Back to Journals » International Journal of Women's Health » Volume 18
Hemorrhagic Shock and Massive Abdominal Wall Hematoma After Cesarean Section in a Patient with Peripartum Acquired Hemophilia A:A Case Report
Authors Huang Q, Chen X, Wu X, Xu S, Zheng X, Li X, Zhang S, Fu S
Received 18 August 2025
Accepted for publication 9 January 2026
Published 28 January 2026 Volume 2026:18 557109
DOI https://doi.org/10.2147/IJWH.S557109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Qiaoyao Huang,1,* Xiaojun Chen,1,* Xiaohuan Wu,2 Shilian Xu,1 Xiaohang Zheng,1 Xueyan Li,3 Shuning Zhang,3 Shuai Fu3
1Department of Gynaecology and Obstetrics, Shenshan Medical Central, Memorial Hospital of Sun Yat-Sen University, Shanwei, 516600, People’s Republic of China; 2Department of Internal Medicine, Shenshan Medical Central, Memorial Hospital of Sun Yat-sen University, Shanwei, 516600, People’s Republic of China; 3Department of Gynaecology and Obstetrics, Memorial Hospital of Sun Yat-Sen University, Guangzhou, 510000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuai Fu, Email [email protected] Shuning Zhang, Email [email protected]
Abstract: Acquired Hemophilia A (AHA), a rare bleeding disorder caused by autoimmune suppression of coagulation factor VIII(FVIII), has a low incidence in perinatal women but carries significant risks of severe hemorrhage. The lack of consensus guidelines and limited clinical data from developing countries underscore the importance of this case report. Consequently, this report informs clinical practice and expands the evidence base for the treatment of AHA. This case describes an extensive abdominal wall hematoma and hemorrhagic shock following a cesarean section in a patient. The condition was successfully managed through comprehensive interventions, including shock resuscitation, endovascular embolization, pharmacological hemostatic therapy, removal of circulating immune complexes, and immunosuppressive therapy. AHA usually causes acute bleeding, and early identification and removal of acquired inhibitors are the main treatment methods. In such cases, endovascular embolization is an effective procedure to control bleeding.
Keywords: acquired hemophilia A, activated partial thromboplastin time, factor VIII inhibitors, endovascular embolization, perinatal
Introduction
Acquired Hemophilia A (AHA) is characterized by the production of neutralizing autoantibodies (inhibitors) against coagulation factor VIII (FVIII). AHA typically presents with significantly reduced FVIII activity levels (<0.3 IU/dL, often <0.01 IU/dL), while FIX, FXI, FXII, and vWF levels remain unimpaired. With an incidence rate of approximately 1/350,000 deliveries during the perinatal period, it carries a mortality rate as high as 20–30%.1–3 The clinical significance of perinatal AHA has become increasingly prominent due to the growing number of older mothers and the widespread use of assisted reproductive technologies. In research on perinatal AHA, the identification and analysis of risk factors are crucial. Key contributing factors include pregnancy-related factors (such as multiple pregnancies, hypertensive disorders of pregnancy, and placental abnormalities), histories of autoimmune diseases (like systemic lupus erythematosus and rheumatoid arthritis), and genetic predisposition (eg, specific HLA genotypes.3–8 Researches indicate that altered immune tolerance during pregnancy serves as a critical mechanism for the development of anti-FVIII autoantibodies.2,9–12 Specifically, some women may experience dysregulation of immune regulatory mechanisms during gestation, leading to autoantibody production and subsequent bleeding associated with AHA. Clinically, this manifests as increased bleeding primarily during delivery and perinatal procedures rather than throughout pregnancy.13–16 Typical clinical presentations include postpartum hemorrhage and non-uterine bleeding.6,13,17 Given the persistent bleeding risks during the puerperium, clinicians typically adopt two approaches: avoiding surgery (which may delay critical treatment windows and potentially lead to organ failure or death) or performing early surgery (which may cause unnecessary interventions and worsen patient outcomes). Therefore, minimally invasive endovascular embolization therapy, which is associated with fewer complications, has been shown to be superior for patients with acute active bleeding, significantly reducing mortality and recurrence rates related to hemorrhagic management.3,18,19 Isolated prolongation of APTT may be observed in some patients. The clinical differential diagnosis should encompass various possibilities, such as hereditary coagulation factor deficiencies; acquired anticoagulants; and drug-induced effects. Therefore, an integrated assessment of the patient’s medical history, specific clinical symptoms, and laboratory findings is essential to facilitate timely identification of the underlying cause and guide appropriate therapeutic interventions.17 We present a case of post-cesarean section abdominal wall hematoma with hemorrhagic shock due to AHA. Through comprehensive treatment, including anti-shock therapy, endovascular embolization, pharmacological hemostasis, antibody elimination, and immunosuppressive therapy, complete remission was achieved. Follow-up examinations over six months showed no recurrence. Despite delayed diagnosis in this case, endovascular embolization proved essential for rapid hemostasis and risk reduction in this case, which provided new clinical insights into early recognition and emergency intervention for peripartum AHA. The study was approved by the Ethics Committee of Shenshan Medical Central, Memorial Hospital of Sun Yat-sen University (2025-SSKY-078), including the permission of publication of case details.
