Back to Journals » International Medical Case Reports Journal » Volume 18
Henna-Induced Intravascular Hemolysis in a Glucose-6-Phosphate Dehydrogenase-Deficient Ghanaian Female Child with Full Defect
Authors Dike NO ![]() , Blankson ES, Segnitome S
, Blankson ES, Segnitome S ![]()
Received 23 April 2025
Accepted for publication 5 August 2025
Published 14 August 2025 Volume 2025:18 Pages 1035—1040
DOI https://doi.org/10.2147/IMCRJ.S534544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tanvi Dhere
Nkechi Oluwakemi Dike,1 Emmanuel S Blankson,2 Sarah Segnitome3
1School of Medical Sciences, University of Cape Coast, Cape Coast, Ghana; 2Emergency Department, Upper West Regional Hospital, Wa, Ghana; 3Emergency Department, Tamale West Hospital, Tamale, Ghana
Correspondence: Nkechi Oluwakemi Dike, School of Medical Sciences, University of Cape Coast, Cape Coast, Ghana, Tel +233-240999102, Email [email protected]; [email protected]
Abstract: Glucose-6-phosphate dehydrogenase (G6PD) deficiency, a sex-linked chromosomal disorder, is the most common enzymopathy in humans. This enzyme, which protects red blood cells, when deficient, predisposes individuals to hemolysis under oxidative stress. Several chemicals and drugs have been commonly known to cause hemolysis in G6PD deficiency. However, an uncommon substance, henna, a plant-based dye used in Africa and Asia, has also been described to trigger hemolysis in G6PD-deficient individuals. It shares similarities in the structural ring and properties with other well-described G6PD hemolytic agents. We present a rare case of severe intravascular hemolysis following topical henna application in an 8-year-old girl with G6PD deficiency, successfully managed at the Upper West Regional Hospital in Ghana.
Keywords: henna, hemolysis, G6PD deficiency, Ghana
Introduction
Glucose-6-phosphate dehydrogenase (G6PD) is a crucial enzyme responsible for protecting human red blood cells (RBCs) from oxidative stress. G6PD deficiency is the most common human enzymopathy, with recent evidence suggesting it affects nearly 330 million people worldwide and that the highest prevalence rates are found among countries in Sub-Saharan Africa.1,2 Based on 2025 systematic review for G6PD epidemiology among 10 malaria endemic countries in Sub-Saharan Africa, studies from Ghana had a prevalence of G6PD deficiency ranging between 10.6 to 20.1%.3
It’s important to note that although G6PD deficiency is inherited through the X chromosome and usually causes more serious clinical presentation in males and homozygous females, heterozygous females with only one affected gene also show, though usually milder clinical features of G69D deficiency due to the unequal inactivation of the G6PD gene on their X chromosomes.4
The G6PD enzyme plays a vital role in the pentose phosphate pathway by facilitating the production of reduced nicotinamide adenine dinucleotide phosphate (NADPH). NADPH, in conjunction with glutathione reductase, maintains adequate levels of reduced glutathione within the red blood cell. Reduced glutathione acts as a critical antioxidant, shielding RBCs from oxidative damage. In individuals with G6PD deficiency, the absence of sufficient NADPH leads to impaired protection against oxidative stress, resulting in red blood cell destruction and subsequent hemolysis.4,5
Patients with G6PD deficiency are highly susceptible to life-threatening hemolysis when exposed to oxidative triggers from exogenous agents. Common agents include medications with strong oxidant properties, such as certain antimalarials (eg, primaquine, dapsone, and tafenoquine) and antibiotics (eg, sulfonamides, nitrofurantoin, and chloramphenicol), and consumption of fava beans.6 Another notable but less commonly known trigger for hemolysis is henna, a plant-based dye. However, for the radical cure of Plasmodium vivax and Plasmodium ovale malaria, current WHO guidelines recommend use of 8-aminoquinolines (eg, primaquine, tafenoquine) only after G6PD testing due to the risk of hemolysis, with patient counseling for potential risks advised after initiation of treatment. For uncomplicated P. falciparum malaria, artemether-lumefantrine remains one of the WHO-recommended first-line treatment. Though generally safe, it may cause mild or subclinical hemolysis, particularly in children with anemia or borderline G6PD activity, hence calling for close monitoring, especially in those under five years of age.7
Henna, derived from the Lawsonia inermis plant, is widely used for cosmetic and medicinal purposes across Southeast Asia, the Middle East, and Africa.8,9 In Northern Ghana, henna plays a prominent role in both cultural and religious practices. In G6PD-deficient individuals, particularly, severe hemolysis has been reported following the topical application of henna dye.9 However, the majority of cases documented in the literature involve male neonates and children.9–13
We present a case involving an 8-year-old girl with a full defect of G6PD, who presented to the Emergency Department of the Upper West Regional Hospital, Ghana, with severe intravascular hemolysis after a topical application of henna to her skin. To the best of our knowledge, this represents the first reported case of henna-induced hemolysis in a G6PD full-defect female child in Ghana.
