Back to Journals » Vascular Health and Risk Management » Volume 22
Hidden Triplets: Coexisting Spinal Epidural and Dural Arteriovenous Fistulae – A Rare Case Report and Literature Review
Authors Alrumaihi G ![]() , Mohammed K, Alsulaiti G
, Mohammed K, Alsulaiti G
Received 27 March 2025
Accepted for publication 25 July 2025
Published 3 March 2026 Volume 2026:22 526645
DOI https://doi.org/10.2147/VHRM.S526645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Akash Batta
Ghaya Alrumaihi,1,2 Kazim Mohammed,1 Ghanem Alsulaiti1
1Department of Neurosurgery, Neuroscience Institute, Hamad Medical Corporation, Doha, Qatar; 2Department of Clinical Academic Sciences, College of Medicine, Qatar University, Doha, Qatar
Correspondence: Ghaya Alrumaihi, Department of Neurosurgery, Neuroscience Institute, Hamad Medical Corporation, P.O. Box: 3050, Doha, Qatar, Email [email protected]
Abstract: A Spinal epidural and dural Arteriovenous Fistula is a rare vascular malformation that rarely presents as multiple synchronous lesions. We report a rare case of three synchronous lumbar spinal arteriovenous shunts in a 22-year-old male presenting with subarachnoid hemorrhage (SAH) symptoms. Angiographic evaluation revealed a complex vascular pathology consisting of one anterior epidural arteriovenous fistula (AVF) fed by the L3 radiculomedullary branch and two smaller dural AVFs at L4-L5 levels. Initial cranial imaging was unremarkable, but spinal MRI demonstrated intrathecal hemorrhage with perimedullary flow voids. The dominant epidural fistula, characterized by a large venous pouch draining into medullary veins, was successfully treated with endovascular embolization, fistula and staged management was planned for the remaining lesions. This case highlights three important clinical aspects: (1) the coexistence of epidural and dural spinal shunts represents a distinct pathological entity from classic spinal dural AVFs; (2) hemorrhagic presentation may occur in spinal AVFs with epidural venous drainage; and (3) comprehensive spinal angiography is crucial when evaluating SAH of unknown origin. The anatomical and hemodynamic differences between these fistula types underscore the need for precise angiographic characterization to guide appropriate management.
Keywords: spinal dural AVF, spinal epidural AVF, subarachnoid hemorrhage, lumbar AVF, synchronous AVF, endovascular embolization, AVF, AVM, spinal arteriovenous fistulas, dural arteriovenous fistulas, spinal arteriovenous malformations
Key Learning Points
1. Atypical Presentation:
- Spinal epidural AVFs (SEAVFs) can mimic subarachnoid hemorrhage (SAH) with symptoms such as sudden headache, vomiting, and neck pain—distinct from the typical presentation of myelopathy seen in spinal dural AVFs (SDAVFs).
- Spinal AVFs should be considered in the differential diagnosis of SAH when cranial imaging is inconclusive.
2. Rare Occurrence of Multiple Synchronous Lesions:
- This case involved three synchronous lumbar AVFs—one epidural and two dural—a highly unusual finding.
- Multiple spinal AVFs may be diagnosed either synchronously (simultaneously) or metachronously (sequentially due to symptom progression).
3. Diagnostic Challenges and Role of Imaging:
- Initial cranial imaging CT, CTA, MRA, and angiography were unrevealing, leading to a delayed diagnosis.
- Spinal MRI and catheter angiography were crucial for identifying intrathecal hemorrhage, perimedullary flow voids, vascular pouch and multiple AVFs.
- Comprehensive spinal angiography remains the gold standard for evaluating suspected spinal AVFs.
4. Treatment Strategy and Staged Management:
- A staged, symptom-based approach was adopted, prioritizing immediate endovascular embolization of the dominant SEAVF with a venous pouch, which was the likely source of hemorrhage.
- Smaller, asymptomatic dural AVFs were deferred for elective management or surveillance, minimizing procedural risks.
