Back to Journals » International Medical Case Reports Journal » Volume 18
High-Dose Biotin Supplementation Exacerbates Chronic Migraine: A Case Report
Authors Sanosi AA
Received 11 August 2025
Accepted for publication 15 December 2025
Published 20 December 2025 Volume 2025:18 Pages 1657—1661
DOI https://doi.org/10.2147/IMCRJ.S558256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Aiman Abdullah Sanosi
Department of Medicine, University of Jeddah, Jeddah, Saudi Arabia
Correspondence: Aiman Abdullah Sanosi, Department of Medicine, University of Jeddah, Jeddah, Saudi Arabia, Email [email protected]
Abstract: Chronic migraine is a complex neurological disorder that has a significant burden on patient’s lives and socioeconomic outcomes, and it is difficult to manage when patients present with comorbid medication overuse headache. This research describes a case of chronic migraine persisting for 20 years, worsening following high-dose biotin supplementation. A female patient with long-standing and well-controlled classic migraine developed a two-month history of daily severe headaches. The patient experienced a significant exacerbation of headaches after initiating biotin 10,000 mcg once daily. The patient developed daily migraines unresponsive to triptans, significantly affecting her quality of life and increasing multiple emergency visits. This may be due to alteration of mitochondrial energy metabolism, which disrupts the synthesis of neurotransmitters, including serotonin pathways and increased oxidative stress and ultimately results in migraine exacerbation. Discontinuation of biotin led to improvement and return to baseline with rare and mild attacks. High-dose biotin may act as a previously unrecognized trigger for migraine exacerbation. Future studies are required to explore the exact mechanisms of high-dose biotin in triggering migraine exacerbation.
Keywords: headache, biotin, neurological effects, worsening outcomes, life quality
Introduction
Chronic migraine is defined as a headache occurring on 15 or more days per month for more than 3 months, while migraine headache occurs on at least 8 days per month.1 Migraine is a disabling primary headache disorder, often precipitated by known triggers including hormonal changes, stress, sleep irregularities, and dietary components.2 The prevalence of migraine and chronic migraine is approximately 14–15% and 1.4–2.2% of the worldwide population, respectively, and it is found to be higher in women (1.7–4.0%) compared to men (0.6–0.7%).3–5 It tremendously influences the patient’s quality of life and also significantly causes personal and socioeconomic burdens.5
Chronic migraine has frequently evolved from poorly managed episodic migraine pain. Chronic migraine treatments involve therapeutic challenges due to poor treatment response to pain. The optimal treatment strategies focus on modifying risk factors, identifying progression triggers, managing comorbidities, and utilizing acute, prophylactic, and non-pharmacological therapies that involve to prevent migraine attacks.6,7 Chronic migraine patients who did not receive appropriate medication were at risk of medication overuse and non-pharmacological strategies associated with headache.8 Medication overuse is considered a critical factor that triggers the progression of migraine into chronic form. Sometimes medications lead to adverse events, including weight loss or gain, sweating, fatigue, nightmares, and gastrointestinal upset.8 Recently, nutritional approaches have emerged as promising strategies for managing migraines.9 For instance, Vitamin D is a nutritional supplement that has potential benefits in managing pain and treating migraine.9 A recent systematic review revealed that Vitamin B significantly reduced the frequency, duration, and severity of migraine.10 In addition, vitamin B6, B12, and folic acid are also helpful in reducing the severity of migraine.11 Supplementation with other nutrients, like omega-3 fatty acids, riboflavin, alpha lipoic acid, probiotics, magnesium, and coenzyme Q10, can also have beneficial effects on the management of migraine attacks.12 Several other novel treatment strategies, including cannabis-based modalities, hormonal and metabolic interventions, targeting the trigeminovascular system, which may prove to be an effective treatment for migraine.13 However, the use of supplements is rarely considered a migraine trigger.
Biotin (vitamin B7), a water-soluble B-complex vitamin, is increasingly used in the metabolism of macronutrients and at high doses for cosmetic benefits. In addition, biotin administration may be beneficial for various neurological disorders, such as multiple sclerosis.14 The dosage of biotin used for nutritional (5000–10000 mcg) and medicinal purposes (5–20 mg) is significantly different and increasingly linked to interference with assays and neurological defects.15 However, high-dose biotin supplementation may alter vascular reactivity, neuronal excitability, or inflammatory mediators and potentially exacerbate migraine severity. While generally regarded as safe, its neurological effects, especially in migraine-prone individuals, are underexplored. This case report illustrates a potential link between high doses of biotin and worsening of chronic migraine, as no previous case reports or studies have linked biotin to migraine exacerbation.
Case Description
A female patient with a long history of chronic classic migraine presented with a two-month history of daily severe headaches. Her prior migraine pattern consisted of infrequent attacks (~once every 2 months), with moderate throbbing pain rated 7/10, right-sided, and associated with visual aura, nausea, vomiting, photophobia, and phonophobia. These symptoms were consistently responsive to sumatriptan.