Case Presentation
An 8-year-old girl presented to the Emergency Department of the Upper West Regional Hospital, Ghana, with a 7-day history of fever, general malaise, scleral icterus, and a one-day history of dark urine and vomiting. Symptoms began three days after the Ramadan celebration, during which she had henna tattoo decorations applied on both hands and one leg.
The patient had previously been treated for malaria with Artemether-Lumefantrine at another facility, with no improvement, leading to her referral. Her parents reported she had no known chronic illnesses or previous similar presentations.
On examination, the patient was febrile (38.0°C), moderately pale, and jaundiced. Henna tattoos were observed on both hands and the left leg. She was tachycardic (143 beats/min), with a respiration rate of 22 breaths/min, and an oxygen saturation (SPO2) of 96% on room air. Heart sounds were normal, with no significant findings in the chest. The abdomen was non-tender but with hepatosplenomegaly (liver palpable 8 cm, spleen 5 cm below the costal margins). Dark-colored urine was observed. Her neurological examination was normal.
Initial laboratory tests revealed significant anemia, characterized by a hypochromic microcytic blood picture, with a marked reduction in hemoglobin levels; leukocytosis, and thrombocytopenia were noted (Table 1). A blood film comment was requested for but its results were not immediately availed.
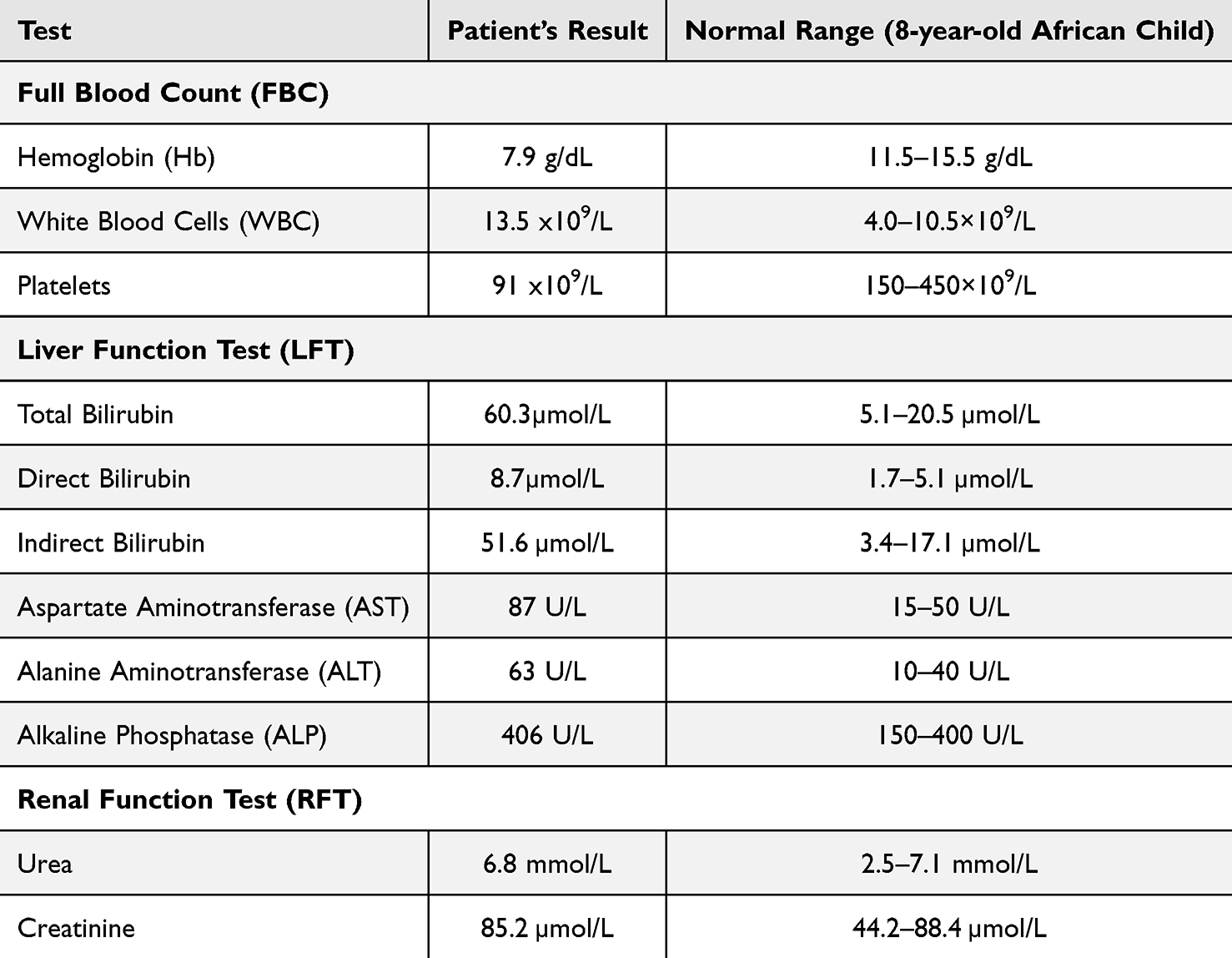 |
Table 1 Table Showing Some of the Patient’s Initial and Additional Laboratory Test Results |
A presumptive diagnosis of severe anemia due to intravascular hemolysis was made, with possible differentials of sickle cell disease, sepsis, partially treated malaria, and G6PD deficiency. She was immediately transfused with one unit of whole blood, hydrated, and started on intravenous Ceftriaxone (1g daily). Her condition worsened, with increased tachypnea and hypoxia (40 breaths/min, SPO2 88% on room air), requiring oxygen therapy. She became severely pale and more jaundiced, with darker urine as can be seen in Figure 1.
 |
Figure 1 Picture Showing Dark, Cola-Colored Urine Collection from the Patient. The image is an original creation of the authors. The picture was taken while the patient was in the hospital. |
Additional laboratory findings, including the initially requested blood film comment revealed no malaria parasites and a heterozygous sickle cell (AS) genotype on hemoglobin electrophoresis. Enzyme activity assay confirmed glucose-6-phosphate dehydrogenase (G6PD) deficiency. Liver function tests (LFTs) demonstrated markedly elevated liver enzymes, with concurrent hyperbilirubinemia (elevated direct and indirect bilirubin), as shown in Table 1. Hypoalbuminemia was also present. Renal function remained within normal limits, and urinalysis was unavailable at the time of presentation. The overall clinical and laboratory picture was consistent with severe intravascular hemolysis.
