Back to Journals » Risk Management and Healthcare Policy » Volume 14
Hepatitis B Vaccination Status and Associated Factors Among Healthcare Professionals Working in Health Centers at Akaki Kality Subcity of Addis Ababa, Ethiopia: A Cross-Sectional Study
Authors Ayana Hordofa M, Hussen Hassan A
Received 2 February 2021
Accepted for publication 1 April 2021
Published 15 April 2021 Volume 2021:14 Pages 1575—1582
DOI https://doi.org/10.2147/RMHP.S287579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Mulatu Ayana Hordofa,1 Abdulhafiz Hussen Hassan2
1Department of Public Health, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia; 2City Administration of Addis Ababa Health Bureau, Addis Ababa, Ethiopia
Correspondence: Mulatu Ayana Hordofa P.O. Box.19 Tel +251911549352
Fax +25111235227
Email [email protected]
Background: People at high risk for hepatitis B virus include healthcare workers in contact with blood and human secretions. Hepatitis B virus is unique compared to other sexually transmitted infections because a highly efficacious vaccine exists. However, there have been few studies conducted around the vaccination status of hospital healthcare workers in Ethiopia. Little is known about vaccination penetration among healthcare professionals working in health centers in Ethiopia.
Objective: To assess hepatitis B vaccination status and associated factors among healthcare professionals working in health centers of Akaki Kality, Addis Ababa, Ethiopia.
Methods: A facility-based cross-sectional study was conducted. Using simple random sampling, 528 healthcare workers were selected. Data were collected using a pre-tested, structured self-administered questionnaire. Data were entered into Epi-data and analyzed using SPSS version 20. Multivariable binary logistic regression analysis was used to identify the significant associations. Adjusted odds ratios were computed to measure the strength of association, with statistical significance considered at p< 0.05.
Results: Among 505 respondents, only 244 (48%) had ever received a hepatitis B vaccine. Monthly income, religion, age, working unit and educational level were found to be statistically associated with vaccinated status.
Conclusion: This study showed that the percentage of healthcare professionals who had received a hepatitis B vaccination was very low. This is a serious public health concern and a challenge for a country with high prevalence of hepatitis B infection. There is a need to promote hepatitis B screening and vaccination among healthcare professionals. The government must play its part by increasing healthcare budgets and prioritize hepatitis B prevention by establishing a national awareness campaign, and making screening and vaccination services available at all public health centers.
Keywords: hepatitis B, vaccination, healthcare professional, heath center, Addis Ababa
Introduction
Hepatitis B is a potentially life-threatening blood-born liver infection caused by the hepatitis B virus (HBV).1 According to the most recent estimates from the Global Burden of Disease study and the World Health Organization (WHO), viral hepatitis is responsible for approximately 1.34 million deaths, annually. The number of HBV-positive individuals was the highest in the African region, accounting for 68% of the global burden.2,3 Working in healthcare has long been recognized as a risk factor for HBV exposure. Hepatitis B, C and HIV (human immunodeficiency virus) infections are the most serious occupational health hazards faced by healthcare workers worldwide. A WHO report estimates that 40% of hepatitis B infection is as a result of occupational exposure, and it has been estimated that 14.4% of hospital workers are infected with hepatitis B virus at any given time.2,4 The incidence of this infection among healthcare workers has been estimated to be 2–4 times the level in the general population.3 A study conducted across two hospitals in Ethiopia on a sample of 267 healthcare workers found the overall prevalence of HBV infection to be 51.3%5
Unlike other sexually transmitted infections (STIs), hepatitis B virus is vaccine preventable. As part of occupational safety measures, all healthcare workers are required to be vaccinated against HBV. According to a report from the US, the overall vaccination coverage against HBV among healthcare personnel was 69.5% and 63.4%, for one and three HBV vaccine doses, respectively.6 Unfortunately, HBV vaccination coverage amongst healthcare workers in most low- and middle-income countries is only 18–39% compared to 67–79% in high-income countries.2,3,5–12 Specific examples include penetration rates of 38.8% in tertiary care centers in North India,13 61.2% in Gauteng province of North Africa,14 and 33.6% in Benin City in Nigeria.15
A study conducted in the public hospitals of Addis Ababa found the majority of the study subjects (72.4%) to have been exposed to blood and blood products. Reports of the prevalence of hepatitis B in Ethiopia vary.5,7–12 Despite a high prevalence of the infection, exposure to blood and blood products, and a high prevalence of needle stick and other injuries from sharp objects, the vaccination status of healthcare workers varies from 3.6% to 30.3% in different regions of Ethiopia.9,16–19 There are various reported factors associated with vaccination status including socio-demographic factors like seniority, gender, work experience, the working unit,6,20,21 level of education, marital status, and age.17,21 Other factors reported are vaccine unavailability and cost,17,22 work pressures, changes of location, lack of knowledge,13,15,20 being careful, and taking standard precautions.13–16,18,23 Factors such as negligence, a low level of perceived susceptibility, fear of side effects, forgetfulness, attitude,20 lack of time, and lack of motivation have also been reported as impacting the penetration of HBV vaccination.13,19,20,23 Though there are few studies conducted at hospitals, as far as the authors search is concerned, there are no studies conducted on hepatitis B vaccination status of healthcare professionals working at health centers in Ethiopia.
