Back to Journals » Patient Preference and Adherence » Volume 19
Home-Based Self-Management After Permanent Pacemaker Implantation: What Should Patients Know
Authors Yan H, Chen YS ![]() , Li Y, Wei GX, Ma F
, Li Y, Wei GX, Ma F ![]() , Hu QL, Ding L, Wei W
, Hu QL, Ding L, Wei W ![]() , Li Y, Bai YJ
, Li Y, Bai YJ
Received 17 April 2025
Accepted for publication 21 August 2025
Published 8 September 2025 Volume 2025:19 Pages 2771—2786
DOI https://doi.org/10.2147/PPA.S535177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Han Yan,1,* Yu Shuang Chen,2,* Yi Li,2 Guan-Xing Wei,2 Fang Ma,3 Qiu Lan Hu,4 Lan Ding,5 Wei Wei,6 Yan Li,7 Yang-Juan Bai2
1Intensive Care Unit of Cardiac Surgery Department, QingDao Municipal Hospital (Group), Qingdao, Shandong, People’s Republic of China; 2The First Department of Cardiology, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 3Nursing Department, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 4Geriatric Intensive Care Unit, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 5Outpatient Department, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 6Department of Gastrointestinal Surgery, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 7Department of Obstetrics, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang-Juan Bai, The First Department of Cardiology, The First Affiliated Hospital of Kunming Medical University, No. 295, Xichang Road, Kunming, Yunnan, 650032, People’s Republic of China, Tel +8613678757051, Email [email protected]
Objective: The purpose of this study is to systematically explore and summarize the best evidence of home-based self-management in patients with permanent pacemaker implantation, providing comprehensive references and guidance for improving the self-management ability of such patients.
Methods: Using the “ 6S” model, a systematic literature search was conducted on home-based self-management in patients with permanent pacemaker implantation. The types of literature included best practice, clinical decision-making, guidelines, expert consensus, systematic review and evidence summary. According to the inclusion and exclusion criteria, two researchers screened the literature, evaluated the quality, extracted the data, synthesized the evidence.
Data Sources: BMJ Best Practice, Up To Date, Joanna Briggs Institute (JBI), the World Health Organization (WHO), the Guidelines International Network (GIN), the National Institute for Health and Care Excellence (NICE), the Registered Nurses Association of Ontario (RNAO), the Scottish Intercollegiate Guidelines Network (SIGN), the American Heart Association (AHA), the Cochrane Library, PubMed, CINAHL, Web of Science, Medlive, CNKI Database, SinoMed (China Biomedical Literature Database), Wanfang Database and VIP Database. The retrieval period spanned from the establishment of these databases until January 31, 2025.
Results: A total of 21 articles were included, 1 best practice, 9 clinical decision-making, 5 guidelines, 3 expert consensus, 1 systematic review, and 2 evidence summaries. Thirty-five pieces of the best evidence from 7 aspects were summarized, including complication management, electromagnetic interference management, sports rehabilitation management, operative limb management, postoperative follow-up management, role management, and emotional management.
Conclusion: This review comprehensively summarized the best evidence home-based self-management in patients with permanent pacemaker implantation. These findings are scientific and referential, and provide evidence-based support for nursing and management of patients during home-based rehabilitation.
Keywords: permanent pacemaker, self-management, best evidence, evidence-based nursing
Introduction
Cardiac pacemakers, referred to as pacemakers, are Cardiovascular Implantable Electronic Devices (CIED) implanted in the body, which release a certain form of electrical pulse to stimulate the heart, enabling it to form and conduct impulses.1 Among them, the permanent pacemaker is currently the most widely applied and also the most effective treatment method for chronic arrhythmia.1 Data presented in the “2023 China Cardiovascular Health and Disease Report” indicate that over 120,000 cardiac pacemaker implantations were carried out in China during 2022.2 Moreover, around 3 million people worldwide are using cardiac pacemakers, and the number is growing at a rate of 15% per year.3 In recent years, with the rapid development of medical technology, this technology has been gradually optimized, which can effectively improve patients’ clinical symptoms, prolong their lifespan and enhance their quality of life.4,5 Studies have shown that the long-term treatment effect of permanent pacemaker implantation was not only related to the quality of the pacemaker and the doctor’s operating techniques, but also closely related to the patient’s self-management behavior after surgery.6 However, it was quite common that patients valued implantation but ignored management. As a result, patients might suffer from adverse consequences caused by poor self-management, such as pocket infections, electrode dislocations and so on.
In 1986, foreign scholar Holroyd7 proposed the concept of self-management, defining self-management as the patient’s assumption of a portion of preventive or therapeutic health care activities with the assistance of health care professionals. Subsequently, scholars Corbin & Strauss8 first put forward the Chronic Illness Trajectory Model in 1991 and described self-management as three independent yet related tasks, namely medical or behavioral management of the disease, role management, and emotional management. The core concept of self-management, which emphasizes the central role of the patient in chronic disease management, is one of the most effective modalities used in the management of chronic diseases at home and abroad to improve the patient’s ability to manage his or her own disease symptoms, treatment, psychology, physiology, and lifestyle changes.9
In addition, a study in the United States found that approximately 11.5% of patients developed pocket hematomas after pacemaker implantation.10 A European study found that incorrect self-management after pacemaker implantation may lead to an increased incidence of infective endocarditis.11 In China, studies have shown that the incidence of adverse reactions after pacemaker implantation is 7.5%,12 and the incidence of anxiety and depression ranges from 29.9% to 38%.13 The reason for these results may be the patient’s lack of correct and effective health management behaviors. Scientific and standardized self-management behavior can improve patients ‘self-management capabilities, improve negative emotions, improve quality of life and improve life quality after discharge, and reduce complications.14 In view of this, improving the home-based/post-hospital self-management ability of patients with permanent pacemaker implantation has important guaranteeing significance for their later-stage rehabilitation, prognosis and quality of life.
However, the current research results have shown that the self-management ability of patients with permanent pacemaker implantation generally presents a phenomenon of being at a low level. A study was conducted among 40 patients in Cairo Benha University Hospital and the National Heart Institute in Egypt to evaluate the the level of home care for patients with permanent pacemakers, and the results showed that 61.7% of the patients were dissatisfied with the total score of self-management practices.15 A Dutch research project that tracked patients for a period of six months subsequent to the implantation of pacemakers found that, on the whole, these patients exhibited relatively low levels of self-management capabilities.16 Therefore, how to effectively provide relevant information and guide patients to master corresponding management skills and improve patients’ home-based self-management capabilities has become an important issue that needs to be solved urgently.
Previous studies have already put forward relevant suggestions on the self-management of patients after permanent pacemaker implantation. Nevertheless, their results were scattered and unfocused. Currently, there is still no comprehensive, standardized and systematic home-based self-management guideline for patients with permanent pacemaker implantation, which is not conducive to carrying out effective education by clinical medical staff. An evidence summary functions was a review of the available evidence concerning one or one set of research questions about a specific topic.17 This study adopts evidence-based approaches to systematically search for high-quality evidence. It extracts and summarizes relevant evidence in accordance with the self-management model proposed by scholars Corbin & Strauss, which encompasses disease management, role management, and emotional management. Its purpose is to provide an evidence-based foundation for home-based self-management in patients with permanent pacemaker implantation.
Methods/Methodology
The Fudan University Center for Evidence-based Nursing has produced a reporting standard based on the JBI’s methods of generating an evidence summary. This standard encompasses problem formulation, literature search, literature screening, literature evaluation, evidence summarization and grading, as well as the generation of practical recommendations. This evidence summary was carried out in accordance with the standard of evidence summary report of the Evidence-based Nursing Center of Fudan University,18 and has been registered with the same center, with the registration number being ES20221000.
Problem Establishment
The evidence-based problem in this review was formulated in accordance with the PIPOST principle, which is shown as follows.