Patient was well controlled for over 10 years on amitriptyline 50 mg nightly and topiramate 50 mg twice daily (Table 1). Prior attempts to taper these medications led to increased frequency of attacks, so she continued this regimen. Her known migraine triggers included sleep disturbances and chocolate, both of which were meticulously avoided.
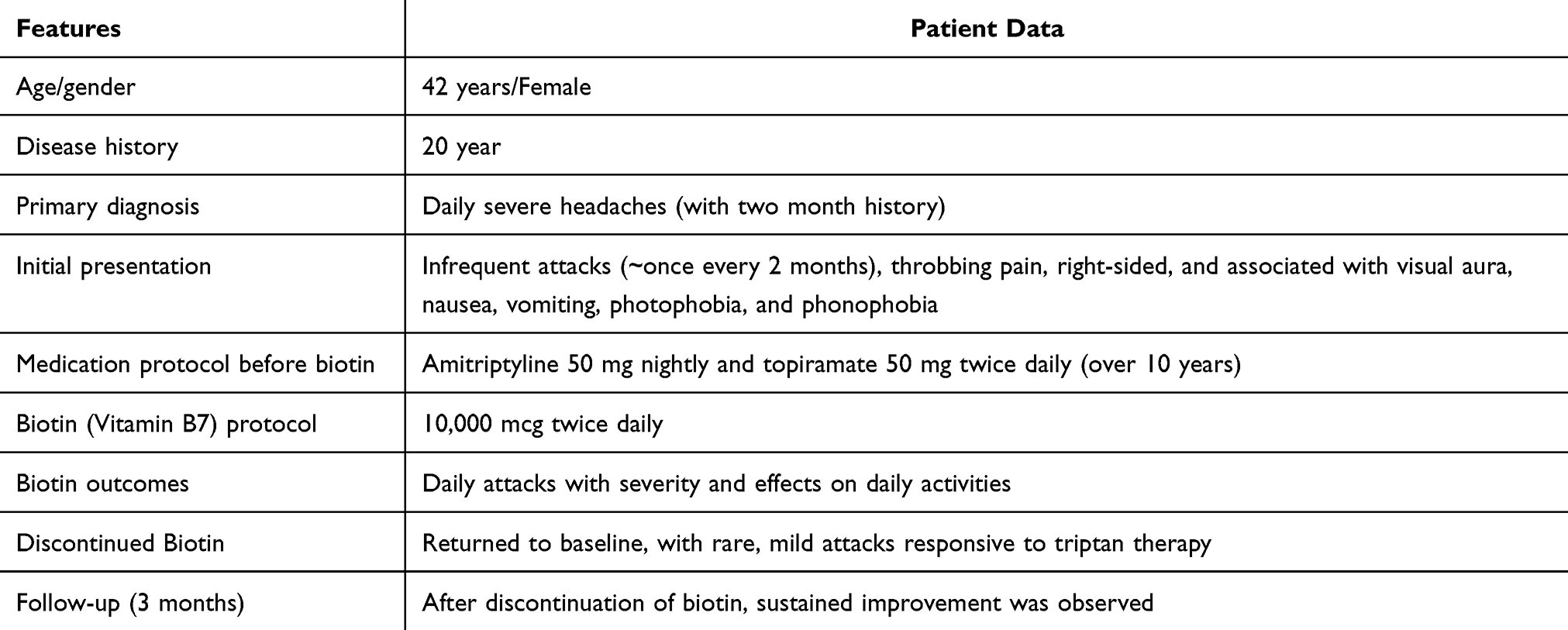 |
Table 1 Clinical and Treatment Summary of a Patient with Chronic Migraine |
Two months before symptom escalation, she began taking high-dose biotin (10,000 mcg) once daily for 3 months as a nutritional supplement, a dosage substantially higher than typical non-prescription formulations, and it is common in over-counter sales. After taking the supplement, a progressive increase was observed in migraine attack frequency and intensity during the first week (daily attacks), with episodes of baseline pattern to more frequent and severe headaches. Meanwhile, confounding factors, such as sleep pattern, menstrual timing, caffeine intake, stress level, and use of other sedative medications, were also evaluated, and no significant changes were reported during the use of biotin. Overall, the headache pattern worsened dramatically, and she experienced daily attacks rated 9/10 in severity, interfering with daily activities and resulting in multiple emergency room (ER) visits. The headaches no longer responded to sumatriptan.