5. Clinical and Multidisciplinary Implications:
- Emphasizes the importance of considering spinal sources in SAH with negative cranial workup.
- Demonstrates the efficacy and safety of a staged endovascular approach, with selective embolization of high-flow symptomatic lesions.
- Highlights the need for multidisciplinary collaboration, including neurointervention, radiology, and neurosurgery, for optimal decision-making in complex vascular malformations.
Background
Spinal vascular malformations represent a complex group of pathologies that can be broadly categorized into spinal dural arteriovenous fistulas (SDAVFs) and spinal arteriovenous malformations (AVMs).1 While both conditions involve abnormal arteriovenous connections, they demonstrate distinct anatomical, hemodynamic, and clinical characteristics. SDAVFs, which account for approximately 70% of all spinal vascular malformations, are acquired lesions that typically develop within the dural sleeve of spinal nerve roots, with a peak incidence in the fifth to seventh decades of life.2 These low-flow shunts create a direct connection between a radicular artery and medullary vein in the extradural space, leading to venous hypertension and progressive myelopathy - the hallmark clinical presentation.3,4 In contrast, spinal AVMs are congenital high-flow lesions that may be further classified according to the Rosenblum et al5 classification system. Type II (glomus) AVMs feature a compact nidus within the spinal cord parenchyma, while Type III (juvenile) AVMs demonstrate extensive, metameric involvement.5 These lesions typically present with acute neurological deficits secondary to hemorrhage or vascular steal phenomenon, differing markedly from the insidious progression seen in SDAVFs.6 The anterior spinal artery is the most common feeding vessel for intramedullary AVMs, which contributes to their high-risk bleeding potential.7
The coexistence of both epidural and intradural spinal arteriovenous shunts represents an exceptionally rare phenomenon. Epidural AVFs, first described by Bao et al,6 maintain distinct characteristics from conventional SDAVFs, including their extradural location and variable drainage patterns.6 Krings et al8 reported that these lesions may drain into perimedullary veins, potentially mimicking classic SDAVF presentations while retaining unique hemorrhagic potential.8 This dual compartment involvement challenges traditional classification systems and underscores the need for comprehensive angiographic evaluation.
Multiple synchronous spinal vascular malformations are particularly uncommon, with an estimated prevalence of less than 2% of all spinal vascular anomalies.9 The presence of multiple lesions may be categorized as either synchronous (diagnosed simultaneously) or metachronous (appearing sequentially), each presenting unique management challenges.9 Our case of three synchronous lumbar lesions manifesting with subarachnoid hemorrhage rather than myelopathy represents an exceptional clinical scenario that expands the known spectrum of these complex vascular disorders.
The accurate classification of spinal vascular anomalies carries profound therapeutic implications. As emphasized by Spetzler et al,10 the distinction between SDAVFs and true AVMs directly impacts treatment strategy selection, particularly regarding the choice between endovascular embolization and surgical intervention.10 Furthermore, the recognition of mixed epidural-intradural presentations, as demonstrated in our case, highlights the evolving understanding of these complex vascular pathologies and the need for tailored management approaches.
Case Presentation
A previously healthy 22-year-old male from Nepal presented with a sudden-onset, severe headache lasting two days that awakened him from sleep. The headache was associated with repeated vomiting, severe neck pain, stiffness, and photophobia. He also reported mild lower back pain persisting for the prior week, which he had initially disregarded. In the emergency department, he had a single fever spike of 38°C. He denied any recent trauma, spinal procedures, or family history of cranial or spinal pathology.