P (population, that is, the target population for the application of evidence) refers to patients after permanent pacemaker implantation;
I (intervention) represents the relevant measures for home self-management of patients with permanent pacemaker implantation;
P (professional, that is, the professional for evidence application) refers to clinical managers, clinical nurses in the department of cardiology, and doctors in the electrophysiology group of the department of cardiology;
O (outcome) was the mastery level of patients regarding the knowledge and skills related to self-management, quality of life, self-efficacy, and levels of anxiety and depression;
S (setting, that is, the evidence application site) was the Department of Cardiology, communities and home settings;
T (type of evidence) included clinical decision-making, clinical practice, guidelines, expert consensus, evidence summary, and systematic review.
Evidence Retrieval
In line with the “6S” model19 and by applying the top-down retrieval principle, we carried out computerized searches in the following evidence-based resource databases: BMJ Best Practice, Up To Date, Joanna Briggs Institute (JBI), the World Health Organization (WHO), the Guidelines International Network (GIN), the National Institute for Health and Care Excellence (NICE), the Registered Nurses Association of Ontario (RNAO), the Scottish Intercollegiate Guidelines Network (SIGN), the American Heart Association (AHA), the Cochrane Library, PubMed, CINAHL, Web of Science, Medlive, CNKI Database, SinoMed (China Biomedical Literature Database), Wanfang Database and VIP Database. The retrieval period spanned from the establishment of these databases until January 31, 2025.
The search strategy implemented in databases was made up of the following terms: (pacemaker, artificial OR artificial cardiac pacemaker* OR artificial pacemaker* OR cardiac pacemaker*artificial OR pacemaker*artificial cardiac OR permanent pacemaker OR pacemaker implantation OR pacemaker OR cardiac pacing OR cardiac implantable electronic device) AND (self-management OR self care OR health education OR self-management intervention OR self-management intervention plan OR self administration OR self monitoring OR patient education OR management program OR disease management OR emotion management OR psychiatric nursing OR medical management OR management) AND (guideline OR meta-analysis OR consensus OR systematic review OR evidence summary). According to the particular demands of each database, the search formula and wildcard characters were adjusted nimbly through the combination of topic terms and free words. An example of an English database search using PubMed with the corresponding search strategy is shown in Table 1.
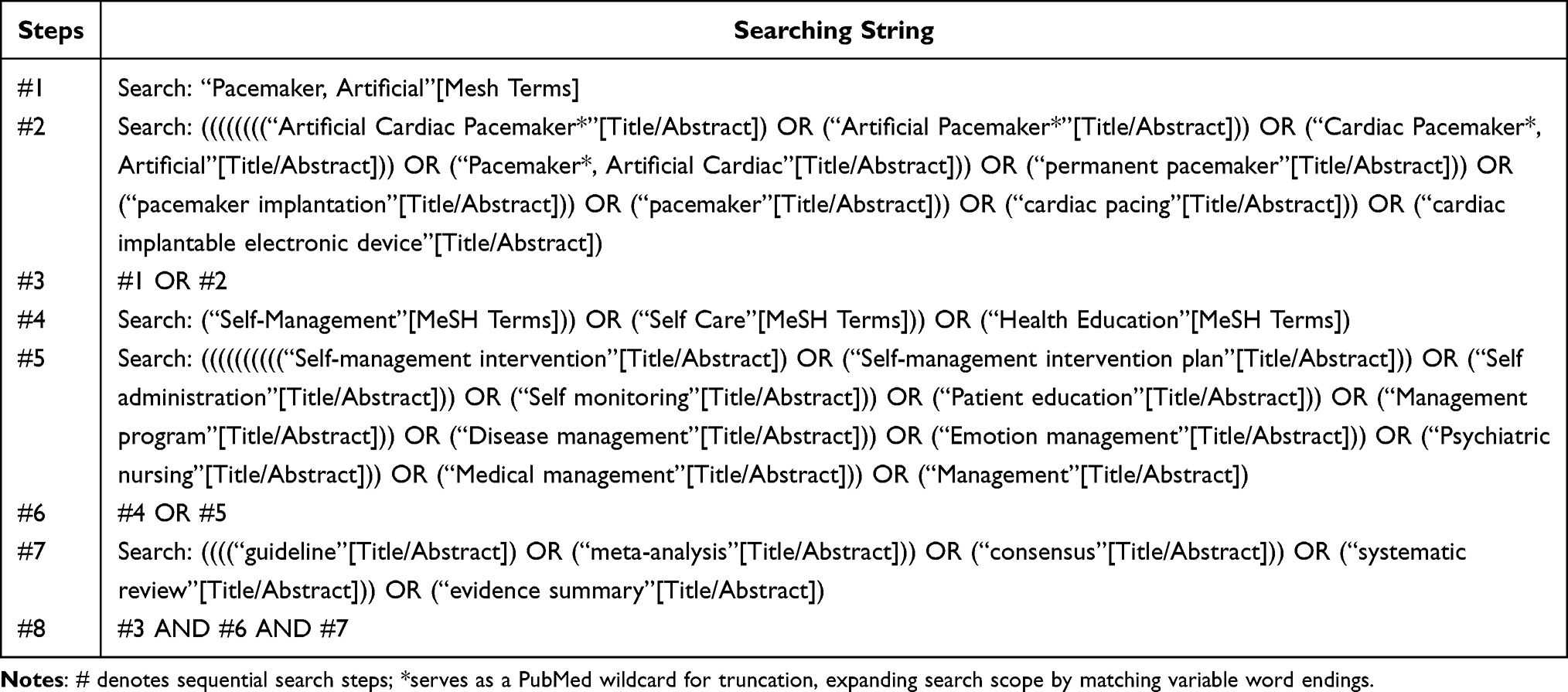 |
Table 1 Literature Search Strategies are Derived from PubMed Database |
Inclusion and Exclusion Criteria of Literature
Inclusion criteria of literature for this study were (1) The objects of study were patients with permanent pacemakers implanted who were aged 18 years or older; (2) The contents of literature referred to home-based self-management interventions for patients with permanent pacemaker implantation, such as self-management, symptom observation, psychological adjustment, and follow-up; (3) The type of study such as best practice, clinical decision-making, guidelines, expert consensus, systematic review and evidence summary was considered; (4) Only the latest versions of updated or revised clinical guidelines were considered; (5) The languages of publication were Chinese and English. Exclusion criteria were (1) Literatures with incomplete information or those from which the full text could not be obtained; (2) Literatures were a plan, draft or only an abstract; (3) Literatures of poor quality after inspection; (4) Republished articles.
Literature Screening
The retrieved literature was imported into Endnote and any duplicated literature was eliminated. Two researchers who had received training in evidence-based medicine independently screened the literatures and conducted a thorough inspection. During the evaluation when the inclusion of the obtained literature was controversial, the literature was discussed with a third critical field evidence-based care specialist to determine inclusion status.
Quality Evaluation of the Literature
Quality Evaluation of the Guidelines
The quality of the guidelines was assessed using the Appraisal of Guidelines for Research and Evaluation II (AGREE II).20 The tool, which consists of 6 dimensions, 23 items and 2 overall evaluation items, is used to assess the scope and purpose, participants, rigor of development, clarity and readability, applicability and independence of articles. On the AGREEII scale, a score of 1 corresponds to strongly disagree and 7 to strongly agree for the evaluation of each item. Standardized scores in each field = [(actual score evaluated − lowest possible score)/(highest possible score − lowest possible score)]×100%. The guidelines recommend division of the standardization score into three grades: if 6 items score ≥60%, it is recommended as a grade A; if ≥3 items score ≥30% with some items with scores <60%, it is recommended as a grade B after modification and improvement; and ≥3 areas with scores <30% are excluded as grade C.
Quality Evaluation of Expert Consensus and Systematic Reviews
The expert consensus and systematic reviews were evaluated by using the appropriate assessment instruments provided by the Australian JBI evidence-based Health Care Centre (2017 edition). The expert consensus evaluation tool is made up of six items which are the source of opinions, the author’s influence in the field, the focus of the views on relevant stakeholders, the logic of the views, the reference to other literature and the agreement of the view with the previous. The evaluation results of each of these items are adjudged using “yes”, “no”, “unclear” and “not applicable”. The evaluation tool for systematic reviews comprises 11 items, with each item evaluated against the criteria of “yes”, “no”, “unclear”, and “not applicable”.