A detailed review of her lifestyle revealed no changes in diet, sleep, work, or medication except for the addition of a new biotin supplement. Additionally, no new stressors, infections, or environmental exposures were identified. The patient’s neurological examination was normal. The temporal correlation raised suspicion for biotin-induced worsening. Thus, biotin was discontinued and there was no change in prophylactic medication. Within one week, the frequency and severity of headaches began to improve. After three weeks, she has returned to her baseline, with rare, mild attacks. She did not resume biotin, and follow-up over the next three months showed sustained improvement.
Discussion
This is the first known case describing a temporal and reversible association between high-dose biotin supplementation and migraine exacerbation, as a literature search from different databases indicated no published studies linking biotin with chronic migraine exacerbation. Due to a high-dose biotin supplement, frequent migraine attacks occurred, and upon discontinuation, improvement in migraine was observed. The patient’s stable headache control for over a decade, absence of new lifestyle triggers, and marked improvement after biotin cessation suggest a potential causal relationship.
Chronic migraine is the most disabling condition of migraine, resulting in reduced quality of life and higher impairment in family functions.16 It is a disorder of neuronal excitability and sensory processing, involving mechanisms such as cortical spreading depression, neurotransmitter imbalance, and neurovascular dysregulation.17 Nutrients and supplements can modulate these pathways; for instance, riboflavin, magnesium, Vitamin D, Vitamin B12, and coenzyme Q10 have shown prophylactic and therapeutic effects.12,18,19 In contrast, the role of biotin (vitamin B7) in migraine pathophysiology has not been investigated in experimental and randomized controlled clinical studies. Biotin is a water-soluble B-complex vitamin that acts as a coenzyme for carboxylase enzymes involved in fatty acid synthesis, amino acid catabolism, and gluconeogenesis.20 It is generally considered safe, even at supraphysiologic doses, emerging data suggest that high-dose biotin can interfere with diagnostic assays21 and may exert broader physiological effects.22
In our clinical case study, a female patient showed worsening of migraine symptoms after overdosing on biotin. Potential mechanisms for biotin-induced migraine worsening in this patient (eg, neuronal hyperexcitability, metabolic shifts, immunological or neurovascular modulation).
Although speculative, potential mechanisms include interfering with neurotransmitter regulation or mitochondrial metabolism, thereby affecting brain energy production and potentially lowering the threshold for cortical spreading depression, and the electrophysiological correlate of migraine aura.12,17 Biotin’s involvement in gluconeogenesis and fatty acid metabolism might alter cerebral energy homeostasis in susceptible individuals.12,20 High-dose biotin has been studied in progressive multiple sclerosis for potential remyelinating effects, suggesting CNS-level activity.14 Interaction with other B-vitamins or competition at absorption sites (eg, with pantothenic acid) could create imbalances indirectly affecting neural function.23 Moreover, it also had adverse interference with certain laboratory assays, including immunoassays that use biotin-streptavidin binding, which can result in misleading outcomes in tests, like thyroid function test.24,25 Meanwhile, this type of interference is primarily a diagnostic concern, while in the case of migraine, it can indirectly affect migraine pathogenesis.
Over-the-counter supplement use is often underreported as a contributor to symptom exacerbation.26 This case underscores the importance of a detailed medication and supplement history in patients with sudden changes in migraine pattern. Interestingly, population-based studies describe new-onset or worsening headaches in users of biotin supplements.27,28 While such data lack scientific rigor, they echo this patient’s experience and warrant further investigation to elucidate the exact mechanism of worsening migraine.
Conclusion
This case suggests a possible link between high-dose biotin and worsening of migraine symptoms. The patient had stable migraines for years, then developed daily severe headaches shortly after starting biotin, with improvement after stopping it. This pattern makes biotin a likely contributor, but not a confirmed cause. It is important to distinguish between an observed association and proven causation. Other factors could have played a role, even if none were identified. It is recommended that clinicians should inquire about the use of supplements in chronic migraine cases. Studies are required to reveal the exact mechanism of worsening migraines using high-dose biotin.
Ethics Approval
Ethical approval was not required for the publication of this case report.
Informed Consent Patient Statement
The patient signed the written informed consent, agreed to the publication of the medical case and understands that this report is intended for scientific and educational purposes.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Arnold M. Headache classification committee of the international headache society (IHS) the international classification of headache disorders. Cephalalgia. 2018;38(1):1–211.
