Back to Journals » International Medical Case Reports Journal » Volume 19
High-Output Heart Failure from A Decade-Old Traumatic AV Fistula: A Case Report
Authors Amini SM ![]() , Hidalgo K, Huang J, Plambeck C, Murray KT, Fadumiye C
, Hidalgo K, Huang J, Plambeck C, Murray KT, Fadumiye C ![]()
Received 22 January 2026
Accepted for publication 17 April 2026
Published 18 May 2026 Volume 2026:19 594595
DOI https://doi.org/10.2147/IMCRJ.S594595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Sara Mariam Amini, Keziah Hidalgo, Justine Huang, Christopher Plambeck, Kyle T Murray, Christopher Fadumiye
Department of Anesthesiology, Medical College of Wisconsin, Milwaukee, WI, USA
Correspondence: Christopher Fadumiye, Email [email protected]
Background: Chronic traumatic arteriovenous fistulas (AVFs) are uncommon but potentially devastating sequelae of penetrating vascular injuries. Persistent high-flow shunting can lead to progressive cardiopulmonary remodeling, pulmonary hypertension, atrial arrhythmias, and high-output heart failure (HOHF).
Case Presentation: We report a 41-year-old male with a chronic high-flow AVF between the left mid-superficial femoral artery and superficial femoral vein secondary to a gunshot wound sustained over a decade prior. Initially managed nonoperatively and later lost to follow-up, he presented with HOHF, atrial fibrillation with rapid ventricular response, pulmonary hypertension. The fistula resulted in extensive venous dilation of the left thigh with marked proximal venous enlargement involving the iliac veins, inferior vena cava, and a large pelvic venous varix, consistent with chronic high-flow shunting. The maximum diameter of the left iliac vein measured 8.7 cm. Preoperative echocardiography demonstrated preserved ejection fraction (50– 55%), biatrial enlargement, moderate tricuspid regurgitation, and elevated pulmonary artery pressures. He underwent planned endovascular repair with invasive hemodynamic monitoring, including right heart catheterization and intraoperative transesophageal echocardiography. Following fistula closure, pulmonary artery pressures decreased (33/20 mmHg to 22/15 mmHg) and cardiac output improved (14.9 L/min to 8.6 L/min). Postoperative recovery was uneventful with controlled hemodynamic management in the cardiovascular ICU. Four-month follow-up imaging showed significant reduction in iliac vein diameter (8.7 cm to 6.2 cm).
Conclusion: This case highlights the cardiovascular consequences of long-standing traumatic AVFs and underscores the importance of multidisciplinary planning and vigilant perioperative management. Notably, significant hemodynamic improvement can occur even after prolonged high-flow states, emphasizing the potential reversibility of cardiopulmonary remodeling with timely intervention.
Keywords: high output heart failure, arterial-venous fistula, echocardiography, gun shot wound
Introduction
Gunshot wounds (GSWs) remain a significant public health concern in the United States, accounting for over 115,000 firearm-related injuries and more than 45,000 deaths annually.1,2 GSWs and other penetrating trauma-related vascular injuries can cause complicated sequelae including arteriovenous fistulas (AVF). AVFs are abnormal connections between an artery and a vein that can form after trauma. If ignored, these fistulas frequently result in progressive hemodynamic concerns, including pulmonary hypertension, atrial arrhythmias, steal syndrome, and thrombotic events. Chronic high-flow fistulas may be linked to pulmonary hypertension, atrial arrhythmias, valve dysfunction, and high-output heart failure (HOHF), even if some AVFs may not cause any symptoms.3–5
Surgical and endovascular interventions play a critical role in the management of traumatic AVFs. However, these fistulas may continue to exist due to a lack of follow-up and delayed detection, which would cause a substantial cardiovascular burden.3 Data on long-standing AVFs in non-dialysis patients undergoing major surgery remain limited but has shown long-term AVF patients may experience permanent cardiac remodeling, which calls for meticulous preoperative planning and interdisciplinary review.6
We present a case of a 41-year-old male with a history of a traumatic left femoral AVF secondary to a GSW over a decade earlier. Initially managed nonoperatively, the fistula ultimately led to HOHF, atrial fibrillation with rapid ventricular response, and pulmonary hypertension. This case emphasizes the importance of early recognition and intervention in traumatic AVF to prevent progressive cardiovascular deterioration. Written informed consent for publication of this case report, including relevant clinical details and accompanying images, was obtained from the patient. The authors confirm that all reasonable efforts were made to protect patient anonymity and that the report adheres to the CARE guidelines for case reports. Institutional approval was not required for the preparation and publication of this report.
