Back to Journals » Psychology Research and Behavior Management » Volume 15
High Social Capital is Associated with Decreased Mental Health Problem Among In-School Adolescents in Eastern Ethiopia: A Cross-Sectional Study
Authors Hunduma G ![]() , Deyessa N
, Deyessa N ![]() , Dessie Y, Geda B
, Dessie Y, Geda B ![]() , Yadeta TA
, Yadeta TA
Received 1 November 2021
Accepted for publication 24 February 2022
Published 4 March 2022 Volume 2022:15 Pages 503—516
DOI https://doi.org/10.2147/PRBM.S347261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Gari Hunduma,1 Negussie Deyessa,2 Yadeta Dessie,3 Biftu Geda,4 Tesfaye Assebe Yadeta1
1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Preventive Medicine, School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 4School of Nursing and Midwifery, College of Health and Medical Sciences, Meda Welabu University, Shashamene, Ethiopia
Correspondence: Gari Hunduma, Tel +251911347558, Email [email protected]
Purpose: The importance of social capital for adolescent mental health has not been explored in low resource settings like Ethiopia. In this study, we examined the association between social capital and mental health problems among in-school adolescents in Harari Regional State, eastern Ethiopia.
Methods: A cross-sectional study was conducted among 3227 in-school adolescents of 13– 19 years. A multistage sampling was used to select participants. Guided self-administered questionnaire was used to collect data. Mental health problem was measured using a self-administered version of the strength and difficulty questionnaire (SDQ), while social capital questionnaire for adolescent students (SCQ-AS) was used to collect data about the condition of social capital. The data were double entered, validated, and cleaned using EpiData 3.1 and analyzed using STATA 14.1. The association between the outcome variable and predictors was analyzed using an ordinal logistic regression model. The result was reported using an odds ratio along with 95% confidence interval (CI) and a p-value < 0.05 was considered statistically significant association.
Results: A total of 740 (22.93%) students had mental health problem, of which 9.7% (95% CI, 8.7– 10.8) and 13.20% (95% CI, 12– 14) were classified as “abnormal” and “borderline”, respectively. Factors associated with decreased mental health problem were increased network of friends at school (AOR = 0.75, 95% CI: 0.58– 0.99), increased trust in school or neighborhood (AOR = 0.52, 95% CI: 0.44– 0.63), and high social cohesion in the community (AOR = 0.75, 95% CI: 0.62– 0.89).
Conclusion: Higher social capital is associated with a decreased mental health problem among in-school adolescents. Prevention and treatment of mental health problems require strengthening social capital at school, household, and in the neighborhood.
Keywords: adolescents, social capital, mental health problems, eastern Ethiopia, in-school
Introduction
Adolescence is a period of quick physical, social, and psychological development, and, for this reason, adolescents are extremely vulnerable to mental problems since it is the age of beginning of hazardous behavior.1,2 Mental and behavioral disorders are a significant contributor to the global burden of disease and disability among adolescents3,4 which accounts 16%.5 Suicide is the third leading cause of death among adolescents aged 15–19 years.6 Half of adult mental health problems begin at age 14 and three-quarters begin in their mid-twenties.7 Moreover, 10% to 20% of adolescents live with mental health problems at a certain stage in their lives, though majority of them are not diagnosed.8,9 In sub-Saharan Africa, about 14.3% of adolescents have significant levels of mental concerns, of which 10% have specific psychiatric conditions.10 Similarly, mental disorder is the leading cause of the burden of non-infectious morbidity, which accounts for 11% of the overall burden of disease in Ethiopia. Furthermore, an estimated 12% to 25% of Ethiopian adolescents are living with mental health problems.11,12 Additionally, there is strong evidence that poor mental health among youth is associated with poorer academic outcomes, substance use and abuse, violence, and poor sexual health.13
Therefore, exploring the factors associated with adolescent mental health is important from a life course perspective because it affects a nation’s human capital.14 Studies from around the world have shown that factors such as socio-demographic, family factors,15 risk behaviors,16 biological factors,17 exposure to violence and adversity18 are predictors of mental health issues for adolescents. In addition, given the positive or negative effect of social factors on the mental health of adolescents,19 critical investigations into these determinants in adolescent mental health are of the highest importance. This has been also indicated by the inclusion of addressing social and cultural domains of social determinants of mental health, including social capital to decrease early death, as also stated in the Sustainable Development Goals.20
Social capital refers to features of social organization, such as networks, norms, and social trust that facilitate coordination and cooperation for mutual benefit.21 Its theory suggests that interpersonal trust, norms of reciprocity, and exchange of social support each constitutes a type of resource and that access to these resources may promote the resilience of the individuals against difficulty.22 Social capital has become the topic of intense discussion, as it may represent a pathway through which public health interventions lead to improved health.23 Social capital is an important mechanism by which the socio-economic status (SES) influences the well-being of adolescents and is a powerful health protection resource that can be used by public health policy to address health apart from socio-economic inequalities.24 Likewise, social capital can act as a buffer for the detrimental impacts of social inequality on youth health.25 Families, schools, peers and neighborhoods26 cover adolescents’ main social networks in the context of social ecosystems and serve as the most dominant social capital for adolescents’ health benefits.27 As a result, most studies have linked different social capital indicators with a range of mental health outcomes.28
The association between social capital and adolescents mental health has been largely examined in high-income countries.29,30 The evidence from these studies show that social capital is positively associated with mental health through influencing health-related behaviors, access to health-care information and facilities, community participation, and provision of social support that helps in buffering of life stressors.31,32 Furthermore, studies suggest that the relative importance of adolescents’ social capital within the family, school and neighborhood context helps to understand the impact of these contexts on adolescents’ mental health.33,34
The psychological well-being of adolescents is dependent on both an individual vulnerability and environmental contexts35 which may differentially affect their social capital and mental health simultaneously.36 As a consequence, social capital has significant association with the mental health of adolescents depending on the location, socio-economic inequalities, ethnic origin and cultural background,37 all of which make the association vary across populations and transnational settings.37,38 As a result, the impacts of social capital on adolescents’ mental health need to be examined in context, particularly in low-income countries where there are significant gaps in the quality and access to mental health care.39
Harari is one of the nine regional states in Ethiopia, located in the eastern part of the country. The region has various unique traditional social organizations or groupings identified by age, sex and social obligations. The gender-based childhood friendship is called marignnat (ie, fraternity) in males and geilnat (ie, women’s peer groups) in girls of the same age and they may be in one neighborhood or classmates. It is gender-based group through which they begin their friendship at the early ages of childhood, and will maintain it throughout their life. Mugad (ie, puberty group) is semi-permanent group (a loose relationship) formed of both boys and girls of the same age (older than 15 or 16), and from the same neighborhood.40,41 This is a stage where groups assume societal obligations and responsibility to protect the society in any adversity to the extent of sacrificing life. Next, mugads will progress to the jama’ah level where a new entrant is accepted and unique set-up is established, hence, where emotion plays a vital role. Lastly, every married person must join afocha which is the backbone of all social institutions and the vanguard of the Hararis.41
Nonetheless, the relationship between social capital and adolescent mental health has been less explored and unclear in low-income countries like Ethiopia, despite it has been extensively studied in high-income countries,42 Thus, this study intends to critically examine the potential associations between social capital and mental health issues among adolescents in the particular context of Harari Regional State of Ethiopia. It is believed this study would contribute to a more targeted, context-sensitive approach to addressing the nexus between social capital and mental health issues, instead of adopting the often recommended universal, broad-based health interventions.
