiences and desired improvements with this care.
Patients and Methods: A two-phase study was performed, including an analysis of questionnaire data and conducted interviews with members of the care panel of the Netherlands Patients Federation. The questionnaire assessed 14 types of interventions, satisfaction (score 0– 10) with received interventions, needs, experiences, and desired improvements in nurses’ support. Interviews further explored experiences and improvements. Data were analyzed using descriptive statistics and a thematic analysis approach.
Results: Fifty-nine participants completed the questionnaire, and 14 of the 59 participants were interviewed. The satisfaction score for interventions was 7.9 (IQR 7– 9). The most common interventions were: “noticing when I don’t take medication as prescribed” (n = 35), “helping me to find solutions to overcome problems with using medications” (n = 32), “helping me with taking medication” (n = 32), and “explaining the importance of taking medication at the right moment” (n = 32). Fifteen participants missed ≥ 1 of the 14 interventions. Most mentioned the following: “regularly asking about potential problems with medication use” (33%), “regularly discussing whether using medication is going well” (29%), and “explaining the importance of taking medication at the right moment” (27%). Twenty-two participants experienced the following as positive: improved self-management of adequate medication taking, a professional patient–nurse relationship to discuss adherence problems, and nurses’ proactive attitude to arrange practical support for medication use. Thirteen patients experienced the following as negative: insufficient timing of home visits, rushed appearance of nurses, and insufficient expertise about side effects and taking medication. Suggested improvements included performing home visits on time, more time for providing support in medication use, and more expertise about side effects and administering medication.
Conclusion: Overall, participants were satisfied, and few participants wanted more interventions. Nurses’ support improved participants’ self-management of medication taking and enabled patients to discuss their adherence problems. Adequately timed home visits, more time for support, and accurate medication-related knowledge are desired.
Keywords: medication adherence, patient preference, home care, home care nurses, patient satisfaction, patient adherence
Introduction
Adherence to prescribed medication regimens is important to cure, slow progression, or reduce the symptoms of diseases. Medication adherence has been defined by Vrijens et al1 as “the process by which patients take their medications as prescribed.” Many home care patients find it difficult to adhere to the medication therapy as recommended by a healthcare professional. Up to 80% of home care patients do not take their medications as prescribed.2 Several factors may contribute to medication non-adherence—factors related to the patient, treatment, and/or healthcare professional.3 For example, patients may forget to take the medications, take incorrect dosages, or not believe the medication is necessary.4,5 Treatment-related factors, such as a complex medication regimen or polypharmacy may also increase the risk of non-adherence.6 Furthermore, there may be insufficient communication among patients, informal caregivers, and healthcare professionals.7,8 Because of non-adherence, patients may not benefit optimally from the therapy, which may cause morbidity, mortality, hospital admissions, and increased healthcare costs.9–14
Adherence is often perceived as the patients’ responsibility, but they can be supported by informal caregivers and primary care professionals, such as professionals from the general practice (eg, clinical nurse specialist, practice nurse, and general practitioner), pharmacy (eg, pharmacy technician and pharmacist), and home care.15 Home care in the Netherlands involves care delivered in patients’ homes by nurses of different educational levels, such as registered nurses, licensed practical nurses, and nurse aides.16,17 The goal of home care is to assist individuals of all ages (but mainly adults) to improve function and live with greater independence, to promote well-being, and to assist individuals in several therapies, such as pharmacotherapy or activities of daily living so they can remain at home and avoid hospital admission or admission to long-term care organizations.18 Home care nurses work intra- and interdisciplinary and their roles concerning medication adherence involve observing and addressing non-adherence.19 Previous research shows that nurses observe medication non-adherence during care provision.19–21 Sino et al21 described that 66.3% of 349 home care nurses observe patients’ medication non-adherence during daily care. Nurses’ support in addressing medication non-adherence should focus on the causes of non-adherence and involve interventions that fit patients’ needs and preferences. Nursing interventions could involve providing advice and education in combination with the teach-back method, proposing and implementing a feasible medication regimen (eg, dose simplification, medication schedules, and involving informal caregivers in medication management), assisting with medication intake, motivating patients to change their medication intake behavior, and providing medication-taking reminders (eg, reminders written or by phone and (automatic) pill dispensers).22–29
To our knowledge, patients’ experiences with nurses’ support in medication adherence are yet unknown. Evaluating patients’ experiences provides the opportunity to determine whether care meets patients’ needs and preferences so as to guide further care improvement. Therefore, the objective of this study is to describe the type of adherence support interventions patients received and need and patients’ experiences with these interventions and desired improvements.
Methods
Study Design
A two-phase study was performed, using electronic questionnaire data followed by structured interviews (January 2019 - July 2020). First, questionnaire data were used to analyze (a) received types of support interventions for medication adherence and (b) patients’ experiences with the support nurses provide in medication adherence. Second, structured interviews with multiple participants were conducted to explore experiences and improvements.
To enhance the transparency of the study approach, execution, analysis, and reporting of research data, the questionnaire study is reported according to the checklist for reporting results of Internet e-surveys (CHERRIES)30 and the structured interview study is reported according to the Standards for Reporting Qualitative Research.31
Ethics
The ethical review board of the University of Applied Sciences Utrecht the Netherlands reviewed the protocol of the interview study (reference number 121-000-2020) and concluded that the study procedure is in compliance with ethical requirements. This research is conducted according to the Declaration of Helsinki of the World Medical Association.32 Participants received both written and oral information regarding the studies and consented to participate.
Phase one: type of adherence support interventions and patients’ experiences with nurses’ support in medication adherence
Study Setting and Participants
Participants were members of the care panel of the Netherlands Patients Federation (NPF). NPF represents Dutch patient organizations and advocates on behalf of patients with regard to healthcare professionals, health insurance companies, and politics.33 The panel consists of 20,670 members who are regularly invited to participate in studies. All panel members were invited by email to participate in the questionnaire study aiming to gather their experiences with support in medication adherence provided by nurses in primary and secondary care. Members were eligible to participate if they had one or more chronic condition(s) and received prescription medication three months prior to the questionnaire invitation. Members participated voluntarily and received no incentives. Members, hereafter described as “participants,” determined if they met the criteria and filled in the questionnaire by themselves or with help of an informal caregiver.
