Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Heart rate variability and incidence of depression during the first six months following first myocardial infarction
Authors Wilkowska A ![]() , Rynkiewicz A
, Rynkiewicz A ![]() , Wdowczyk J, Landowski J
, Wdowczyk J, Landowski J ![]() , Cubała WJ
, Cubała WJ ![]()
Received 16 April 2019
Accepted for publication 22 May 2019
Published 10 July 2019 Volume 2019:15 Pages 1951—1956
DOI https://doi.org/10.2147/NDT.S212528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Alina Wilkowska,1 Andrzej Rynkiewicz,2 Joanna Wdowczyk,3 Jerzy Landowski,1 Wiesław Jerzy Cubała1
1Department of Psychiatry, Faculty of Medicine, Medical University of Gdansk, Gdańsk, Poland; 2Department of Cardiology and Cardiosurgery, Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland; 3First Department of Cardiology, Faculty of Medicine, Medical University of Gdansk, Gdańsk, Poland
Background: Post-myocardial depression is a highly prevalent condition worsening the course and prognosis of coronary artery disease. One of the possible pathogenetic factors is dysregulation of the autonomous nervous system, resulting in heart rate variability reduction.
Methods: Twenty two patients hospitalised due to a first myocardial infarction were included. The Beck Depression Inventory (BDI) was used to rate the severity of their depressive symptoms.
Results: Depressive symptomatology, defined as BDI ≥10, was present in 36.3% of the patients. Increase in heart rate variability (HRV) was observed in both groups during the first 6 months after the myocardial infarction. The HRV was significantly lower in the depressed group compared to patients without depression.
Conclusion: Presence of depression after the myocardial infarction (MI) is associated with a significant decrease of the time domain HRV measure SDNN (standard deviation of all normal RR intervals) and with its slower increase during at least a three months period.
Keywords: depression, myocardial infarction, autonomic nervous system, heart rate variability
Introduction
Patients with heart disease are four times more likely to develop depression than the general population and depression is an independent risk factor for cardiac morbidity and mortality. Low heart rate variability (HRV), which reflects increased sympathetic and/or inadequate parasympathetic modulation of heart rate, is a strong predictor of mortality in patients with CHD.1–3 Although the link between HRV and depression is yet to be fully elucidated, research has shown a relatively consistent association between reductions in HRV and major depressive disorder (MDD).4,5 Depression in patients with no history of somatic morbidity results in an autonomic nervous system imbalance in the form of sympathetic hyperactivity, parasympathetic impairment, or both6,7 This autonomous system dysregulation reflected by reduced HRV is also observed in coronary artery disease (CAD) patients without depression.8 Heart rate variability is reduced after reperfused MI during the first 24 hrs,9 about two weeks after the MI10 and it increases during the subsequent 12 months.11 It seems that the effect on HRV imbalance is also pronounced in patients with depression and CAD12 and with depression after MI.13
We hypothesized that HRV after reperfused MI is lower in patients with depression and the increase in HRV is slower in depression group.
The aim of this study was to observe the change in the time domain of the HRV measure (SDNN) in patients after a first MI according to the presence of depression.
Methods
Subjects
Twenty-two patients were admitted to the tertiary reference centre for cardiology with their first acute MI with ST elevation (STEMI). Table 1 presents the demographic and clinical characteristics of the study population. The 22 patients took part in another study on the biological effects of depression discussed in detail elsewhere14 and completed the follow-up period with 24 h ECG recordings. Each patient underwent invasive coronary angiography and revascularization with stent implantation in culprit lesion. All patients received standard pharmacological treatment: antiplatelet drugs – clopidogrel and aspirin, statin, beta blocker and ACE inhibitor in standard doses.