Methods
Study Settings and Design
The Harari region is located in eastern Ethiopia, 511 km from the capital Addis Ababa. Harari is the smallest region in Ethiopia, integrated into the Eastern Hararghe zone of the National Regional State of Oromia. Unlike most other regions of Ethiopia, the majority (54.2%) of the region’s population lives in urban settings.43 The capital of the region is the medieval era city of Harar, a dominantly city of Islamic religion yet a multi-ethnic, multi-linguistic and multi-cultural city. It is also considered as the most sacred city of Islam as a result of the rich collection of important Islamic monuments, including 82 mosques and 102 shrines.44 Trade is the principal source of income for the inhabitants of the region. Psychoactive substances like khat (Catha edulis), tobacco and coffee constitute important part of commercial activities. In connection with this, there is a high prevalence of culture of consuming khat in the community where approximately one-quarter of youth do so.43 Khat is the dominant cash crop in most of Harari’s rural sub-districts.44,45
A cross-sectional school survey design was adopted to carry out this study. During the study period, there were a total of 112 schools, of which 85 have both primary level (7th–8th grades) and secondary level (9th–12th grades) students. The data were collected from November 24 to December 31, 2020.
Population and Sampling
From the total of 112, 23 schools from both urban and rural areas, both public and private, were selected to be involved in this study. Multistage stratified sampling was used to select the schools and eligible students. First, the schools were stratified into urban versus rural, public schools versus private schools, and primary versus secondary schools. Then, 23 schools representing all the strata were randomly selected using lottery method proportionally. Finally, from each grade level of each school, sections were randomly chosen by lottery method considering the number of sections and students in those sections and all students of the selected sections were included in the study. In other words, the source population included all in-school adolescents in Harari Regional State whereas adolescents in the randomly selected schools constituted the study population. The sample size of the participant adolescents was calculated using OpenEpi stat software with the assumption of 32% proportion of adolescents with low social capital who have a mental health disorder (P1), an odds ratio of 0.62,46 95% level of confidence (Zα/2 = 1.96), 80% power of detection with 1:1 ratio and design effect = 2. After considering a 15% non-response rate, the sample became 1702. However, the data for this article was extracted from a large school-based mental health survey that encompassed 3227 adolescent students.
Data Collection
A structured and standardized guided self-administered questionnaire was used for collecting the data. The questionnaire includes items on sociodemographic characteristics, psychosocial factors, behavioral factors, and adolescent mental health problems. Mental health professionals and language experts revised the final version of the questionnaire to rephrase, modify, and conceptualize it based on inputs from the experts. Also, the questionnaire was pre-tested, and Cronbach’s alpha for reliability and validity was checked before the primary data collection. Accordingly, the report showed acceptable (>70%) reliability coefficient for each measure.
The process of data collection was carried out with the adolescent students inside their schools. A suitable setting (rooms) was arranged for those students whose room was “not suitable” for completing the questionnaire. The maximum classroom size was reduced to 25 students as a result of the COVID-19 pandemic and this was a good opportunity for the students to silently reflect and fill out the questionnaire. Also, orientation was given to them on the purpose of the study as well as on how to complete the questionnaire to maintain data quality. Two data collectors were assigned per session to facilitate and guide the students.
Variables and Measurements
A standard questionnaire used in earlier studies was adopted to assess social capital domains, socio-demographic variables, psychosocial variables and socio-economic status of the participants. Mental health problems (related to a range of mental problems such as emotional problems, conduct problems, hyperactivity/inattention and peer relationship problems) were assessed using the strength and difficulty questionnaire (SDQ-25).47 The SDQ has 25 items categorized into five sub-scales of five items each of which measures the conduct, hyperactivity, emotional and peer relationship problems and prosocial behaviors. The first four problem sub-scales contribute to a total difficulty score, and the fifth sub-scale is used to identify strengths. Each item is answered on a 3-point Likert scale ranging from “Not true” (rated as 0), “Somewhat true” (rated 1) to “Certainly true” (rated 2). “Somewhat true” is always noted as 1, but the notation of “Not true” and “Certainly true” varies depending on the scale elements.48 The SDQ was scored using the predictive algorithm converted into Stata syntax available on the SDQinfo website.49,50 Higher scores on the SDQ scale are associated with a greater risk of mental health problems.
By applying the method of score banding reported by Goodman, the self-completed version of SDQ total difficulties score was categorized into “Normal” (0–15), “Borderline” (16–19), and “Abnormal” (20–40) scores.37,48 The banding for each subcategory was described as follows. For emotional problems, the categories are Normal (0–5), Borderline (6), and Abnormal (7–10) scores. For conduct problems, the cut-off point for the Normal, Borderline, and Abnormal categories was (0–3), (4), and (5–10), respectively. The hypersensitivity problems subscale category is Normal (0–5), Borderline (6), and Abnormal (7–10), while the peer problem subscale for Normal, Borderline and Abnormal are (0–3), (4–5), and (6–10), respectively. For prosocial behaviors, the cut-off point for the Normal, Borderline and Abnormal categories were (6–10), (5) and (0–4), respectively.48 For each of the five subscales the score ranged from 0 to 10. The sum of the first four problem domains (excluding the prosocial behavior items) was used to generate total difficulties score ranging from 0 to 40, which is further categorized as Normal (score ≤15), Borderline (score 16–19), and Abnormal (score 20–40). The total SDQ was used and it showed a Cronbach’s α of 0.73. The alpha coefficients for each problem subscales were 0.53 for emotional symptoms, 0.51 for conduct problems, and 0.46 for hyperactivity, and 0.31 for peer problems subscale.