Data Collection methods and Process
The electronic questionnaire was developed by the NPF in collaboration with the Dutch Institute for Rational Use of Medicine (IRUM) as part of the development of a Dutch nursing guideline for improving medication adherence. The questions gathered participants’ self-reports regarding the adherence support interventions (n = 14) they received or wanted, satisfaction with received adherence support interventions, experiences (positive and negative) about adherence support interventions received, and desired improvements for the support in medication adherence by nurses of home care organizations (ie, registered nurses and licensed practical nurses) (see Appendix A.docx) and hospitals/general practices (ie, registered nurses, licensed practical nurses, and/or practice nurses).
Eight interventions were derived from the literature (presented in Table 2)34–36 and supplemented with six adherence support interventions that nurses could perform in clinical practice. The questions were self-constructed by the NPF and IRUM and were not tested on participants. For this study, data of participants with support in medication adherence provided by nurses of home care organizations was included.
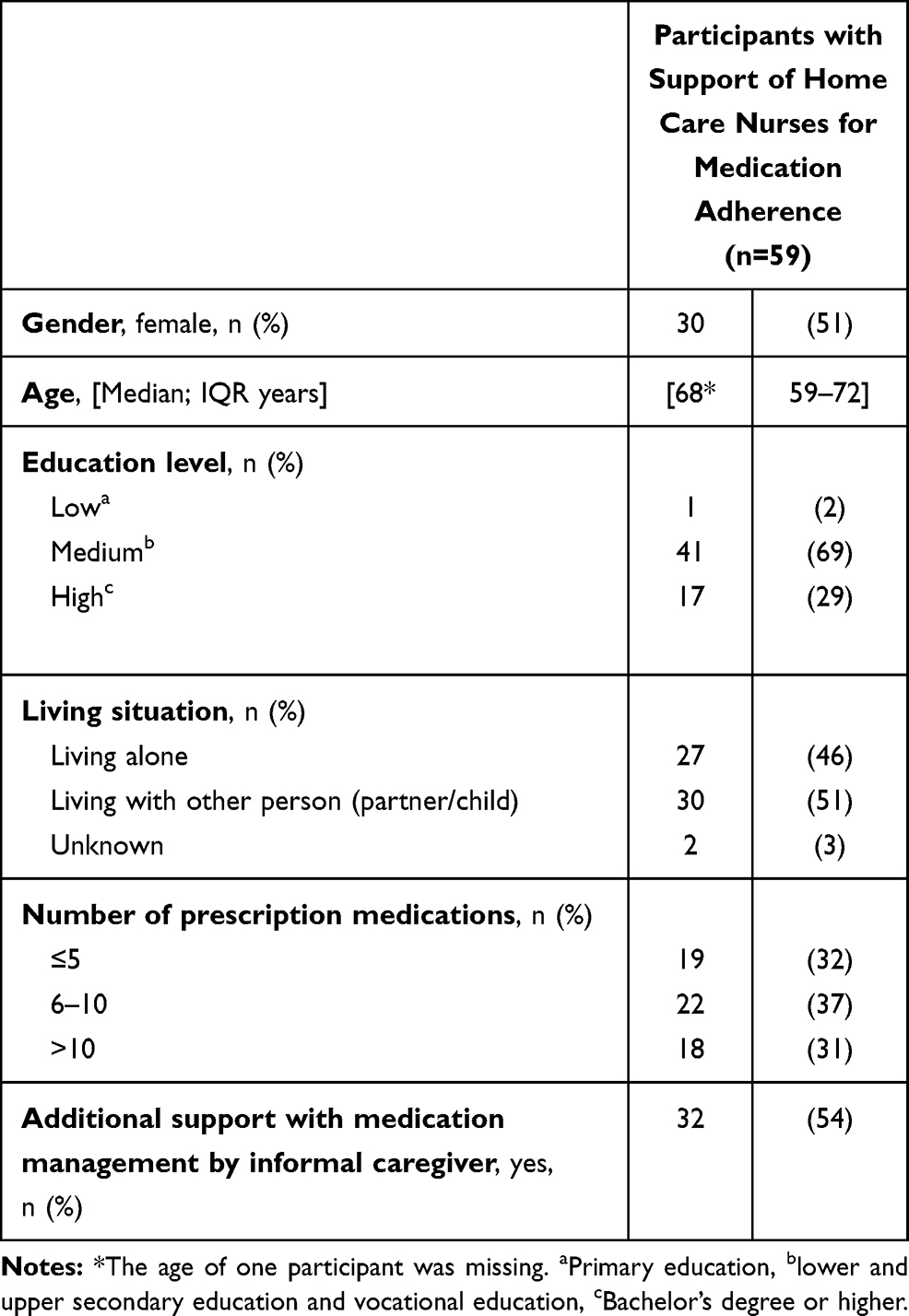 |
Table 1 General Characteristics of Participants of the Questionnaire Study (n = 59) |
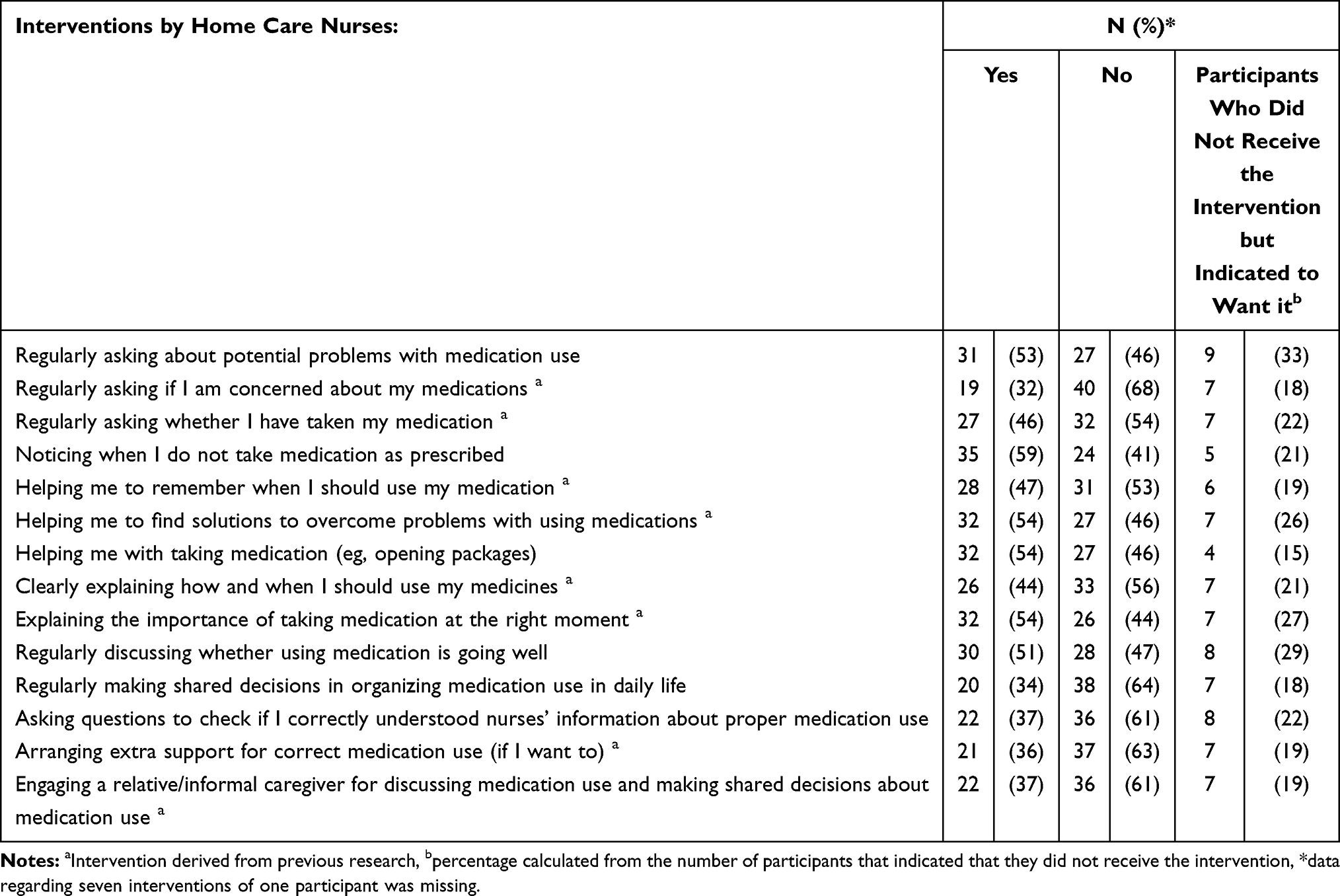 |
Table 2 Type of Received Adherence Support Interventions Indicated by 59 Participants |
Medication adherence is one of the therapies for which home care nurses can assist patients of all ages. Patients or their informal caregiver or physician can ask a home care nurse to assess which support is needed and on which level (ie, no or partial autonomy) and to start the support and perform regular evaluations of the effectiveness and efficiency.
Patients can have home care facilitated by care services in kind or via a personal health budget. Care services in kind means that a home care organization decides on the type of care a patient receives as well as how and at what time this will be delivered. A personal health budget allows patients to manage which home care nurse provides support and at what time the support will be provided.37 Patients choose one of these types and can switch freely between them at any moment. When patients switch, a home care nurse needs to assess the needed support again. Health insurance companies cover all or parts of the costs of these services.
The questionnaire data used for this study covered the following information categories:
- Provided and wanted adherence support interventions and satisfaction
Participants indicated for 14 adherence support interventions if they did or did not receive the intervention. If they indicated that they did not receive the intervention, they were asked whether they want the intervention. Furthermore, participants were asked to rate overall satisfaction with received interventions, using a numeric rating scale ranging from 0 to 10 (0 = low and 10 = high).
Participants could answer open-ended questions about positive and negative experiences with received care and suggested improvements.
Participants could fill in general characteristics such as gender, age, education level, living situation, support with medication management by an informal caregiver, and number of prescription medications.