Materials and Methods
Study Area, Design and Period
A facility-based cross-sectional study was conducted in the health centers of Akaki Kality, subcity of Addis Ababa, the capital city of Ethiopia, from May 15 to June 15, 2020. At time of study, the subcity region contained 10 health centers.
Study Population
The study population was healthcare professionals in roles such as health officers, nurses, midwives, and laboratory technicians. This sample population was selected due to their frequent contact with patients’ blood and bodily fluids, and because they are considered to be at a higher risk of acquiring HBV.
Sample Size
The study has got two specific objectives: Accordingly, the sample size was calculated for the two objectives and the larger sample size was taken.
For the first specific objective, it was calculated by using the single population proportion formula, assuming proportion (p) of staff vaccinated (based on Black Lion hospital in 2015, where the proportion was 51%), p=51%, a confidence level of confidence =95% (Z α/2 = 1.96), a significance of 5% and margin of error (d) of 5%.
Using single population proportion formula, the minimum sample size required (n) for the first objective was calculated to be 384. Assuming a non-response rate of 10%, it became 423 participants.
The required sample size for second objective was determined using double population proportion using Epi-info version 7.2.2.6 stat calc software as presented below. Factors that have significant association with corresponding odds ratio in previous studies are selected to calculate sample taking the following assumptions based on previous studies conducted in Shashemane. Confidence level 95%, Power of the study 80%, associated variable “cost of the vaccine”. %exposed with outcome, %unexposed with the outcome. Adjusted odds ratio (AOR) 1.7 and a 10% nonresponse rate, the sample size became 528. And therefore sample size for the second objective was taken as it gave optimum sample size.
Sampling Procedure
For each health center, an allocation of personnel was calculated that was proportionate to the total size of the center. Potential participants in each health facility were selected by using a computer-generated random number method and a list of all the health workers who were at risk of contact with patients’ blood and bodily fluid at the center.
Data Collection Tools and Procedures
Data were collected using self-administered, structured questionnaires. The questionnaire tool was adapted from similar studies conducted on similar study populations. Data were collected by four diploma-holding healthcare professionals. Identified personnel were approached in the workplace setting.
Description of Variables
The dependent variable was hepatitis B vaccination status.
The independent variables were socio-demographic variables, not feeling at risk, fear of side effects, current unit of work, behavioral factors, fear of needles, negligence or forgetfulness, work load, health service factors and availability of information, availability of the vaccine, and cost.
Data Quality Assurance
The questionnaire was first prepared in English and then translated into the local language, Amharic. To confirm that the translation had been consistently carried out, the questionnaire was then translated back from Amharic to English by another language expert. The questionnaire was pilot-tested on 5% of the sample, and any necessary corrections to the questionnaire were made accordingly. Training was given for data collectors and supervisors. Completed questionnaires were checked by the supervisors on a daily basis for completeness.
Data Processing and Data Analysis
Data entry was undertaken using Epi-data version 3.1 and analysis was conducted using SPSS 20 for Windows. Data were checked for completeness, and any incomplete questionnaire was excluded from the analysis. Following data entry, data cleaning was conducted to avoid any missing values, outliers, and other inconsistencies before analysis. Analysis was undertaken using commands like frequency, find, and list. The data was explored to visualize the general features using descriptive statistics including frequency, and mean and standard deviation. A multivariable binary logistic regression analysis was used to identify the factors that were significantly associated with the dependent variable. Adjusted odds ratios were computed to determine the strength of association. Statistical significance was considered at a level of p<0.05.
Ethical Considerations
Ethical approval was obtained from the institutional review board of Rift Valley University Department of Public Health. Following this permission was sought and successfully obtained from Addis Ababa public health research and emergency management directorate Bureau, and from the Akaki Kality subcity health office. Further, permission to conduct the research was requested and obtained from the administrative body of Akaki Kality subcity Health Office. An information sheet was prepared and given to all study participants to obtain informed verbal consent. All participants were informed of the aim and purpose of the study and their participation was voluntary. Verbal informed consent was approved by the ethics committee, and that this study was conducted in accordance with the Declaration of Helsinki. The name of the participant was not asked, instead a code number was used to ensure anonymity and confidentiality throughout the study.
Results
Sociodemographic Characteristics
A total of 505 respondents completed the questionnaire, making the response rate 96%. Of this sample, 226 (44.8%) were nurses. The mean age of respondents was 29 years and 292 (57.2%) were female. Regarding educational status, 343 (67.9%) were holders of a first degree. 226 (44.8%) of the respondents were Orthodox Christians and 283 (56%) were single. The mean monthly income for the respondents was 6665.56 Ethiopian Birr. Among the respondents, 416 (82.4%) had less than 9 years’ experience, and the mean duration of service was 6.37 years (Table 1).
