Back to Journals » Clinical Ophthalmology » Volume 19
Histopathological Changes After Standard and Novel Endoscopic Cyclophotocoagulation versus Transscleral Cyclophotocoagulation in Human Cadaveric Eyes
Authors Alryalat SA ![]() , Capitena Young CE, Pantcheva MB, Ender P, Seibold LK, Kahook MY
, Capitena Young CE, Pantcheva MB, Ender P, Seibold LK, Kahook MY
Received 25 April 2025
Accepted for publication 1 December 2025
Published 6 December 2025 Volume 2025:19 Pages 4463—4468
DOI https://doi.org/10.2147/OPTH.S536736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Saif Aldeen Alryalat,1 Cara E Capitena Young,2 Mina B Pantcheva,2 Paula Ender,3 Leonard K Seibold,2 Malik Y Kahook2
1Department of Ophthalmology and Visual Science, University of Illinois Chicago, Chicago, IL, USA; 2Department of Ophthalmology, University of Colorado School of Medicine, Sue Anschutz-Rodgers Eye Center, Aurora, CO, USA; 3BVI Medical, Waltham, MA, USA
Correspondence: Saif Aldeen Alryalat, Department of Ophthalmology and Visual Science, University of Illinois Chicago, Chicago, IL, USA, Email [email protected]
Purpose: To compare the histological effects of a novel endo-cyclophotocoagulation (ECP) device (Leos, BVI Medical, Waltham, MA), a standard ECP (BVI Medical, Waltham, MA), and transscleral cyclophotocoagulation (TCP) on the ciliary body and processes in human cadaveric eyes.
Patients and Methods: Cross-sectional histological analysis of three cadaveric human eyes, where each laser method was used to treat a segment of the ciliary body and ciliary processes of each eye. Each treated eye was then prepared for histologic assessment by dissecting the anterior segment away from the posterior segment to isolate the ciliary processes and adjacent tissues, followed by segmenting them according to the specific treatment protocol. After fixation in blocks, 8 μm sections were prepared, dewaxed in xylene, hydrated in decreasing concentrations of ethanol, stained with haematoxylin and eosin/phloxine, and examined histologically using standard light microscopy.
Results: Histologic examination revealed that both standard and novel ECP caused contraction of the ciliary processes and disruption of the pigmented epithelium with minimal effect on stromal architecture. TCP resulted in disruption of the ciliary body muscle, stroma, ciliary processes, and both pigmented and non-pigmented ciliary epithelium.
Conclusion: The novel ECP led to similar tissue changes to the standard ECP in human cadaveric eyes. TCP led to extensive tissue disruption that extended beyond the ciliary processes into the stroma and adjacent ciliary muscles, which is consistent with previous studies of TCP. Future prospective clinical studies would provide data on how the novel ECP device compares to both standard ECP and TCP in both safety and efficacy.
Keywords: aqueous humor, ciliary body, transscleral cyclophotocoagulation, endoscopic cyclophotocoagulation, intraocular pressure
Introduction
Glaucoma, a leading cause of irreversible blindness worldwide, is characterized by progressive optic nerve damage.1 Intraocular pressure (IOP), being the only modifiable risk factor for this disease, can be managed pharmacologically, with laser treatment, or through invasive surgical intervention.2 Transcleral Cyclophotocoagulation (TCP) was first employed in the early 1960s for pressure reduction via xenon arc photocoagulation.3 In subsequent years, Neodymium: Yttrium-Aluminum-Garnet (Nd:YAG) lasers were used as an alternative, followed by the introduction of the diode laser in the 1980s and 1990s. The introduction of the diode laser was a transformative change as it led to an improved safety profile compared to earlier modalities.4 Another alternative approach to cyclophotocoagulation utilizes an endoscopic approach, known as endoscopic cyclophotocoagulation (ECP). ECP was first introduced in the 1990s and provides a more targeted approach using direct visualization of the ciliary processes at the time of treatment.5
One of the limitations of TCP is the inability to specifically target the ciliary processes. This can lead to complications such as prolonged inflammation, severe pain, hyphema, and hypotony, that are believed to be related to deeper tissue disruption and associated inflammation.6 Recent innovation in TCP technology has been associated with more favorable safety and efficacy outcomes,7,8 specifically with the use of MicroPulse lasers but still lacks targeted treatment capabilities. In contrast, ECP has been associated with less extensive histological disruption of targeted tissues while remaining effective at lowering IOP.9 Since the initial ECP device in the 1990s, minimal change has been made to the instrumentation.