Panel members who consented to participate and met the criteria received an email with a link to the electronic questionnaire. One reminder was sent within two weeks via email, if participants had not completed the electronic questionnaire. The electronic questionnaire could be completed during a four-week period in January–February 2019. Participants could complete the questionnaire only once and were able to review and change their answers. Data from the electronic questionnaire were automatically exported to an Excel database.
Data Analysis
Provided and Wanted Adherence Support Interventions and Satisfaction
Descriptive statistics were used to describe the received adherence support interventions (yes/no) and the wanted interventions in numbers and percentages; satisfaction with interventions was reported as a median and interquartile range (IQR). One participant was lacking data regarding age and for seven of the 14 interventions. The available data from the participant was included in the analysis.
Positive and Negative Experiences with Support in Medication Adherence and Suggested Improvements
Data to open-ended questions were analyzed by using the thematic approach of Braun and Clarke (2006) that consists of six steps.38 In the first step, the researcher (NED) and a research assistant (EP) read the data using ATLAS.ti software for coding and analysis (version 8.0, Scientific Software Development GmbH, Berlin, Germany) in order to become familiar with the data. In the second step, codes were assigned to paragraphs that reflected positive and negative experiences with care and desired improvements. To assure inter-rater reliability, the coding process was performed individually, and codes were discussed afterwards until consensus was reached.
Steps three to six were performed when the interview data were available; these steps are described in more detail in Phase 2.
General Participant Information
Descriptive statistics were used to describe general participants’ information in number and percentages. This information includes gender, education level (primary education = low, lower and upper secondary education and vocational education = medium, and bachelor’s degree or higher = high), living situation (alone, living together), number of prescriptions (≤ 5, 6–10, > 10), and additional support in medication management by informal caregivers (yes, no). A median and IQR was used for age.
Phase two: Structured interviews regarding experiences and suggested improvements
Study Setting and Participants
The interview study was conducted among participants who completed the questionnaire and received medication adherence support by home care nurses. Twenty-four participants indicated in the questionnaire study their willingness to participate in an interview study. The participants were approached in June 2020. First, they received an email from the NPF with general information (aim and procedure) of the interview study and an invitation to participate. If participants did not respond within one week after the email was sent, they were approached by telephone (also by the NPF) to ask whether they were interested in participating. All responding participants were then called by the researcher (NED) to schedule the interview. Verbal consent was obtained from each participant, and participants could withdraw from the study at any time.
Data Collection Methods and Process
Face-to-face interviews in participants’ homes was the preferred data collection method; however, due to the COVID-19 pandemic, telephone interviews were conducted.