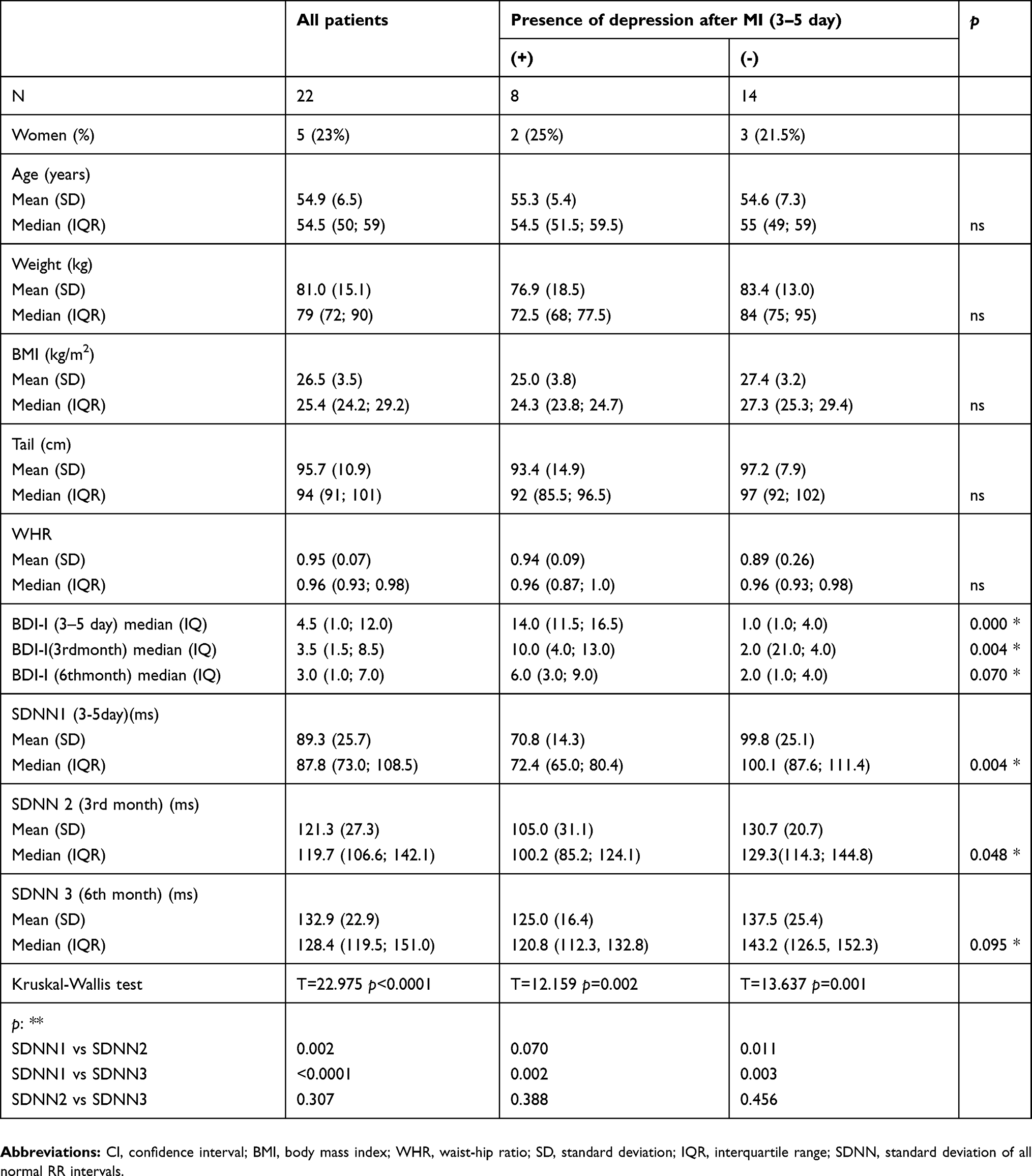 |
Table 1 Demographic and clinical variables |
The left ventricle ejection fraction (LVEF) was ≥40%. The exclusion criteria were endocrine diseases such as diabetes, hypo- or hyperthyroidism, severe renal or hepatic failure, hormone therapy, active substance use disorder and the presence of psychiatric disorders other than depression, anxiety disorders, and stress related and adjustment disorders.
All the patients were diagnosed with the Structured Clinical Interview for DSM-IV Axis I Disorders15 three times during the six months period after MI: specifically, on the third day and in the 3rd and 6th month after MI.
The intensity of depressive symptoms was estimated three times during 6 months of observation with Beck Depression Inventory (BDI-I).16
The cut-off score of ≥10 for BDI-I qualified the subjects to the depression group; it was present in 36.3% of the patients.
The study was approved by the Independent Ethics Committee of the Medical University of Gdansk (approval number NKEBN/205/2006). For each participant, written informed consent was obtained.
Heart rate variability measurement
A straightforward metric of HRV, termed the SDNN, is the standard deviation of all normal RR intervals (those measured between consecutive sinus beats). The SDNN may be easily calculated from a 24 hr Holter monitor. In calculating SDNN, any RR interval that begins or ends with a PAC or PVC is simply deleted from the sequence. SDNN is typically measured over 24 hrs and reported in units of ms.
The patients underwent 24 hr ECG monitoring for HRV measurement at three time points after the MI: 3–5 days, 3 months and 6 months. Twenty-four-hour ECG Holter recordings were analysed on a Del Mar Reynolds system (Spacelabs Healthcare, United States). The sampling rate of the ECG was 128 Hz, which ensured 8 ms accuracy for the times of identification of R-peaks of the QRS complex. The quality of the ECG recordings and accuracy of R-peak detection were verified by visual inspection by experienced cardiologists. All normal beats were carefully annotated, so that only normal sinus rhythms were considered in our investigations. Each signal was edited to preserve the RR-intervals between normal-to-normal beats only. Longer segments with wrong data were deleted. Hours with an overall quantity of normal-to-normal beats of less than 95% were excluded from further analysis.
Psychiatric evaluation
Patients were interviewed 24–72 h after admission to ascertain the presence of a major depressive episode (DSM-IV TR criteria). The diagnosis of depression was made on the basis of clinical interview and the intensity of depressive symptoms was appraised with the use of BDI. Subsequent psychiatric evaluation with the use of the same tools was performed after 3 and 6 months from the day of the MI. The evaluations were conducted by an experienced psychiatrist blinded to the HRV results. Depressed patients were not treated pharmacologically due to relatively mild symptoms, but received psychological support.
