Back to Journals » Clinical Interventions in Aging » Volume 15
Home-Based Cognitively Assistive Robots: Maximizing Cognitive Functioning and Maintaining Independence in Older Adults Without Dementia
Authors Van Patten R, Keller AV ![]() , Maye JE
, Maye JE ![]() , Jeste DV
, Jeste DV ![]() , Depp C, Riek LD, Twamley EW
, Depp C, Riek LD, Twamley EW ![]()
Received 12 March 2020
Accepted for publication 18 May 2020
Published 13 July 2020 Volume 2020:15 Pages 1129—1139
DOI https://doi.org/10.2147/CIA.S253236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Ryan Van Patten,1– 3 Amber V Keller,2 Jacqueline E Maye,4 Dilip V Jeste,1,3,5 Colin Depp,1,3 Laurel D Riek,6– 8 Elizabeth W Twamley1,2,4
1Department of Psychiatry, University of California San Diego, La Jolla, CA 92093, USA; 2Research Service, VA San Diego Healthcare System, San Diego, CA 92161, USA; 3Sam and Rose Stein Institute for Research on Aging, University of California San Diego, La Jolla, CA 92063, USA; 4Center of Excellence for Stress and Mental Health, VA San Diego Healthcare System, San Diego, CA 92161, USA; 5Department of Neurosciences, University of California San Diego, La Jolla, CA 92063, USA; 6Computer Science and Engineering, University of California San Diego, La Jolla, CA 92063, USA; 7Department of Emergency Medicine, University of California San Diego, La Jolla, CA 92063, USA; 8Contextual Robotics Institute, University of California San Diego, La Jolla, CA 92063, USA
Correspondence: Ryan Van Patten
Department of Psychiatry, University of California San Diego, 9500 Gilman Drive (9116A), La Jolla, CA 92093, USA
Tel +1540-649-4702
Fax +1 619-471-9017
Email [email protected]
Abstract: Promoting health and prolonging independence in the home is a priority for older adults, caregivers, clinicians, and society at large. Rapidly developing robotics technology provides a platform for interventions, with the fields of physically and socially assistive robots expanding in recent years. However, less attention has been paid to using robots to enhance the cognitive health of older adults. The goal of this review is to synthesize the current literature on home-based cognitively assistive robots (CAR) in older adults without dementia and to provide suggestions to improve the quality of the scientific evidence in this subfield. First, we set the stage for CAR by: a) introducing the field of robotics to improve health, b) summarizing evidence emphasizing the importance of home-based interventions for older adults, c) reviewing literature on robot acceptability in older adults, d) highlighting important ethical issues in healthcare robotics, and e) reviewing current findings on socially assistive robots, with a focus on translating findings to the CAR context. With this foundation in place, we then review the literature on CAR, identifying gaps and limitations of current evidence, and proposing future directions for research. We conclude that CAR is promising and feasible and that there is a need for more methodologically rigorous evaluations of CAR to promote prolonged home-based independence in older adults.
Keywords: aging, cognitive status, healthy aging, autonomy, successful aging, technology
Plain Language Summary
Most older people prefer to remain healthy and active in their homes rather than moving into assisted living centers. Technology is being used to help with this goal and one example of this is robots in the homes of older adults to assist them with their cognitive functioning. This paper reviews research on robots to help older adults stay cognitively healthy in their homes. We discuss robots in general, the importance of placing robots in the home rather than in nursing homes, ethical issues, and robots to help people remain socially engaged and mentally active. Finally, we conclude that robots to improve cognitive functions is a promising area of research and we provide suggestions for scientists to continue to make headway in this area.
Introduction
In light of the aging population, one approach to enhancing quality of life in older adults capitalizes on ongoing developments in the field of healthcare technology to support independence in the home.1,2 In particular, the subdiscipline of robotics is expanding and innovating at a rapid pace,3 driven by advancements in hardware, artificial intelligence (AI), and internet connectivity.4 However, empirical data on robots to promote healthy aging are still nascent,5 and researchers from foundational disciplines (eg, engineering/robotics, psychology, geriatrics, biology) have only recently begun developing the requisite interprofessional collaborations.6 Consequently, there is a great opportunity for scientific progress, and the movement to use robots to promote home-based health in older adults deserves our full attention.
One promising application of robotic interventions in older adults has occurred in the rapidly-expanding field of socially assistive robots (SAR),7,8 where SAR represents the integration of assistive robots and socially intelligent robots leveraged to improve social health. However, despite the fact that cognitive skills such as language, memory, and executive functions are also integral to functional status and overall wellness,9–11 less attention has been paid to using robots to enhance the cognitive health of older adults.12,13 In order to delineate and then fuel this line of inquiry, we propose the construct of cognitively assistive robots (CAR) to refer to robots designed to support healthy cognitive functioning. Given the centrality of cognition to independence and quality of life in aging populations in particular, we aim to synthesize the available research pertaining to cognitive robotic interventions in older adults. Additionally, we emphasize robots specifically tailored to promote autonomy in the home, as this is a key objective of older adults themselves,14,15 as well as secondary and tertiary stakeholders such as caregivers, physicians, and policymakers.3,16 Consequently, we focus our conceptual review on older adults without dementia (ie, those who are cognitively healthy and/or those who have mild cognitive impairment [MCI]).17 First, we set the stage with a brief discussion of older adults in home environments and then we transition to three core issues related to healthcare robots in older adults: a) acceptability, b) ethics, and c) efficacy/effectiveness of SAR in older adults. Finally, we review the available research in CAR and conclude with recommendations for future CAR investigations. Overall, we believe that the successful implementation of home-based CAR as we describe it could a) improve quality of life for older adults by allowing for prolonged independent aging in place, b) reduce demand on caregivers for older adults with cognitive decline, and c) attenuate healthcare costs by delaying institutionalization for as long as is safe and feasible.