2. Zobdeh F, Eremenko II, Akan MA, et al. The epigenetics of migraine. Inter J Molecular Sci. 2023;24(11):9127. doi:10.3390/ijms24119127
3. Steiner TJ, Stovner LJ. Global epidemiology of migraine and its implications for public health and health policy. Nat Rev Neurol. 2023;19(2):109–117. doi:10.1038/s41582-022-00763-1
4. Buse DC, Manack AN, Fanning KM, et al. Chronic migraine prevalence, disability, and sociodemographic factors: results from the American migraine prevalence and prevention study. Headache. 2012;52(10):1456–1470. doi:10.1111/j.1526-4610.2012.02223.x
5. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache. 2018;58(4):496–505. doi:10.1111/head.13281
6. Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55:103–122. doi:10.1111/head.12505_2
7. Kristoffersen ES, Lundqvist C. Medication-overuse headache: a review. J Pain Res. 2014;367–378. doi:10.2147/JPR.S46071
8. Lipton RB, Munjal S, Buse DC, Fanning KM, Bennett A, Reed ML. Predicting inadequate response to acute migraine medication: results from the A merican migraine prevalence and prevention (AMPP) study. Headache. 2016;56(10):1635–1648. doi:10.1111/head.12941
9. Hu C, Fan Y, Wu S, Zou Y, Qu X. Vitamin D supplementation for the treatment of migraine: a meta-analysis of randomized controlled studies. Ame J Emerg Med. 2021;50:784–788. doi:10.1016/j.ajem.2021.07.062
10. Chen Y-S, Lee H-F, Tsai C-H, et al. Effect of Vitamin B2 supplementation on migraine prophylaxis: a systematic review and meta-analysis. Nutrit Neurosci. 2022;25(9):1801–1812. doi:10.1080/1028415X.2021.1904542
11. Shaik MM, Gan SH. Vitamin supplementation as possible prophylactic treatment against migraine with aura and menstrual migraine. BioMed Res Inter. 2015;2015:469529. doi:10.1155/2015/469529
12. Hajhashemy Z, Golpour-Hamedani S, Eshaghian N, Sadeghi O, Khorvash F, Askari G. Practical supplements for prevention and management of migraine attacks: a narrative review. Front Nutrit. 2024;11:1433390. doi:10.3389/fnut.2024.1433390
13. Pellesi L, Do TP, Hougaard A. Pharmacological management of migraine: current strategies and future directions. Expert Opinion Pharmacotherapy. 2024;25(6):673–683. doi:10.1080/14656566.2024.2349791
14. Tourbah A, Lebrun-Frenay C, Edan G, et al. MD1003 (high-dose biotin) for the treatment of progressive multiple sclerosis: a randomised, double-blind, placebo-controlled study. Multiple Sclerosis J. 2016;22(13):1719–1731. doi:10.1177/1352458516667568
15. Mock DM. Biotin: from nutrition to therapeutics. J Nutrit. 2017;147(8):1487–1492. doi:10.3945/jn.116.238956
16. Dresler T, Caratozzolo S, Guldolf K, et al. Understanding the nature of psychiatric comorbidity in migraine: a systematic review focused on interactions and treatment implications. J Headache Pain. 2019;20(1):51. doi:10.1186/s10194-019-0988-x
17. Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. 2018;17(2):174–182. doi:10.1016/S1474-4422(17)30435-0
18. Fila M, Chojnacki C, Chojnacki J, Blasiak J. Nutrients to improve mitochondrial function to reduce brain energy deficit and oxidative stress in migraine. Nutrients. 2021;13(12):4433. doi:10.3390/nu13124433
19. Nattagh-Eshtivani E, Sani MA, Dahri M, et al. The role of nutrients in the pathogenesis and treatment of migraine headaches. Biomed Pharmacotherapy. 2018;102:317–325. doi:10.1016/j.biopha.2018.03.059
20. Ross AC, Caballero B, Cousins RJ, Tucker KL. Modern Nutrition in Health and Disease. Jones & Bartlett Learning; 2020.
21. Colon PJ, Greene DN. Biotin interference in clinical immunoassays. J Appl Laboratory Med. 2018;2(6):941–951. doi:10.1373/jalm.2017.024257
22. Said HM. Biotin: biochemical, physiological and clinical aspects. Water Soluble Vitamins. 2011;1–19.
23. Calderón‐Ospina CA, Nava‐Mesa MO. B Vitamins in the nervous system: current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci Therapeutics. 2020;26(1):5–13. doi:10.1111/cns.13207
24. Ardabilygazir A, Afshariyamchlou S, Mir D, Sachmechi I. Effect of high-dose biotin on thyroid function tests: case report and literature review. Cureus. 2018;10(6):e2845. doi:10.7759/cureus.2845
25. Gifford JL, Sadrzadeh SMH, Naugler C. Biotin interference: underrecognized patient safety risk in laboratory testing. Canadian Family Physician. 2018;64(5):370.
26. Birnbaum G, Stulc J. High dose biotin as treatment for progressive multiple sclerosis. Multiple Sclerosis Related Disord. 2017;18:141–143. doi:10.1016/j.msard.2017.09.030
27. Chiu HY, Tsai PS, Lee CC, Liu YT, Huang HC, Chen PY. The association between use of dietary supplements and headache or migraine complaints. Headache. 2014;54(2):355–363. doi:10.1111/head.12180
28. Drugs.com Biotin side effects. https://www.drugs.com/sfx/biotin-side-effects.html.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.