Quality Evaluation of Evidence Summary
The evidence summary employed the CASE checklist for evaluation, which comprises 10 items, and the evaluation criteria for each item are “yes”, “partially yes” and “no”.21
Evidence Summary and Grading
Two researchers who had received evidence-based training extracted and summarized the evidence from the included literature. Any disagreements are resolved through negotiation or with the assistance of a third-party researcher. In cases where the evidence conclusions are contradictory, high-quality and recently published evidence from peer-reviewed journals will be given priority. In order to determine the reliability of the evidence, we will grade the evidence. This study utilized the evidence pre-classification system from the 2014 JBI intervention study to assess the evidence, employing a rating scheme ranging from Level 1 to Level 5.
Results
Information of Included Literature
A total of 1688 relevant literatures were retrieved in this review. After excluding the articles that did not meet the inclusion criteria of this study, a total of 21 articles were finally included for analysis. These 21 articles include 1 best practice, 9 clinical decision-making, 5 guidelines, 3 expert consensuses, 1 systematic review, and 2 evidence summary (Figure 1). The overall attributes of the literature were shown in Table 2.
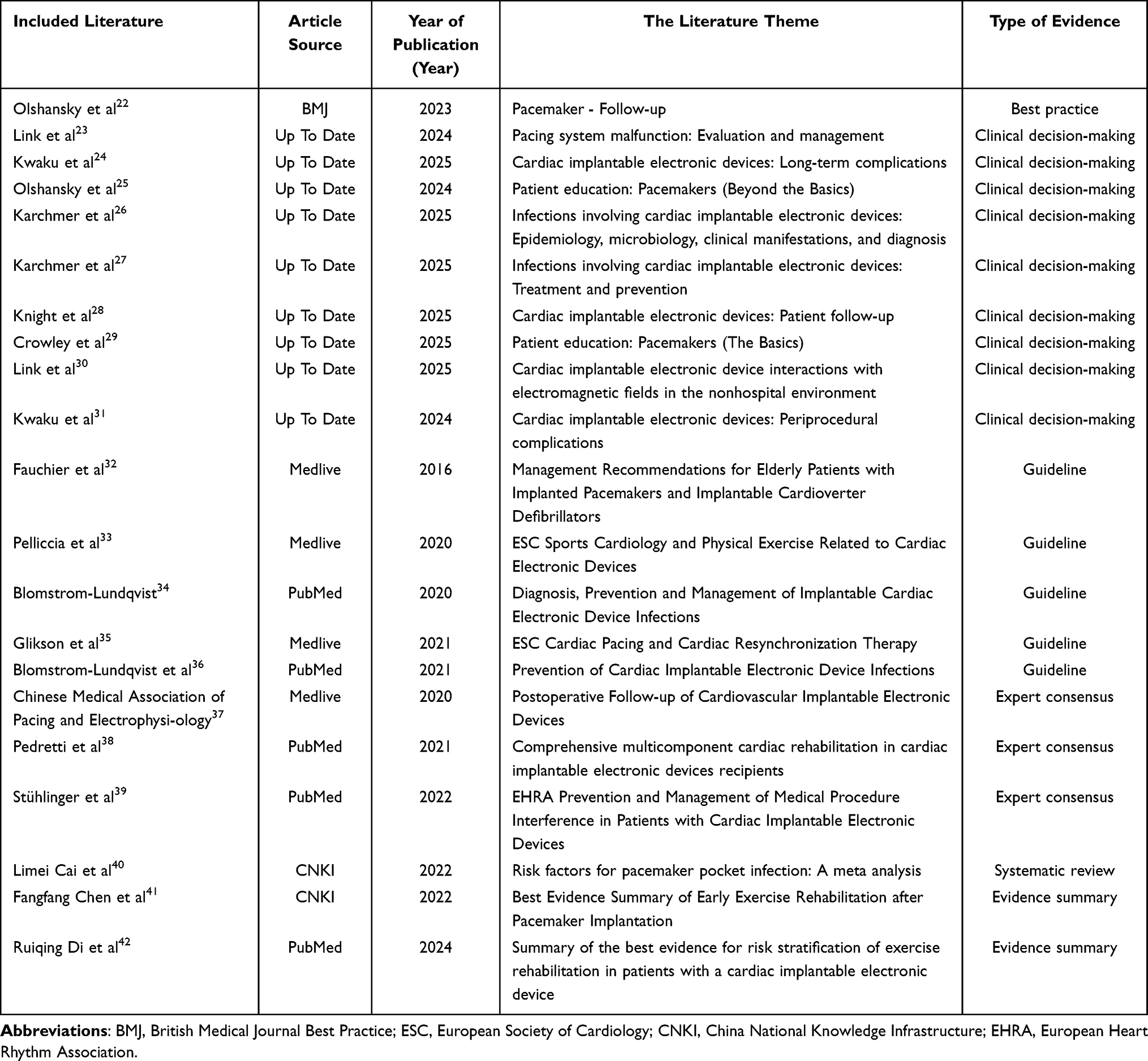 |
Table 2 General Characteristics Included in the Literature (n=21) |
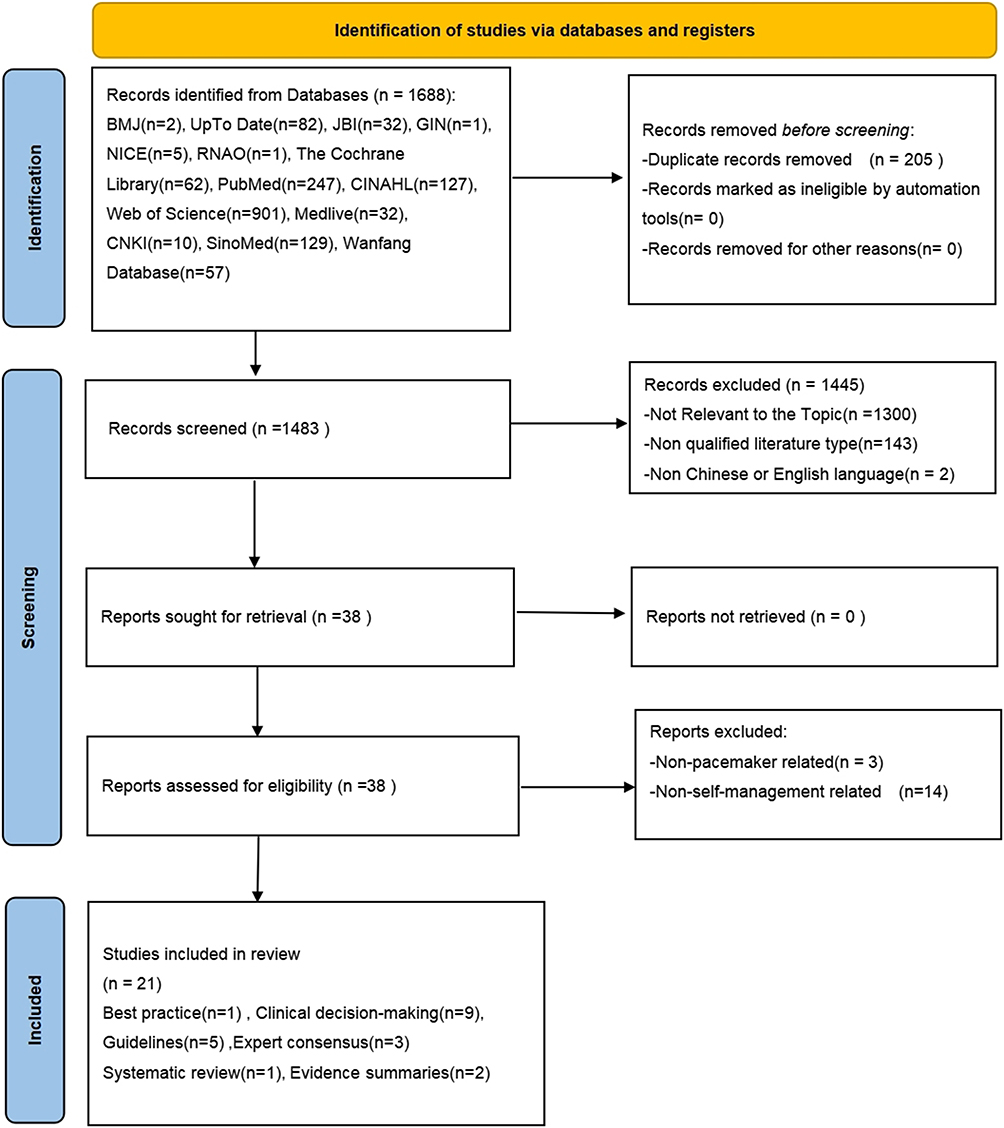 |
Figure 1 Flow chart of literature screening. Abbreviations: BMJ, British Medical Journal Best Practice; JBI, Joanna Briggs Institute; GIN, Guidelines International Network; NICE, National Institute for Health and Care Excellence; RNAO, Registered Nurses Association of Ontario; CNKI, China National Knowledge Infrastructure. |
Quality Evaluation Results of the Included Literature
Quality Evaluation Results of Guidelines
Five guidelines32–36 were included in this study and the evaluation results indicated a grade of “A”, demonstrating the exemplary quality of the evidence summary. The comprehensive evaluation results of the guides’ quality was presented in Table 3.