Social capital was measured using a social capital questionnaire for adolescent students (SCQ-AS) which has 12 items divided into four domains. The domains include social cohesion at school, the network of friends at school, social cohesion in the community or neighborhood, and trust in the school and community or neighborhood with four, three, two, and three items, respectively.51 Each question has three possible response (ie, I agree (3), I have no opinion/I do not know (2), and I disagree (1).51 However, items 11 and 12 had reversed scores (negative questions). The sum of the score ranged from 12 to 36 for the total social capital score (ie, 4 to 12 for the first domain, 3 to 9 for the second domain, 2 to 6 for the third domain, and 3 to 9 for the fourth domain). A higher score indicates higher social capital for all fields. The score was categorized by the quartile and dichotomized as “lowest” if the value of the sum of the scores is less or equal to the 1st quartile and “highest” if the value is higher than the value of the 1st quartile.52 The Cronbach’s α reliability score for the whole social capital scale (SCQ-AS) in this study was 0.71 and its subscales are as follows: social cohesion at school = 0.40; the network of friends at school = 0.60; social cohesion in the community or neighborhood = 0.70; and, trust in the school and community or neighborhood = 0.50.
The family-related psychosocial variables including living arrangements, manner of bringing-up and parent’s living situation were assessed using a standard questionnaire formulated based on literature. Socioeconomic status included parents’ educational status, occupation, and wealth were considered and indexed. Wealth index was measured using number and kind of known goods the family owns as reported by the adolescent and analyzed using the principal component analysis.53
Data Processing and Analysis
The data were double entered, validated, and cleaned using EpiData 3.1 and analyzed using STATA 14.1. Descriptive statistics of the categorical data was summarized using the Chi-square test. Those variables with p-value <0.20 in the bivariate analyses were considered in the multivariable analyses. The relationship between social capital and mental health problem was identified using multivariable ordinal logistic regression (OLR). The parallel line assumption and Brant supported the OLR model. Stepwise multiple models were used to examine the relationship between social capital domains and mental health problems. Model 1 shows the relationship between the first dimension of adolescent social capital, namely ‘social cohesion at school’, and mental health problems. Model 2 shows the relationship between the second dimension of adolescent social capital, namely “network of friends at school”, and mental health problems. Model 3 shows the relationship between the third dimension of adolescent social capital, namely ‘trust in school or neighborhood’, and mental health problems. Model 4 shows the relationship between the fourth dimension of adolescent social capital – ie, “social cohesion in the neighborhood” – and mental health problems. Model 5 is the final model that shows the association between all dimensions of adolescent social capital domains and mental health problems. The result was reported using odds ratio along with 95% confidence interval. Finally, p-value <0.05 was considered as statistically significant association.
Results
Sociodemographic Characteristics
A total of 3227 adolescent students were included in the study. The mean age of the respondents was 15.69 (±1.79) years, ranging from 13 to 19 years. The majority of the respondents were from urban (83.85%) and live with both biological parents (71.34%). Half of them were girls (51.75%), who were in the primary schools (51.84%) and Muslims (54.2%). More than six in ten respondents reported high social capital in all domains where social cohesion at school, networking with friends at school, trust in school or neighborhood, and social cohesion in the neighborhood were 61.2%, 77.7%, 66.5%, and 66.07%, respectively. Overall, about seventy percent of the participants were scored highest in the total social capital score (Table 1).
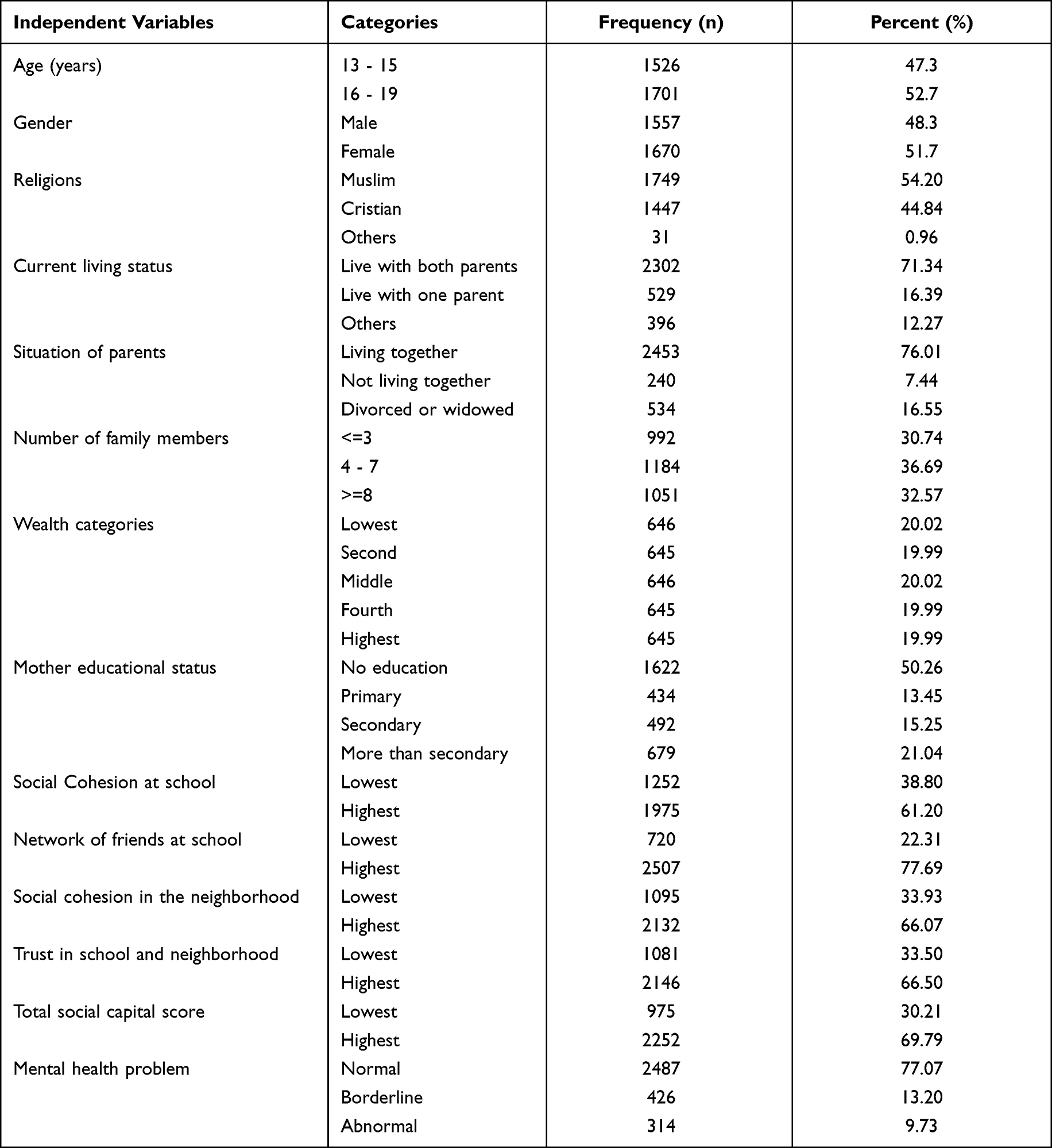 |
Table 1 Socio-Demographic Characteristics of the Respondent’s (n = 3227) in Harari Regional State, Eastern Ethiopia, 2020 |
Mental Health Problem and Its Association with Social Capital
Analysis of the obtained data revealed a total of 740 (22.93%, 95% CI, 21.5–24.4) adolescents had experienced mental health problems, of which 9.7% (95% CI, 8.7–10.8) and 13.20% (95% CI, 12–14) fall in the “abnormal” and “borderline” classification, respectively. Both “borderline” and “abnormal” mental health problems were lower among adolescents with highest social capital score across all domains. In41 the bivariate analyses age, sex, religion, family size, parental occupation and wealth index were associated with mental health problems at p < 0.20. Likewise, the prevalence of “borderline” and “abnormal” categories of mental health problem score was lower compared with the highest social capital score across all social capital domains. Additionally, the chi-square tests showed significant associations between categories of mental health problems and each of the social capital domains (p < 0.001) (Table 2).