An interview guide was constructed by the authors. The interview guide opened with a general introduction of the interview aim and procedure and was followed with open-ended questions. The participants were asked whether they still received support for medication adherence by home care nurses, what type of support they receive(d), and what their experiences had been with this support. Participants were asked to indicate if they were in need of extra support, if they received the extra support, and if they could suggest improvements to the nurses’ support. Furthermore, questions were asked about the participants’ general characteristics. The interview guide that was followed is detailed in Appendix B.docx. The interview guide was tested in three interviews with participants by the researcher (NED) to check the clarity of the questions and to make final revisions if needed. No adjustments were required. The interview data from the test interviews were included in the data analyses. Interviews were conducted by the researcher (NED) in July 2020. The interviewer has been trained in interview techniques and had experience in performing interviews from a previous project. Interviews were digitally audio recorded to enable verbatim transcription. Mean interview length was 36 minutes (range 31–45 minutes). Audio files were deleted from the record system after they were transcribed. Transcriptions were stored on a secure server of the University.
Data Analysis
Data were analyzed by the researcher (NED) and a research assistant (EP). First, steps one and two of the thematic approach of Braun and Clarke (2006), as described in phase one, were performed. Then, steps three to six were performed as follows: codes of the questionnaire data (analyzed in phase one) and the interview data were brought together under potential themes based on their similarities (step three). In the fourth step, the researcher and research assistant checked the names of the themes for completeness and clarity with the research team. Finally, the meaning of the themes was described and complemented with quotes which led to a detailed description of the results (step six). General information of participants with experiences and suggested improvements of both the questionnaire study and the interview study (ie, gender, age, education level, living situation, number of prescriptions) were analyzed using descriptive statistics.
Results
General Participant Characteristics
In total, 3130 panel members out of 20,670 panel members indicated a willingness to participate in the questionnaire study, and 2753 panel members (87%) completed the questionnaire. In total, 175 participants (6%) received care by a home care nurse, of which 59 participants (33%) received medication adherence support. About half of the participants were female, the median age was 68 (IQR 59–72), and most of the participants used 6–10 medications on a daily basis (Table 1). Six participants completed the questionnaire with the help of an informal caregiver.
Twenty-four persons were invited for the interview study, fourteen agreed to participate, two did not want to participate, and eight could not be contacted using their personal contact details.
Provided and Wanted Adherence Support Interventions and Satisfaction
Participants received one or more of the 14 adherence support interventions. Satisfaction with interventions was rated with a 7.9 (IQR 7–9). The most received adherence support interventions are “noticing when I don’t take medication as prescribed” (n = 35), “helping me to find solutions to overcome problems with using medications” (n = 32), “helping me with taking medication” (eg, opening packages) (n = 32), and “explaining the importance of taking medication at the right moment” (n = 32). The least provided interventions were “regularly asking if I am concerned about my medications” (n = 19), “regularly making shared decisions in organizing medication use in daily life” (n = 20), and “arranging extra support for correct medication use (if I want to)” (n = 21). Fifteen out of the 59 participants indicated the need for one or more interventions. The most frequently wanted interventions involved “regularly asking about potential problems with medication use” (33%), “regularly discussing whether using medication is going well” (29%), and “explaining the importance of taking medication at the right moment” (27%) (Table 2).
Positive and Negative Experiences with Support in Medication Adherence and Suggested Improvements
In total, 22 participants in the questionnaire (n = 8) and interview study (n = 14) indicated positive and negative experiences and suggested improvements. Information on participants’ characteristics is presented in Table 3.
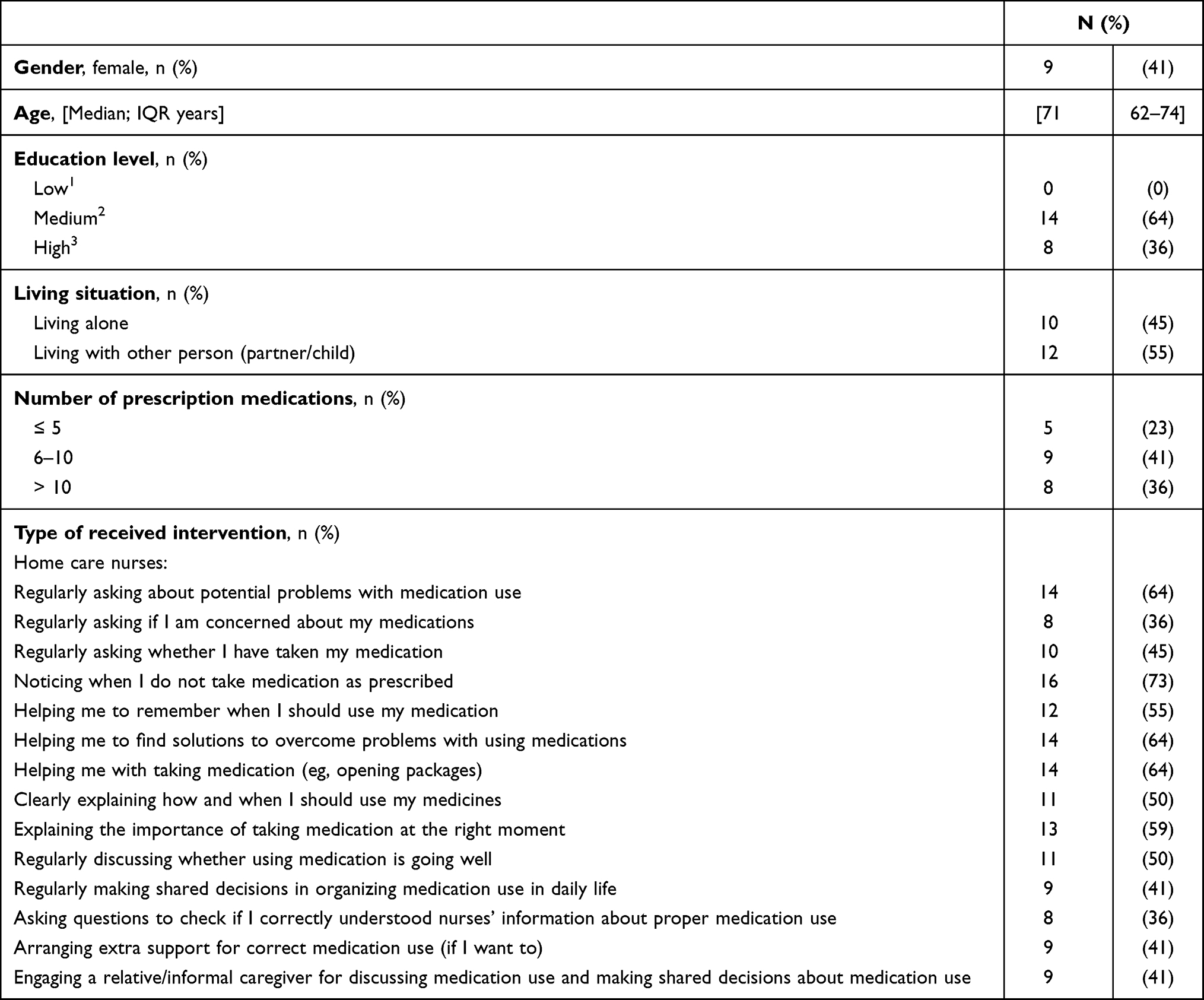 |
Table 3 General Characteristics of Participants Who Indicated Having Positive and Negative Experiences with Support in Medication Adherence and Suggested Improvements (n = 22) |
The study findings resulted in seven themes categorized in three positive and two negative experiences and two improvements.