A diagnosis of severe intravascular hemolysis due to G6PD deficiency, precipitated by henna application, was made. The henna connection was established after further inquiry which revealed symptom onset was three days after its application for the Ramadan celebration. The patient had no previous exposure to henna.
Significant improvements occurred after the henna tattoos were removed with lime. She received a second unit of blood and continuous hydration with intravenous fluids. Her jaundice subsided, and her urine color improved. After 12 days of hospitalization, she was discharged with a hemoglobin level of 10.2 g/dL and was prescribed folic acid.
At a follow-up review a week after discharge, the patient had no new complaints. Her parents were counseled and educated about G6PD deficiency before her final discharge.
Discussion
Henna has been historically and contemporarily used across Africa and Asia for cultural and ceremonial purposes, often applied topically to the skin in decorative patterns and tattoos (Figure 2). In Ghana, henna powder and dyes are primarily used for cosmetic purposes, such as adorning brides during weddings and marking religious events, such as Ramadan, as seen in this case. Henna is also widely used during other traditional festivities.8,9 In this instance, the powdered form of henna, locally referred to as lele, was applied.
 |
Figure 2 Image Showing a Typical Henna Application on the Hands. The image is an originally sourced creation from one of the authors. |
The active compound in henna, lawsone (2-hydroxy-1,4-naphthoquinone; C10H6O3), is a naphthoquinone structurally related to naphthalene (C10H8), another well-known hemolytic agent in G6PD-deficient individuals (Figure 3A and B). Naphthalene is the active ingredient in mothballs, which are widely utilized in Ghana as insect repellents for clothing, air fresheners, and even water purifiers in many homes. Additionally, mothballs have been used locally to treat certain respiratory conditions.14,15
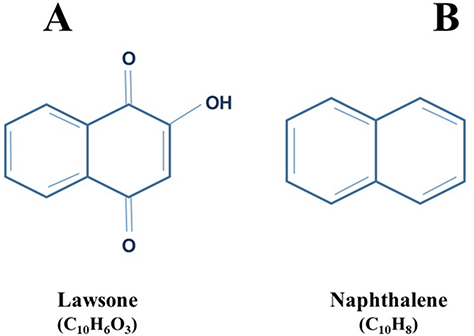 |
Figure 3 Similarities of Structural Rings of Lawsone (A) and Naphthalene (B). The structural ring designs and labels are the authors’ creations. |
Mothballs (camphor) are recognized as triggers for severe neonatal jaundice in G6PD-deficient babies.11 Despite the extensive use of henna in Northern Ghana, no prior documented reports have linked it with G6PD deficiency-induced hemolysis in the region.