Clinical Course
A 41-year-old male with history significant for a left traumatic AVF between the mid left superficial femoral artery and vein, heart failure with preserved ejection fraction (HFpEF), atrial fibrillation, pulmonary hypertension, moderate tricuspid regurgitation and patent foramen ovale presented for a scheduled endovascular repair (EVAR) of left femoral AVF. This fistula developed as sequelae of a GSW sustained over ten years prior to this surgery. Three months prior to the surgery, he presented to the emergency department with a week of worsening chest pressure, shortness of breath, and epigastric pain with vitals showing a blood pressure of 134/78, heart rate at 112, and respiratory rate at 24. At baseline, he was independently functional and able to perform all his activities of daily living without difficulty. Initial electrocardiogram showed that he was in new atrial fibrillation with rapid ventricular rate. Physical exam showed jugular venous distension, a 3/6 diastolic murmur, bruit over right upper thigh, and bilateral lower extremity edema. Initial labs drawn showed chronic anemia, no electrolyte abnormalities, elevated BNP at 4241, and normal troponins. Updated echocardiogram was consistent with acuteness on previously undiagnosed chronic HOHF with a D-shaped left ventricle and other values shown in Table 1. In the emergency department, he underwent successful electrical cardioversion, started on metoprolol and nicardipine infusion for rate control, and given diuresis with targeted clinical improvement. Vascular surgery consulted during admission diagnosed his AVF as the root cause of the heart failure, and he was followed for outpatient medical optimization prior to the scheduled surgery. Imaging demonstrated that the fistula resulted in extensive venous dilation of the left thigh with marked proximal venous enlargement involving the iliac veins, inferior vena cava, and a large pelvic venous varix. At that time, his greatest left iliac vein diameter measured 8.7 cm (Figure 1), with normal values ranging between 0.8–1.2 cm. Although his AVF was initially being monitored with periodic imaging, he was unfortunately lost to follow up 5 years after the initial injury.
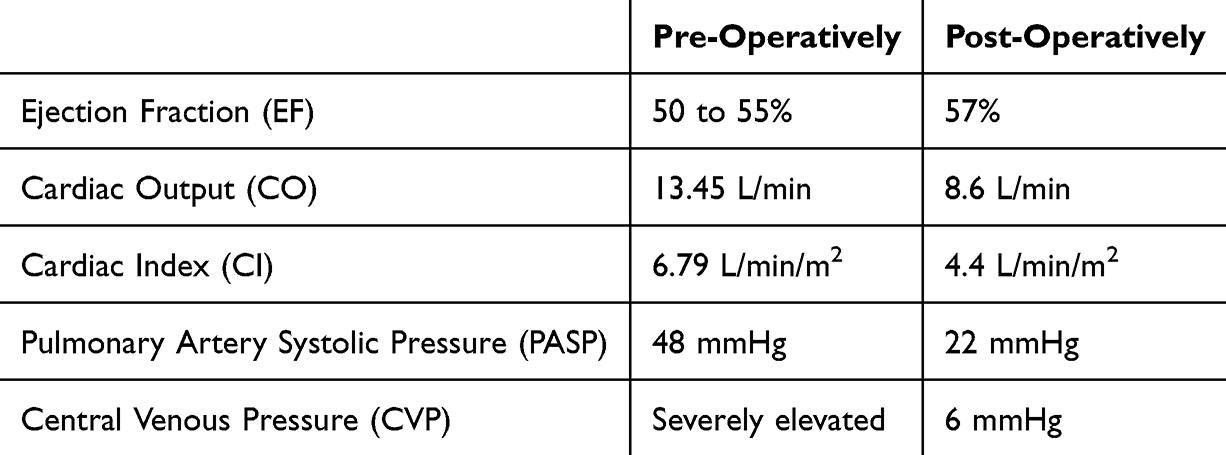 |
Table 1 Echocardiogram Values Pre- and Post-Operatively |
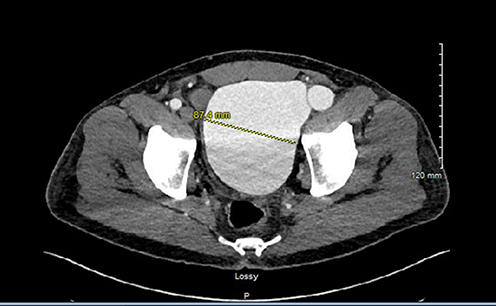 |
Figure 1 Contrast-enhanced computed tomography angiography (CTA) of the pelvis, axial view, soft tissue view, obtained on admission. Shows marked dilation of the left common iliac vein, measuring 8.7 cm in maximum transverse diameter. |
His surgery was planned with pre-operative cardiovascular ICU admission for right heart catheterization and Swan-Ganz placement and close post-operative blood pressure management. A repeat echocardiogram showed similar values to his initial presentation 3 months prior in the emergency department. Induction performed with midazolam, propofol, fentanyl, and rocuronium, then with sevoflurane for maintenance. Patient’s hemodynamics remained stable with no significant changes in BP, CVP or PAP. Mean arterial pressure (MAP) was maintained between 60–80 mmHg with a phenylephrine infusion (0.3–0.6 mcg/kg/min) throughout the entire case. A test clamp by the surgeon induced an immediate increase in systolic BP by 30 mmHg and decrease in HR from 80s to 50s. After stent deployment, the same occurred, which was treated with 0.4 mg of glycopyrrolate, with improvement of BP and HR back to baseline. Apart from the test clamp and the stent deployment, the patient’s hemodynamics stayed within 20% of his baseline throughout the case. Trans-esophageal echocardiogram after stent deployment showed improvement in his hemodynamics (Table 1).