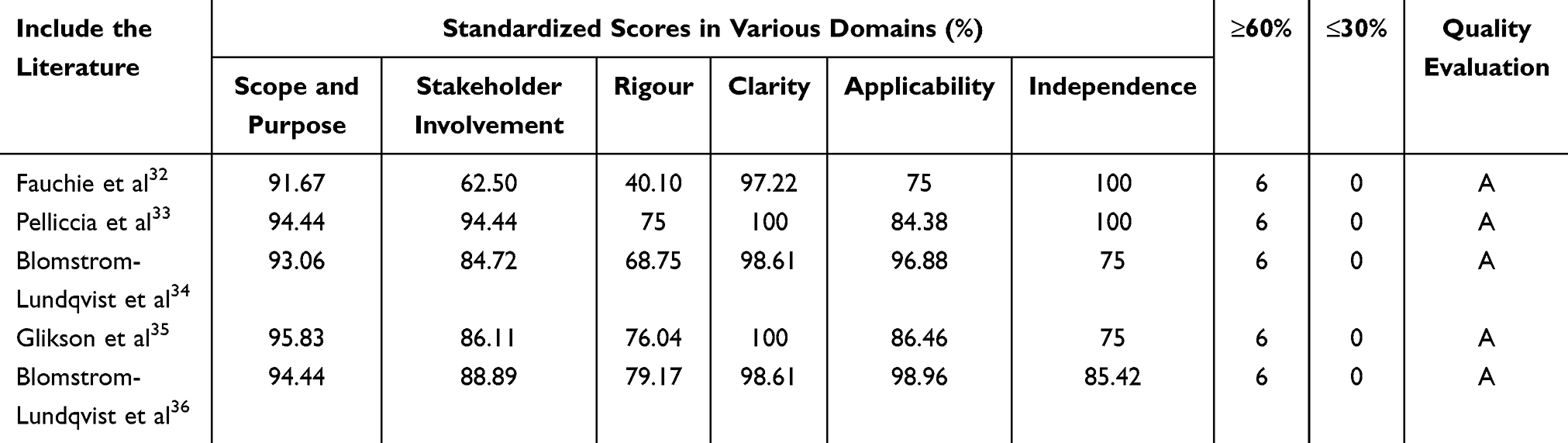 |
Table 3 Quality Evaluation Results of the Guidelines (n = 5) |
Quality Evaluation Results of Expert Consensus
A total of 3 expert consensuses37–39 were included in this study. After quality assessment, all of them were incorporated, and the evaluation results are shown in Table 4.
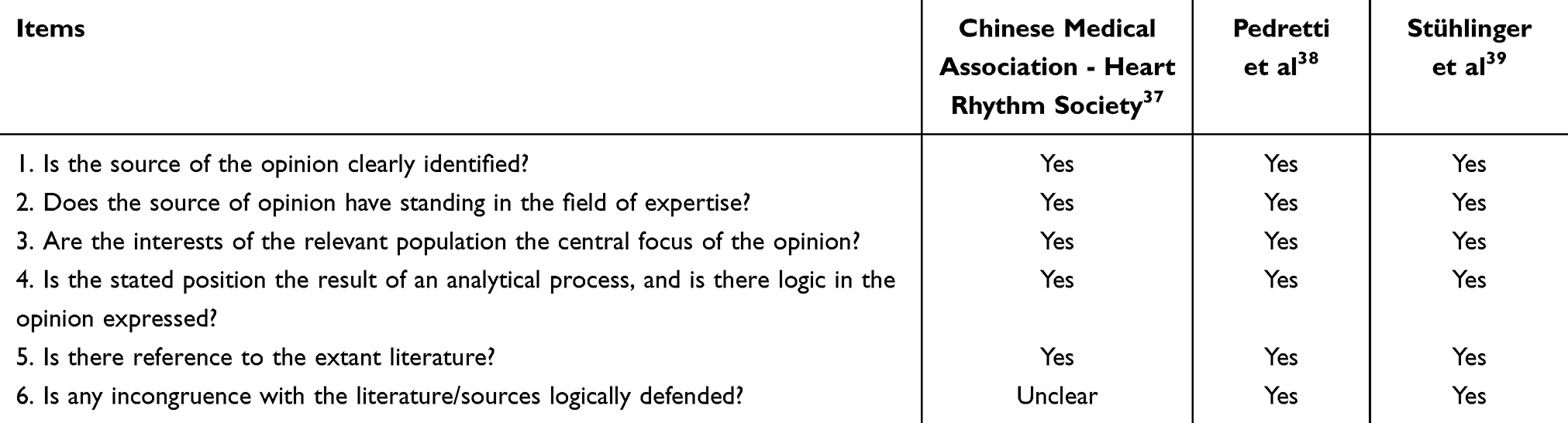 |
Table 4 Quality Evaluation of the Expert Consensus (n=3) |
Quality Evaluation Results of Systematic Reviews
One systematic review40 was incorporated. For item 9 “Was the possibility of publication bias assessed?”, the evaluation result was “Not applicable”. In contrast, all other items were assessed positively as “Yes”. The material was widely regarded as having a high overall quality.
Quality Evaluation Results of Evidence Summary
This study included 2 evidence summaries41,42 that were evaluated using the CASE checklist. For Fangfang Chen’s evidence summary, the evaluation result of item 9 “Were potential biases avoided?” was “Partially Yes”, while the evaluation results of all the other items were “Yes”. For Ruiqing Di’s evidence summary, the evaluation results of all items were “Yes”. Both of the two evidence summaries are of high exemplary quality.
Summary of Evidences
A total of 35 pieces of best evidence were summarized in this study, which were divided into seven evidence themes: complication management, electromagnetic interference management, sports rehabilitation management, operative limb management, follow-up management, role management, and emotional management. Figure 2 visually illustrates these seven themes along with their key evidence, and labels the corresponding evidence items. The detailed descriptions, sources, and quality levels of the evidence are listed in Table 5.