Case Presentation
Written informed consent for publication has been obtained from the patient. A 33-year-old multiparous woman was transferred to our hospital’s obstetrics department on January 3, 2025. She had persistent postoperative incision bleeding from a cesarean section that had lasted for one day. Prior to pregnancy, the patient maintained regular menstrual cycles without history of menorrhagia, easy bruising, skin rashes, joint pain, or fever. She denied previous hematological disorders or family genetic predispositions. This pregnancy resulted from assisted reproductive technology (ART) due to tubal factors. Prenatal checkups showed no abnormalities. On January 2, 2025, she underwent a second cesarean section under general anesthesia for threatened labor, scarred uterus, and full-term pregnancy. Preoperative activated partial thromboplastin time (APTT) was prolonged to 90.7 seconds but was not immediately addressed due to urgent surgical needs. The surgery was completed smoothly, with intraoperative blood loss of 300 mL. Two hours after surgery, continuous incision bleeding developed, necessitating secondary suture reinforcement, hemostatic injections, intramuscular vitamin K1, intermittent transfusion of 4.5U suspended red blood cells, 800 mL frozen plasma, and 12U cryoprecipitate. However, the bleeding continued. Twenty-seven hours postoperatively, the patient was transferred to our hospital. Physical examination revealed an anemic appearance without skin rashes, petechiae, or ecchymosis. The uterine fundus was firm and transverse. The incision site showed active dark red oozing with firm tissue within 5 cm around it. A hard subcutaneous nodule approximately 5×5 cm was palpable 4 cm lateral to the left umbilicus, with mild tenderness. No other abdominal tenderness or rebound was noted. Vaginal examination showed scant dark red bloody lochia, while cervical and vaginal mucosa remained normal with no abnormalities. Blood tests revealed: red blood cell count 2.21 × 10^12/L, hemoglobin 60 g/L, platelet count 190.0 × 10^9/L, hematocrit 16.6%. Coagulation tests showed prothrombin time 10.0s, international normalized ratio (INR) 0.84, fibrinogen 3.14 g/L, activated partial thromboplastin time 67.7s, thrombin time 14.3s, and D-dimer 1.46 μg/L. Simultaneous treatment with wound compression and hemostatic therapy.
On January 3, 2025, we performed an exploratory surgery under general anesthesia to examine the incision, debride the hematoma, and suture the wound. This procedure was necessary due to continuous bleeding from the incision site, and vascular activity in the wound could not be ruled out. During the procedure, extensive subfascial and dark red blood clots were observed. The hematoma extended approximately 3 to 4 centimeters above the umbilicus. Active bleeding was noted from both infraperitoneal arterial branches traversing the fascia. Dense adhesions between the rectus abdominis muscle and peritoneum caused multiple active hemorrhages in the rectus space and on the peritoneal surface. No active bleeding was detected in the pelvic or abdominal cavities, only a small amount of old dark red exudate was present (Figure 1).