Most of the documented cases of life-threatening hemolysis associated with G6PD deficiency in the literature involve males, which aligns with the X-linked inheritance pattern of this enzyme defect. Due to X–inactivation or lyonization, heterozygous females display a mosaic of G6PD activity, ranging from normal to severely deficient.12,13
There is limited data on G6PD deficiency in females, particularly in Northern Ghana. Therefore, a high index of suspicion is required when evaluating female patients presenting with hemolytic anemia, even in the absence of a family history. G6PD deficiency should be considered a differential diagnosis in cases of intravascular hemolysis in regions where henna is widely used, especially among girls and women.
Additionally, residing in a malaria-endemic area, the patient’s initial presentation with fever could have suggested a malarial complication. However, her blood film showed no malaria parasites, which could be attributed to the full course of antimalarial treatment she had received prior to her presentation at our facility.
Furthermore, certain antibiotics commonly prescribed in Ghana may induce hemolysis in G6PD-deficient individuals (Table 2).
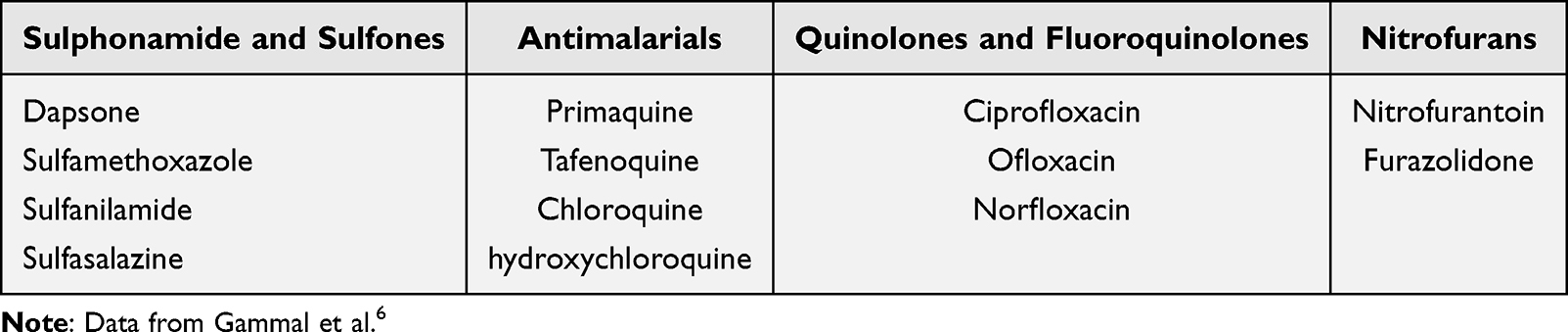 |
Table 2 List of Some Hemolysis-Inducing Medications in Glucose-6-Phosphate Dehydrogenase Deficiency |
Severe hemolysis can lead to acute renal failure as a result of hemoglobinuria.13,16 This can be mitigated through adequate hydration. In resource-limited settings, monitoring the resolution of dark-colored urine via continuous urine collection, urinalysis, and regular renal function tests is crucial to prevent hemoglobinuria-induced acute renal failure.16
In this case, the absence of renal impairment may be attributed to aggressive hydration. The liver function test findings were consistent with intravascular hemolysis. Management of this case focused on symptomatic treatment, including the removal of the precipitating agent-henna-which was successfully cleansed using lime. Although there is limited empirical evidence supporting topical use of lime for henna removal, anecdotal reports suggest use of this practice in various local communities.
Conclusion
This case underscores two critical points: the risk of severe hemolysis associated with henna use in a G6PD-deficient child and the occurrence of G6PD deficiency in females. These findings emphasise the need for public health awareness regarding the need for compulsory G6PD testing before application of henna. In many low-resource settings, G6PD screening at birth is limited, often only performed in male neonates. We recommend expanding G6PD deficiency screening to include both sexes where feasible. In regions where screening is unavailable, clinicians should maintain a high index of suspicion for G6PD deficiency in female children presenting with hemolysis, to facilitate earlier diagnosis and management.
Ethical Considerations
No institutional approval was required to publish the case details as a departmental ethics committee approved study of our case.