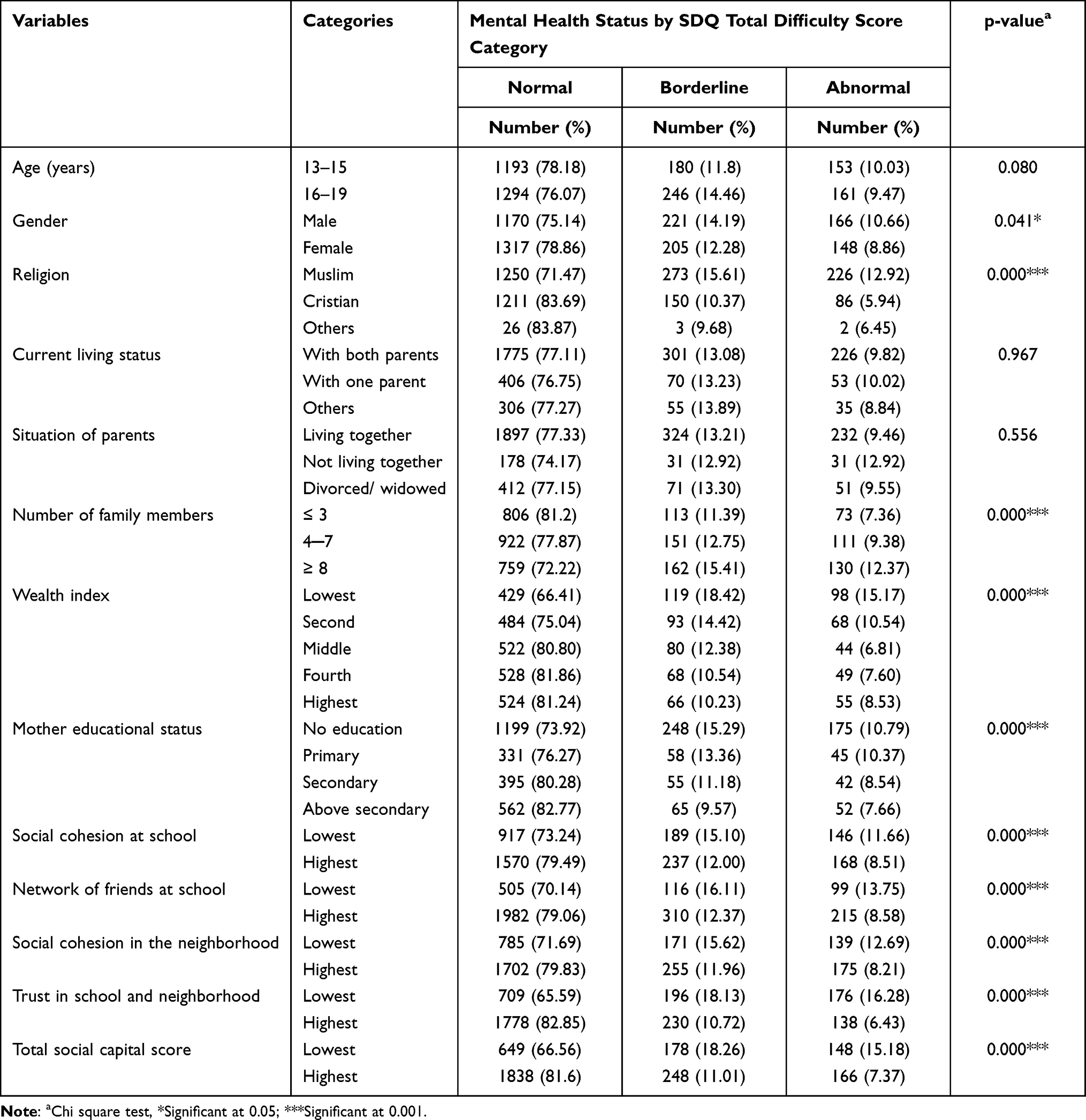 |
Table 2 Distribution of Control Variables and Social Capital Domains with the Prevalence of Mental Health Problems Among Adolescents of 13 to 19 Years (n = 3227) in Harari Regional State, Eastern Ethiopia, 2020 |
In a similar manner, in the multivariable ordinal logistic regression religion, household wealth, style of bringing up, and parental occupation were significantly associated with mental health problems. Mental health problems were less likely among Christians (AOR = 0.70, 95% CI: 0.57–0.87), and families in the middle wealth index (AOR = 0.70, 95% CI: 0.53–0.92). Whereas mental health problems were most likely in adolescents who were raised without families (AOR = 1.63, 95% CI: 1.1–2.4), with merchant parents (AOR = 1.27, 95% CI: 1.01–1.6) and farmers (AOR = 1.90, 95% CI: 1.44–2.5) in relation to employees and other day-workers.