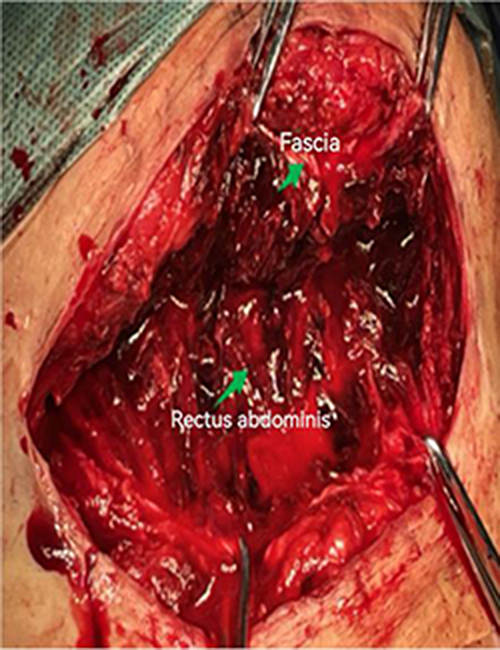 |
Figure 1 Bleeding from the inferior epigastric artery during debridement. |
The urinary catheter was removed 24 hours after debridement. Following ambulation, significant swelling developed around the incision 2 centimeters above the umbilicus, accompanied by fever and tachycardia. Repeated blood tests showed a progressive decrease in hemoglobin to 55 g/L, accompanied by hypotension (blood pressure 80/50 mmHg) and active bleeding at the incision site. Intravenous fluid resuscitation and blood transfusion were immediately administered.
Following a multidisciplinary(MDT) consultation on January 6, a definitive abdominal artery angiography with selective embolization was planned. During the Seldinger procedure for right femoral artery, leakage of contrast agent was detected in the left and right inferior epigastric arteries puncture (Figures 2–6). After embolization of these sites, the patient was transferred to the ICU for continued intensive care.
 |
Figure 2 Angiography of the inferior epigastric artery branch (left). A red circle marks the area of contrast extravasation, identifying the active bleeding site. |
 |
Figure 3 After interventional embolization of the inferior epigastric artery branch (left). |
 |
Figure 4 A bleeding artery with contrast extravasation, marked by a red circle to identify the active site. |
 |
Figure 5 Angiography of the inferior epigastric artery branch (right). A red arrow marks the area of contrast extravasation, identifying the active bleeding site. |
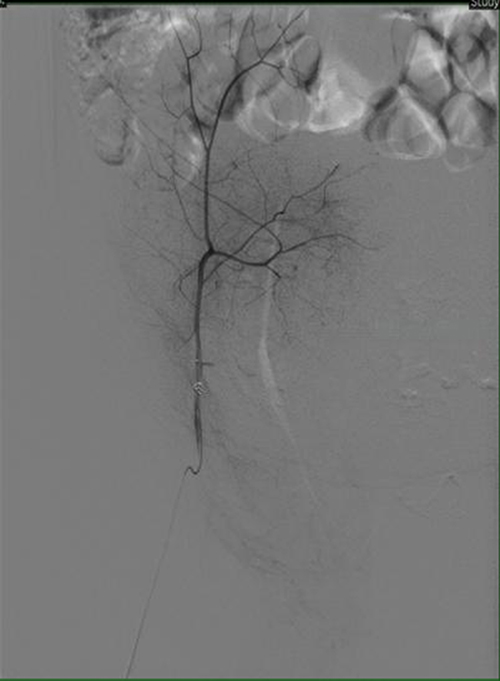 |
Figure 6 After interventional embolization of the inferior epigastric artery branch (right). |
Previous laboratory tests showed a coagulation factor VIII level of 0.2%. The inhibitor titer was 64 Bethesda Units (BU). After excluding lupus anticoagulants and disseminated intravascular coagulation (DIC), routine parameters including fibrinogen, lactate dehydrogenase (LDH), uric acid, and antiphospholipid antibodies were found to be normal. The diagnosis was confirmed to be acquired hemophilia A (coagulation factor VIII deficiency). Treatment focused on controlling and preventing bleeding, as well as eliminating inhibitors. The patient was then transferred to the hematology department for further therapy, including hormone therapy with methylprednisolone, immunosuppressant therapy with azathioprine, rituximab therapy. Subsequent testing revealed undetectable coagulation factor VIII inhibitors, with prothrombin time (PTT) and coagulation factor VIII levels normalized. The timeline for the entire episode of treatment outlined above is shown in a diagram (Figure 7).