In reviewing the literature in SAR and CAR, it became evident that the relevant studies are heterogeneous in terms of aims and scope of the publishing journal (eg, engineering/robotics, psychology, medicine), style of publication (eg, scientific article, conference proceeding, technical report), and type of data presented (eg, literature review, qualitative observation, single subject design, technical robot description, group-based quantitative evaluation). That is, the literature is scattered across disciplines, early data on CAR are embedded in papers on other topics (eg, SAR), and conventional search terms (eg, “cognitive robot”) did not produce manuscripts on robotic interventions to improve cognition. Consequently, a systematic review and/or meta-analysis might omit important aspects of the literature (see, eg, Alnajjar et al)13 and we believe that a conceptual review is the most appropriate method for presenting available research. In order to implement the review, we explored the SAR literature, with a focus on a wide array of search terms in multiple databases, as well as references from recent papers.
Home Environments
Most people prefer to age in place, remaining self-sufficient in their own homes rather than transitioning into assisted living facilities.14 Aging in place is associated with better mental health and well-being,18 as well as with lower healthcare costs.16 Interventions to promote home-based autonomy can be as simple as hand rails in the shower and ramps leading into doorways,19 although mild to moderate cognitive impairments would likely require more significant support. Older adults who do transition to assisted living environments frequently do so out of necessity rather than personal choice, often due to declines in cognitively mediated instrumental activities of daily living (IADLs) such as financial management.15 Consequently, cognitive interventions to maintain independence in IADLs and allow older adults to age comfortably in place are highly desirable.18
Social robots offer a promising mode of service delivery for interventions targeting cognitive and functional abilities.12,15,20 However, the majority of this research has been conducted in institutions such as skilled nursing facilities rather than older adults’ homes,12,21 likely because studies in home environments require more resources per participant.22 Moreover, the significant differences in institutions compared to private homes have implications for the initial design of the robots, as well as for the eventual interpretation of research results;15 consequently, studies conducted in institutional settings may not apply directly to home settings. Importantly, although the home-based older adult robotics literature is still growing, several publications on robots created for in-home care have provided early support. For example, Kidd and Breazeal23 demonstrated success of a home-based robotic weight loss coach in 45 adults, Tsai et al24 reported on the development of a telepresence robot designed to allow older adults to communicate easily with friends and family, and Orejana et al20 showed that robots in the homes of four older adults reduced utilization of healthcare resources and enhanced quality of life. These studies provide preliminary evidence of feasibility in home environments and set the stage for more methodologically rigorous experimental work in the future.
Acceptability
Unfortunately, the idea of autonomous robots engenders fear and unease for many people, likely due in part to decades of media and science fiction portrayals of robots as malevolent entities.25,26 Older adults in particular can be slow to adopt new technologies,27 including robots,28 and their reticence may be related to the concern that using an assistive device signals dependency and fragility.29 Indeed, schemas related to helplessness and disability can become embedded in the morphology, functionality, and communication style of products, and robots that communicate ageist messages are likely to be met with resistance and/or rejection.29–31 Consequently, we advocate for the rejection of a deficit model of aging in robot design, instead replacing it with evidence-based social models of aging, emphasizing appreciation of resilience and reserve over weakness and disability,31 and likely enhancing the acceptance and ultimate success of robot-based interventions.
Although, on average, older adults are less apt to embrace new technology than are younger adults, a subset of older individuals are receptive toward and enjoy interacting with robots,1,32 including in their homes.33 Meanwhile, for those older people who are hesitant to adopt non-biased robots, real-world interactions can improve overall attitudes and interest in future use.34,35 Moreover, we believe that embedding the creation of assistive robots into a well-supported engineering framework such as human-centered design36 may further enhance acceptance. Finally, on a broader level, robot acceptability may increase over time, even in the absence of intervention, as newer cohorts of aging adults (eg, Generation X, Millennials) will have more life experience with computerized devices.37
When considering the design of acceptable robotic interventions in the near-term, existing literature provides several insights into the specific system characteristics that will be most appealing and effective in aging populations. First and foremost, older adults prefer devices that are easy to use and healthcare robots are more effective when designed in a simple, straightforward manner.3,12,29,38 Second, robots should be personalized and adaptable.3,6,28,29,39 No single physical shape or behavioral pattern will suit every user, and allowing for personalization and choice (eg, regarding color) is associated with more positive user experiences.40 Third, regarding robot morphology, multiple investigators have reported that small size (eg, maximum height: 125cm in Broadbent et al;29 maximum weight: 1.6kg in Hutson et al)28 and moderately anthropomorphized features41 are desirable to older adults. In contrast, large, fully humanoid robots are unappealing and tend to evoke a sense of unease, consistent with the “uncanny valley” hypothesis.42 Fourth, with respect to personality, sociability (eg, initiating conversations spontaneously, exhibiting affect and humor) appears to engender positive reactions28,43 and matching robot to user personality has received support as well.44,45
Ethical Issues
Above and beyond acceptability, there are important ethical concerns to examine prior to the implementation of healthcare robots such as SAR and CAR in older adult populations. Similar to other areas of rapid innovation (eg, gene editing),46 scientific progress can quickly outpace philosophical deliberation, potentially leading to injustice and even outright harm to vulnerable groups such as older adults with cognitive impairments.25 In the field of healthcare robots, there are a number of potential dilemmas to consider, including deception, feelings of objectification, a loss of personal freedom, feelings of emotional attachment to a robot, and the substitution of contact with robots for contact with people.4,8,25,47 Additional ethical issues worthy of consideration include data privacy of the humans interacting with robots and liability from potential adverse events.48,49 Although a detailed discussion of these issues is beyond the scope of the current review, researchers have begun responding to a number of these concerns; for example, Bogue4 and Calo et al47 highlight the fact that effective social robots are designed to promote human-human engagement rather than replacing it with human-machine contact. Additionally, a code of ethics for human-robot interactions has been proposed,48 and a preliminary strategy to integrate ethics into robotics has been released.50 Consequently, scientists and engineers have begun contemplating important ethical issues in healthcare robotics, and early recommendations can be used to approach CAR interventions in a responsible manner that avoids undue harm to older adult users.