Positive experiences: In total, 22 participants indicated positive experiences, which are divided into the following themes: (1) improved self-management of medication intake, (2) a professional patient–nurse relationship to discuss adherence problems, and (3) proactive attitude to arrange practical support for medication use.
(1) Improved self-management of medication taking: Several participants indicated that home care nurses’ support, such as the arrangement of aids (eg, weekly pill boxes, multidose drug dispensing systems) and nurses’ advice, provides the opportunity for adequate intake and helped them to take medication independently.
“They advised me to store the medications on a few specific locations in my home instead of multiple locations. I am now able to take the medications correctly by myself, because of using these locations.” - Participant 7. Male, 56 years
(2) A professional patient–nurse relationship to discuss adherence problems: Several participants indicated that they experienced a professional patient–nurse relationship with the home care nurse. They considered it important to be open and ask questions and to share adherence problems. They stated that they experienced a professional relationship with the home care nurses they have frequent contact with. A professional relationship was less often experienced with other care professionals such as physicians and pharmacists.
“Yes, I discuss my issues with the nurse. I am satisfied with contact I have with my nurse. I see her frequently. I think this relation with the nurse, well I am convinced this is not possible to have this with my general practitioner or a medical specialist. I discuss the problems with nurses rather than with them.” - Participant 2. Male, 52 years
(3) Proactive attitude to arrange practical support for medication use: Several participants mentioned that they struggled with taking medication correctly and in time. They were satisfied that home care nurses observed the problems and proactively proposed practical support that helped them take the medication correctly and on time. The practical support involved providing tools such as a multidose drug dispensing system and a weekly pill organizer, and arranging for tablets to be split by the pharmacy.
I could not distinguish the pills and some needed to be split in two halves. The nurse observed my issues to select the right pills to be splitted and suggested and arranged the use of a multi dose drug dispensing system.” - Participant 20. Female, 60 years
Negative experiences: 13 participants indicated negative experiences, leading to the following themes: (4) Timing of home visits and nurses appeared rushed, and (5) insufficient expertise about side effects and taking medication.
(4) Timing of home visits and nurses appeared rushed: Several participants indicated that home care nurses failed to arrive at the time they agreed on. The consequences were that medications were not administered at the recommended moment and participants could not schedule other activities because they did not know if they could start other activities in time. This resulted in feelings of dissatisfaction. Furthermore, participants indicated that home care nurses appeared rushed during home visits. They thought that nurses had insufficient time to support them and participants therefore felt stressed.
“I hope the nurses can arrive in time to give the medications at the right time. At noon, before the lunch, I need Insulin, NovoRapid, before I eat my lunch. But it happens frequently that the nurse is not in time to give the insulin. I start my lunch and the nurse comes later and then she gives me the insulin. It is very annoying.” - Participant 5. Female, 81 years.
Some of these participants indicated that they changed care provision from services in kind to the personal health budget procedure. Since changing to the personal health budget procedure, they have had the experience of nurses arriving on time, so that they were able to plan other activities and were certain that medications were administered at the recommended time.
(5) Insufficient expertise about side effects and taking medication: Several participants indicated that they believe that home care nurses’ expertise concerning side effects and taking medication correctly was insufficient. Participants mentioned they received insufficient answers to questions about side effects and received different advice from nurses on how to use medication correctly.
“In my opinion the expertise of the home care nurses is, well it is low.
[Can you motivate your answer?]
For example, if I ask questions about side effects for my medications, I don’t get an answer or advice. I think they don’t know it. I don’t want advice anymore of home care nurses.” - Participant 46. Male, 69 years
Some participants mentioned that because of the differences in advice from the nurses, they stopped the home care provision and started support by informal caregivers.
“I get different advice from the nurses on how to inhale the medication. Also, information on mouth washing differs. Some nurses say that I don’t need to wash my mouth. Since these difference occurred, I have asked my informal caregiver to assist with the inhaler medication. I believe she is the only one who can do it correctly.” - Participant 23. Male, 75 years
Suggested improvements: Participants indicated two improvements which are related to the negative experiences: (6) performing home visits on time and more time for providing support, and (7) increasing expertise about side effects and medication use.
(6) Performing home visits on time and more time for providing support: Participants wished that nurses could conduct home visits more on time so that they (a) can get medications at the recommended time which would reduce their feelings of stress and (b) have the opportunity to plan and perform other activities which in turn reduces their dissatisfaction. Furthermore, participants mentioned that they wished that nurses could have more time for providing support in medication use. They believe that more time could reduce the rushed appearance of nurses.
(7) More expertise about side effects and taking medication: A few participants mentioned that nurses’ expertise about side effects and taking medication needs to be improved through additional education.
Discussion
The objective of this study was to describe patients’ experiences regarding medication adherence support interventions provided by home care nurses. To our knowledge, this is the first study that gives insight into these patients’ experiences. This research showed that participants receive several adherence support interventions from home care nurses; however, some participants indicated that they were in need of more support interventions. Furthermore, this research provided insight into both positive and negative experiences with home care nurses’ support and improvements suggested by participants. These outcomes and the implications are discussed below.