 |
Figure 7 Timeline of key events, laboratory values, and interventions for the patient. Activated partial thromboplastin time (APTT); Hemoglobin (HB); Coagulation factor VIII activity (F-VIII:C); Bethesda Units (BU). |
Discussion
Diagnosing and managing perinatal acquired hemophilia A is challenging. This is mainly because standardized guidelines are lacking, and the pathophysiology is not well understood. Bleeding symptoms of AHA include soft tissue hematomas, mucosal bleeding, genital bleeding, intracranial hemorrhage, and persistent bleeding following trauma or surgery.1,2,20–22 Even in patients without visible bleeding, prolonged activated partial thromboplastin time (APTT) suggests possible acquired coagulopathy.17 This case report demonstrates a definitive diagnosis of acquired hemophilia A following postpartum fatal hemorrhage caused by progressive surgical wound hematoma with persistent coagulopathy. Diagnosing AHA requires distinguishing it from primary hemophilia, disseminated intravascular coagulation (DIC), hemolytic anemia, and other rare diseases.2,4,23 As AHA is exceptionally uncommon, most cases are identified incidentally during post-hemorrhagic etiological investigations, often leading to delayed diagnosis and treatment after excluding other potential causes. Persistent APTT prolongation unresponsive to mixed prothrombin time (PTT) testing suggests possible antithrombotic factor deficiency or severe coagulation factor depletion. The mixed prothrombin time test evaluates PTT changes through plasma mixing with normal plasma. Therefore, when isolated PTT elevation is detected preoperatively in patients without prior coagulation abnormalities, particularly when no identifiable etiology exists, AHA should be urgently considered.17 In clinical practice, early identification of high-risk factors is crucial. Studies indicate that patients undergoing ART face higher relative risk of perinatal coagulation disorders compared to naturally conceived women.2,14,17,24 This phenomenon may result from hormonal fluctuations and placental dysfunction in ART recipients, leading to increased coagulation risks. Research suggests that placenta-derived FVIII antigen exposure, Treg cell dysfunction, and abnormal B-cell activation may be primary mechanisms disrupting perinatal immune tolerance.25,26 This phenomenon may result from hormonal fluctuations and placental dysfunction in ART recipients, leading to increased coagulation risks. Therefore, enhanced coagulation monitoring and personalized intervention strategies are necessary in prenatal care for these high-risk groups. In this case, the patient conceived through ART, although laboratory tests showed significant prolongation of APTT, AHA was not initially considered, and further confirmatory tests were not performed. The plasma inhibitor was not removed promptly, and coagulation did not improve. This led to a worse prognosis, a longer and more difficult treatment, and increased the financial burden on the patient’s family.
The patient in this case presented with persistent postoperative active bleeding accompanied by signs of shock. For emergency management, bypass agents such as recombinant activated factor VII (rFVIIa) or activated prothrombin complex concentrate (aPCC) should be prioritized as hemostatic agents.1,4,17,27 The patient with hemodynamic stability during acute active bleeding may benefit from conservative measures like fluid transfusion and coagulation factor correction, while unstable patient may require aggressive treatment. Nowadays, percutaneous endovascular embolization can rapidly control bleeding and reduce complication risks in perinatal-onset hemophilia A patient, especially those undergoing frequent short-term surgeries and experiencing tissue edema. After multidisciplinary consultation, we decided to implement shock treatment alongside percutaneous transcatheter arterial embolization to achieve hemostasis. This approach successfully controlled the bleeding and avoided the trauma associated with a repeat surgical intervention. Studies have shown that early identification and accurate diagnosis are key factors in improving patient outcomes, while timely initiation of immunosuppressive therapy is crucial for controlling disease progression and enhancing survival rates.17,21,28,29
Immunosuppressive therapy plays a crucial role during the perinatal period in treating acquired hemophilia A (AHA) and related coagulation disorders. These treatments aim to control bleeding and improve overall patient outcomes. In clinical practice, glucocorticoids, rituximab, and combination chemotherapy regimens (such as cyclophosphamide) are primary treatment options.17 Studies have shown that patients receiving glucocorticoid therapy experienced significantly reduced bleeding incidence and improved post-treatment prognosis.6,17,30 However, for patients who still develop severe bleeding or coagulation dysfunction after glucocorticoid use, rituximab can substantially enhance clinical outcomes.29,31 Evidence indicates that combining rituximab with glucocorticoids enhances therapeutic efficacy while reducing bleeding risks.17 Through judicious use of medications including glucocorticoids, rituximab, and cyclophosphamide, effective bleeding control and improved patient outcomes can be achieved. However, clinicians must closely monitor treatment responses and adjust regimens promptly to ensure optimal therapeutic effects and minimize side effects. This case report presents a patient who achieved complete remission through these therapies, with no recurrence observed over a six-month follow-up period, indicating a favorable prognosis. This case report demonstrates that effective blood vessel embolization, combined with appropriate use of glucocorticoids and rituximab, improved the patient’s prognosis. This improvement followed successful hemorrhage control. It should be noted that this study is a case report with a limited follow-up duration and therefore may not adequately reveal long-term effects or late complications associated with the disease.