SAR as a Model for CAR
Robots that can sense and synthesize social behavior have existed since the mid-20th century, but early systems were low in complexity due to limited computing power.51 With advances in AI, current software can better model and respond to human behavior, thereby broadening the potential therapeutic scope of SAR. In terms of robot platforms, the landscape of social robots available for healthcare purposes continues to widen, and appearances can range from zoomorphic to anthropomorphic to mechanoid.52 The current review will not detail available robot morphologies, as previous authors have addressed this issue extensively.8,12,28 Instead, given that the available robots designed to address cognitive outcomes are currently embedded in the SAR literature, we will briefly review the state of the evidence on the impact of SAR on relevant outcomes in older adults.
Two systematic reviews of SAR for older adults in 8622 and 1353 investigations reported small, positive effects on engagement, interaction, medication use, and well-being, as well as reduced stress and loneliness. Moreover, many researchers make a conceptual distinction between companion-type and service-type SAR, where the former provide emotional support and the latter provide functional assistance.31 Companion-type social robots are often described as similar to therapy animals, but without the need for food, water, or cleaning, and without the danger of allergic reactions or unpredictable behavior.6,54 In contrast, service-type robots typically offer more practical assistance, which can be programmed with a high degree of adaptability and flexibility, and these features are integral when working with human partners.38,51 One service-type robot that is particularly relevant to CAR is the behavior-change robot. This approach capitalizes on social influence to promote positive behavior change, as the robot can be viewed as a coach that helps to encourage and motivate users to work toward personal goals.55 For example, three studies reported positive outcomes with respect to a) participants’ preference for a robotic coach over alternative designs, b) enjoyment in interacting with the robotic coach, c) tracking of their own exercise behavior, and d) engagement in exercise.23,55,56 Importantly, the behavior change platform is relevant in the context of evidence-based interventions designed to encourage the adoption of compensatory cognitive strategies57,58 and other pro-cognitive behaviors such as aerobic exercise.59
CAR
Assistive robots are now recognized as a potential platform from which to launch cognitive assessments60,61 and cognitive interventions15 in older adults, with the latter ranging from prolonging functioning in people with dementia32 to protecting cognition in healthy older adults.12 Given the efficacy of cognitive training in older adults without dementia,11 in contrast to impaired learning and retention of new information in people with dementia,62 targeting independently-living, older adults without dementia may be a particularly efficient and effective approach. Specifically, we believe that CAR interventions will be capable of prolonging residence in the home and delaying the transition to an assisted living facility, without over-burdening caregivers. This emphasis is consistent with reports that older adults are interested in robotic assistance if it helps them maintain autonomy in home-based IADLs.28,63
Importantly, robots in particular, relative to virtual electronic devices, may be well positioned to provide cognitive assistance. An overt physical embodiment is integral to robots’ overall effectiveness, and physically embodied platforms are both a) more preferred and enjoyable64,65 and b) more effective in eliciting positive behavior change56 than are intangible systems with comparable software. Additionally, robots’ physical presence allows them to support many tasks that a virtual system cannot (eg, ambulation, reaching/grasping), which could be of use in the provision of assistance with IADLs.
Although there is currently no formal cognitive branch of healthcare robotics, insight may be gleaned from the limited CAR research embedded in the SAR literature. For example, Zafrani and Nimrod5 argued that the SAR model can be utilized in assistive robots that are designed to affect outcomes other than interpersonal functioning. In this vein, while SAR is conceptualized as the integration of assistive robots and socially intelligent robots, we propose CAR as the synthesis of a) assistive robots, b) socially intelligent robots, and c) cognitive interventions.66,67 CAR platforms could be designed to provide both compensatory cognitive training interventions57,58,68,69 and restorative drill-and-practice interventions,70,71 with the ultimate goal of maintaining independence in IADLs. Cognitive “prosthetics” (eg, a robot-delivered reminding system) could also be used to scaffold cognitive and instrumental tasks that would otherwise require assistance from a caregiver.66 Moreover, although we are not aware of current research on the topic, CAR are theoretically well equipped to attenuate cognitive load, which can interfere with both intellectual and motor tasks. In this way, CAR is built upon and closely related to SAR, but with a distinct end goal (ie, improving cognition rather than increasing/enhancing social interaction).
CAR Interventions
Although formal cognitive training is uncommon in the robotics literature (but see Tsiakas et al72), there is broad interest in providing direct IADL assistance, often in the form of reminders to complete daily living tasks. For example, medication reminding systems have been used to address older adults’ reported desire to receive robotic assistance with medication management.29,33 One such system is Pearl, a home-based healthcare robot with software capable of storing a person’s schedule and assisting with medication management.67 Additionally, the robots Cafero and iRobiQ were specifically designed to target quality of life in older adults and include appointment and medication reminders.34 At present, these robots are not commercially available, but they represent potential prototypes to inform future engineering projects. Finally, the European Union’s ENabling Robot and assisted living environment for Independent Care and Health Monitoring of the Elderly (ENRICHME) project is designed to enhance autonomy in people with MCI by improving exercise, interpersonal engagement, and medication management.4 In terms of direct empirical support, Pu et al53 reported results from a conceptual review of the literature suggesting that robotic interventions can indeed improve medication adherence in older adults.