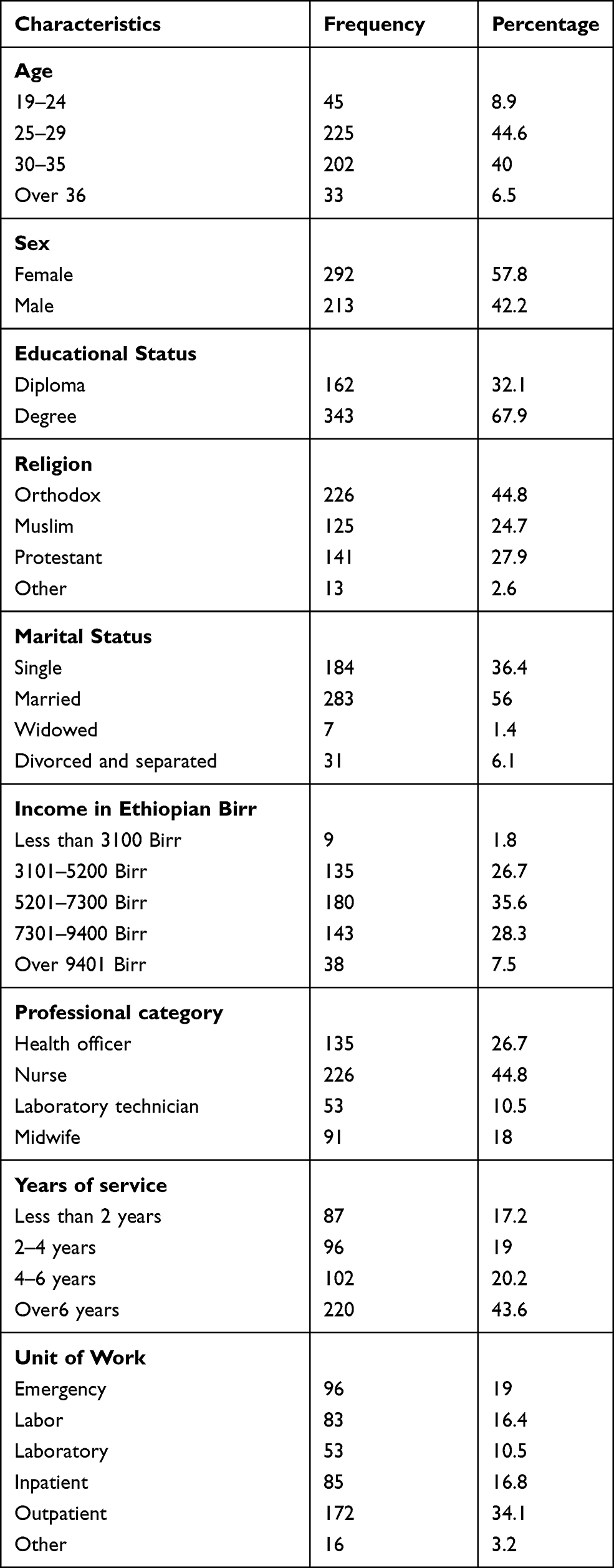 |
Table 1 Socio-Demographic Characteristics of Healthcare Workers in Akaki Kality. Addis Ababa, Ethiopia. 2020 |
Hepatitis B Exposure of Study Participants
Of the sample, 404 (80%) said that their usual work involves the identification of patients, of which 166 (41%) did this by sending patient samples for laboratory diagnosis. Concerning the use of infection prevention measures when caring for hepatitis B patients, 503 (99.6%) participants responded that they do use these. Among these, 500 (99%) said that they dispose of sharp materials properly, whereas among respondents who reported not to use infection prevention measures (50%) said that this was because they do not have access to the protective equipment. When asked whether they deliver the same standard of care for hepatitis B patients, 339 (67.1%) responded they did (Tables 2 and 3).
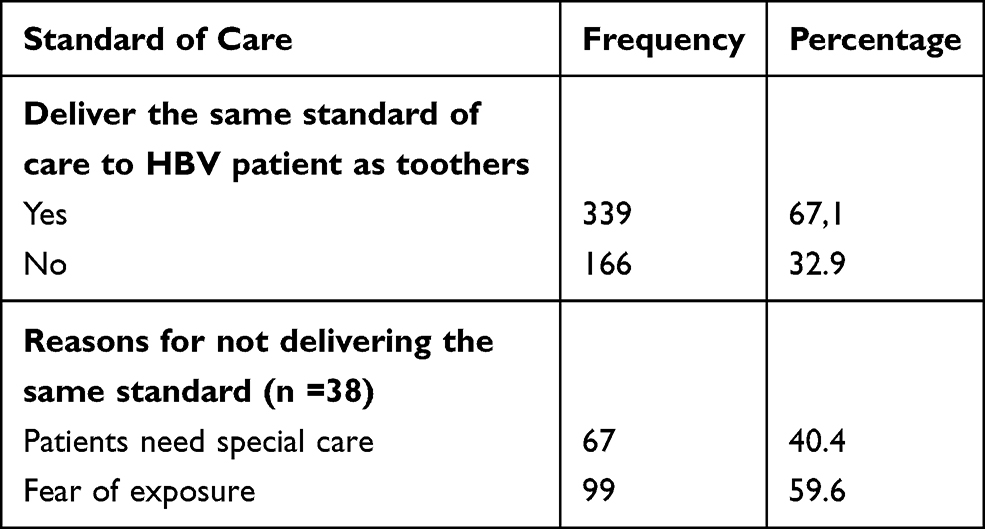 |