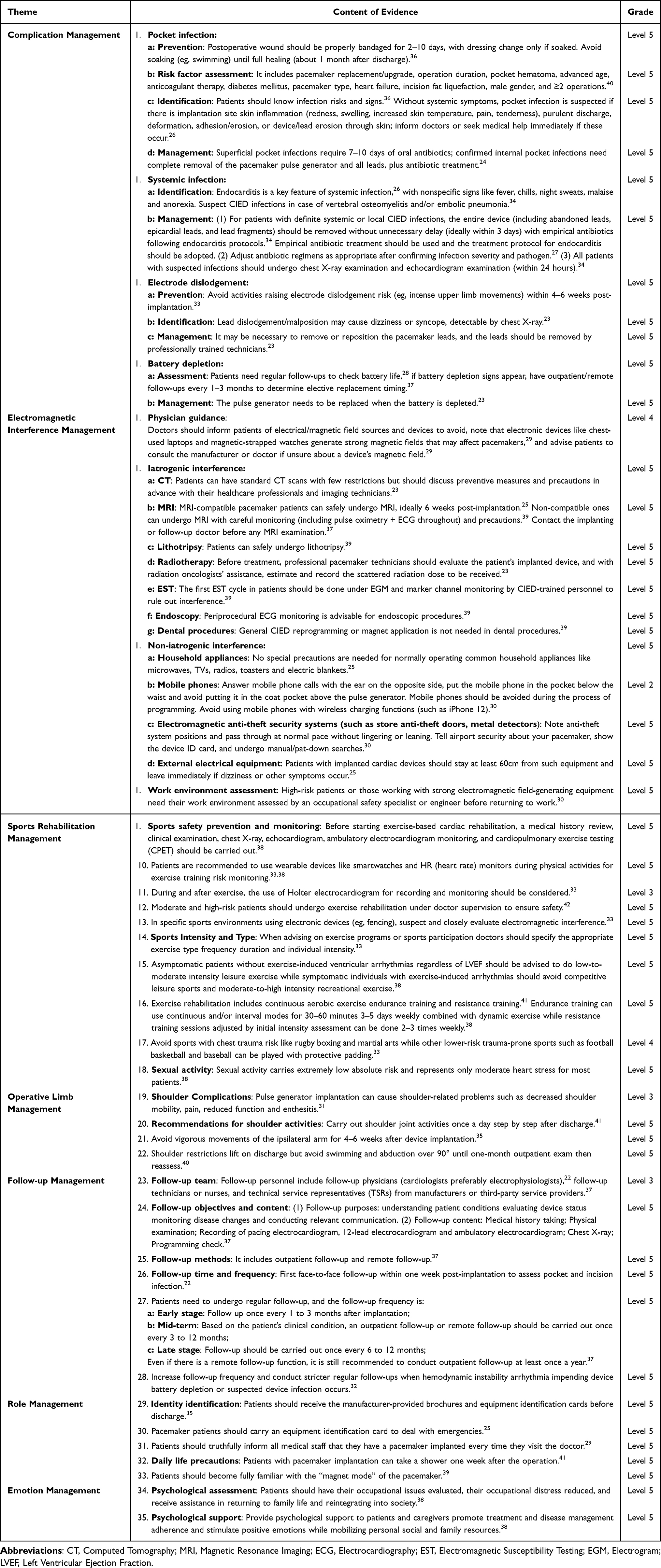 |
Table 5 Best Evidence Summary for Home-Based Self-Management in Patients with Permanent Pacemaker Implantation |
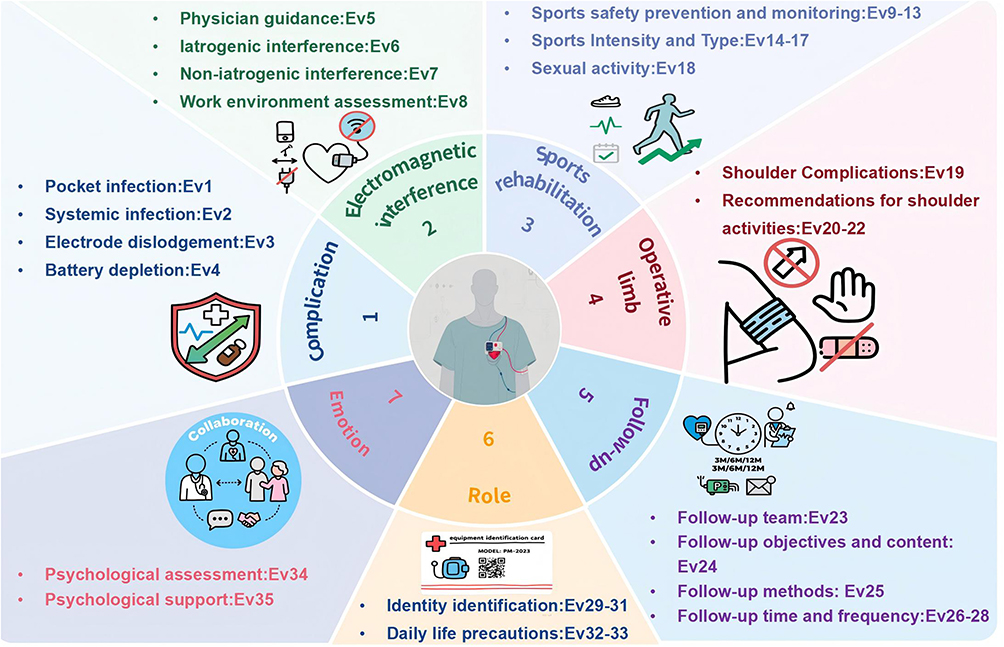 |
Figure 2 Key Evidence for home-based self-management in patients with permanent pacemaker implantation. Abbreviation: Ev, Evidence. |
Discussion
In light of Corbin & Strauss’s self-management model,43 self-management is divided into disease management, role management, and emotional management. Relying on the self-management model, this study has summarized the relevant evidence concerning home-based self-management of patients who have received permanent cardiac pacemaker implantation.43 Detailed information was furnished for patients from seven perspectives, namely complication management, electromagnetic interference management, sports rehabilitation management, operative limb management, follow-up management, role management, as well as emotion management. Through multi-dimensional and systematic management strategies, scientific and standardized home care guidance is provided for patients, which can effectively enhance patients’ self-management ability and improve the long-term prognosis.
Effective Self-Management Contributes to Lowering Complication Risks
Evidence items 1–4 regarding the complication management in this study summarized several common postoperative complications and provided patients with professional information related to diseases for prevention, identification and treatment respectively. Effective self-management by patients can enhance their vigilance towards the early signs of infection, such as redness, swelling, heat, and pain at the incision site,44 and their early detection and reporting of these symptoms may facilitate timely intervention, thereby preventing the spread of infection. However, Some research findings45,46 have demonstrated that after being discharged from the hospital, patients not only have insufficient understanding of complications and their management and lack relevant knowledge regarding disease management, but also have an eagerness for the support of professionals and a great demand for professional care related to permanent pacemakers. Providing patients with information related to permanent pacemakers and disease knowledge can assist them in detecting problems in a timely manner and reducing the incidence rate of complications.46 Therefore, it is recommended that clinical nurses make full use of the evidence from this study, adopt effective measures and conduct targeted health education for patients with permanent pacemaker implantation. By providing professional guidance to them, patients can fully understand and master the scientific information on home self-management, which facilitates their performance in self-disease management, effectively improves prognosis and enhances the quality of life.
Strengthening Patients’ Awareness of the Risks of Electromagnetic Interference is Crucial for Ensuring Their Home Safety
The management of electromagnetic interference is a crucial part of the home self-management for patients with pacemakers. Although modern pacemakers have enhanced anti-interference capabilities in their design, the electromagnetic fields that are ubiquitous in daily life and medical environments may still have an impact on the function of pacemakers.47 Electromagnetic interference may cause abnormal functions of the pacemaker. For example, it can inhibit pacing (resulting in bradycardia) or trigger inappropriate rapid discharges.48 Electromagnetic interference may come from a variety of sources, including medical devices, household appliances, and even new types of electronic devices.48,49 However, with the popularization of new types of household appliances and portable electronic devices, it is difficult for patients to clearly identify which devices can interfere with the pacemaker and the extent of the interference. Patients’ lack of awareness of these risks may lead them to overlook potential sources of electromagnetic interference (EMI) in their daily lives, or fail to fully inform medical staff about the fact that they have a pacemaker when seeking medical treatment, thus increasing the risk of EMI occurrence. Therefore, Evidence 6–8 summarizes the common situations of electromagnetic interference in both iatrogenic and non-iatrogenic scenarios, and elaborates in detail on the relevant preventive measures, which can provide practical guidance for patients. In the future, medical institutions should strengthen patient education. In addition to conducting routine health education during hospitalization, they can also develop mobile phone applications to send reminders and alarms to patients, which can deepen patients’ understanding and help them achieve more effective home-based self-management.