On admission to the ICU, he had palpable bilateral femoral, dorsalis pedis, and posterior tibialis pulses, he was initiated on low intensity heparin drip and remained intubated and sedated during flat bedrest. He was weaned off sedation and extubated the evening after his surgery without complications. His hemodynamic goals were maintained with MAP 60–80 mmHg and SBPs below 140 mmHg by utilizing hydralazine and a nicardipine infusion. A beta blocker was not added due to intermittent heart rate readings in the 40 bpm. Once he was transitioned off titratable infusions to scheduled anti-hypertensives, he was transferred to the surgical floor for the remainder of his recovery. A four-month post-operative follow up CTA of the pelvis showed a reduction in the left iliac vein diameter to 6.2 cm from 8.7 cm (Image 2) and a negative myocardial perfusion stress test (Figure 2).
 |
Figure 2 Contrast-enhanced computed tomography angiography (CTA) of the pelvis, axial view, soft tissue view, obtained at four-month post-operative follow-up after AVF repair. The left common iliac vein now measures 6.2 cm in maximum transverse diameter, 29% reduction from pre-operative figure (Figure 1). |
Discussion
AVFs can be formed through a variety of origins, separated by congenital and acquired causes, with the acquired causes further separated into traumatic, iatrogenic (dialysis access, procedural complications), infections, or idiopathic. Regardless of the cause, they all share a key hemodynamic hallmark. That is a direct arterial-to-venous shunting that increases preload and reduces systemic vascular resistance, predisposing to HOHF. Traumatic AVFs include an added risk of going undiagnosed or untreated and most often result from penetrating injuries, commonly involving the femoral and iliac vessels.5 Chronic high-flow shunts can lead to right-sided volume overload, valvular regurgitation, and pulmonary hypertension.3
There have been several case reports of HOHF due to long-standing AVFs describing sequelae including right-sided volume overload, valvular regurgitation, and pulmonary hypertension, all of which improved following definitive intervention.7–9 Our case is notable for its duration, over a decade post-trauma, and the extreme iliac venous dilation, yet endovascular repair achieved marked hemodynamic improvement without cardiopulmonary compromise, illustrating that even chronic AVFs can show partial reversibility of cardiopulmonary remodeling when corrected. AVFs also pose risks for hemorrhage, as demonstrated in two case reports of fatal exsanguination in patients with chronic renal failure and ulcerated AVFs, exacerbated by inflammation, necrosis, and repeated trauma to the vascular site.9 Other complications of AVFs, described largely in dialysis populations but applicable to high-flow states, include lymphedema, infection, aneurysm, stenosis, steal syndrome, ischemic neuropathy, and thrombosis.10 These complications were potential sequelae in our patient putting him at a daily risk of exsanguination from activities as simple as a Valsalva maneuver or coughing, heightened by him being lost to follow up for a decade.
An AVF increases venous return, risking hyperdynamic circulation with subsequent elevated cardiac output and heart rate. This increase in venous return bypasses the normal low-resistance venous system and directly enters the high-pressure arterial system, which can progressively worsen and lead to HOHF as seen in this patient. The resulting venous congestion raises peripheral venous pressure, causing peripheral edema and renal dysfunction. The increased right ventricular workload can additionally result in right heart failure and tricuspid regurgitation.4
Preoperative preparation should include consideration of invasive monitors, vasoactive medications, and updated studies and labs. For this patient, there was planned pre-operative admission to the cardiovascular ICU to obtain an updated echocardiogram, evaluate his hemodynamics, particularly his pulmonary artery pressures, and more closely monitor his blood pressure. Depending on the different complications arising from AVFs, the invasive monitors chosen may differ. Since this patient presented with severe pulmonary hypertension and an AVF of a major artery, it was crucial to be able to monitor his pulmonary artery pressures and monitor his cardiac function with TEE.