In addition to medication management, robots also have the potential to positively impact spatial navigation,73 calendar organization,12 and communication with friends and family.34,74 Researchers have even reported on “memory games,”20,30 often delivered via music.75 For example, Tapus et al64 described the task “Song Discovery” in a robotic test-bed platform. The game entails locating and pressing a button representing a song played over the speakers. In a subsequent paper, the authors presented the music game to ten people with dementia.76 No inferential statistics were reported, but, based on a visual examination of individual-level data, improvements occurred in reaction times and error rates as a result of extended practice.
CAR Systems
Central to the success of CAR is the delivery method. There are several examples of robot platforms through which cognitive interventions could be implemented. For example, a range of non-mobile, tabletop robots provide activities such as conversational support, cognitive games, and positive social affect (eg, Companionbot).32 Other platforms, such as the Scitos G3, are embedded within a smart home environment, and are designed for videoconferencing, schedule management, centralized control of smart appliances and utilities, and transmission of health data to appropriate professionals.77 Scitos G3 tracks users’ movements in the home and can approach them in order to initiate conversations; it also provides greetings and farewells when they enter or leave the home and suggests health behaviors (eg, exercising, nutritious snacks) when appropriate. Such technological advances provide the foundation from which cognitive interventions could be successfully delivered, but the current science is years behind the technology and the literature in robotic cognitive interventions is plagued by three major methodological limitations. First, the cognitive interventions that have been deployed are not evidence-based and, consequently, we cannot be confident that there will be positive therapeutic effects. Second, study designs are non-experimental with small sample sizes, thereby limiting causal inference. Third, most dependent variables are not standardized, psychometrically sound, or objective, thereby limiting interpretation of cognitive and functional improvements. Overall, similar to the Rabbitt et al8 conclusion about the SAR literature, the current evidence for CAR is nascent. Importantly, while it is possible to program a cognitive intervention into an interactive robot, we do not yet know if the intervention effects are actually reliable and valid.3 In Table 1, we highlight the six most promising CAR studies to date based on the quality of a) the robot hardware and software, b) the research methodology, and c) the cognitive intervention.74,78–82
 | 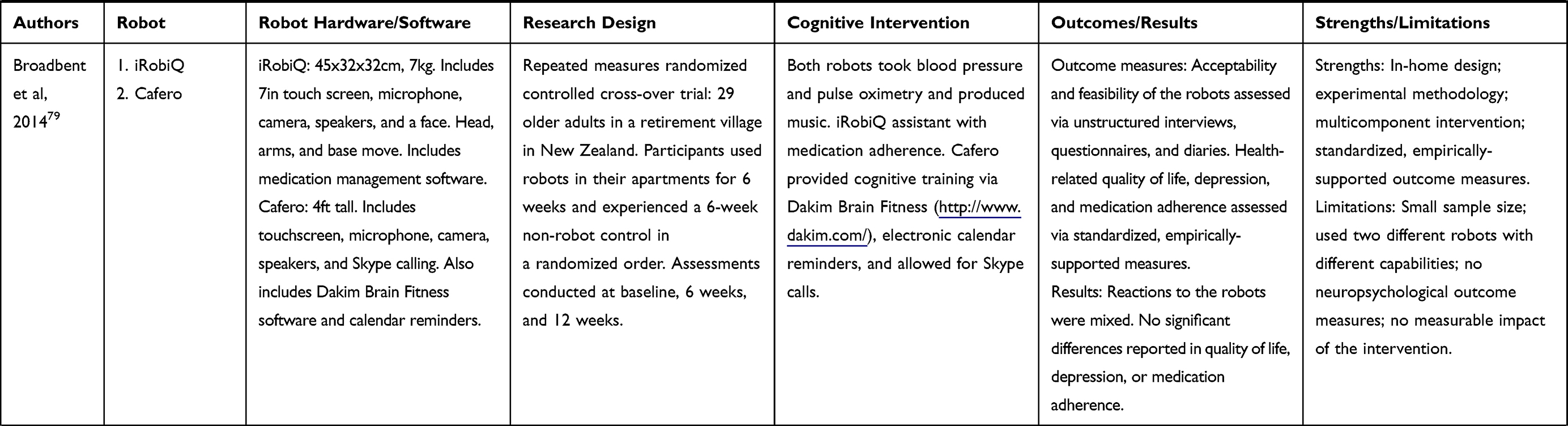 | 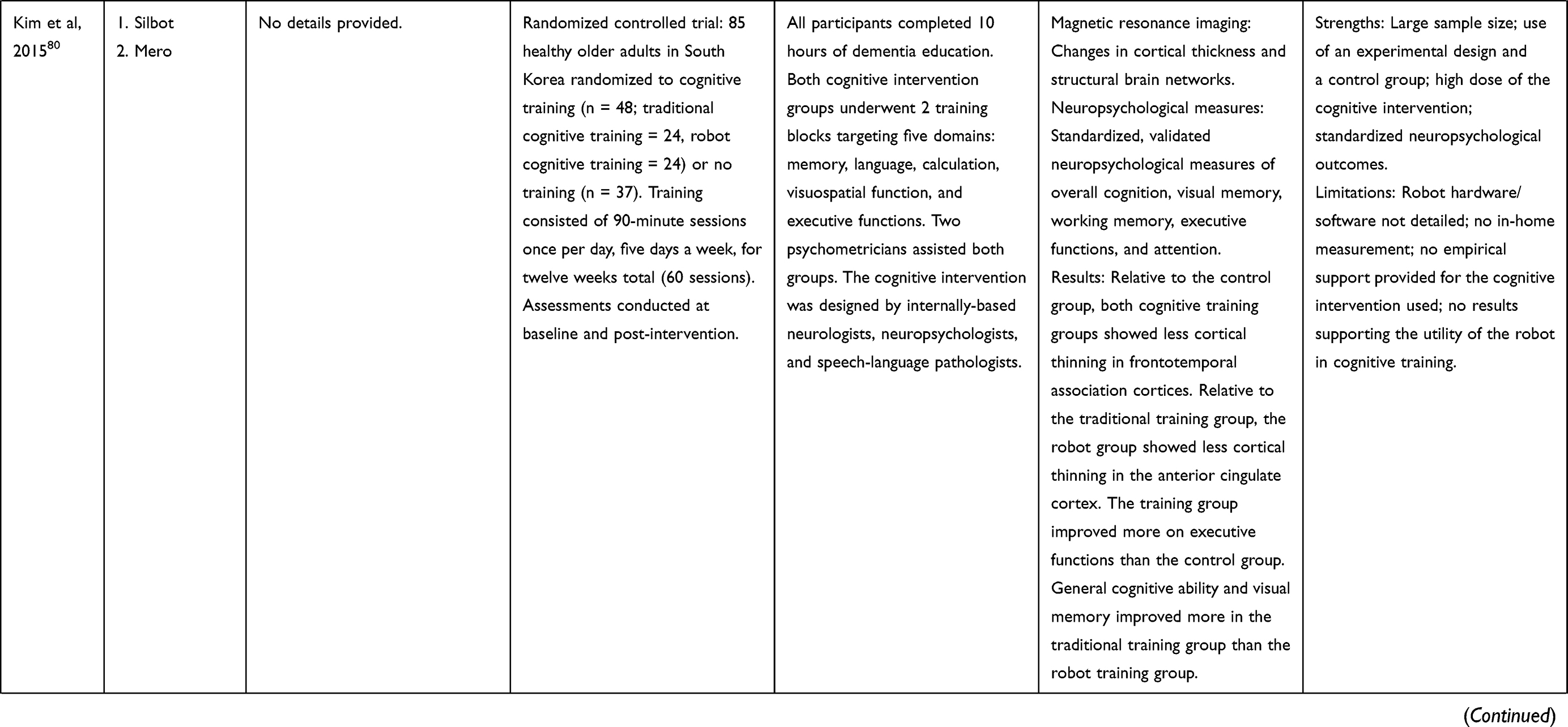 |
Table 1 Promising CAR Studies |
Future Directions