Scientific Sports Rehabilitation Training and Management of the Limb Operated on Can Effectively Improve the Quality of Life of Patients
A study has pointed out that patients with permanent pacemaker implantation have a relatively high incidence rate of postoperative kinesiophobia, and the incidence rate of shoulder-related problems or shoulder function impairment within three months after the operation is as high as 60%.41 The possible reasons are that patients keep the operative limb immobilized for a long time due to the fear of pain or concerns about the occurrence of postoperative complications, which leads to limited movement of the shoulder joint. Over time, this has adverse effects on patients’ physical and psychological conditions and reduces their quality of life.50 It can be seen from this that exercise rehabilitation is of great importance to the medical management of diseases in patients with permanent pacemaker implantation. Based on this, this study has aggregated the relevant evidence in two aspects, namely exercise rehabilitation management and operative limb management. The evidence suggests that exercise rehabilitation guidance should be provided for patients after the operation. For patients without clinical symptoms and without exercise-induced ventricular arrhythmia, it is recommended that they participate in low-to-moderate intensity physical activities.38 However, the study38 also pointed out that since the majority of patients with permanent pacemaker implantation are elderly patients, they may have comorbidities at varying levels, such as congestive heart failure, myocardial infarction, and so on. Moreover, inappropriate exercise may result in the occurrence of complications like lead dislocation or cardiac arrhythmia. Therefore, evidence items 9–13 in this study provide recommendations for safety precautions and monitoring during exercise to ensure the safety of exercise rehabilitation. Evidence items 14–18 recommend formulating individualized exercise plans for patients, including the most appropriate intensity, types of exercise, frequency, and duration. Previous studies have verified that exercise rehabilitation after surgery can optimize patients’ cardiac function and exercise capacity, with remarkable long-term prognosis.51 Therefore, it is necessary for clinical professionals to formulate personalized exercise plans for patients in the future, conduct more high-quality research, explore exercise rehabilitation programs that are specific, safe and effective for postoperative patients in our country, encourage and guide patients to exercise, so as to relieve patients’ pain and improve their comfort.
Attach Importance to the Follow-Up Management of Patients and Improve the Follow-Up Compliance
As an electronic device, the permanent pacemaker still requires regular follow-up for the programming of its working status after implantation. However, in clinical practice, the phenomenon of emphasizing implantation while neglecting follow-up is quite prominent.52 Discharged patients and their family members often overlook the importance of follow-up. In addition, studies have indicated that the outpatient follow-up rate of pacemaker patients in China is only between 55% and 65%.53 Therefore, evidence item 23 summarizes the professional follow-up team required in the follow-up management of permanent pacemakers, especially the establishment of the positions of follow-up technicians or nurses. Evidence items 24 to 28 summarize the purposes and contents of follow-up, as well as the methods and frequencies that patients and their family members need to be aware of. On the one hand, this can enhance patients’ awareness of the importance of regular follow-up. On the other hand, it also provides patients with relevant information regarding follow-up management. Regular follow-up can not only prevent the occurrence of complications but also have a positive impact on patients’ psychological state and alleviate their negative emotions.54 Therefore, hospitals are in urgent need of further optimizing various management systems related to follow-up, focusing on strengthening the training of professional personnel and comprehensively improving the professional qualities of the follow-up team. Meanwhile, when providing guidance to patients after discharge, clinical medical staff should focus on explaining the significance of follow-up work to the patients and their families, and meticulously inform them of the specific procedures, contents, expected results and other relevant key knowledge points of follow-up work, ensuring the smooth progress of patients’ subsequent rehabilitation.
Clear Role Perception and a Positive Psychological Status Can Contribute to Enhancing Patients’ Enthusiasm and Perseverance in Self-Management
The implantation of a permanent pacemaker represents a long-term process in which the patient and the implanted device coexist and adapt to each other. During this period, patients need to learn to accommodate the changes in lifestyle, as well as the rights and obligations of their family roles brought about by the implantation of the pacemaker. In self-management, role management involves patients maintaining, changing or creating meaningful behaviors to adapt to new life roles.55 Therefore, evidence items 29 to 33 in this study indicate that patients need to make changes in their self-identity and daily life behaviors, such as in medical consultation and bathing, to ensure that permanent pacemakers can serve patients safely and effectively. Patients with permanent pacemaker implantation may experience a series of negative emotions after surgery, such as anxiety, depression, and self-perceived burden, and these emotions may not show significant improvement for a long period of time.56 Emotion management refers to patients’ self-coping with and management of various negative emotions.55 Evidence items 34 to 35 suggest that medical staff should conduct psychological assessments on patients and provide appropriate psychological support. However, at present, the relevant evidence regarding role management and emotion management for patients with permanent pacemaker implantation in clinical practice is limited, and there is still a lack of high-quality evidence. Currently, some scholars have already conducted studies on the impacts of different psychological interventions on patients’ negative emotions. However, there are few relevant studies on patients’ self-intervention. Therefore, it is recommended that relevant original research can be further carried out in the future to supplement the evidence related to role management and emotion management for patients with permanent pacemaker implantation, and to promote the overall level of patients’ home-based self-management.
Cultural Considerations in Home-Based Self-Management Practices
While the current evidence synthesis provides guidance for home-based self-management in patients with permanent pacemakers, successful implementation requires careful consideration of cultural differences between Eastern and Western contexts. Research indicates that variations in cultural norm, regional, and healthcare system significantly influence patients’ health beliefs and self-management behaviors.57–60 Western healthcare paradigms typically emphasize patient autonomy,61 particularly in digital self-monitoring, where patients seek to take primary responsibility for managing their devices through digital health platforms and independent decision-making.62,63 This approach typically encourages patients to take an active and independent role in monitoring symptoms and adhering to follow-up schedules. In contrast, within East Asian cultural contexts that emphasize family involvement in healthcare decision-making, patients typically demonstrate greater reliance on familial support, with relatives actively participating in medication reminders, lifestyle modifications, and care-related decisions.64,65 Moreover, cultural attitudes toward physical activity also differ. Western guidelines typically encourage the early resumption of moderate exercise, whereas Chinese patients may exhibit greater caution or even inactivity, shaped by the traditional health belief in “conserving energy” after surgery.66 Furthermore, regional disparities in healthcare accessibility cannot be ignored. Urban patients have access to structured cardiac rehabilitation programs and convenient specialist follow-ups, while rural populations often face challenges such as limited medical resources, low health literacy, and financial constraints.67 Therefore, contextual adaptation of the practical application of evidence-based evidence, based on cultural norms and regional healthcare capacities, is crucial to ensuring its effectiveness in diverse clinical settings.
Summary and Perspectives
Limitations of this study: (1) The included literature lacks original studies such as randomized controlled trials, and this potential bias may weaken the strength of the evidence-based recommendations. (2) The included literature has regional and population differences, which may limit the generalizability of evidence related to patients’ home-based self-management in different contexts. (3) The literature search was restricted to English and Chinese databases, with no inclusion of literature in other languages. This may lead to selection bias and overlook valuable evidence from non-English/non-Chinese sources.
The implications of this study for clinical practice and future research: (1) When applying evidence clinically, personalized and feasible self-management plans should be formulated based on patients’ cultural backgrounds, living habits and local medical standards. (2) Clinical staff should establish multidisciplinary teams to provide systematic guidance tailored to individual patients, and improve patients’ and their families’ awareness of and compliance with self-management through targeted health education to ensure effective application of evidence. (3) More high-quality original studies should be conducted in the future to accumulate abundant high-quality evidence and consolidate the evidence-based foundation of self-management strategies. (4) The evidence repository should be continuously updated with timely inclusion of new research findings to enhance the robustness and adaptability of recommendations.
Conclusion
This study summarized 7 aspects of complication management, electromagnetic interference management, exercise rehabilitation management, operative limb management, follow-up management, role management, and emotion management in patients implanted with permanent pacemakers, with a total of 35 best pieces of evidence, providing a structured evidence-based basis for the home-based self-management of patients with permanent pacemaker implantation in clinical practice. However, in the process of clinical promotion, full attention should be paid to patients’ cultural backgrounds and regional differences in medical resources, and personalized guidance should be implemented to ensure the relevance of evidence application. Future research should conduct more original studies to enrich the evidence-based foundation of the evidence repository. Meanwhile, the dynamic update of the evidence repository must be guaranteed, and scientific screening should be carried out based on the verification results of the feasibility, applicability, and effectiveness of evidence in clinical practice. By continuously optimizing home-based self-management strategies for patients with permanent pacemakers, the patients’ quality of life will ultimately be improved.