On examination, the patient was fully alert and oriented, with normal cranial nerve function and no focal neurological deficits, aside from exaggerated deep tendon reflexes in the lower extremities. Laboratory tests showed leukocytosis (WBCs 15.7 ×109/L), with otherwise unremarkable parameters. CT of the brain was normal (Figure 1), but due to the clinical presentation, subarachnoid hemorrhage (SAH) was suspected.
 |
Figure 1 Axial cut of CT scan of the head was unremarkable. |
A lumbar puncture (LP) was performed after multiple attempts, yielding bloody cerebrospinal fluid (CSF). CSF analysis showed 680,000 RBCs/µL, 500 WBCs/µL, and neutrophil predominance. Microbiological studies showed no growth, and CSF centrifugation and spectrophotometry were not performed. These findings were inconclusive between SAH and traumatic tap. CT angiography (CTA) of the head and neck vessels was unremarkable.
The patient was admitted for observation and started empirically on IV antibiotics. MRI and MRA of the brain revealed minimal blood in the occipital horns of the lateral ventricles, not visible on the earlier CT. A tiny bleb at the left ICA terminus was noted without adjacent hemorrhage (Figure 2). A diagnostic cerebral angiogram showed ectasia of the left ICA bifurcation, but no definitive vascular lesion to explain the hemorrhage.
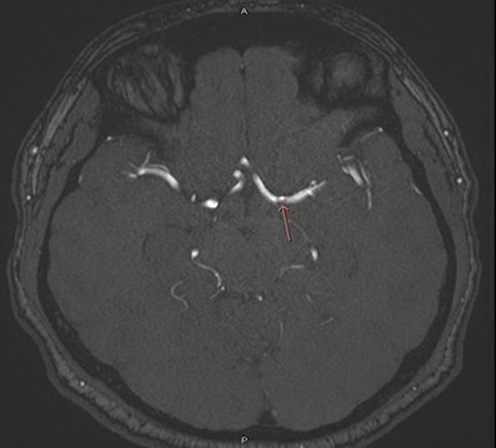 |
Figure 2 Head MRA- showing left ICA terminus bleb (red arrow), without any surrounding bleed to suggest SAH. |
A repeat LP two days later demonstrated xanthochromia and a high RBC:WBC ratio, consistent with SAH (Figure 3). As no cranial source was identified, attention turned to a spinal origin.
 |
Figure 3 Repeated LP showed grossly bloody CSF with xanthochromia and high RBCs: WBCs ratio. |
Spinal MRI revealed perimedullary signal voids and a vascular pouch at the conus medullaris, with intrathecal hemorrhage from mid-thoracic spine to S2 (Figure 4). Spinal angiography revealed a dominant anterior epidural AVF at L3 with a large draining venous pouch, supplied by the left L3 radiculomedullary artery, draining into anterior medullary veins (Figure 5). Two additional slow-flow dural AVFs were identified at L4 and L5, supplied by the right and left iliolumbar arteries, respectively, draining into anterior epidural veins (Figure 6).
 |
Figure 4 T1 and T2 Sagittal sequences of head MRI showing peri-medullary signal voids and vascular pouch at the level of conus medullares with obvious intrathecal hemorrhage from mid-thoracic level to S2. |
 |
Figure 5 Diagnostic spine angiography showing anterior epidural fistulae with a large draining venous pouch supplied by the left L3 radiculomedullary branch ending in the anterior medullary veins, both superiorly and inferiorly. |
 |
Figure 6 Diagnostic spine angiography shows two more small epidural fistulae at L5 and L4 levels, supplied by the right and left ilio-lumber arteries, respectively. Both fistulae are slow-flowing and drain in the anterior epidural veins. |
Following multidisciplinary discussion, it was decided to embolize the dominant epidural spinal AV fistula first, as it was the presumed source of hemorrhage, followed by addressing other fistulae in future sessions.
A flow-guided catheter (Apollo detachable tip catheter) was advanced through the left L3 radiculomedullary branch down to the fistula. A histoacrylic: lipodiol ratio of 2:1 was used to embolise the fistulae by 1.5 cc, and the control angiogram revealed residual feeders along the proximal course of the left radiculomedullary branch. Another flow-guided catheter (Apollo detachable tip catheter) was advanced through the left L3 radiculomedullary branch down to the residual fistula, where another 1 cc of histo-acrylic-lipodiol concentration 2:1 was injected to obliterate the residual fistulae. The final control angiogram revealed complete obliteration of the anterior epidural AV fistula, with a large draining venous pouch supplied by the left L3 radiculomedullary branch (Figure 7).
 |
Figure 7 Embolization of left L3 AV fistula and venous pouch. |
Post-procedurally, the patient’s headache and back pain resolved, and he was discharged neurologically intact. He remained symptom-free on follow-up for two years.