Consent for Publication
Written informed consent for publication was obtained from the guardian.
Acknowledgments
Special acknowledgment to Dr. Saeed Gausu and Dr. Edward Nyaaba, who were part of the team that attended to the patient while on admission and gave helpful information to the authors in documenting the case. We also acknowledge, with gratitude, Ms. Mariyah S. and Mrs. Safiya S. for supporting the authors with one of the images used in this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that no conflicts of interest that could appear to have influenced this work.
References
1. Nkhoma ET, Poole C, Vannappagari V, Hall SA, Beutler E. The global prevalence of glucose-6-phosphate dehydrogenase deficiency: a systematic review and meta-analysis. Blood Cells Mol Dis. 2009;42(3):267–278. doi:10.1016/j.bcmd.2008.12.005
2. Francis RO, Jhang JS, Pham HP, Hod EA, Zimring JC, Spitalnik SL. Glucose-6-phosphate dehydrogenase deficiency in transfusion medicine: the unknown risks. Vox Sang. 2013;105(4):271–282. doi:10.1111/vox.12068
3. Taleb M, Brahim AT, Yebouk C, et al. Epidemiology of glucose-6-phosphate dehydrogenase deficiency in 10 malaria-endemic countries in sub-Saharan Africa: a systematic review. Pan Afr Med J. 2025;50:7. doi:10.11604/pamj.2025.50.7.45066
4. World Health Organization. Glucose-6-phosphate dehydrogenase deficiency. Bull World Health Organ. 1989;67(6):601–611.
5. Wajcman H, Galactéros F. Le déficit en glucose-6 phosphate déshydrogénase: protection contre le paludisme et risque d’accidents hémolytiques. C R Biol. 2004;327(8):711–720. doi:10.1016/j.crvi.2004.07.010
6. Gammal RS, Pirmohamed M, Somogyi AA, et al. Expanded clinical pharmacogenetics implementation consortium guideline for medication use in the context of G6PD genotype. Clin Pharmacol Ther. 2023;113(5):973–985. doi:10.1002/cpt.2735
7. World Health Organization. WHO Guidelines for Malaria, 30 November 2024. World Health Organization; 2024.
8. Quainoo AK, Gali NM, Mahunu GK. Henna (Lawsonia inermis): a neglected plant in Ghana. Ghana J Hortic. 2017;12(1):32–38.
9. Kheir A, Gaber I, Gafer S, Ahmed W. Life-threatening haemolysis induced by henna in a Sudanese child with glucose-6-phosphate dehydrogenase deficiency. East Mediterr Health J. 2017;23(1):28–30. doi:10.26719/2017.23.1.28
10. Kandil HH, al-Ghanem MM, Sarwat MA, al-Thallab FS. Henna (Lawsonia inermis Linn.) inducing haemolysis among G6PD-deficient newborns. A new clinical observation. Ann Trop Paediatr. 1996;16(4):287–291. doi:10.1080/02724936.1996.11747840
11. Raupp P, Hassan JA, Varughese M, Kristiansson B. Henna causes life threatening haemolysis in glucose-6-phosphate dehydrogenase deficiency. Arch Dis Child. 2001;85(5):411–412. doi:10.1136/adc.85.5.411
12. Söker M, Devecioğlu C, Haspolat YK, Dikici B, Doğru Ö. Henna induced acute hemolysis: henna induced acute hemolysis in a G6PD-deficient patient: a case report. 2000. Available from: https://hdl.handle.net/11468/8390.
13. Devecioğlu C, Katar S, Doğru O, Taş MA. Henna-induced hemolytic anemia and acute renal failure. Turk J Pediatr. 2001;43(1):65–66.
14. Scutti S. Profile: fogarty Scholar Dr. Nauzley Abedini studies neonatal jaundice in Ghana - Fogarty International Center @ NIH. Fogarty International Center; 2020. Available from: https://www.fic.nih.gov:443/News/GlobalHealthMatters/march-april-2020/Pages/nauzley-abedini-neonatal-jaundice-ghana.aspx.
15. Soghoian S, Nyadedzor C, Ed Nignpense B, Clarke EEK, Hoffman RS. Health risks of using mothballs in Greater Accra, Ghana. Trop Med Int Health. 2012;17(1):135–138. doi:10.1111/j.1365-3156.2011.02885.x
16. Rosado Rubio C, Fraile Gómez P, García Cosmes P, Díez Bandera R, González Álvarez C. Intravascular haemolysis and renal failure. Nefrología. 2011;31(5):621–622. doi:10.3265/Nefrologia.pre2011.Jun.10941
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.