Conclusion
We report a rare case of perinatally acquired hemophilia A, in which the patient developed an abdominal wall hematoma following cesarean delivery; this hematoma led to hemorrhagic shock, underscoring the critical importance of timely diagnosis and decisive intervention. Percutaneous embolization targeting the bleeding vessels played a key role in controlling the acute hemorrhage. Successful management of perinatally acquired hemophilia A requires close multidisciplinary collaboration, including obstetrics, hematology, anesthesiology, and interventional radiology. Given the rarity and diagnostic challenges of this disorder, enhancing awareness, establishing early identification protocols, and implementing standardized management protocols are essential to reducing maternal and neonatal hemorrhagic complications and improving survival and functional outcomes.
Ethical Statement
The study was approved by the Ethics Committee of Shenshan Medical Central, Memorial Hospital of Sun Yat-sen University (2025-SSKY-078).
Funding
This study was supported by Projects of Shanwei Science and Technology Bureau for Social Development (No. 2024C031).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zuner E, Desage S, Rezigue H, et al. Current trends and advances in the management of acquired hemophilia A. Blood Rev. 2025;74:101320. doi:10.1016/j.blre.2025.101320
2. Tengborn L, Baudo F, Huth-Kuhne A, et al. Pregnancy-associated acquired haemophilia A: results from the European acquired haemophilia (EACH2) registry. Bjog-Int J Obstet Gy. 2012;119(12):1529–9. doi:10.1111/j.1471-0528.2012.03469.x
3. Knoebl P, Marco P, Baudo F, et al. Demographic and clinical data in acquired hemophilia A: results from the European acquired haemophilia registry (EACH2). J Thromb Haemost. 2012;10(4):622–631. doi:10.1111/j.1538-7836.2012.04654.x
4. Lindahl R, Nummi V, Lehtinen AE, et al. Acquired haemophilia A in four north European countries: survey of 181 patients. Brit J Haematol. 2023;201(2):326–333. doi:10.1111/bjh.18611
5. Tian C, Perija B, Kotb R, et al. Acquired haemophilia A: a 15-year population-based review of incidence rate, patient demographics and treatment outcomes. Haemophilia. 2023;29(5):1269–1275. doi:10.1111/hae.14845
6. Lehoczki A, Fekete M, Mikala G, et al. Acquired hemophilia A as a disease of the elderly: a comprehensive review of epidemiology, pathogenesis, and novel therapy. Geroscience. 2025;47(1):503–514. doi:10.1007/s11357-024-01317-7
7. Pardos-Gea J, Martin-Fernandez L, Closa L, et al. Key genes of the immune system and predisposition to acquired hemophilia A: evidence from a Spanish cohort of 49 patients using next-generation sequencing. Int J Mol Sci. 2023;24(22):16372. doi:10.3390/ijms242216372
8. Shoji-Asahina A, Nakatani E, Imaichi Y, et al. Risk factors, treatment and survival rates of late-onset acquired haemophilia A: a cohort study from the Shizuoka Kokuho Database. Haemophilia. 2023;29(3):799–808. doi:10.1111/hae.14793
9. Paidas MJ, Hossain N. Unexpected postpartum hemorrhage due to an acquired factor VIII inhibitor. Am J Perinat. 2014;31(8):645–654.