In this study, self-reports of patients about support received from home care nurses were analyzed. We would like to mention that the results of this study present only adherence support by home care professionals. Besides home care nurses, other primary care professionals have a role in providing adherence support, such as pharmacists and general practitioners.15 It could be that the participants of our study did receive more adherence support than presented, because they were delivered by other care professionals.
It is interesting that several participants expressed the need for more medication adherence interventions by home care nurses. These participants did not participate in the interview study; therefore, it was not possible to explore reasons why these participants did not receive the support. It could be that participants did not ask home care nurses for extra support but asked other healthcare professionals instead. A study by Law et al39 showed that patients expected medication support from doctors and pharmacists rather than nurses. Furthermore, it could be that participants who experienced insufficient time for medication adherence support did not ask questions because they did not want to increase the burden on nurses by asking for extra care. On the other hand, it could be that home care nurses did not ask participants about their needs. We did not examine the perspective of nurses on this subject, but the existing literature shows that several reasons exist for this situation. It could be that nurses lack reflective skills for patients’ needs or lack time due to work overload; or perhaps they choose other priorities in care provision or believe that providing support in medication adherence is the responsibility of the patient only.8,26 Reflective skills, for example, contribute to the detection of patients’ experiences with provided care and patient needs.40 Many studies showed that nurses reflect on care they have provided, but not on care that should be provided.41–44
In this study, three positive themes of nurses’ support with medication use were found. It was found that nurses’ support contributed to taking medication as recommended and independently. It is known from previous research that nurses are able to observe inappropriate medication use20,45 and that they propose and implement adherence support interventions that contribute to patients’ medication adherence.24,46–49 Another positive theme is the professional nurse–patient relationship by which patients were able to ask questions and share problems regarding medication adherence. A professional patient–nurse relationship is associated with medication adherence,50 so home care nurses are encouraged to build and maintain a professional relationship with patients.
However, negative experiences were also found in this study. Participants experienced problems with nurses’ timing of home visits, which resulted in dissatisfaction and medications that were not taken on time. This is in line with previous research that showed that nurses were not always able to give medication on time51 and that this could have clinical consequences.52,53 Furthermore, participants perceived that the nurses’ expertise about the medication was insufficient. This could have several consequences such as medication non-adherence. It is known that an adequate level of professional knowledge is essential for patient adherence.54,55 In this study, nurses’ knowledge has not been assessed, but it has been criticized before. In a study by Simonsen et al56, it was found that knowledge about pharmacology and drug management by the majority of the 203 studied nurses was insufficient, and an association was found between insufficient knowledge and medication errors. Other studies have indicated that nurses feel unqualified to provide advice and desire more education.19,26,57
In a study by De Baetselier et al19, it was shown that 63.4% out of 6719 nurses do not feel qualified to provide patient education; and Sino et al21 show that about 65% of 507 home care nurses want more education.
Interestingly, four participants in the interview study indicated having had home care via care service in kind but were dissatisfied with nurses’ timing of home visits. For this reason, they switched to home care provided via a personal health budget and subsequently experienced that home care nurses performed the home visits in time. It could be that the personal health budget results in more patient satisfaction with provided care, which is known in England.58,59 However, we cannot draw this conclusion from the limited data of our study.
Implications for Practice and Future Research
The findings of this study are important for home care nurses who are involved in patients’ medication adherence support, and it provides suggestions for further research. Home care nurses are advised to better evaluate patients’ needs for medication adherence support and better align their support to patients’ needs and preferences so as to improve their adherence to medication. However, we want to mention that nurses do not have to do this alone. Nurses can collaborate with other care primary care professionals to evaluate patients’ needs and discuss which professional provides support.
Furthermore, home care nurses should focus on the timing of home visits, so that patients can take medications in time. Moreover, it may prevent harmful situations and patient dissatisfaction. The professional patient–nurse relationship was experienced as positive by participants in this study and since it has been associated with medication adherence in previous research50, home care nurses are encouraged to build and maintain a professional relationship with patients.
More attention can be given to nurses’ knowledge. Nurses should be able to evaluate their own expertise and to increase it with education if needed. In order to evaluate expertise, nurses could use knowledge evaluation tests.
Future research should explore home care nurses’ experiences in providing medication adherence support. As participants expressed the need for more interventions by home care nurses, it would be interesting to study home care nurses’ perspective about reflecting on patients’ needs.
Strengths and Limitations
This study has some strengths and limitations. Due to the COVID-19 pandemic, face-to-face interviews in the home setting were replaced by telephone interviews. The telephone interviews allowed us to continue this research. An advantage of the interviews via telephone could be that it may create an atmosphere in which participants were able to disclose sensitive information about received nurses’ support.60 A disadvantage of telephone interviews could be the inability of the interviewer to observe and respond to participants’ nonverbal communication. However, we believe that using telephone interviews in this study population did not limit our assessment of participants’ experiences, since the participants were already used to participating in telephone interview studies.
The results of this study are based on the experiences of a small part of the home care population. There could be experiences in the population of home care patients that have not been studied in our research. These limitations could result in an underestimation of home care patients’ experiences with regard to home care nurses’ support.
Conclusions
This study showed that participants overall were satisfied with nurses’ medication adherence support with a few participants wanted more interventions. Nurses’ support improved participants’ self-management of medication taking and enabled patients to discuss their adherence problems. Participants’ experiences regarding nurses’ medication adherence support can be improved with adequately timed home visits, more time for medication adherence support, and more accurate medication-related knowledge.
Ethics Statement
The ethical review board of the University of Applied Sciences Utrecht the Netherlands reviewed the protocol of the interview study (reference number 121-000-2020) and concluded that the study procedure is in compliance with ethical requirements. All participants gave informed consent prior to study commencement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Marcia Vervloet reports grants from AbbVie, grants from Pfizer, grants from Teva, grants from AstraZeneca, outside the submitted work. Dr Marjorie Nelissen-Vrancken reports grants from ZonMw, during the conduct of the study. The authors declare that there is no conflict of interest.
References
1. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
2. Mongkhon P, Kongkaew C. Medication non-adherence identified at home: a systematic review and meta-analysis. Qual Prim Care. 2017;25(2):73–80.
3. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; 2003. Available from: http://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf;jsessionid=8D53CCE3C89AE6164D4B6645BFB951C6?sequence=1. Accessed March 12, 2020
4. Sino CGM, Sietzema M, Egberts TC, Schuurmans MJ. Medication management capacity in relation to cognition and self-management skills in older people on polypharmacy. J Nutr Health Aging. 2014;18(1):44–49. doi:10.1007/s12603-013-0359-2
5. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
6. Coleman CI, Limone B, Sobieraj DM, et al. Dosing frequency and medication adherence in chronic disease. J Manag Care Pharm. 2012;18(7):527–539. doi:10.18553/jmcp.2012.18.7.527
7. Linn AJ, van Weert JC, Schouten BC, Smit EG, van Bodegraven AA, van Dijk L. Words that make pills easier to swallow: a communication typology to address practical and perceptual barriers to medication intake behavior. Patient Prefer Adherence. 2012;6:871–885. doi:10.2147/PPA.S36195
8. van Dulmen S. What makes them (not) talk about proper medication use with their patients? An analysis of the determinants of GP communication using reflective practice. Int J Pers Cent Med. 2011;1(1):27–34. doi:10.5750/ijpcm.v1i1.4
9. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982–2017. doi:10.1136/bmjopen-2017-016982
10. Halpern R, Becker L, Iqbal SU, Kazis LE, Macarios D, Badamgarav E. The association of adherence to osteoporosis therapies with fracture, all-cause medical costs, and all-cause hospitalizations: a retrospective claims analysis of female health plan enrollees with osteoporosis. J Manag Care Pharm. 2011;17(1):25–39. doi:10.18553/jmcp.2011.17.1.25
11. Tohme F, Mor MK, Pena-Polanco J, et al. Predictors and outcomes of non-adherence in patients receiving maintenance hemodialysis. Int Urol Nephrol. 2017;49(8):1471–1479. doi:10.1007/s11255-017-1600-4
12. Walsh CA, Cahir C, Tecklenborg S, Byrne C, Culbertson MA, Bennett KE. The association between medication non-adherence and adverse health outcomes in ageing populations: a systematic review and meta-analysis. Br J Clin Pharmacol. 2019;85(11):2464–2478. doi:10.1111/bcp.14075
13. Leendertse AJ, Egberts AC, Stoker LJ; HARM Study Group. Frequency of and risk factors for preventable medication-related hospital admissions in the Netherlands. Arch Intern Med. 2008;168(17):1890–1896.
14. Lghoul-Oulad Saïd F, Hek K, Flinterman LE, et al. Prevalence and incidence rate of hospital admissions related to medication between 2008 and 2013 in The Netherlands. Pharmacoepidemiol Drug Saf. 2020;29(12):1659–1668. doi:10.1002/pds.5122
15. Lelie - van der Z. LESA: organization of care for chronic medication (LESA: organisatie van zorg bij chronische medicatie); 2020. Available from: https://richtlijnen.nhg.org//files/2020-05/lesa_organisatie_van_zorg_bij_chronische_medicatie.pdf.
16. Dilles T, Stichele RV, Van Rompaey B, Van Bortel L, Elseviers M. Nurses’ practices in pharmacotherapy and their association with educational level. J Adv Nurs. 2010;66(5):1072–1079. doi:10.1111/j.1365-2648.2010.05268.x
17. Lee JK, Alshehri S, Kutbi HI, Martin JR. Optimizing pharmacotherapy in elderly patients: the role of pharmacists. Integr Pharm Res Pract. 2015;4:101–111. doi:10.2147/IPRP.S70404
18. Hughes RG. Patient Safety and Quality: An Evidence-Based Handbook for Nurses.
19. De B. EUPRON: nurses’ practice in interprofessional pharmaceutical care in Europe. A cross-sectional survey in 17 countries. BMJ Open. 2020;10(6):e036269
20. Ellenbecker CH, Frazier SC, Verney S. Nurses’ observations and experiences of problems and adverse effects of medication management in home care. Geriatr Nurs. 2004;25(3):164–170. doi:10.1016/j.gerinurse.2004.04.008
21. Sino CGM. Medication management in homecare patients. Utrecht University; 2013.
22. Hornnes N, Larsen K, Boysen G. Blood pressure 1 year after stroke: the need to optimize secondary prevention. J Stroke Cerebrovasc Dis. 2011;20(1):16–23. doi:10.1016/j.jstrokecerebrovasdis.2009.10.002
23. Barnason S, Zimmerman L, Hertzog M, Schulz P. Pilot testing of a medication self-management transition intervention for heart failure patients. West J Nurs Res. 2010;32(7):849–870. doi:10.1177/0193945910371216
24. Rinfret S, Rodes-Cabau J, Bagur R, et al. Telephone contact to improve adherence to dual antiplatelet therapy after drug-eluting stent implantation. Heart. 2013;99(8):562–569. doi:10.1136/heartjnl-2012-303004
25. Parker R, Frampton C, Blackwood A, Shannon A, Moore G. An electronic medication reminder, supported by a monitoring service, to improve medication compliance for elderly people living independently. J Telemed Telecare. 2012;18(3):156–158. doi:10.1258/jtt.2012.SFT108
26. van Dijk L, Huis A, de Groot K, Vervloet M, Lescure D, Francke A. Improving medication adherence by nurses (Improving van medicatietrouw door verpleegkundigen). Bevorderen van medicatietrouw door verpleegkundigen en verzorgenden; 2017. Available from: https://www.nivel.nl/sites/default/files/bestanden/Knelpuntenanalyse_medicatietrouw_verpleegkundigen_verzorgenden.pdf.
27. Conn VS, Ruppar TM, Enriquez M, Cooper P. Medication adherence interventions that target subjects with adherence problems: systematic review and meta-analysis. Res Social Adm Pharm. 2016;12(2):218–246. doi:10.1016/j.sapharm.2015.06.001
28. Kini V, Ho PM. Interventions to improve medication adherence: a review. JAMA. 2018;320(23):2461–2473. doi:10.1001/jama.2018.19271
29. Butcher HK, Bulechek GM, Dochterman JM, Wagner CM. Nursing Interventions Classification.
30. Eysenbach G. Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):34. doi:10.2196/jmir.6.3.e34
31. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
32. World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull World Health Organ. 2001;79(4):373.
33. Netherlands Patients Federation. No title. Available from: https://www.patientenfederatie.nl/algemeen/netherlands-patients-federation.