For adolescents who had the highest social cohesion at school (AOR = 0.71, 95% CI: 0.60–0.85), the odds of being at combined borderline and abnormal level of mental health problem score decreased by 29% as compared to adolescents who had the lowest social cohesion at school (Model 1). For adolescents who had the highest network, compared to the lowest network, of friends at school, the odds of high versus low-level mental health problem score are 0.63 times lower (AOR = 0.63, 95% CI: 0.53–0.77) (Model 2). Adolescents who had the highest trust in school or neighborhood had the lowest level of mental health problem score by 50% compared to students who had the lowest trust in school or neighborhood (AOR = 0.50, 95% CI: 0.42–0.60) (Model 3). Higher social cohesion in the community (AOR = 0.66, 95% CI: 0.55–0.89) also reduces mental health problem score by 44% than lower social cohesion in the community (Model 4).
In the final model (Model 5), all social capital factors and control variables regressed together. The results revealed that highest network of friends at school (AOR = 0.75, 95% CI: 0.58–0.99), in contrast to the lowest, highest trust in school or neighborhood (AOR = 0.52, 95% CI: 0.44–0.63), in contrast to the lowest, and highest social cohesion in the community (AOR = 0.75, 95% CI: 0.62–0.89), in contrasts to lowest, remained constantly lowering the level of mental health problem score (Table 3).
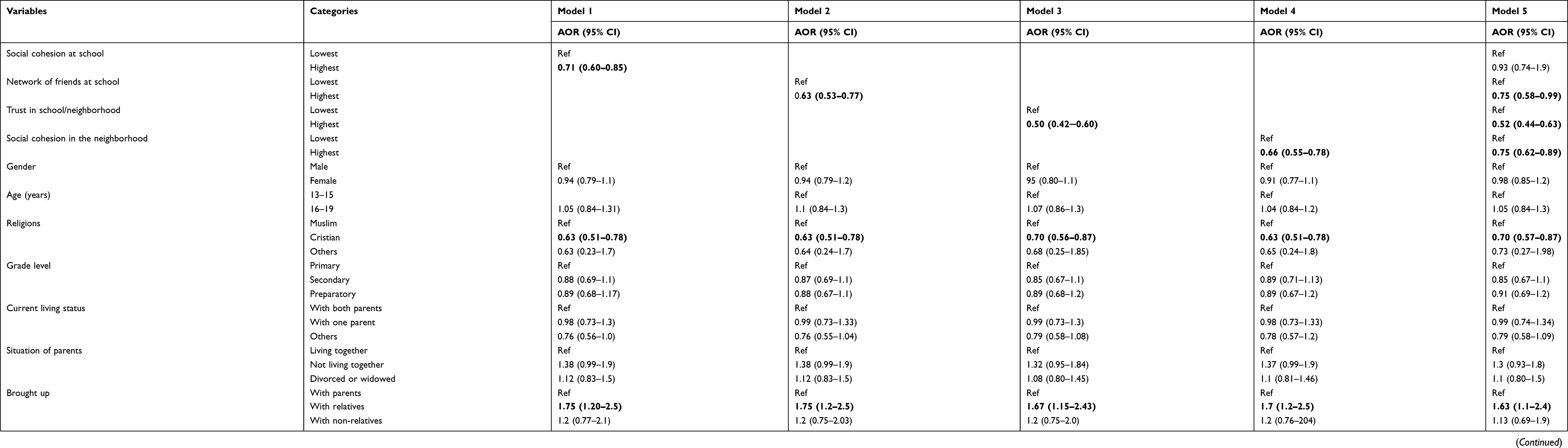 |
Table 3 Association of Social Capital with Mental Health Problems Among Adolescents of 13 to 19 Years (n = 3227). In Harari Regional State, Eastern Ethiopia, 2020 |
Discussion
To iterate, this study was conducted to assess the association between social capital and mental health problems among in-school adolescents in Harari region of eastern Ethiopia. The findings indicated that one in five adolescents had mental health problems. A network of friends at school, trust at school or neighborhoods, and social cohesion in the communities are associated with level of mental health problems.
In this study, adolescents with high social cohesion in the neighborhood were less likely to experience mental health problems. This finding is further supported by previous evidence in United States,54 Brazil,55 South Africa,56 and Kenya.57 Bourdieu argues that an individual’s contact with networks results in an accumulation of shared exchanges, obligations and identities that in turn provide potential support and access to resources.58 Cohesive neighborhoods with common social expectations may have a positive impact on adolescents’ mental health.54 The possible explanation for this is in more cohesive communities, adolescents may benefit from the informal social control that prevents them from engaging in risky health behaviors such as addictions, unsafe sexual relationships and other factors. In addition, the exploration of multiple behavioral patterns in adults through increased social learning and positive emotional and instrumental support59 may protect adolescents’ mental health. Hence, neighborhood quality may affect family management practices, which might be related to adolescent health adjustment.60
Specific to the study setting, multi-ethnic groups lived together with many intercommunal associations and neighborhood organizations that have built a deeply-rooted culture of peace, tolerance and ties61 over the past centuries.41,62 This may increase social integration, cohesion and connections among the community giving the individual a good sense of life that may improve the protection and promotions of mental health among adolescents in the region.41,63 Moreover, people in the region commonly eat and drink communally which might have strengthened inter-communal relationships.62 In families with strong and cohesive bonds between their members, engagement in frequent joint activities appear to create an environment where adolescents can achieve better health and wellbeing.34 This implies that strong social cohesion embedded in local communities may have greater protective power against adolescent mental health problems. Yet, this needs further extensive investigation and exploration of intervention strategies to reduce the prevalent mental health problems.
The findings of this study reveal that a higher level of trust in school or neighborhood lowers adolescent mental health problems. This finding is consistent with previous studies in Lithuania,64 Iran,65 South Africa,56 and Kenya.57 The reason might be that trustworthiness of others might help to facilitate the individual’s perceived social support from neighbors and friends. This, in turn, makes adolescents more likely to have faith in their neighborhood and friends66,67 which, subsequently, enhances resilience and reduces vulnerability to mental health problems through receiving social support from them. The trust might also interfere with the severity of the psychosocial risk of adolescents’ mental health problems by playing a buffering role against negative trauma-related cognition.68 Adolescents with high trust frequently spend their time with neighborhood friends, engage in games, sports, and other activities with mutual communication69 that may increase the sense of belongingness which may promote better mental health. In Harari Region, Muslim and Christian students learn in mixed (both in terms of gender and religion) schools, study or play together, and visit the homes of their friends together, and all these often lead to lifelong relationships.40,41 Hence, these communal rituals might help them to develop a chance to develop high social support that facilitates greater expression of trust,70 which, in-turn, may support the development of health and well-being among adolescents.