Recently, a novel ECP device (Leos BVI Medical Waltham, MA, USA), has been developed which utilizes a customized LED illumination and digital camera system with higher resolution of 40,000 pixels compared to 17,000 pixels of the standard commercialized system. The novel ECP system utilizes a single use, 19-gauge endoscope probe with integrated laser delivery. The endoscopic video image is displayed on a large “heads-up” display, providing a detailed and magnified view of the intraocular structures. When utilizing the laser, the red aiming beam is displayed on the target tissue and laser energy is delivered precisely to the intended area. The technical steps of using the laser is the same as the standard ECP, which also utilize 810 nm diode laser. Unlike the standard ECP system that relies on the user’s assistant to manually adjust parameters such as image focus, illumination and orientation, the automated features of the novel device eliminates some of the challenges that are currently associated with endoscopy. The advancements in the new technology may allow for enhanced precision and thorough treatment of the ciliary epithelium and potentially reducing under- or over-treatment, thereby improving patient outcomes. This study aims to compare the histological effects of standard ECP, the novel ECP device and TCP on the ciliary body and surrounding structures in human cadaveric eyes.
Materials and Methods
This experimental study was a comparative histologic analysis between standard ECP, the novel ECP laser and TCP on cadaveric human eyes. Eyes were obtained from the Lions World Vision Institute in Tampa Eye Bank (Tampa, Florida). Institutional review board waiver was obtained from The University of Colorado for this tissue-based laboratory analysis. The study was conducted in accordance with the latest declaration of Helsinki.
All three eyes were obtained within 24hrs of death and had brown irides with no history of glaucoma, intraocular laser or implanted devices other than intraocular lenses. The eyes were each inflated with balanced salt solution injected through the optic nerve with a 25‐gauge needle until physiologic IOP was achieved on digital palpation. This allowed for proper external application of cyclophotocoagulation using the TCP G-probe. The first and second eye were divided into thirds; a control third, a novel ECP third (0.25W), and either the standard ECP (0.25W) or transscleral cyclophotocoagulation (TCP, 2.5W 2–4 seconds). The third eye was divided in half with one-half treated with the novel ECP (0.25W) and the other half with TCP (2.5W 2–4 seconds). Permanent marker was used to mark the margins of the eyes and mark the laser treatment boundaries, with safety margins between treatment areas left. These marks were also used for future dissection.
Both standard ECP and novel ECP were conducted using either the commercially available EndoOptiks® System (BVI Medical Waltham, MA) with 19-gauge, reusable, laser microendoscope or the investigational novel ECP device (BVI Medical, Waltham, MA) with 19-gauge, single-use, laser microendoscope probe. Both devices utilize the same, continuous wave, 810nm diode laser, coupled with a 640nm red aiming beam diode laser. A 2.4 mm keratome was used to create a clear corneal incision, and the anterior chamber was reformed with viscoelastic (Healon, Advanced Medical Optics, Santa Ana, CA, USA). Viscoelastic was injected under the iris to expand the ciliary sulcus for better visualization of the ciliary processes. ECP was performed in the designated treatment area on continuous mode at 0.25 W, with ciliary process whitening and shrinkage marking the endpoint.
The TCP laser treatment was administered using an Iridex 810nm diode laser (Mountain View, CA SLx diode laser photocoagulation system) with a single use handheld G-probe. With light to moderate pressure, the handheld G-probe was applied to the conjunctival surface, positioned 1.2 mm from the limbus (a distance defined by the G-probe footplate). Based on clinical protocol, the probe was oriented perpendicular to the visual axis to deliver transscleral laser pulses of approximately 2.5 Watt for 2 to 4-second duration, targeting the pars plicata region. Treatments were conducted and titrated as needed with the goal of minimal popping of the ciliary processes.