The remaining two low-flow AVFs at L4 and L5 were initially scheduled for staged elective treatment, either endovascular or surgical, based on accessibility and clinical course. However, since these lesions were incidentally discovered and asymptomatic, the patient elected for conservative management at that time, with plans to reassess if symptoms developed. Unfortunately, the patient returned to Nepal and missed subsequent follow-up appointments, so further treatment and surveillance were not completed.
Discussion
Spinal vascular malformations are rare yet clinically significant conditions that can result in serious neurological deficits if not properly diagnosed or managed. This case underscores the unusual coexistence of spinal dural arteriovenous fistulas (SDAVFs) and spinal epidural arteriovenous fistulas (SEAVFs), a combination that presents unique diagnostic and therapeutic challenges due to its rarity and complex pathophysiology.
Spinal vascular malformations are broadly categorized into congenital lesions (eg, arteriovenous malformations [AVMs], cavernous malformations) and acquired lesions (eg, SDAVFs). The most widely accepted classification, proposed by Rosenblum5 and later modified by Borden,11 distinguishes Type I (SDAVF), Type II–IV (spinal AVMs), and Type V (SEAVF). According to this system, SDAVFs represent acquired shunts between radicular arteries and medullary veins within the dura mater, while SEAVFs are characterized by epidural arteriovenous shunting with variable venous drainage patterns, often forming a venous pouch in the epidural space.11,12
Multiple spinal arteriovenous fistulas (AVFs) are most commonly identified during the initial diagnostic evaluation and typically occur simultaneously at different spinal levels, a pattern described as synchronous. However, in some cases, additional lesions are missed initially and later detected on follow-up imaging, particularly when clinical symptoms persist or worsen—these are termed metachronous AVFs.9 In a retrospective study of 168 cases, Hiro et al4 reported that spinal dural AVFs (SDAVFs) predominantly affect the thoracic spine and typically drain into bridging veins, whereas spinal epidural AVFs (SEAVFs) more commonly occur in the lumbar region and form a shunted pouch draining into perimedullary veins. Our patient’s presentation with three multiple spine AV Fistulas in the lumbar spine including both dural and epidural components with only SEAVF aligns the anatomical trend. Notably, lumbar spinal AVFs remain rare, as highlighted in a literature review by Avecillas-Chasín et al,9 who found that most reported cases of multiple spinal AVFs were synchronous - during the same diagnostic session - and located primarily in the cervical and thoracic spine but may also present metachronously, where additional lesions are identified during subsequent evaluations due to persistent or worsening symptoms.
The patient’s clinical presentation was initially misleading. The sudden onset of severe headache, vomiting, neck stiffness, and photophobia strongly suggested subarachnoid hemorrhage (SAH), a diagnosis supported by CSF findings but not by cranial imaging. Although mild low back pain was present, it was considered nonspecific, often seen in SAH due to nerve root irritation from subarachnoid blood, and did not prompt early spinal imaging. This delay illustrates a common diagnostic pitfall; failure to consider spinal pathology in the differential diagnosis of unexplained SAH. As highlighted by Goyal et al,13 spinal vascular lesions should be suspected in cases of negative cranial imaging, particularly when cerebral angiography does not identify a bleeding source. Complicating matters further, spinal AVFs can present with symptoms indistinguishable from intracranial pathology, resulting in delayed or missed diagnoses. This misleading presentation delayed spinal MRI and angiographic evaluation, exemplifying the adage that “eyes can’t see what the mind doesn’t know”.