Funding
This work was supported by Yunnan health training project of high level talents grant (D-2024023) and Yunnan Provincial Department of Education Scientific Research Fund Project (2024J0212).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Steffen MM, Osborn JS, Cutler MJ. Cardiac implantable electronic device therapy: permanent pacemakers, implantable cardioverter defibrillators, and cardiac resynchronization devices. Med Clin North Am. 2019;103(5):931–943. doi:10.1016/j.mcna.2019.04.005
2. Center for Cardiovascular Diseases The Writing Committee of the Report on Cardiovascular HDIC, N. Report on cardiovascular health and diseases in China 2023: an updated summary. Biomed Environ Sci. 2024;37(9):949–992. doi:10.3967/bes2024.162
3. Cecchin F, Halpern DG. Cardiac arrhythmias in adults with congenital heart disease: pacemakers, implantable cardiac defibrillators, and cardiac resynchronization therapy devices. Card Electrophysiol Clin. 2017;9(2):319–328. doi:10.1016/j.ccep.2017.02.013
4. Herry M, Laghlam D, Touboul O, et al. Pacemaker implantation after aortic valve replacement: rapid-deployment Intuity® compared to conventional bioprostheses. Eur J Cardiothorac Surg. 2020;58(2):335–342. doi:10.1093/ejcts/ezaa068
5. Mahmood A, Andrews R, Fenton M, et al. Permanent pacemaker implantation after pediatric heart transplantation: risk factors, indications, and outcomes. Clin Transplant. 2019;33(4):e13503. doi:10.1111/ctr.13503
6. Min W, Weigang L. Analysis of life time and influencing factors after pacemaker implantation. Shaanxi Med J. 2018.
7. Holroyd KA, Creer T. Self-management of chronic disease: handbook of clinical interventions and research. Patient Educ Couns. 1986.
8. Corbin JM, Strauss A. A nursing model for chronic illness management based upon the Trajectory Framework. Sch Inq Nurs Pract. 1991;5(3):155–174. doi:10.1891/0889-7182.5.3.155
9. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. doi:10.1016/S0738-3991(02)00032-0
10. Sridhar AR, Yarlagadda V, Yeruva MR, et al. Impact of haematoma after pacemaker and CRT device implantation on hospitalization costs, length of stay, and mortality: a population-based study. Europace. 2015;17(10):1548–1554. doi:10.1093/europace/euv075
11. Özcan C, Raunsø J, Lamberts M, et al. Infective endocarditis and risk of death after cardiac implantable electronic device implantation: a nationwide cohort study. Europace. 2017;19(6):1007–1014. doi:10.1093/europace/euw404
12. Qingmei T, Xinghe S, Le G, Wei Z, Wei L, Feng S. Incidence of major adverse events associated with cardiac pacemaker implantation: a meta-analysis. Chin Gen Pract. 2019;22(11):1334.
13. Lin Y, Liu HH, Chen YT. Research on psychological issues in patients with implanted cardiac rhythm devices. Chin J Clin. 2022;2022(006):050.
14. Khalil HH, Soliman MS, Ahmed HA, Hamza EA. Effect of Educational Program on Outcomes of Patients Undergoing Permanent Pacemakers’ Implantation. Evidence-Based Nurs Res. 2020;2(4):13. doi:10.47104/ebnrojs3.v2i4.167
15. Hanaa A, Ebtisam M. Home care for patients with permanent pacemaker insertion. IOSR J Nurs Health Sci. 2017;6(4):49–57.
16. Udo EO, van Hemel NM, Zuithoff NP, et al. Long term quality-of-life in patients with bradycardia pacemaker implantation. Int J Cardiol. 2013;168(3):2159–2163. doi:10.1016/j.ijcard.2013.01.253
17. Peng F, Wang H, Li J, et al. Best evidence summary for prevention and management of enteral feeding intolerance in critically ill patients. J Clin Nurs. 2024;33(3):781–796. doi:10.1111/jocn.16934
18. Munn Z, Lockwood C, Moola S. The development and use of evidence summaries for point of care information systems: a streamlined rapid review approach. Worldviews Evid Based Nurs. 2015;12(3):131–138. doi:10.1111/wvn.12094
19. Alper BS, Haynes RB. EBHC pyramid 5.0 for accessing preappraised evidence and guidance. Evidence Based Med. 2016;21(4):123–125. doi:10.1136/ebmed-2016-110447
20. Hoffmann-Eßer W, Siering U, Neugebauer EA, Brockhaus AC, Lampert U, Eikermann M. Guideline appraisal with AGREE II: systematic review of the current evidence on how users handle the 2 overall assessments. PLoS One. 2017;12(3):e0174831. doi:10.1371/journal.pone.0174831
21. Foster MJ, Shurtz S. Making the Critical Appraisal for Summaries of Evidence (CASE) for evidence-based medicine (EBM): critical appraisal of summaries of evidence. J Med Libr Assoc. 2013;101(3):192–198. doi:10.3163/1536-5050.101.3.008
22. Olshansky B. Pacemaker - Follow-up. 2023. Available from: https://bestpractice.bmj.com/topics/zh-cn/832/monitoring.
23. Link MS. Pacing system malfunction: evaluation and management. 2024. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/zh-Hans/pacing-system-malfunction-evaluation-and-management?search=Pacing%20system%20malfunction%3A%20Evaluation%20and%20management&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
24. Kwaku KF. Cardiac implantable electronic devices: long-term complications. 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/cardiac-implantable-electronic-devices-long-term-complications?search=Cardiac%20implantable%20electronic%20devices%3A%20Long-term%20complications&source=search_result&selectedTitle=1~150&display_rank=1.
25. Olshansky B. Patient education: pacemakers (Beyond the Basics). 2024. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/pacemakers-beyond-the-basics?search=Patient%20education%3A%20Pacemakers%20(Beyond%20the%20Basics)&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
26. Karchmer AW. Infections involving cardiac implantable electronic devices: epidemiology, microbiology, clinical manifestations, and diagnosis. 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/zh-Hans/infections-involving-cardiac-implantable-electronic-devices-epidemiology-microbiology-clinical-manifestations-and-diagnosis?search=Infections%20involving%20cardiac%20implantable%20electronic%20devices%3A%20Epidemiology%2C%20microbiology%2C%20clinical%20manifestations%2C%20and%20diagnosis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
27. Karchmer AW. Infections involving cardiac implantable electronic devices: treatment andprevention. 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/infections-involving-cardiac-implantable-electronic-devices-treatment-and-prevention?search=Infections%20involving%20cardiac%20implantable%20electronic%20devices%3A%20Treatment%20and%20prevention&source=search_result&selectedTitle=1~150&display_rank=1.
28. Knight BP. Cardiac implantable electronic devices: patient follow-up. 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/zh-Hans/cardiac-implantable-electronic-devices-patient-follow-up?search=Cardiac%20implantable%20electronic%20devices%3A%20Patient%20follow-up&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
29. Crowley K, Hume K, Martin KA, McLaurin M. Patient education: pacemakers (The Basics). 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/pacemakers-the-basics.
30. Link MS. Cardiac implantable electronic device interactions with electromagnetic fields in the nonhospital environment. 2025. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/cardiac-implantable-electronic-device-interactions-with-electromagnetic-fields-in-the-nonhospital-environment.