After treatment application, each eye was dissected cross-sectionally at the level of pars plana. Each section was then divided into control and treatment segments as shown in Figure 1, which provides illustrative details of the methodology. Each section was placed in 10% Neutral buffered formalin (Sigma-Aldrich, St. Louis, MO, USA), sealed and labeled, and shipped to the tissue processing facility in insulating bag under wet ice.
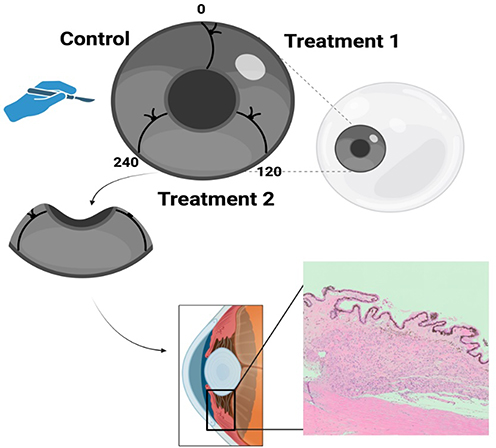 |
Figure 1 Illustration of the study protocol. Each cadaveric eye was divided into segments according to the treatment applied, dissected, processed and analyzed for histological assessment. |
Histological Analysis
The specimens from the tissue were washed with a 0.1 M phosphate‐buffered solution, dehydrated in increasing concentrations of propanol, cleared with xylene and placed in a paraffin tissue processor (Miles Tissue‐Tek VIP, model 2000, Spectron Corp, Burlington, WA, USA). After removing the cassettes from the processor, they were placed into the holding tank of the embedding center. Using heated forceps, each specimen was transferred to an embedding mold partially filled with paraffin wax and oriented appropriately. The molds were then filled completely with the wax and placed on a cooling plate overnight. The paraffin wax blocks were removed gently from the molds, 8 μm sections were prepared, dewaxed in xylene, hydrated in decreasing concentrations of ethanol, stained with haematoxylin and eosin/phloxine, and examined histologically using standard light microscopy.
Image Analysis
Light microscopy (LM) images were analyzed and compared qualitatively to assess for the presence and amount of ciliary tissue disruption and/or damage with a focus on the following parameters:
- Separation of the ciliary epithelium from the stroma
- Coagulation of collagen and destruction of ciliary body stroma
- Tissue disorganization and destruction
- Damage to adjacent sclera and iris tissue.
Results
Tissue analysis revealed histological changes in all treated sections regardless of method used compared to normal architecture in the control sections (Figure 2A–D). The ECP treated tissues (both standard and the novel) showed blunting of the ciliary processes without separation of epithelium from the stroma, coagulation of collagen, or injury to the ciliary muscle or surrounding tissues. In contrast, TCP showed wide destruction and disorganization of tissue architecture with coagulative damage to the ciliary body stroma and muscle and loss of epithelial lining of the ciliary processes. These findings were consistent for all treated tissue samples across all treated eyes. There was no evidence of damage to surrounding scleral or iris tissue in any of the treated samples across all laser modalities.