Although the healthcare robotics literature is exciting and promising, much work remains to be done. Based on the evidence reviewed above, we present seven recommendations for future CAR researchers in order to propel the field toward the ultimate goal of widespread, real-world implementation of robotic interventions to improve cognition. First, conduct investigations in the real-world environment of independently-living older adults – ie, their homes (see, e.g., Schroeter et al77). This may include simulated lab-based home environments initially, in order to enhance internal validity and reduce cost.83 Second, maintain and advance interdisciplinary research teams, including technical (engineering) and scientific (psychology, neuropsychology, geriatrics) collaborators. Third, closely adhere to ethical guidelines.48,50 Fourth, prioritize models of social aging over a deficit model of aging31 in design and implementation. Fifth, select a set of evidence-based robotic platforms and move forward with rigorous scientific investigation of each platform rather than introducing new robotic systems into the current market. Sixth, and relatedly, select a robot with the following evidence-based features for further investigation: a) ease of use, b) personalization and adaptability, c) small in size and moderately anthropomorphized features, and d) sociability and ability to be matched to users’ personalities. Seventh, address methodological limitations from the SAR/CAR literature; that is, studies would benefit from a) a theoretical basis, b) recruitment of large samples, c) inclusion of evidence-based cognitive interventions, d) experimental designs with appropriate control groups, and e) administration of standardized, psychometrically-sound, objective neuropsychological and functional tests as dependent variables.
Consequently, we provide a broad framework for future researchers to use in ongoing investigations into CAR. However, the current review is limited by a dearth of literature on the topic, and so our recommendations remain broad. As the field progresses, we encourage future researchers to turn their attention to important nuanced topics such as the ideal method for CAR delivery in the home, the degree of technical assistance required by older adults for a successful intervention, the extent to which home-based robots benefit from augmentation by human therapists, and the initial costs and later healthcare savings associated with these interventions.
Conclusion
Aging populations across the globe are in need of creative, innovative treatments in order to support health and wellness in the later stages of life. There is a small but growing literature focused on healthcare robots stationed in the homes of older adults to promote wellness and independence. We propose that more resources be allocated to robots to improve cognitive health, as this is an area where there is a) potential for great benefit to older adults and to society, and b) little methodologically rigorous research. Ultimately, by capitalizing on interdisciplinary knowledge and skill, we are confident that CAR researchers will be equipped to produce high-quality scientific evidence that will support and enhance the aging process, leading to happier, healthier, more autonomous older adults all over the world.
Disclosure
No conflicts of interest were declared. The authors disclosed receipt of the following financial support for the authorship and/or publication of this article: Funding for this study was provided, in part, by the National Institutes of Health (grant R01MH094151-01 to D.V.J. [PI]), by the National Institute of Mental Health T32 Geriatric Mental Health Program (grant MH019934 to D.V.J. and E.W.T. [PIs]), the Stein Institute for Research on Aging at the University of California, San Diego.