Table 2 Standard of Care Delivery Status Among Healthcare Workers in Akaki Kality, Addis Ababa, Ethiopia, 2020 |
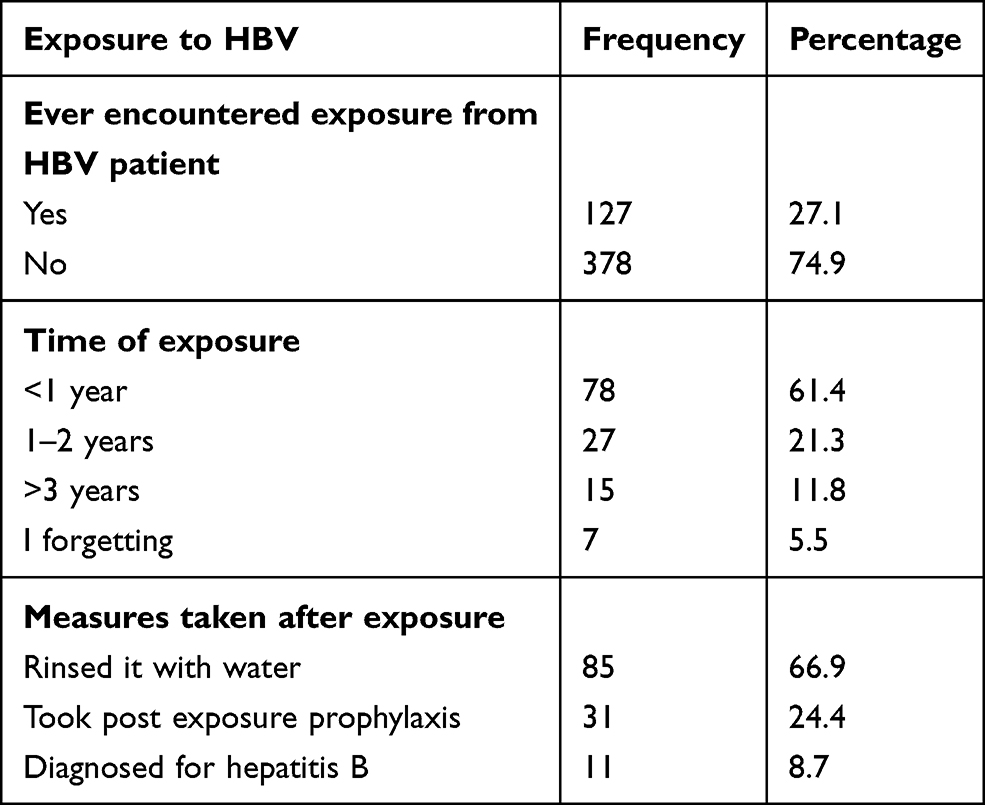 |
Table 3 HBV Exposure Status of Healthcare Workers in Akaki Kality, Addis Ababa, Ethiopia. 2020 |
Hepatitis B Screening and Vaccine Utilization Status of Study Participants
Of the respondents, 359 (71.1%) reported that they had been tested for HBV. Of those tested, 162 (45.1%) had not received a test within the last 1–2 years. For those who had never been tested, the most commonly cited reason (n = 75; 51.7%) was cost (Table 4). Regarding hepatitis B vaccination status, only 244 (48%) respondents said that they had ever received a hepatitis B vaccine, whereas 261 (52%) responded they have never received the hepatitis B vaccine. Of those who had received the hepatitis B vaccine, 22 (9%) had received only one dose, whereas 107 (43.9%) had received two doses, 115 (47.1%) had received three doses and 2 (0.8%) had received three doses and a booster dose (Figure 1).