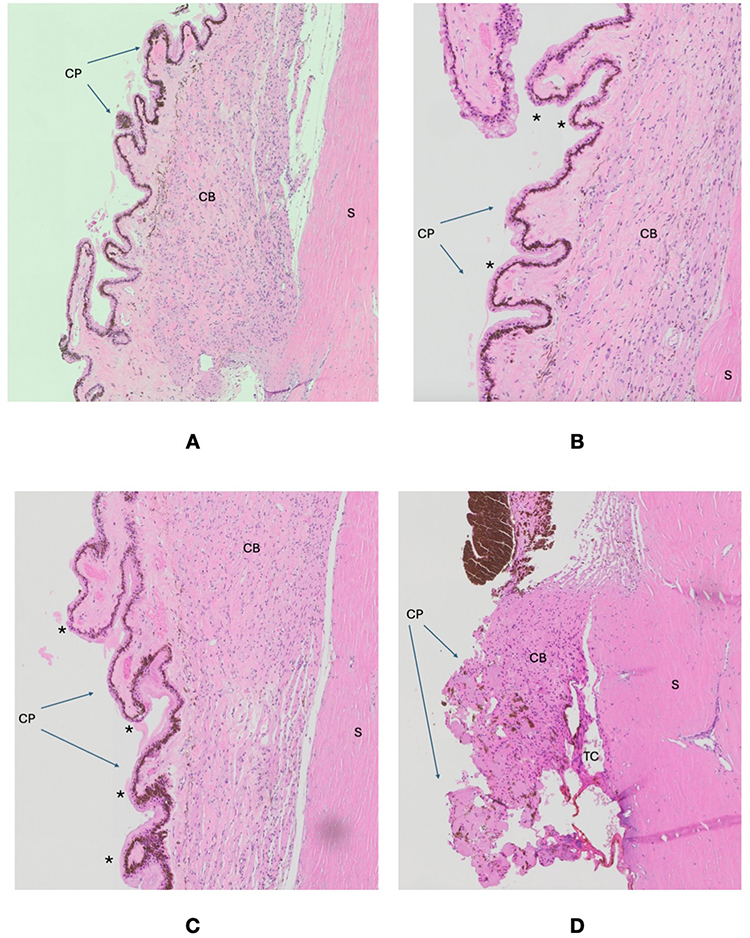 |
Figure 2 (A) Untreated control tissue: Light microscopy images for the ciliary body stroma (CB), ciliary processes (CP) and adjacent sclera (S) showing normal architecture. (B) Light microscopy images for the ciliary body stroma (CB), ciliary processes (CP) and adjacent sclera (S) treated with standard endoscopic cyclophotocoagulation (ECP) showing blunting of the ciliary processes (*) without separation of epithelium from the stroma, coagulation of collagen, or injury to the ciliary muscle or surrounding tissues. (C) Light microscopy images for the ciliary body stroma (CB), ciliary processes (CP) and adjacent sclera (S) treated with novel endoscopic cyclophotocoagulation (novel ECP) showing blunting of the ciliary processes (*) without separation of epithelium from the stroma, coagulation of collagen, or injury to the ciliary muscle or surrounding tissues. (D) Light microscopy images for the ciliary body stroma (CB), ciliary processes (CP) and adjacent sclera (S) treated with transscleral cyclophotocoagulation (TCP) showing wide destruction and disorganization of CB tissue architecture with tissue cleavage (TC) and coagulative damage to the ciliary body stroma and muscle and loss of epithelial lining of the ciliary processes. |
Discussion
In this study, we describe the ocular histologic effects after cyclophotocoagulation using a novel ECP device. Treatment with this novel technology resulted in similar histological findings as standard ECP with both ECP modalities resulting in less tissue disruption compared to TCP, as evaluated by LM. These findings support the assertion that the endoscopic approach to cyclophotocoagulation, regardless of instrumentation version, offers a more targeted approach, achieving effective ablation of ciliary epithelium while minimizing collateral tissue disruption.