References
1. Beer JM, Smarr C-A, Chen TL, et al. The domesticated robot: design guidelines for assisting older adults to age in place.
2. Pruchno R. Technology and aging: an evolving partnership. Gerontologist. 2019;59(1):1–5. doi:10.1093/geront/gny153
3. Riek LD. Healthcare robotics. Commun ACM. 2017;60(11):68–78. doi:10.1145/3127874
4. Bogue R. Europe leads the way in assistive robots for the elderly. Ind Robot Int J. 2017;44(3):253–258. doi:10.1108/IR-02-2017-0041
5. Zafrani O, Nimrod G. Towards a holistic approach to studying human–robot interaction in later life. Gerontologist. 2019;59(1):e26–e36. doi:10.1093/geront/gny077
6. Kolling T, Haberstroh J, Kaspar R, Pantel J, Oswald F, Knopf M. Evidence and deployment-based research into care for the elderly using emotional robots: psychological, methodological and cross-cultural facets. GeroPsych. 2013;26(2):83–88. doi:10.1024/1662-9647/a000084
7. Feil-Seifer D, Mataric MJ. Defining socially assistive robotics.
8. Rabbitt SM, Kazdin AE, Scassellati B. Integrating socially assistive robotics into mental healthcare interventions: applications and recommendations for expanded use. Clin Psychol Rev. 2015;35:35–46. doi:10.1016/j.cpr.2014.07.001
9. Pan C-W, Wang X, Ma Q, Sun H-P, Xu Y, Wang P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci Rep. 2015;5(1):17301. doi:10.1038/srep17301
10. Pereira RR, Pontes MD, Silva AO, et al. Quality of life and the cognitive condition of elderly served in family health unit. Int Arch Med. 2015. doi:10.3823/1854
11. Rebok GW, Ball K, Guey LT, et al. Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J Am Geriatr Soc. 2014;62(1):16–24. doi:10.1111/jgs.12607
12. Robinson H, MacDonald B, Broadbent E. The role of healthcare robots for older people at home: a review. Int J Soc Robot. 2014;6(4):575–591. doi:10.1007/s12369-014-0242-2
13. Alnajjar F, Khalid S, Vogan AA, Shimoda S, Nouchi R, Kawashima R. Emerging cognitive intervention technologies to meet the needs of an aging population: a systematic review. Front Aging Neurosci. 2019;11:291. doi:10.3389/fnagi.2019.00291
14. Moosaei M, Das SK, Popa DO, Riek LD. Using facially expressive robots to calibrate clinical pain perception.
15. Mitzner TL, Chen TL, Kemp CC, Rogers WA. Identifying the potential for robotics to assist older adults in different living environments. Int J Soc Robot. 2014;6(2):213–227. doi:10.1007/s12369-013-0218-7
16. Wick JY. Aging in place: our house is a very, very, very fine house. Consult Pharm. 2017;32(10):566–574. doi:10.4140/TCP.n.2017.566
17. Smith GE, Bondi MW. Mild Cognitive Impairment and Dementia: Definitions, Diagnosis, and Treatment. Oxford University Press; 2013.
18. Wiles JL, Leibing A, Guberman N, Reeve J, Allen RES. The meaning of “aging in place” to older people. Gerontologist. 2012;52(3):357–366. doi:10.1093/geront/gnr098
19. Szanton SL, Thorpe RJ, Boyd C, et al. Community aging in place, advancing better living for elders: a bio-behavioral-environmental intervention to improve function and health-related quality of life in disabled older adults. J Am Geriatr Soc. 2011;59(12):2314–2320. doi:10.1111/j.1532-5415.2011.03698.x
20. Orejana JR, MacDonald BA, Ahn HS, Peri K, Broadbent E. Healthcare robots in homes of rural older adults. In: Tapus A, André E, Martin J-C, Ferland F, Ammi M, editors. Social Robotics. Vol. 9388. Springer International Publishing; 2015:512–521. doi:10.1007/978-3-319-25554-5_51
21. Broekens J, Heerink M, Rosendal H. Assistive social robots in elderly care: a review. Gerontechnology. 2009;8(2):94–103. doi:10.4017/gt.2009.08.02.002.00
22. Kachouie R, Sedighadeli S, Khosla R, Chu M-T. Socially assistive robots in elderly care: a mixed-method systematic literature review. Int J Hum Comput Int. 2014;30(5):369–393. doi:10.1080/10447318.2013.873278
23. Kidd CD, Breazeal C. Robots at home: understanding long-term human-robot interaction.
24. Tsai TC, Hsu Y-L, Ma A-I, King T, Wu C-H. Developing a telepresence robot for interpersonal communication with the elderly in a home environment. Telemed J E Health. 2007;13(4):407–424. doi:10.1089/tmj.2006.0068
25. Riek LD. Robotics technology in mental health care. In: Luxton D, editor. Artificial Intelligence in Behavioral and Mental Health Care. Elsevier; 2015:185–203. doi:10.1016/B978-0-12-420248-1.00008-8.