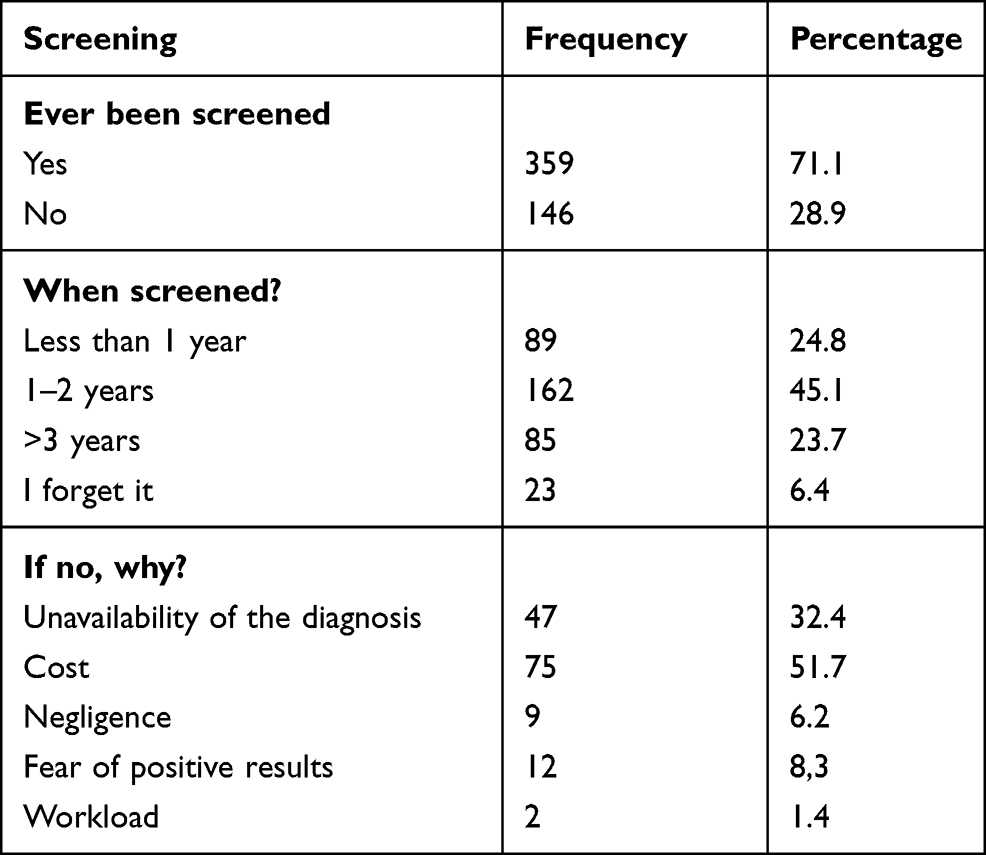 |
Table 4 Testing for HBV Infection Among Healthcare Workers in Akaki Kality, Addis Ababa, Ethiopia, 2020 |
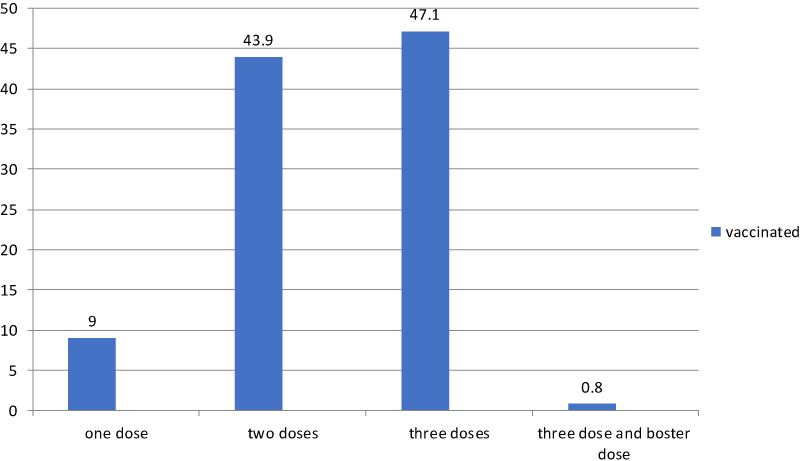 |
Figure 1 Number of hepatitis B vaccine doses taken by healthcare workers, Akaki Kality, Addis Ababa, Ethiopia. 2020. |
In total, 117 participants (48%) had completed the vaccination with an appropriate schedule. Of those who had not completed the schedule, 30 (23.6%) said that this was because they forgot to attend subsequent appointments to complete the schedule, 57 (44.9%) they said the subsequent vaccination doses were too costly,23 (18.1%) said that subsequent dosed were unavailable, 14 (5.7%) had missed doses, and 3 (1.2%) said they were still awaiting subsequent doses to complete the schedule (see Tables 4 and 5).
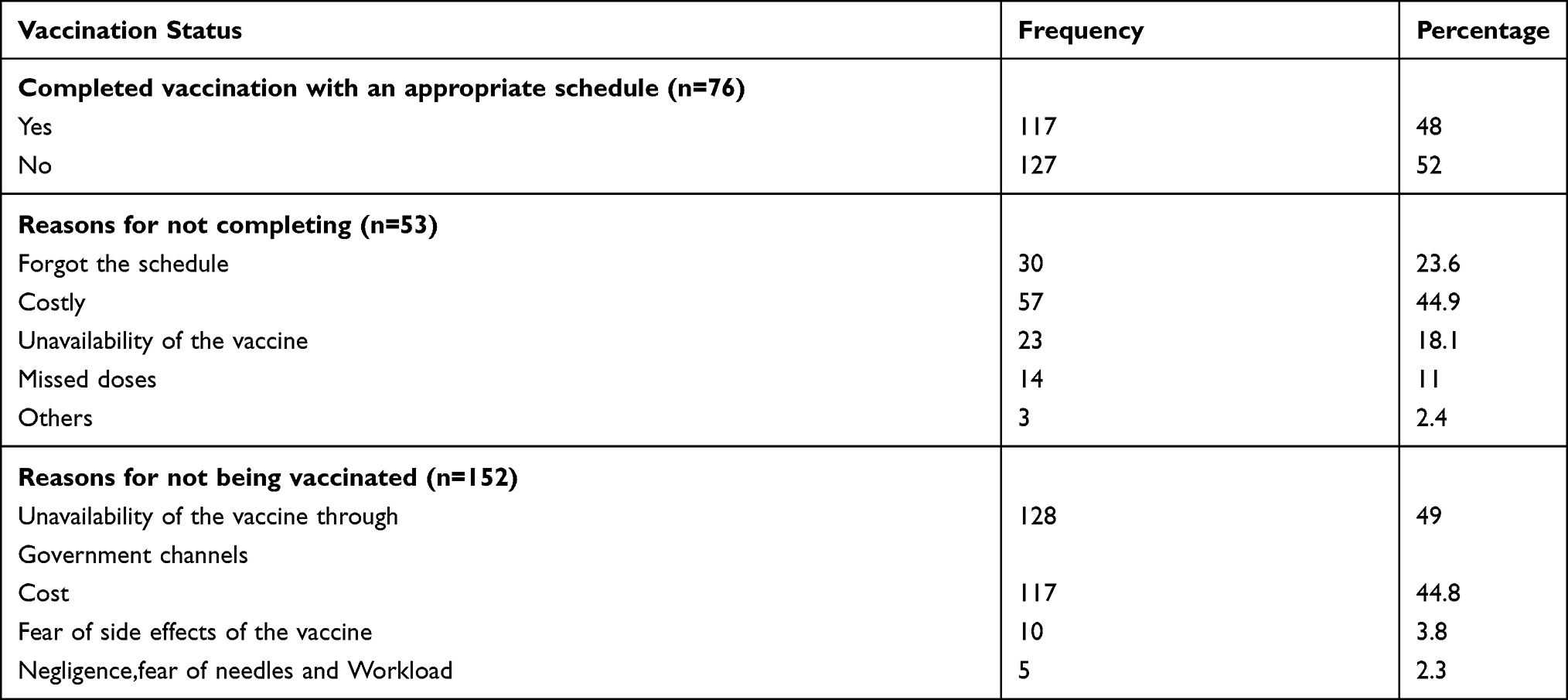 |
Table 5 Hepatitis B Vaccination Status of Healthcare Workers at Akaki Kality, Addis Ababa, Ethiopia. 2020 |
Factors Associated with HBV Vaccination
Analysis of participant responses identified that monthly income, working unit, educational level, age, and religion were found to be significantly associated with the likelihood of having received HBV vaccination (see Table 6).
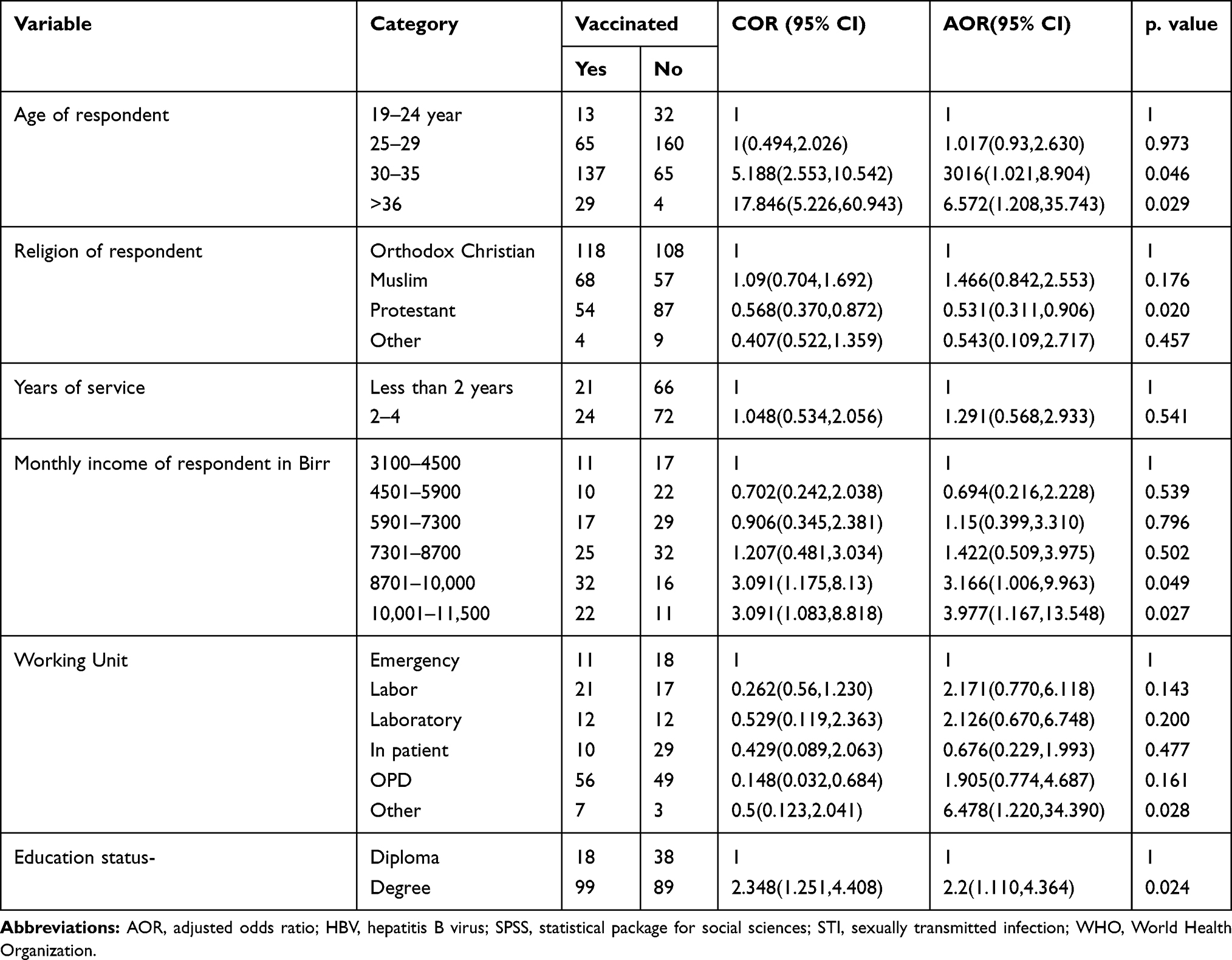 |
Table 6 Factors Associated with Vaccination for Hepatitis B Virus Among Healthcare Professionals in Akaki Kality, Addis Ababa, Ethiopia. 2020 |
Discussion
This study showed that the level of reported hepatitis B vaccination among healthcare workers in health centers in Addis Ababa was similar to that reported in study conducted on a similar sample in Nigeria. Having said that, the vaccination rate reported in the present study is higher than that of studies conducted in a tertiary care center in north India,13 as well as health centers in Gauteng province of North Africa,14 Benin City in Nigeria,15 Shashemane,19 Hawasa,18 and Bahir Dar.16 These studies were conducted over a five-year period, and as such there may have been improvements in the vaccination rate of the populations studied due to the widespread global efforts made to raise awareness of healthcare professionals in order to increase the uptake of Hepatitis B testing and vaccination in recent years.