Clinically, ECP represents the only micro-invasive glaucoma surgery (MIGS) that targets aqueous production rather than drainage, a mechanism that might have an additive effect when combined with other procedures targeting aqueous outflow.10–12 Since its release, ECP has been utilized both as a standalone procedure and in combination with cataract surgery as a means of safely yet effectively lowering IOP in glaucoma patients. Comparative studies between TCP and ECP have shown significant IOP reduction with both treatments, but with a consistently better safety profile for ECP.13 Traditional TCP has been plagued by complications such as phthisis, hypotony, and prolonged inflammation. MicroPulse transscleral laser therapy specifically was developed to mitigate these risks through a shortened duty cycle with cycling periods of the laser on and off to allow ocular tissues to cool and better dissipate laser energy during treatment. However, both transscleral techniques still have a relatively high percentage of complications and extensive histological destruction is not uncommon due to the lack of direct tissue visualization with the transscleral approach.14,15 In contrast, prospective and retrospective studies to date have shown excellent efficacy and safety of ECP in the reduction of IOP and medication burden in glaucoma.16 Two recent systematic reviews with meta-analysis further support the efficacy and safety of ECP as an IOP-lowering modality in both adults,17 and children with glaucoma.18 In comparison to the existing standard ECP and TCP, the novel ECP provide the safety of the standard TCP along with more advanced technology and targeting advantage that would provide better feedback to physician.
Histologically, one study comparing the effects of MicroPulse TCP and traditional TCP, which utilizes a continuous wave approach, on the ciliary body showed extensive thermally induced changes that involved the ciliary stroma, capillary vascular network, smooth muscle, and basement membrane of the pigmented ciliary epithelium for both modalities.19 Such extensive tissue involvement beyond the ciliary processes is not observed in histologic evaluation of eyes treated with ECP.9,20
While the present study is the first to assess treatment effects of the novel ECP treatment histologically, there are a few limitations of note. As with most cadaveric histological studies, the number of eyes tested is relatively small with three eyes included with qualitative analysis of tissue. Additionally, while such studies are important in showing tissue effect, it is unclear how this will translate to clinical outcomes. Clinical studies assessing both efficacy and safety are necessary to further validate any novel laser or surgical techniques.
Conclusions
The novel ECP device effectively coagulates the ciliary epithelium with histologic findings similar to that of traditional commercialized ECP. Furthermore, we found greater collateral tissue damage with TCP as compared to both the novel and traditional ECP, which is consistent with prior work leveraging the endoscopic approach. These findings support the continued investigation of the novel ECP for future clinical use.
Acknowledgment
BVI sponsored the study through an unrestricted research grant.
Disclosure
Malik Y. Kahook: Consultant to FCI, New World Medical, and SpyGlass Pharma, Ownership of SpyGlass Pharma, Patent Royalties from Alcon, New World Medical, FCI, and SpyGlass Pharma
Cara E. Capitena Young: No relevant disclosures
Mina B. Pantcheva: No relevant disclosures
Paula Ender: Employed by BVI Medical
Leonard K. Seibold: Consultant to New World Medical, Abbvie, and Thea
Saif Aldeen Alryalat: No relevant disclosures
References
1. Zhang N, Wang J, Li Y, Jiang B. Prevalence of primary open angle glaucoma in the last 20 years: a meta-analysis and systematic review. Sci Rep. 2021;11(1):13762. doi:10.1038/s41598-021-92971-w
2. Schwartz K, Budenz D. Current management of glaucoma. Curr Opin Ophthalmol. 2004;15(2):119. doi:10.1097/00055735-200404000-00011
3. Weekers R, Lavergne G, Watillon M, et al. Effects of photocoagulation of ciliary body upon ocular tension. Am J Ophthalmol. 1961;52(2):156–163. doi:10.1016/0002-9394(61)91110-2
4. Hennis HL, Stewart WC. Semiconductor diode laser transscleral cyclophotocoagulation in patients with glaucoma. Am J Ophthalmol. 1992;113(1):81–85. doi:10.1016/S0002-9394(14)75758-7
5. Ishida K. Update on results and complications of cyclophotocoagulation. Curr Opin Ophthalmol. 2013;24(2):102–110. doi:10.1097/ICU.0b013e32835d9335
6. Sheheitli H, Persad PJ, Feuer WJ, et al. Treatment outcomes of primary transscleral cyclophotocoagulation. Ophthalmol Glaucoma. 2021;4(5):472–481. doi:10.1016/j.ogla.2020.12.014
7. Johansyah CAP, Bambang L. A systematic review of cyclophotocoagulation techniques: continuous wave versus micropulse for glaucoma treatment. Beyoglu Eye J. 2024;9:1–7. doi:10.14744/bej.2024.47123
8. Almeida INF, Resende ICTP, Magalhães LM, et al. Double-arc slow-coagulation transscleral cyclophotocoagulation laser protocol: one-year effectiveness and safety outcomes. Ophthalmol Glaucoma. 2024;7(6):580–586. doi:10.1016/j.ogla.2024.06.008
9. Pantcheva MB, Kahook MY, Schuman JS, Noecker RJ. Comparison of acute structural and histopathological changes in human autopsy eyes after endoscopic cyclophotocoagulation and trans-scleral cyclophotocoagulation. Br J Ophthalmol. 2007;91(2):248–252. doi:10.1136/bjo.2006.103580
10. Kirk S, Kirk C, Barnes R, Kirk T. Minimally invasive glaucoma surgeries, is two better than one? Invest Ophthalmol Visual Sci. 2020;61:976.