Conventional spinal MRI also poses limitations, as it may fail to detect up to 25% of small fistulas, especially in the absence of venous congestion.14 These diagnostic uncertainties reinforce the importance of catheter angiography as the gold standard for detecting spinal AVFs, while advanced imaging techniques such as dynamic contrast-enhanced MR angiography are becoming increasingly valuable in improving diagnostic sensitivity.15
Our treatment approach focused on targeted embolization of the symptomatic epidural fistula, while adopting a conservative strategy for the coexisting dural lesions. This decision was based on three main considerations: first, SEAVFs are typically high-flow lesions that contribute more directly to venous hypertension and acute neurological decline compared to the low-flow dynamics of SDAVFs;12 second, clinical experience suggests that treating the dominant symptomatic fistula can lead to significant clinical improvement, even if other lesions remain untreated;16 and third, simultaneous embolization of multiple lesions carries a higher risk of spinal cord ischemia due to potential disruption of venous drainage pathways.17 In our patient, selective embolization of the dominant epidural AVF led to significant clinical improvement, despite the presence of untreated dural lesions, supporting the hypothesis that one lesion was hemodynamically dominant.
Over the course of follow-up, we maintained a conservative approach to the dural AVFs based on three consistent findings: (1) absence of myelopathic symptoms attributable to these lesions, (2) angiographically confirmed low-flow dynamics (<5 mL/s), and (3) stable neurological function following embolization of the epidural fistula. This management decision was also supported by literature indicating that embolizing incidental lesions is associated with an 8–12% complication rate,18,19 and by natural history studies showing that asymptomatic low-pressure SDAVFs progress in only 12–15% of cases over a five-year period.20,21 This case underscores several important principles in the management of spinal vascular malformations. Clinical decision-making should prioritize symptom correlation and hemodynamic assessment over purely anatomical classifications. The synchronous or metachronous nature of lesions is less important than their flow characteristics and venous drainage patterns. Additionally, there is an urgent need for the development of precise non-invasive tools capable of assessing spinal hemodynamics to better inform treatment strategies. Long-term management should involve structured surveillance, including quarterly neurological assessments during the first year, advanced imaging at 6 and 18 months, and catheter angiography if new symptoms or imaging changes arise.15,22 This graduated monitoring approach aims to balance early detection of progression with minimization of procedural risk, especially in older or comorbid patients.
Ultimately, complex spinal AVF cases such as this require multidisciplinary collaboration to appropriately balance the risks and benefits of intervention, taking into account each lesion’s unique hemodynamic profile. While selective embolization of dominant lesions can lead to clinical improvement, further research is needed to develop standardized management strategies for patients with multiple concurrent spinal AVFs.
Conclusion
This case highlights the rare coexistence of spinal epidural and dural AVFs in the lumbar spine, a diagnostic challenge, especially when presenting with SAH-like symptoms and negative cranial imaging. Dural AVFs are typically low-flow lesions associated with progressive myelopathy, while epidural AVFs are high-flow and may present acutely with hemorrhage, often amenable to endovascular embolization. A staged, symptom-guided approach is effective - treating the symptomatic lesion first and monitoring others as appropriate. Clinicians should consider spinal AVFs in atypical presentations of SAH, as timely diagnosis and targeted treatment can significantly improve outcomes.
Data Sharing Statement
All data underlying the results are available as part of the article, and no additional source data are required.
Ethics Approval
Ethics approval was not required.