Conclusion
Patients who present with chronic traumatic AVFs after a GSW pose unique challenges, particularly when there has been a prolonged interval between the initial injury and definitive management. The degree of physiologic derangement is often proportional to the duration of the lesion, as sustained high-flow shunting leads to increased venous return, reduced systemic vascular resistance, and a hyperdynamic circulatory state. Over time, this results in progressive cardiac remodeling, including right-sided chamber dilation, functional valvular regurgitation, and HOHF.
Pulmonary hypertension in chronic AVFs is multifactorial, initially driven by increased pulmonary blood flow and shear stress, and later by pulmonary vascular remodeling with rising pulmonary vascular resistance. If left untreated, these changes may ultimately progress to right ventricular dysfunction. In this patient, long-standing shunting led to significant venous dilation and cardiopulmonary compromise, highlighting the cumulative effects of delayed intervention and loss to follow-up. Despite these chronic changes, definitive closure of the AVF resulted in immediate hemodynamic improvement, including reductions in pulmonary artery pressures and cardiac output. This finding supports prior reports that cardiopulmonary changes associated with high-flow states may at least be partially reversible following elimination of the shunt, although the extent of recovery likely depends on the duration and severity of remodeling.
From a perioperative perspective, managing patients with chronic AVFs requires meticulous hemodynamic control to maintain adequate perfusion while avoiding abrupt shifts in preload and afterload after fistula closure. In this case, preoperative optimization, invasive hemodynamic monitoring, and careful intraoperative blood pressure management were critical in preventing further complications. Intervention in chronic traumatic AVFs is typically indicated in patients with symptomatic heart failure, progressive chamber enlargement, pulmonary hypertension, or significant vascular dilation. This case underscores the importance of early recognition, multidisciplinary planning, and individualized anesthetic management. The reversibility of HOHF, even after a decade-long AVF, highlights a key teaching point: timely repair can prevent progressive cardiac remodeling and reduce morbidity associated with chronic high-flow states.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. About nonfatal injury data (WISQARS). 2024. Available from: https://wisqars.cdc.gov/about/nonfatal-injury-data.
2. Centers for Disease Control and Prevention. Firearm mortality. National Center for Health Statistics; 2025. Available from: https://www.cdc.gov/nchs/state-stats/deaths/firearms.html.
3. Chen JK, Johnson PT, Fishman EK. Diagnosis of clinically unsuspected posttraumatic arteriovenous fistulas of the pelvis using CT angiography. Am J Roentgenol. 2007;188(3):W269–5. doi:10.2214/AJR.05.1230
4. Nara T, Yoshikawa D, Saito S, Tanabe Y, Morita T, Goto F. Perioperative management of biventricular failure after closure of a long-standing massive arteriovenous fistula. Can J Anaesth. 2001;48(7):702–706. doi:10.1007/BF03016837
5. Smith RS, Elliott DC. Traumatic arteriovenous fistulas: delayed diagnosis and implications for cardiovascular health. J Trauma Acute Care Surg. 2015;78(5):1045–1052. doi:10.1097/TA.0000000000000601
6. Gibson K, Farber MA, Zelenock GB, Cronenwett JL. Vascular complications of arteriovenous fistulas: long-term outcomes and management strategies. J Vasc Surg. 2009;49(4):945–951. doi:10.1016/j.jvs.2008.12.036
7. He T, He X, Yuan X-M. High-output heart failure secondary to iatrogenic arteriovenous fistula: a case report. World J Cardiol. 2025;17(4):104748. doi:10.4330/wjc.v17.i4.104748
8. Morikawa K, Setoguchi H, Yoshino J, Makizono R, Yokoo T, Takahashi S. Anesthetic management of a patient with aortocaval fistula. J Anesth. 2009;23(1):111–114. doi:10.1007/s00540-008-0711-6
9. Veldhoen RA, Chan W, Mahaffey R, D’Arsigny CL. Traumatic pulmonary hypertension secondary to arteriovenous fistula and remote gunshot wound. Can J Anaesth. 2019;35(2):229.e11–229.e13. doi:10.1016/j.cjca.2018.12.003
10. Volk MC, Honnekeri P, Ghobrial J. High-output heart failure from arteriovenous dialysis access: a structured approach to diagnosis and management. Cleveland Cl J Med. 2025;92(6):362–372. doi:10.3949/ccjm.92a.24114
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.