26. Riek LD, Adams A, Robinson P. Exposure to cinematic depictions of robots and attitudes towards them.
27. Lee CC, Czaja SJ, Moxley JH, et al. Attitudes toward computers across adulthood from 1994 to 2013. Gerontologist. 2018;59(1):22–33. doi:10.1093/geront/gny081
28. Hutson S, Lim SL, Bentley PJ, Bianchi-Berthouze N, Bowling A. Investigating the suitability of social robots for the wellbeing of the elderly. In: D’Mello S, Graesser A, Schuller B, Martin J-C, editors. Affective Computing and Intelligent Interaction. Vol. 6974. Springer Berlin Heidelberg; 2011:578–587. doi:10.1007/978-3-642-24600-5_61
29. Broadbent E, Stafford R, MacDonald B. Acceptance of healthcare robots for the older population: review and future directions. Int J Soc Robot. 2009;1(4):319–330. doi:10.1007/s12369-009-0030-6
30. Neven L. ‘But obviously not for me’: robots, laboratories and the defiant identity of elder test users. Sociol Health Illn. 2010;32(2):335–347. doi:10.1111/j.1467-9566.2009.01218.x
31. Lee HR, Riek LD. Reframing assistive robots to promote successful aging. ACM Trans Hum Robot Interact. 2018;7(1):1–23. doi:10.1145/3203303
32. Abdollahi H, Mollahosseini A, Lane JT, Mahoor MH. A pilot study on using an intelligent life-like robot as a companion for elderly individuals with dementia and depression.
33. Šabanović S, Chang W-L, Bennett CC, Piatt JA, Hakken D. A robot of my own: participatory design of socially assistive robots for independently living older adults diagnosed with depression. In: Zhou J, Salvendy G, editors. Human Aspects of IT for the Aged Population. Design for Aging. Vol. 9193. Springer International Publishing; 2015:104–114. doi:10.1007/978-3-319-20892-3_11
34. Broadbent E, Jayawardena C, Kerse N, Stafford RQ, MacDonald BA. Human-robot interaction research to improve quality of life in elder care—an approach and issues.
35. Stafford RQ, Broadbent E, Jayawardena C, et al. Improved robot attitudes and emotions at a retirement home after meeting a robot.
36. Zhou L, Li Y, Bai S. A human-centered design optimization approach for robotic exoskeletons through biomechanical simulation. Robot Auton Syst. 2017;91:337–347. doi:10.1016/j.robot.2016.12.012
37. Mitzner TL, Boron JB, Fausset CB, et al. Older adults talk technology: technology usage and attitudes. Comput Hum Behav. 2010;26(6):1710–1721. doi:10.1016/j.chb.2010.06.020
38. Meng Q, Lee MH. Design issues for assistive robotics for the elderly. Adv Eng Inform. 2006;20(2):171–186. doi:10.1016/j.aei.2005.10.003
39. Woodworth B, Ferrari F, Zosa TE, Riek LD. Preference learning in assistive robotics: observational repeated inverse reinforcement learning.
40. Sung J, Grinter RE, Christensen HI. Pimp my roomba: designing for personalization.
41. Wu Y-H, Fassert C, Rigaud A-S. Designing robots for the elderly: appearance issue and beyond. Arch Gerontol Geriatr. 2012;54(1):121–126. doi:10.1016/j.archger.2011.02.003
42. Mori M. Bukimi no tani [the uncanny valley]. Energy. 1970;7:33–35.
43. Kim Y, Kwak SS, Kim M-S. Am I acceptable to you? Effect of a robot’s verbal language forms on people’s social distance from robots. Comput Hum Behav. 2013;29(3):1091–1101. doi:10.1016/j.chb.2012.10.001
44. Tapus A, Matarić MJ. User personality matching with a hands-off robot for post-stroke rehabilitation therapy. In: Proc Int Symp Exper Robot (ISER), 2006, Rio de Janeiro, Brazil.165–175.
45. Tapus A, Mataric MJ, Scassellati B. The grand challenges in socially assistive robotics. Robot Autom Mag. 2007;14(1):1–7. doi:10.1109/MRA.2007.339605
46. Gyngell C, Douglas T, Savulescu J. The ethics of germline gene editing. J Appl Philos. 2017;34(4):498–513. doi:10.1111/japp.12249
47. Calo CJ, Hunt-Bull N, Lewis L, Metzler T. Ethical implications of using the paro robot, with a focus on dementia patient care.
48. Riek L, Howard D. A code of ethics for the human-robot interaction profession. Proc We Robot. 2014.
49. Schaerer E, Kelley R, Nicolescu M.
50. van Wynsberghe A. A method for integrating ethics into the design of robots. Ind Robot Int J. 2013;40(5):433–440. doi:10.1108/IR-12-2012-451
51. Fong T, Nourbakhsh I, Dautenhahn K. A survey of socially interactive robots. Robot Auton Syst. 2003;42(3–4):143–166. doi:10.1016/S0921-8890(02)00372-X
52. Klamer T, Allouch SB. Acceptance and use of a social robot by elderly users in a domestic environment.
53. Pu L, Moyle W, Jones C, Todorovic M. The effectiveness of social robots for older adults: a systematic review and meta-analysis of randomized controlled studies. Gerontologist. 2018;59(1):e37–e51. doi:10.1093/geront/gny046
54. Robinson H, MacDonald B, Kerse N, Broadbent E. The psychosocial effects of a companion robot: a randomized controlled trial. J Am Med Dir Assoc. 2013;14(9):661–667. doi:10.1016/j.jamda.2013.02.007
55. Fasola J, Mataric MJ. Using socially assistive human–robot interaction to motivate physical exercise for older adults. Proc IEEE. 2012;100(8):2512–2526. doi:10.1109/JPROC.2012.2200539
56. Fasola J, Mataric M. A socially assistive robot exercise coach for the elderly. J Hum Robot Interact. 2013;2(2):3–32. doi:10.5898/JHRI.2.2.Fasola
57. Twamley EW, Vella L, Burton CZ, Heaton RK, Jeste DV. Compensatory cognitive training for psychosis: effects in a randomized controlled trial. J Clin Psychiatry. 2012;73(09):1212–1219. doi:10.4088/JCP.12m07686
58. Twamley EW, Jak AJ, Delis DC, Bondi MW, Lohr JB. Cognitive symptom management and rehabilitation therapy (CogSMART) for veterans with traumatic brain injury: pilot randomized controlled trial. J Rehabil Res Dev. 2014;51(1):59–70. doi:10.1682/JRRD.2013.01.0020
59. Wang C, Redgrave J, Shafizadeh M, Majid A, Kilner K, Ali AN. Aerobic exercise interventions reduce blood pressure in patients after stroke or transient ischaemic attack: a systematic review and meta-analysis. Br J Sports Med. 2018;