10. Lulla RR, Allen GA, Zakarija A, et al. Transplacental transfer of postpartum inhibitors to factor VIII. Haemophilia. 2010;16(1):14–17. doi:10.1111/j.1365-2516.2009.02049.x
11. Alippe Y, Hatterschide J, Coyne CB, et al. Innate immune responses to pathogens at the maternal-fetal interface. Nat Rev Immunol. 2025;25(12):869–884. doi:10.1038/s41577-025-01191-0
12. Wang J, Han T, Zhu X. Role of maternal-fetal immune tolerance in the establishment and maintenance of pregnancy. Chinese Med J-Peking. 2024;137(12):1399–1406. doi:10.1097/CM9.0000000000003114
13. Ejaz A, O’Doherty C, Sharpley FA, et al. Acquired haemophilia A diagnosed during pregnancy. Obstet Med. 2023;16(1):56–58. doi:10.1177/1753495X211049987
14. Oberlin A, Krenitsky NM, Gandhi C, et al. Acquired hemophilia A: a rare, acquired coagulopathy in the postpartum setting. AJP Rep. 2023;13(4):e85–8. doi:10.1055/a-2198-7888
15. Nowak KM, Carpinteiro A, Szalai C, et al. Acquired hemophilia A: a permanent challenge for all physicians. Medicines. 2022;9(3). doi:10.3390/medicines9030021
16. Arruda VR, Lillicrap D, Herzog RW. Immune complications and their management in inherited and acquired bleeding disorders. Blood. 2022;140(10):1075–1085. doi:10.1182/blood.2022016530
17. Tiede A, Collins P, Knoebl P, et al. International recommendations on the diagnosis and treatment of acquired hemophilia A. Haematologica. 2020;105(7):1791–1801. doi:10.3324/haematol.2019.230771
18. Albuquerque T, Monsignore LM, de Castro-Afonso LH, et al. Transarterial embolization with n-butyl cyanoacrylate for the treatment of abdominal wall hemorrhage. Diagn Interv Radiol. 2020;26(3):216–222. doi:10.5152/dir.2019.19348
19. Minici R, Fontana F, Venturini M, et al. A multicenter retrospective cohort study evaluating the clinical outcomes of patients with coagulopathy undergoing transcatheter arterial embolization (TAE) for acute non-neurovascular bleeding. Medicina-Lithuania. 2023;59(7):1333.
20. Qian L, Ge H, Hu P, et al. Pregnancy-related acquired hemophilia A initially manifesting as pleural hemorrhage: a case report. Medicine. 2019;98(3):e14119. doi:10.1097/MD.0000000000014119
21. Zanon E. Acquired hemophilia A: an update on the etiopathogenesis, diagnosis, and treatment. Diagnostics. 2023;13(3):420. doi:10.3390/diagnostics13030420
22. Kanitthamniyom C, Siladech P, Polpichai N, et al. Combined life-threatening internal organ bleeding and postpartum hemorrhage associated with acquired hemophilia A. Clin Case Rep. 2024;12(1):e8399. doi:10.1002/ccr3.8399
23. James AH, Pacheco LD, Konkle BA. Management of pregnant women who have bleeding disorders. Hematol-Am Soc Hemat. 2023;2023(1):229–236.
24. Attanasio M, Cirillo M, Coccia ME, et al. Factors VIII and Von Willebrand levels in women undergoing assisted reproduction: are their levels associated with clinical pregnancy outcome? Mediterr J Hematol I. 2020;12(1):e2020058. doi:10.4084/mjhid.2020.058
25. Evangelidis N, Kotsiou N, Evangelidis P, et al. Genetics and epigenetics in acquired hemophilia A: from bench to bedside. Curr Issues Mol Biol. 2024;46(6):5147–5160. doi:10.3390/cimb46060309
26. Schultze-Florey CR, Thol FR, Aleksandrova K, et al. Anti-CD19 CAR-T cell therapy for acquired hemophilia A. Leukemia. 2025;39(4):980–982. doi:10.1038/s41375-025-02554-1
27. Bannow BS, Konkle BA. How I approach bleeding in hospitalized patients. Blood. 2023;142(9):761–768. doi:10.1182/blood.2021014766
28. Marino R. Acquired hemophilia A: bleeding pattern and hemostatic therapeutic strategies. Medicina-Lithuania. 2023;59(10):1739.
29. Levesque H, Viallard JF, Houivet E, et al. Cyclophosphamide vs rituximab for eradicating inhibitors in acquired hemophilia A: a randomized trial in 108 patients. Thromb RES. 2024;237:79–87. doi:10.1016/j.thromres.2024.03.012
30. Tiede A. Immunotherapy of acquired hemophilia A. Hematol-Am Soc Hemat. 2023;2023(1):19–23.
31. Rungjirajittranon T, Suwanawiboon B, Nakkinkun Y, et al. First-line immunosuppressive therapies for acquired hemophilia A: a 25-year cohort experience and network meta-analysis. Thromb Res. 2024;241:109067. doi:10.1016/j.thromres.2024.109067
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.