Moreover, the findings of this study indicate a network of friends at school decreases mental health problems. Similarly, studies in United States indicated that a high network of friends could matter so much that having sufficient friends with a healthy mood could have the probability of reliving someone from depression.71 Further, school connectedness and a sense of belongingness may have a substantial protective impact on adolescent mental health. In addition, a higher frequency of contact and a higher network of friends are linked to increasing social trust, reducing stress and improving mental health.72
In the present study setting, there is gender-based childhood friendship with the same age in boys and girls called marignnat (ie, fraternity) and geilnat (ie, women’s peer groups). These groups may be in one neighborhood or classmates where they begin their friendship at the early ages of childhood and they often maintain it throughout their life. There is also a group called mugad (ie, puberty group) which is a semi-permanent group (a loose relationship) formed of both boys and girls of the same age (older than 15 or 16), and from the same neighborhood.40,41 It is at this stage that the groups assume societal obligations and responsibility to protect the society in any adversity to the extent of sacrificing their life. Next, the mugads progress to the jama’ah, a level where a new entrant is accepted and a unique set-up where emotions play the biggest role is established.41 These social formations may not only build opportunities for the adolescents to increase their own social networks at school and neighborhoods but also support them to acquire and mobilize protective forms of social capital within a range of different networks. Likewise, the findings of this study affirm promotion of friendship between adolescents can reduce both incidence and prevalence of mental health problems.
The strength of this study is the inclusion of urban and rural students derived both from public and private schools. This removes major socioeconomic confounders. In addition, the study used validated tools which were guided and self-administered. Yet, this study has some limitations. Primarily, the study utilized a cross-sectional design that may not exclude possible reverse causality between mental health and social capital and vice versa. For instance, good mental health can lead to high social capital for families, neighbors and schools, and adolescents with higher scores of mental health problems are expected to report lower levels of social capital. To add, the greater the problems associated with peer relationships, the poorer the social capital. Therefore, future studies should investigate the same associations as in this study on the same sample, with prospective study design, to answer the question on the inverse causation between the variables. Another limitation of this study is that it analyzed social capital based on students’ level of perception, which might be affected by several student characteristics. Finally, Covid-19 pandemic which was prevalent during the study period was not considered in this study as a confounder, but it might have influenced the social capital perceptions among students.
Conclusion
One-fifth of the school adolescents have mental health problems. The highest in-school networks of friends, trust at school or neighborhood, and neighborhood social cohesion predicts the adolescent’s mental health problems. This highlights strengthening in-school networks of friends, trust at school or neighborhoods, and neighborhood social cohesion substantially contributes to reducing the problems. Tailored interventions targeting prevention strategies of mental health problems should include the social capital at the individual, neighborhood and community level to prevent the problem and promote mental health in adolescents and other social age groups.
Abbreviations
ADHD, attention deficit hypersensitivity disorder; AOR, adjusted odds ratio; OLR, ordinal logistic regression; SCQ-AS, social capital questionnaire for adolescent students; SDG, sustainable development goal; SDQ, strength and difficulty questionnaire.
Data Sharing Statement
All the data used for this study are included in the article. Additional data are available from the corresponding author on a reasonable request.
Ethical Approval
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University, College of Health and Medical Sciences with Ref. No IHRERC/149/2019. A formal letter of cooperation was addressed to the Education Bureau of the Harari Region and to each school. Respondents, parents/guardians and school principals were provided with clear and adequate information regarding the research, including purpose, procedures, potential risks and benefits. The adolescents were informed that their participation was voluntary and that not participating in the study would not disadvantage the family or adolescents, and that they could stop completing the questionnaire at any time or skip questions they did not want to answer. Written informed and signed voluntary consent from one of the parents or guardians and school principals and written voluntary assent from the adolescents were obtained for participants between 13 and 17 years age. Those participants who were 18 years and older provided their consent. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality. All data collected were anonymized and kept on personal computer protected with password. All information remained anonymous and confidential. Both participants and their parents were informed that the information gathered would be disseminated to assist in knowledge generation only. The study was conducted following the Declaration of Helsinki’s ethical principles for Medical research involving human subjects.
Acknowledgments
The authors would like to thank Haramaya University for funding this study. We would also like to thank Harari Region Education Office, involved schools’ directors and teachers, participants, and data collectors for meticulously facilitating and conducting the work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and, all agreed to be accountable for all aspects of the work.
Funding
This study was funded by the University of Haramaya Scientific Research Grant number (HURG-2020-02-01-92) after defending the study proposal. The funder has no role in the design of the study and collection, analysis, or interpretation of data as well as in writing the manuscript.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. UNICEF. The adolescent brain: a second window of opportunity. Florence: UNICEF Office of Research; 2021. Available from: https://www.unicef-irc.org/publications/933-the-adolescent-brain-a-second-window-of-opportunity-a-compendium.html.
2. World Health Organization. Global Accelerated Action for the Health of Adolescents ( AA-HA!): Guidance to Support Country Implementation. World Health Organization; 2017.
3. Saxena S. Excess mortality among people with mental disorders: a public health priority. Lancet Public Health. 2018;3(6):e264–e265. doi:10.1016/S2468-2667(18)30099-9
4. Kessler RC, Avenevoli S, Costello EJ, et al. Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the National Comorbidity Survey Replication Adolescent Supplement. Arch Gen Psychiatry. 2012;69(4):372–380. doi:10.1001/archgenpsychiatry.2011.160
5. Vos T, Barber RM, Bell B, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. lancet. 2015;386(9995):743–800.
6. World Health Organization. Social determinants of mental health. World Health Organization; 2014. Available from: https://apps.who.int/iris/handle/10665/112828.
7. WHO. Adolescent mental health; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health.
8. Kessler RC, Angermeyer M, Anthony JC, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry. 2007;6(3):168.
9. World Health Organization. Adolescent mental health; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health.
10. Cortina MA, Sodha A, Fazel M, Ramchandani PG. Prevalence of child mental health problems in sub-Saharan Africa: a systematic review. Arch Pediatr Adolesc Med. 2012;166(3):276–281. doi:10.1001/archpediatrics.2011.592
11. Ministry of Health of Ethiopia. National Adolescent and Youth Health Strategy (2016–2020) Federal Democratic Republic of Ethiopia Ministry of Health. Addis Ababa: Ministry of Health of Ethiopia; 2016.