60. Varrasi S, Di Nuovo S, Conti D, Di Nuovo A. A social robot for cognitive assessment.
61. Logan LM, Semrau JA, Debert CT, Kenzie JM, Scott SH, Dukelow SP. Using robotics to quantify impairments in sensorimotor ability, visuospatial attention, working memory, and executive function after traumatic brain injury. J Head Trauma Rehabil. 2018;33(4):E61–E73. doi:10.1097/HTR.0000000000000349
62. Butters N, Granholm E, Salmon DP, Grant I, Wolfe J. Episodic and semantic memory: a comparison of amnesic and demented patients. J Clin Exp Neuropsychol. 1987;9(5):479–497. doi:10.1080/01688638708410764
63. Johnson MJ, Johnson MA, Sefcik JS, et al. Task and design requirements for an affordable mobile service robot for elder care in an all-inclusive care for elders assisted-living setting. Int J Soc Robot. 2017;1–20.
64. Tapus A, Tapus C, Mataric M. The role of physical embodiment of a therapist robot for individuals with cognitive impairments.
65. Forlizzi J. How robotic products become social products: an ethnographic study of cleaning in the home.
66. Alm N, Astell A, Ellis M, Dye R, Gowans G, Campbell J. A cognitive prosthesis and communication support for people with dementia. Neuropsychol Rehabil. 2004;14(1–2):117–134. doi:10.1080/09602010343000147
67. Pollack M. Autominder: a case study of assistive technology for elders with cognitive impairment. Generations. 2006;30(2):67–69.
68. Greenaway MC, Hanna SM, Lepore SW, Smith GE. A behavioral rehabilitation intervention for amnestic mild cognitive impairment. Am J Alzheimers Dis Demen. 2008;23(5):451–461. doi:10.1177/1533317508320352
69. Stringer AY. Ecologically-oriented neurorehabilitation of memory: robustness of outcome across diagnosis and severity. Brain Inj. 2011;25(2):169–178. doi:10.3109/02699052.2010.541894
70. Lustig C, Shah P, Seidler R, Reuter-Lorenz PA. Aging, training, and the brain: a review and future directions. Neuropsychol Rev. 2009;19(4):504–522. doi:10.1007/s11065-009-9119-9
71. Mahncke HW, Connor BB, Appelman J, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci. 2006;103(33):12523–12528. doi:10.1073/pnas.0605194103
72. Tsiakas K, Kyrarini M, Karkaletsis V, Makedon F, Korn O. A taxonomy in robot-assisted training: current trends, needs and challenges. Technologies. 2018;6(4):119. doi:10.3390/technologies6040119
73. Montemerlo M, Pineau J, Roy N, Thrun S, Verma V. Experiences with a mobile robotic guide for the elderly.
74. Tanaka M, Ishii A, Yamano E, et al. Effect of a human-type communication robot on cognitive function in elderly women living alone. Med Sci Monit Int Med J Exp Clin Res. 2012;18(9):CR550.
75. Martın F, Aguero C, Canas JM, et al. Robots in therapy for dementia patients. J Phy Agents. 2013;7(1):8.
76. Tapus A, Tapus C, Mataric MJ. The use of socially assistive robots in the design of intelligent cognitive therapies for people with dementia.
77. Schroeter C, Mueller S, Volkhardt M, et al. Realization and user evaluation of a companion robot for people with mild cognitive impairments.
78. Ahn HS, Santos MPG, Wadhwa C, MacDonald B. Development of brain training games for a healthcare service robot for older people. In: Beetz M, Johnston, Williams M-A, editors. Social Robotics. Vol. 8755. Springer International Publishing; 2014:1–10. doi:10.1007/978-3-319-11973-1_1
79. Broadbent E, Peri K, Kerse N, et al. Robots in older people’s homes to improve medication adherence and quality of life: a randomised cross-over trial. In: Beetz M, Johnston B, Williams M-A, editors. Social Robotics. Vol. 8755. Springer International Publishing; 2014:64–73. doi:10.1007/978-3-319-11973-1_7
80. Kim GH, Jeon S, Im K, et al. Structural brain changes after traditional and robot-assisted multi-domain cognitive training in community-dwelling healthy elderly. Amitay S, ed. PLoS One. 2015;10(4):e0123251. doi:10.1371/journal.pone.0123251
81. Otake-Matsuura M, Tokunaga S, Watanabe K, et al. Photo-integrated conversation moderated by robots for cognitive health in older adults: a randomized controlled trial. Geriatr Med. 2019. doi:10.1101/19004796
82. Sawami K. Cognitive ability and psychological effectiveness of brain training dance robot therapy for elderly people. OA J Neuropsychiatry. 2019. doi:10.33118/oaj.neuro.2019.01.004
83. Richardson J, Law M, Wishart L, Guyatt G. The use of a simulated environment (Easy Street) to retrain independent living skills in elderly persons: a randomized controlled trial. J Gerontol a Biol Sci Med Sci. 2000;55(10):M578–M584. doi:10.1093/gerona/55.10.M578
84. Anh HS, Santos MPG, Wadhwa C, MacDonald B. Development of brain training games for a healthcare service robot for older people.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.