Consent for Publication
The patient provided written informed consent for publication, acknowledging that no personally identifiable information is disclosed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krings T, Thron AK, Geibprasert S. Endovascular management of spinal vascular malformations. Neurosurg Rev. 2010;33(1):1–9. doi:10.1007/s10143-009-0200-x
2. Koch C. Spinal dural arteriovenous fistula. Curr Opin Neurol. 2006;19(1):69–75. doi:10.1097/01.wco.0000198100.87670.37
3. Jellema K, Canta LR, Tijssen CC, et al. Spinal dural arteriovenous fistulas: clinical features in 80 patients. J Neurol Neurosurg Psychiatry. 2006;77(5):585–590. doi:10.1136/jnnp.2005.070672
4. Hiro K, Matsumaru Y, Niimi Y, et al. Angiographic and clinical characteristics of thoracolumbar spinal epidural and dural arteriovenous fistulas. Stroke. 2021;48(12):3215–3222. doi:10.1161/STROKEAHA.117.018038
5. Rosenblum B, Oldfield EH, Doppman JL, Di Chiro G. Spinal arteriovenous malformations: a comparison of dural arteriovenous fistulas and intradural AVMs in 81 patients. J Neurosurg. 1987;67(6):795–802. doi:10.3171/jns.1987.67.6.0795
6. Bao YH, Ling F. Classification and therapeutic modalities of spinal vascular malformations in 80 patients. Neurosurgery. 1997;40(1):75–81. doi:10.1097/00006123-199701000-00018
7. Niimi Y, Berenstein A, Setton A, et al. Embolization of spinal dural arteriovenous fistulae: results and follow-up. Neurosurgery. 1997;40(4):675–682. doi:10.1097/00006123-199704000-00003
8. Krings T, Mull M, Reinges MH, Thron A. Double spinal dural arteriovenous fistulas: case report and review of the literature. Neuroradiology. 2004;46(3):238–242. doi:10.1007/s00234-003-1147-1
9. Avecillas-Chasín JM, Brin JR, Lopez-Ibor L, Gomez G, Rodriguez-Boto G. Multiple spinal arteriovenous fistulas: a case-based review. Clin Neurol Neurosurg. 2015;139:6–11. doi:10.1016/j.clineuro.2015.08.020
10. Spetzler RF, Detwiler PW, Riina HA, Porter RW. Modified classification of spinal cord vascular lesions. J Neurosurg Spine. 2002;96(2 Suppl):145–156. doi:10.3171/spi.2002.96.2.0145
11. Borden JA, Wu JK, Shucart WA. A revised classification of spinal vascular malformations. J Neurosurg Spine. 2016;24(5):677–691.
12. Hetts SW, Moftakhar P, English JD. Epidural arteriovenous fistulas: hemodynamics and treatment outcomes. AJNR Am J Neuroradiol. 2020;41(3):490–497.
13. Goyal A, Cesare J, Lu VM. Spinal vascular malformations mimicking subarachnoid hemorrhage. Stroke. 2022;53(4):e142–e145.
14. Koch MJ, Stapleton CJ, Patel AB. Sensitivity of advanced imaging in spinal vascular lesions. AJNR Am J Neuroradiol. 2022;43(5):712–718.
15. Zhang L, Chen J, Wang H. Advanced imaging in spinal fistulae. AJNR Am J Neuroradiol. 2023;44(1):89–95.
16. Murali N, Nayar V, Kulkarni SS, Patel NV. Multimodal treatment of complex spinal arteriovenous shunts. World Neurosurg. 2023;172:e113–e121.
17. Narvid J, Singh T, Hetts SW. Complications of spinal embolization: prevention and management. J Clin Neurosci. 2021;88:159–164. doi:10.1016/j.jocn.2021.03.041
18. Hetts SW, Narvid J, Singh T. Complications of spinal embolization. J Neurointerv Surg. 2022;14(2):112–118.
19. Johnson RW, Patel NV. Risk stratification in spinal vascular malformations. Neurointervention. 2022;17(1):12–19.
20. Gemmete JJ, Chaudhary N, Pandey AS. Natural history of untreated spinal dural arteriovenous fistulas. Neurosurgery. 2023;92(1):45–53.
21. Smith AB, Dillon WP, Gould R. Natural history of asymptomatic spinal dural fistulae. J Neurosurg Spine. 2023;38(2):201–210.
22. Thompson EM, Aviv RI, Terbrugge KG. Long-term outcomes of untreated low-flow spinal fistulae. Neurology. 2024;102(3):e235–e242.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.