11. Klug E, Chachanidze M, Nirappel A, et al. Outcomes of phacoemulsification and endoscopic cyclophotocoagulation performed with dual blade ab interno trabeculectomy or trabecular micro-bypass stent insertion. Eye. 2022;36(2):424–432. doi:10.1038/s41433-021-01475-4
12. Francis BA, Flowers B, Dastiridou A, et al. Endoscopic cyclophotocoagulation and other cyclodestructive methods: histopathologic comparison of in vivo treatment in humans and monkeys. Ophthalmol Glaucoma. 2019;2(6):413–421. doi:10.1016/j.ogla.2019.08.008
13. Lanzagorta-Aresti A, Montolío-Marzo S, Davó-Cabrera JM, Piá-Ludeña JV. Transscleral versus endoscopic cyclophotocoagulation outcomes for refractory glaucoma. European J Ophthalmol. 2021;31(3):1107–1112. doi:10.1177/1120672120914230
14. Hwang YH, Lee S, Kim M, Choi J. Comparison of treatment outcomes between slow coagulation transscleral cyclophotocoagulation and micropulse transscleral laser treatment. Sci Rep. 2024;14(1):23944. doi:10.1038/s41598-024-75246-y
15. Moussa K, Feinstein M, Pekmezci M, et al. Histologic changes following continuous wave and micropulse transscleral cyclophotocoagulation: a randomized comparative study. Trans Vision Sci Technol. 2020;9(5):22. doi:10.1167/tvst.9.5.22
16. Francis BA, Berke SJ, Dustin L, Noecker R. Endoscopic cyclophotocoagulation combined with phacoemulsification versus phacoemulsification alone in medically controlled glaucoma. J Cataract Refract Surg. 2014;40(8):1313–1321. doi:10.1016/j.jcrs.2014.06.021
17. Amaral DC, Louzada RN, Moreira PHS, et al. Combined endoscopic cyclophotocoagulation and phacoemulsification versus phacoemulsification alone in the glaucoma treatment: a systematic review and meta-analysis. Cureus. 2024;16(3):e55853. doi:10.7759/cureus.55853
18. Elhusseiny AM, Hassan AK, Elsaman AS, et al. Continuous wave transscleral cyclophotocoagulation and endoscopic cyclophotocoagulation in childhood glaucoma: a meta-analysis. J Glaucoma. 2024;33(6):456. doi:10.1097/IJG.0000000000002365
19. Maslin JS, Chen PP, Sinard J, et al. Histopathologic changes in cadaver eyes after MicroPulse and continuous wave transscleral cyclophotocoagulation. Can J Ophthalmol. 2020;55(4):330–335. doi:10.1016/j.jcjo.2020.03.010
20. Pantcheva MB, Kahook MY, Schuman JS, et al. Comparison of acute structural and histopathological changes of the porcine ciliary processes after endoscopic cyclophotocoagulation and transscleral cyclophotocoagulation. Clin Exp Ophthalmol. 2007;35(3):270–274. doi:10.1111/j.1442-9071.2006.01415.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.