12. Federal Democratic Republic of Ethiopia Ministry of Health. National Mental Health Strategy 2012/13–2015/2016. Addis Ababa: Ministry of Health; 2012.
13. World Health Organization. Adolescent and young adult health; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions.
14. Oluwaseyi SD, Fotso AS. The effect of family and neighbourhood social capital on youth mental health in South Africa. J Adolesc. 2020;83:22–26. doi:10.1016/j.adolescence.2020.06.009
15. Wüstner A, Otto C, Schlack R, Hölling H, Klasen F, Ravens-Sieberer U. Risk and protective factors for the development of ADHD symptoms in children and adolescents: results of the longitudinal BELLA study. PLoS One. 2019;14(3):e0214412. doi:10.1371/journal.pone.0214412
16. Wang GS, Hoyte C. Common substances of abuse. Pediatr Rev. 2018;39(8):403–414. doi:10.1542/pir.2017-0267
17. Lamis DA, Dvorak RD. Mindfulness, nonattachment, and suicide rumination in college students: the mediating role of depressive symptoms. Mindfulness. 2014;5(5):487–496. doi:10.1007/s12671-013-0203-0
18. Wang S, Xu H, Zhang S, et al. Linking childhood maltreatment and psychological symptoms: the role of social support, coping styles, and self-esteem in adolescents. J Interpers Violence. 2020;37:0886260520918571.
19. Williams DR, Priest N, Anderson N. Understanding associations between race, socioeconomic status, and health: patterns and prospects. In: The Social Medicine Reader. Vol. II.
20. World Health Organization. Calouste gulbenkian foundation. In: Social Determinants of Mental Health. Geneva: World Health Organization; 2014.
21. Mohnen SM, Groenewegen PP, Völker B, Flap H. Neighborhood social capital and individual health. Soc Sci Med. 2011;72(5):660–667. doi:10.1016/j.socscimed.2010.12.004
22. Li C, Jiang S, Fang X. Effects of multi-dimensional social capital on mental health of children in poverty: an empirical study in Mainland China. J Health Psychol. 2017;25:1359105317737608.
23. Coll‐Planas L, Del Valle Gómez G, Bonilla P, Masat T, Puig T, Monteserin R. Promoting social capital to alleviate loneliness and improve health among older people in S pain. Health Soc Care Community. 2017;25(1):145–157. doi:10.1111/hsc.12284
24. Addae EA. The mediating role of social capital in the relationship between socioeconomic status and adolescent wellbeing: evidence from Ghana. BMC Public Health. 2020;20(1):1–11. doi:10.1186/s12889-019-8142-x
25. De Clercq B, Vyncke V, Hublet A, et al. Social capital and social inequality in adolescents’ health in 601 Flemish communities: a multilevel analysis. Soc Sci Med. 2012;74(2):202–210. doi:10.1016/j.socscimed.2011.10.025
26. Ge T. Effect of socioeconomic status on children’s psychological well-being in China: the mediating role of family social capital. J Health Psychol. 2020;25(8):1118–1127. doi:10.1177/1359105317750462
27. Shiell A, Hawe P, Kavanagh S. Evidence suggests a need to rethink social capital and social capital interventions. Soc Sci Med. 2018;257:111930.
28. Morgan A, Svedberg P, Nyholm M, Nygren J. Advancing knowledge on social capital for young people’s mental health. Health Promot Int. 2021;36(2):535–547. doi:10.1093/heapro/daaa055
29. Agampodi TC, Agampodi SB, Glozier N, Siribaddana SJ. Measurement of social capital in relation to health in low and middle income countries (LMIC): a systematic review. medicine. 2015;128:95–104.
30. Rothon C, Goodwin L, Stansfeld SJ. Family social support, community “social capital” and adolescents’ mental health and educational outcomes: a longitudinal study in England. Epidemiology. 2012;47(5):697–709.
31. Grosso A. Social support as a predictor of HIV testing in at-risk populations: a research note. J Health Hum Serv Adm. 2010;33:53–62.
32. Morgan A, Haglund BJ. Social capital does matter for adolescent health: evidence from the English HBSC study. Health Promot Int. 2009;24(4):363–372. doi:10.1093/heapro/dap028
33. Morgan AR, Rivera F, Moreno C, Haglund BJ. Does social capital travel? Influences on the life satisfaction of young people living in England and Spain. BMC Public Health. 2012;12(1):1–12. doi:10.1186/1471-2458-12-138
34. Novak D, Emeljanovas A, Mieziene B, Štefan L, Kawachi I. How different contexts of social capital are associated with self-rated health among Lithuanian high-school students. Glob Health Action. 2018;11(1):1477470. doi:10.1080/16549716.2018.1477470
35. Jonsson KR, Busfield J, Södergren M, Karen M, Adjei NK. Social capital, deprivation and psychological well-being among young adolescents: a multilevel study from England and Wales. Int J Environ Res Public Health. 2020;17(10):3420. doi:10.3390/ijerph17103420
36. McLaren L, Hawe P. Ecological perspectives in health research. J Epidemiol Community Health. 2005;59(1):6–14. doi:10.1136/jech.2003.018044
37. Drukker M, Buka SL, Kaplan C, McKenzie K, Van Os J. Social capital and young adolescents’ perceived health in different sociocultural settings. Soc Sci Med. 2005;61(1):185–198. doi:10.1016/j.socscimed.2004.11.041
38. Islam MK, Merlo J, Kawachi I, Lindström M, Gerdtham U-G. Social capital and health: does egalitarianism matter? A literature review. Int J Equity Health. 2006;5(1):1–28. doi:10.1186/1475-9276-5-3
39. Kola L, Kohrt BA, Hanlon C, et al. COVID-19 mental health impact and responses in low-income and middle-income countries: reimagining global mental health. Lancet Psychiatry. 2021;8:535–550. doi:10.1016/S2215-0366(21)00025-0
40. Zekaria A. Harari basketry through the eyes of Amina Ismael Sherif. Ethiopia: Traditions of Creativity. Michigan State University Museum East Lansing; 1999:47–63.
41. Ahmed WM. History of Harar and the Hararis. Harar, Harari People Regional State Culture, Heritage and Tourism Bureau; 2008.