The multivariate analysis shows that respondents in the age group of 30–35 years and over 35 years were more likely to have received hepatitis B vaccination than those aged 19–24 years. This is consistent with previous studies17,21 and maybe due to older healthcare workers having a greater fear of infection exposure. And also due to their lack of experience or more up-to-date on job training the younger may not take the vaccination. Income was also found to be a predictor of vaccination status, with higher incomes being associated with a higher likelihood of having been vaccinated. This may be because of the cost of the vaccination itself, as the hepatitis B vaccine is not provided for free in government health centers.
The working unit was another factor significantly associated with the likelihood of having received a hepatitis B vaccination. It may be that some units are at a lower infection risk than others, and therefore are more reluctant to take the vaccine. Those with bachelors’ degrees were more likely to have been vaccinated compared staff with diplomas, echoing the findings reported by previous studies.17,21 This may be due to an intrinsic connection between educational level and salary, with holders of bachelors’ degrees being paid more compared to staff with diplomas. Alternatively, or additionally, it may be more directly down to the level of education attainment, with diploma holders being less aware of the seriousness of HBV infection. Finally, followers of the Protestant religion were less likely to have been vaccinated compared to those of the Orthodox religion. In contradiction to previously published studies, the factors of gender, work experience,6,20,21 marital status,17,21 unavailability, and cost of the vaccine17,22 were not found to be significantly associated with vaccine uptake in the present study.
The strength of the current study is that the study was conducted among healthcare professionals working in health center, whereas many previously published studies have focused on hospital workers. However, due to the cross-sectional study design, recall and temporal bias may have been introduced into the sample. Similarly, the study did not include the hepatitis tests.