34. de Bruin M, Dima AL, Texier N, van Ganse E; ASTRO-LAB group. Explaining the Amount and consistency of medical care and self-management support in asthma: a survey of primary care providers in France and the United Kingdom. J Allergy Clin Immunol Pract. 2018;6(6):1916–1925.e7. doi:10.1016/j.jaip.2018.04.039
35. de Bruin M, Viechtbauer W, Schaalma HP, Kok G, Abraham C, Hospers HJ. Standard care impact on effects of highly active antiretroviral therapy adherence interventions: a meta-analysis of randomized controlled trials. Arch Intern Med. 2010;170(3):240–250. doi:10.1001/archinternmed.2009.536
36. de Bruin M, Viechtbauer W, Hospers HJ, Schaalma HP, Kok G. Standard care quality determines treatment outcomes in control groups of HAART-adherence intervention studies: implications for the interpretation and comparison of intervention effects. Health Psychol. 2009;28(6):668–674. doi:10.1037/a0015989
37. National Institute for Public Health and the Environment. Personal budget and care services in kind. 2020; Available from: https://www.government.nl/topics/care-and-support-at-home/question-and-answer/-difference-between-personal-budget-pgb-and-care-services-in-kind.
38. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
39. Law AV, Ray MD, Knapp KK, Balesh JK. Unmet needs in the medication use process: perceptions of physicians, pharmacists, and patients. J Am Pharm Assoc. 2003;43(3):394–402. doi:10.1331/154434503321831111
40. Oelofsen N. Using reflective practice in frontline nursing. Nurs Times. 2018;108(24):22–24.
41. Gustafsson C, Asp M, Fagerberg I. Reflection in night nursing: a phenomenographic study of municipal night duty registered nurses’ conceptions of reflection. J Clin Nurs. 2009;18(10):1460–1469. doi:10.1111/j.1365-2702.2008.02438.x
42. Teekman B. Exploring reflective thinking in nursing practice. J Adv Nurs. 2000;31(5):1125–1135. doi:10.1046/j.1365-2648.2000.01424.x
43. Asselin ME, Schwartz-Barcott D, Osterman PA. Exploring reflection as a process embedded in experienced nurses’ practice: a qualitative study. J Adv Nurs. 2013;69(4):905–914. doi:10.1111/j.1365-2648.2012.06082.x
44. Riley J, Beal JA, Lancaster D. Scholarly nursing practice from the perspectives of experienced nurses. J Adv Nurs. 2008;61(4):425–435. doi:10.1111/j.1365-2648.2007.04499.x
45. Bergqvist M, Ulfvarson J, Andersén Karlsson E. Nurse-led medication reviews and the quality of drug treatment of elderly hospitalized patients. Eur J Clin Pharmacol. 2009;65(11):1089–1096. doi:10.1007/s00228-009-0728-2
46. Garcia-Aymerich J, Hernandez C, Alonso A, et al. Effects of an integrated care intervention on risk factors of COPD readmission. Respir Med. 2007;101(7):1462–1469. doi:10.1016/j.rmed.2007.01.012
47. Antonicelli R, Mazzanti I, Abbatecola AM, Parati G. Impact of home patient telemonitoring on use of β-blockers in congestive heart failure. Drugs Aging. 2010;27(10):801–805. doi:10.2165/11538210-000000000-00000
48. Granger BB, Ekman I, Hernandez AF, et al. Results of the chronic heart failure intervention to improve medication adherence study: a randomized intervention in high-risk patients. Am Heart J. 2015;169(4):539–548. doi:10.1016/j.ahj.2015.01.006
49. Insel KC, Einstein GO, Morrow DG, Koerner KM, Hepworth JT. Multifaceted prospective memory intervention to improve medication adherence. J Am Geriatr Soc. 2016;64(3):561–568. doi:10.1111/jgs.14032
50. Kerse N, Buetow S, Mainous AG, Young G, Coster G, Arroll B. Physician-patient relationship and medication compliance: a primary care investigation. Ann Fam Med. 2004;2(5):455–461. doi:10.1370/afm.139
51. Kalisch BJ, Xie B. Errors of omission: missed nursing care. West J Nurs Res. 2014;36(7):875–890. doi:10.1177/0193945914531859
52. Dijkstra NESC. Potential clinical consequences of medication process problems in older home care patients. J Geriatr Med Gerontol. 2020;6(085). doi:10.23937/2469-5858/1510085
53. Lisby M, Nielsen LP, Mainz J. Errors in the medication process: frequency, type, and potential clinical consequences. Int J Qual Health Care. 2005;17(1):15–22. doi:10.1093/intqhc/mzi015
54. Delavar F, Pashaeypoor S, Negarandeh R. The effects of self-management education tailored to health literacy on medication adherence and blood pressure control among elderly people with primary hypertension: a randomized controlled trial. Patient Educ Couns. 2020;103(2):336–342. doi:10.1016/j.pec.2019.08.028
55. Taibanguay N, Chaiamnuay S, Asavatanabodee P, Narongroeknawin P. Effect of patient education on medication adherence of patients with rheumatoid arthritis: a randomized controlled trial. Patient Prefer Adherence. 2019;13(13):119–129. doi:10.2147/PPA.S192008
56. Simonsen BO, Johansson I, Daehlin GK, Osvik LM, Farup PG. Medication knowledge, certainty, and risk of errors in health care: a cross-sectional study. BMC Health Serv Res. 2011;11(1):175–6963. doi:10.1186/1472-6963-11-175
57. Sino CG, Munnik A, Schuurmans MJ. Knowledge and perspectives of Dutch home healthcare nurses regarding medication frequently used by older people. Int J Older People Nurs. 2013;8(2):131–138. doi:10.1111/j.1748-3743.2012.00336.x
58. Davidson J. Personal health budgets: experiences and outcomes for budget holders at nine months. Fifth interim report; 2012. Available from: https://www.phbe.org.uk/documents/interim-report-june-2012.pdf.
59. van Ginneken E, Groenewegen PP, McKee M. Personal healthcare budgets: what can England learn from the Netherlands? BMJ. 2012;344(mar06 3):e1383. doi:10.1136/bmj.e1383
60. Novick G. Is there a bias against telephone interviews in qualitative research? Res Nurs Health. 2008;31(4):391–398. doi:10.1002/nur.20259
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.