42. Maass R, Kloeckner CA, Lindstrøm B, Lillefjell M. The impact of neighborhood social capital on life satisfaction and self-rated health: a possible pathway for health promotion? Health Place. 2016;42:120–128. doi:10.1016/j.healthplace.2016.09.011
43. Central Statistical Authority (CSA). The 2007 Population and Housing Census of Ethiopia: “Statistical Report for Harari Region” for the Census; Population and Housing Census of 2007. Centeral Statistical Agency-Ministry of Finance and Economic Development; 2007.
44. Harari Bureau of Finance and Economic Development. Baseline data of Harari region (Harar, 2010). 2010.
45. INDEPTH Network. Harar urban HDSS INDEPTH core dataset 2012–2016 (Release 2018). Version: v1. Dataset; 2018. Available from: https://doi.org/10.7796/INDEPTH.ET042.CMD2016.v1.
46. Novak D, Kawachi I. Influence of different domains of social capital on psychological distress among Croatian high school students. Int J Ment Health Syst. 2015;9(1):18. doi:10.1186/s13033-015-0010-1
47. Meltzer H, Gatward R, Goodman R, Ford T. Mental health of children and adolescents in Great Britain. Int Rev Psychiatry. 2003;15(1–2):185–187. doi:10.1080/0954026021000046155
48. Goodman R, Meltzer H, Bailey V. The Strengths and Difficulties Questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry. 1998;7(3):125–130. doi:10.1007/s007870050057
49. Boyer NR, Miller S, Connolly P, McIntosh E. Paving the way for the use of the SDQ in economic evaluations of school-based population health interventions: an empirical analysis of the external validity of SDQ mapping algorithms to the CHU9D in an educational setting. Qual Life Res. 2016;25(4):913–923. doi:10.1007/s11136-015-1218-x
50. Information for researchers and professionals about the Strengths and Difficulties Questionnaire. Available from: http://www.sdqinfo.com/.
51. Paiva PCP, Paiva HN, Oliveira Filho PM, et al. Development and validation of a social capital questionnaire for adolescent students (SCQ-AS). PLoS One. 2014;9(8):e103785. doi:10.1371/journal.pone.0103785
52. Rajão SD, Zarzar PM, Ferreira RC, Ferreira EFE. The social capital among adolescent students of a Brazilian municipality. Cien Saude Colet. 2019;24:4061–4070. doi:10.1590/1413-812320182411.14052017
53. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
54. Donnelly L, McLanahan S, Brooks-Gunn J, et al. Cohesive neighborhoods where social expectations are shared may have positive impact on adolescent mental health. Health Aff. 2016;35(11):2083–2091. doi:10.1377/hlthaff.2016.0721
55. Kingsbury M, Clayborne Z, Colman I, Kirkbride JB. The protective effect of neighbourhood social cohesion on adolescent mental health following stressful life events. Psychol Med. 2020;50(8):1292–1299. doi:10.1017/S0033291719001235
56. Chola L, Alaba O. Association of neighbourhood and individual social capital, neighbourhood economic deprivation and self-rated health in South Africa–a multi-level analysis. PLoS One. 2013;8(7):e71085. doi:10.1371/journal.pone.0071085
57. Musalia J. Social capital and health in Kenya: a multilevel analysis. Soc Sci Med. 2016;167:11–19. doi:10.1016/j.socscimed.2016.08.043
58. Bourdieu P, Richardson JG. Handbook of Theory and Research for the Sociology of Education. Greenwood Press New York; 1986.
59. Silk JS, Sessa FM, Sheffield Morris A, Steinberg L, Avenevoli S. Neighborhood cohesion as a buffer against hostile maternal parenting. J Fam Psychol. 2004;18(1):135. doi:10.1037/0893-3200.18.1.135
60. Kliewer W, Cunningham JN, Diehl R, et al. Violence exposure and adjustment in inner-city youth: child and caregiver emotion regulation skill, caregiver–child relationship quality, and neighborhood cohesion as protective factor. J Clin Child Adolesc Psychol. 2004;33(3):477–487. doi:10.1207/s15374424jccp3303_5
61. Burton RFS. First Footsteps in East Africa. Good Press; 2019.
62. Shetler JB, Yehualashet D. Building a “City of Peace” through Intercommunal Association Muslim-Christian Relations in Harar, Ethiopia, 1887–2009. J Religion Conflict Peace. 2010;4(1):3.
63. Saeri AK, Cruwys T, Barlow FK, Stronge S, Sibley CG. Social connectedness improves public mental health: investigating bidirectional relationships in the New Zealand attitudes and values survey. Austral NZ J Psychiatry. 2018;52(4):365–374. doi:10.1177/0004867417723990
64. Novak D, Popovic S, Emeljanovas A, Mieziene B, Kristicevic T, Popovic S. Are family, neighbourhood and school social capital associated with psychological distress among Lithuanian high-school students? A cross-sectional study. Int J Sport Manag Recreat Tour. 2016;23:75–89.
65. Mohammadi MR, Badrfam R, Zandifar A, et al. Social capital of parents of children and adolescents and its relation to psychiatric disorders; a population-based study. Community Ment Health J. 2022;2022:1–11.
66. Uslaner EM. The Moral Foundations of Trust. Cambridge University Press; 2002.
67. Uslaner EM. The foundations of trust: macro and micro. Cambridge J Econ. 2007;32(2):289–294. doi:10.1093/cje/bem039
68. Bhattacharyya S, Davis J, Vogl T, et al. Enhancing Autonomy with Trusted Cognitive Modeling. Association for Unmanned Vehicle Systems International; 2015.
69. Morrow V. Young people’s explanations and experiences of social exclusion: retrieving Bourdieu’s concept of social capital. Int J Sociol Soc Policy. 2001;21:37–63. doi:10.1108/01443330110789439
70. Pei F, Wang Y, Wu Q, McCarthy KS, Wu S. The roles of neighborhood social cohesion, peer substance use, and adolescent depression in adolescent substance use. Child Youth Serv Rev. 2020;112:104931. doi:10.1016/j.childyouth.2020.104931
71. Hill EM, Griffiths FE, House T. Spreading of healthy mood in adolescent social networks. Proc Royal Soc B. 2015;282(1813):20151180. doi:10.1098/rspb.2015.1180
72. Van der Horst M, Coffé H. How friendship network characteristics influence subjective well-being. Soc Indic Res. 2012;107(3):509–529. doi:10.1007/s11205-011-9861-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.