Conclusion
In a study of 505 randomly selected healthcare workers from health centers across the Akaki Kality subcity of the Addis Ababa, Ethiopia, almost half the respondents reported that they had received at least a partial dosing schedule of the hepatitis B vaccine. However, of these, only half reported to have received three complete doses of hepatitis B vaccine. Vaccination penetration was significantly associated with the age, religion, income, and working unit of the respondent. Efforts must be made to vaccinate healthcare workers against HBV free of cost or at lower cost as this is a serious public health concern and challenge for healthcare workers in health centers throughout low- and middle-income countries.
Acknowledgments
Our gratitude goes to all study participants and data collectors for their genuine participation and cooperation. We would also like to extend our thanks to the administrative bodies of AkakiKalitysubcity Health Office and health centers for their total cooperation. We would like to thank Rift Valley University for their technical support in conducting the study. We would like to extend our gratitude to Rebecca Dewey (from University of Nottingham, UK) for thorough English language edition and correction of the final manuscript.
Disclosure
The authors declare that they have no competing interests in relation to this work.
References
1. Churchill Livingstone. Churchill’s Illustrated Medical Dictionary. Churchill Livingstone; 1989.
2. World Health Organization. Global Hepatitis Report 2017. World Health Organization; 2017.
3. Akyıldız M, Ahıskalı E, Zeybel M, Yurdaydın C. Regional epidemiology, burden, and management of hepatitis B virus in the Middle East. Clin Liver Dis. 2019;14(6):212. doi:10.1002/cld.887
4. Auta A, Adewuyi EO, Tor-Anyiin A, et al. Health-care workers’ occupational exposures to body fluids in 21 countries in Africa: systematic review and meta-analysis. Bull World Health Organ. 2017;95(12):831. doi:10.2471/BLT.17.195735
5. Kedir Yimer Seid MD. Serological and Molecular Characterization of Hepatitis B, C and D Viruses Infections Among Health Professionals in Ras Desta and Tikuranbessa Hospitals [unpublished thesis work]. Addis Ababa, Ethiopia; 2005.