31. Kwaku KF. Cardiac implantable electronic devices: periprocedural complications. 2024. Available from: http://www--uptodate--cn--https.uptodatecn.slyy.qfclo.com:2222/contents/zh-Hans/cardiac-implantable-electronic-devices-periprocedural-complications?search=Cardiac%20implantable%20electronic%20devices%3A%20Periprocedural%20complications&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
32. Fauchier L, Alonso C, Anselme F, et al. Position paper for management of elderly patients with pacemakers and implantable cardiac defibrillators: groupe de Rythmologie et Stimulation Cardiaque de la Société Française de Cardiologie and Société Française de Gériatrie et Gérontologie. Arch Cardiovasc Dis. 2016;109(10):563–585. doi:10.1016/j.acvd.2016.04.004
33. Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: the Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur Heart J. 2021;42(1):17–96. doi:10.1093/eurheartj/ehaa605
34. Blomström-Lundqvist C, Traykov V, Erba PA, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Europace. 2020;22(4):515–549. doi:10.1093/europace/euz246
35. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA). Rev Esp Cardiologia. 2022;75(5):430.
36. Blomstrom-Lundqvist C, Ostrowska B. Prevention of cardiac implantable electronic device infections: guidelines and conventional prophylaxis. Europace. 2021;23(Suppl 4):iv11–19. doi:10.1093/europace/euab071
37. Electrophysiology CMAoPa, Chinese Medical Doctor Association HRSC. Expert consensus on the follow-up of cardiovascular implantable electronic devices (2020). Chin J Card Arrhythmia. 2020;24(6):532–544.
38. Pedretti RFE, Iliou MC, Israel CW, et al. Comprehensive multicomponent cardiac rehabilitation in cardiac implantable electronic devices recipients: a consensus document from the European Association of Preventive Cardiology (EAPC; Secondary prevention and rehabilitation section) and European Heart Rhythm Association (EHRA). Eur J Prev Cardiol. 2021;28(15):1736–1752. doi:10.1093/eurjpc/zwaa121
39. Stühlinger M, Burri H, Vernooy K, et al. EHRA consensus on prevention and management of interference due to medical procedures in patients with cardiac implantable electronic devices. Europace. 2022;24(9):1512–1537. doi:10.1093/europace/euac040
40. Limei C, Lingling S, Jieshan C. Risk factors for pacemaker pocket infection: a meta analysis. South China J Cardiovasc Dis. 2022;28(3):246–250.
41. Fangfang C, Linxiao Y, Yan H, Yahua Z. Best evidence summary of early exercise rehabilitation after pacemaker implantation. J Nurs. 2022;29(8).
42. Ruiqing D, Zheng H, Huifang H, Siyu L. Summary of the best evidence for risk stratification of exercise rehabilitation in patients with a cardiac implantable electronic device. Front Cardiovasc Med. 2024;11:1455486. doi:10.3389/fcvm.2024.1455486
43. Corbin JM. The corbin and strauss chronic illness trajectory model: an update. Sch Inq Nurs Pract. 1998;12(1):33–41.
44. Saliba É, Massie E, Sia YT. Review of cardiac implantable electronic device related infection. Res Rep Clin Cardiol. 2016;7:137–146. doi:10.2147/RRCC.S75682
45. Zhiying S, Feng Z, Zhuqin Z, Manhui H. A qualitative research on the psychological experience of patients after permanent pacemaker implementation. Nurs J Chin People’s Liberat Army. 2018.
46. Rayamajhi N, Sharma K, Mahotra NB, Aryal B. Knowledge and practice regarding self-care management among patients with permanent pacemaker at cardiac center. J Nepal Health Res Counc. 2021;19(2):355–361. doi:10.33314/jnhrc.v19i2.3491
47. Steffel J. Electromagnetic interference in pacemaker patients. ESC CardioMed. 2018.
48. Samuels JM, Overbey DM, Wikiel KJ, Jones TS, Robinson TN, Jones EL. Electromagnetic interference on cardiac pacemakers and implantable cardioverter defibrillators during endoscopy as reported to the US Federal Drug Administration. Surg Endosc. 2021;35(7):3796–3801. doi:10.1007/s00464-020-07872-2
49. Juan L, Peng YG. Cardiovascular implantable electronic devices: perioperative management for anesthesiologists. Perioper Care Oper Room Manag. 2023;33.
50. Girgenti R, Buttafarro MA, Ammirata M, La Russa A, Agnese V, Messina M. Quality of life and psychological distress in a cohort of patients with left ventricular assist device. G Ital Cardiol. 2021;22(3):233–238. doi:10.1714/3557.35343
51. Nazir A. Exercise as a modality to improve heart transplantation-related functional impairments: an article review. World J Transplant. 2024;14(3):91637. doi:10.5500/wjt.v14.i3.91637
52. Slotwiner D, Yu J, Zhang M, Al-Khatib SM. Cardiac implantable electronic device patient follow-up: assessment of U.S. practice. Heart Rhythm. 2024.
53. Yuexiang Z, Zhaoliang S, Hongyang G, Kun L, Jianping G. The follow-up study for clinical compliance in patients with permanent pacemaker implantation. Chin Circ J. 2014.
54. Donglin X, Chengen M, Sujia W. Regular follow-up and pacemaker parameter program on psychological conditions of patients with a cardiac pacemaker. J Shandong Univ. 2008.
55. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
56. Sikora K, Łuczyk RJ, Wawryniuk A, Łuczyk M, Zwolak A. Anxiety and depression intensity and the quality of life of patients with an implanted pacemaker. J Educ Health Sport. 2021;11(6):170–177. doi:10.12775/JEHS.2021.11.06.018
57. Snowden LR, Yamada A-M. Cultural Differences in Access to Care. Annu Rev Clin Psychol. 2005;1(1):143–166. doi:10.1146/annurev.clinpsy.1.102803.143846
58. Okeme ABK, Godwins OP, Gusen MJ, Gbaa T, Pam-Tok AO, Uwe VE. Understanding the impact of cultural factors on healthcare outcomes: a data-driven comparison of US and Nigerian Healthcare Systems. Am J Hum Psychol. 2024;2(1):146–158. doi:10.54536/ajhp.v2i1.3393
59. Liu X, Liu B. Superior medical resources or geographic proximity? The joint effects of regional medical resource disparity, geographic distance, and cultural differences on online medical consultation. Soc Sci Med. 2024;350:116911. doi:10.1016/j.socscimed.2024.116911
60. Hickson SV. Healthcare disparities. Clin Integr Care. 2024;22:100181. doi:10.1016/j.intcar.2023.100181
61. Todorovic Z, Protic D. Patient autonomy and informed consent in critically lll. Hosp Pharmacol - Int Multidiscip J. 2017;4(1):463–468. doi:10.5937/hpimj1701463T
62. Gilbar R, Miola J. One size fits all? On patient autonomy, medical decision-making, and the impact of culture. Med Law Rev. 2014;23(3):375–399. doi:10.1093/medlaw/fwu032
63. Robinson SA, Zocchi MS, Netherton D, et al. Secure messaging, diabetes self-management, and the importance of patient autonomy: a mixed methods study. J Gen Intern Med. 2020;35(10):2955–2962. doi:10.1007/s11606-020-05834-x
64. Wiedyaningsih C, Widyakusuma NN, Suryawati S. The role of family caregivers in medication adherence of elderly in Asian setting: a scoping review. Indones J Pharmacol Ther. 2023;4(2). doi:10.22146/ijpther.8379
65. Pan J-D, Ho KY, Guan G-F, et al. Asian family members’ participation in advance care planning: an integrative review. Palliat Med. 2025;39(3):373–390. doi:10.1177/02692163251317856
66. Rong X, Peng Y, Yu HP, Li D. Cultural factors influencing dietary and fluid restriction behaviour: perceptions of older Chinese patients with heart failure. J Clin Nurs. 2016;26:717–726. doi:10.1111/jocn.13515
67. Pierce JB, Ng SM, Stouffer JA, Williamson CA, Stouffer GA. Rural/Urban disparities in cardiovascular disease in the US—what can be done to improve outcomes for rural Americans? Am J Cardiol. 2025;248:10–15. doi:10.1016/j.amjcard.2025.03.033
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evidence Summary for Self-Management Education in Patients with Non-Alcoholic Fatty Liver Disease
Yang Y, Cao J, Zhang L, Liu J, Li M
Patient Preference and Adherence 2026, 20:590068
Published Date: 24 April 2026