6. Byrd KK, Lu P-J, Murphy TV. Hepatitis B vaccination coverage among health-care personnel in the United States. Public Health Rep. 2013;128(6):498–509. doi:10.1177/003335491312800609
7. Akalu GT, Woldemariam A, Shewaye A, Geleta D, Demise A, Debele M. Burden of hepatitis-B infections and risk factors among healthcare workers in resource limited setting, Addis Ababa, Ethiopia. EC Microbiol. 2016;4(4):722–731.
8. Dabsu R, Ejeta E. Seroepidemiology of hepatitis B and C virus infections among pregnant women attending antenatal clinic in selected health facilities in East Wollega Zone, West Oromia, Ethiopia. Biomed Res Int. 2018;2018:2018. doi:10.1155/2018/4792584
9. Desalegn Z, Selassie SG. Prevalence of hepatitis B surface antigen (HBsAg) among health professionals in public hospitals in Addis Ababa, Ethiopia. Ethiop J Health Dev. 2013;27(1).
10. Frempong MT, Ntiamoah P, Annani-Akollor ME, et al. Hepatitis B and C infections in HIV-1 and non-HIV infected pregnant women in the Brong-Ahafo Region, Ghana. PLoS One. 2019;14(7):e0219922. doi:10.1371/journal.pone.0219922
11. Gebremariam AA, Tsegaye AT, Shiferaw YF, Reta MM, Getaneh A. Seroprevalence of hepatitis B virus and associated factors among health professionals in University of Gondar Hospital, Northwest Ethiopia. Adv Prev Med. 2019;2019:2019. doi:10.1155/2019/7136763
12. Yizengaw E, Getahun T, Geta M, et al. Sero-prevalence of hepatitis B virus infection and associated factors among health care workers and medical waste handlers in primary hospitals of North-West Ethiopia. BMC Res Notes. 2018;11(1):437. doi:10.1186/s13104-018-3538-8
13. Pathak R, Chaudhary C, Pathania D, Ahluwalia SK, Mishra PK, Kahlon AS. Hepatitis B vaccine: coverage and factors relating to its acceptance among health care workers of a tertiary care center in North India. Int J Med Sci Public Health. 2013;3(1):1. doi:10.4103/2230-8598.109324
14. Africa PN. Knowledge, Attitudes and Practices of Health Care Workers Regarding Hepatitis B Vaccination, in the Ekurhuleni Metro, Gauteng Province [unpublished thesis work]. University of Limpopo (Medunsa Campus); 2010.
15. Obi A, Ofili A. Hepatitis B vaccination uptake among doctors in Benin City, Edo State, Nigeria. J Community Med Health Educ. 2013;3(7):246.
16. Abeje G, Azage M. Hepatitis B vaccine knowledge and vaccination status among health care workers of Bahir Dar City administration, Northwest Ethiopia: a Cross Sectional Study. BMC Infect Dis. 2015;15(1):30. doi:10.1186/s12879-015-0756-8
17. Biset Ayalew M, AdugnaHorsa B. Hepatitis B vaccination status among health care workers in a tertiary hospital in Ethiopia. Hepat Res Treat. 2017;2017:2017. doi:10.1155/2017/6470658
18. Bedaso A, Duko B, Fedlu R. Knowledge on HBV vaccine and vaccination status among health care workers of Hawassa University Comprehensive Specialized Hospital, Hawassa, Southern Ethiopia: a Cross Sectional Study. BMC Res Notes. 2018;11(1):912. doi:10.1186/s13104-018-4023-0
19. Abebaw T-A, Aderaw Z, Gebremichael B. Hepatitis B virus vaccination status and associated factors among health care workers in Shashemene Zonal Town, Shashemene, Ethiopia: a Cross Sectional Study. BMC Res Notes. 2017;10(1):1–9. doi:10.1186/s13104-017-2582-0
20. Bante A, Debalkie M, Getie A, et al. Hepatitis B vaccination and its associated factors among health care workers working in WolayitaSodo Hospitals, Southern Ethiopia: a Cross-Sectional Study. J Infect Dis Immun. 2019;11(1):1–10. doi:10.5897/JIDI2019.0184
21. Ouédraogo H, Kouanda S, Tiendrébeogo S, et al. Statut vaccinal contre le virus de l’hépatite B et facteursassociésparmi le personnel de santé au Burkina Faso. Med Sante Trop. 2013;23(1):72–77.
22. Yuan Q, Wang F, Zheng H, et al. Hepatitis B vaccination coverage among health care workers in China. PLoS One. 2019;14(5):e0216598. doi:10.1371/journal.pone.0216598
23. Akibu M, Nurgi S, Tadese M, Tsega WD. Attitude and vaccination status of healthcare workers against hepatitis B infection in a teaching hospital, Ethiopia. Scientifica. 2018;2018:1–8. doi:10.1155/2018/6705305
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.