Statistics
Statistical procedures were performed using statistical software StatsDirect v. 3.1.22. Continuous data are described by both means and standard deviations as well as medians and interquartile ranges (IQR), ordinals by medians and interquartile ranges.
The distribution pattern of all continuous variables was assessed with the Shapiro-Wilk test. All were characterized by a normal distribution. However, because of the small number of groups in comparative analyses, we used non-parametric tests: Mann-Whitney U test for two groups, Kruskal-Wallis for more groups.
Results
Depending on the presence of depression in the first 3–5 days after the MI, the entire group was subdivided into two groups. The depression group included 8 patients (2 women), the group without depression – 14 (including 3 women). Two patients were diagnosed with major depression. The mean age was 55.3 years in the depression group and 54.6 years in the no depression group.
There was a significant increase of SDNN during the observation time in both groups: with depression (D+) and without depression (D-) (Table 1). Pairwise comparison shows significant differences between the analysed time-point except for the difference between 3 and 6 months in the D- group. In the D+ group the only significant difference was found between the 3–5th day and 6th month.
The SDNN value was significantly lower in the D+ group compared to the D- group on the 3-5th day and in the 3rd month. There was no significant difference in the 6th month.
Discussion
In this study of patients with first MI we found that HRV was significantly lower in the depressed group compared to patients without depression, which indicates greater autonomic dysfunction in depressed subjects. We also observed a gradual increase of the HRV time domain measure in both groups, but in the depression group it took longer. No difference between the groups was observed after 6 months from the MI.
These results are consistent with other studies on heart rate variability in depressed patients after myocardial infarction,13,17–22 although there are also contrary results where no differences associated with HRV were found.23 Only some of the mentioned studies had a longitudinal design13,20,21,24 and most of them were not designed to observe HRV changes in relation to the presence of depression during follow-up. Two of them had HRV follow up at two time points with psychiatric evaluation.13,24 To our knowledge, this is the only study with 3 time points of 24 h ECG recording accompanied by direct psychiatric evaluation.
The percentage of patients with MDE detected in our study (ie 23%) is comparable to the published figures of in-patients with ACS (15–20%).25,26 The standard cut off point of 10 in the BDI scale17 was used in other trials17,21,27 and it was proved that patients with mild to moderate depression after MI also have reduced HRV.21 It seems also true for stable CAD patients.28
The association between CAD and MDD has been investigated for more than 20 years. HRV reflects the balance between sympathetic and parasympathetic systems, as increased sympathetic activity or decreased parasympathetic activity can reduce HRV, whereas decreased sympathetic activity, or increased parasympathetic activity will result in increased HRV.29 Low heart rate variability has been proposed as a candidate mechanism linked to both ACS and depression.30–33 Depressed patients have reduced medication compliance34 and have more difficulty coping with the stress of an illness.35,36 HRV has been associated with cognitive deficits, especially in tasks relying on the frontal cortex.37 In addition, reduced HRV has been associated with emotional deficits and in particular with emotional inflexibility.38 Interestingly, neuroimaging meta-analysis found an association between HRV and activity of the major neuronal areas involved in cognitive and emotional flexibility (the anterior cingulate and prefrontal cortex, the insula and the amygdala).39 HRV, therefore, may not only represent an important link between MDD and CAD, but may actually be fundamentally related to the aetiology of the psychiatric symptoms seen in patients with MDD.
Presence of depression is correlated with a worse prognosis after myocardial infarction40,41 and CAD.1,42,43 Decreased HRV is likely to contribute to elevated risk in depressed patients after MI. More studies are needed to clarify biological and psychological mechanisms underlying this interlink. Future studies should focus on identifying treatments that improve both depression and HRV, and determining their effect on survival in this group of patients.44
Study limitations
A limitation of the present study is the small number of participants and no data on smoking. Another limitation is that many patients received drugs such as beta-blockers, angiotensin converting enzyme (ACE) inhibitors, benzodiazepines, and opiates, which possibly influenced the HRV. However, in our study group, the distribution of patients receiving these drugs was similar in all subgroups and the HRV was not significantly affected by these drugs.
This study results are limited to the population free of comorbid diabetes mellitus and other endocrinological conditions which could influence cortisol values measured in another part of this study.14
Conclusion
Depression is a common psychiatric disorder in patients after myocardial infarction. Presence of depression after the MI is associated with a significant decrease of the time domain HRV measure (SDNN) and with its slower increase during at least a three months period. The observation supports the concept that depression increases the autonomic derangement post MI for a longer time.
Ethics
This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
This project was financed by the Research Fund in 2007–2012 as an investigative project (agreement number: 2821/B/P01/2007/33) and by the Medical University of Gdańsk, Poland (Grant No. ST-02-0039/07/221).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Carney RM, Freedland KE. Depression and heart rate variability in patients with coronary heart disease. Cleve Clin J Med. 2009;76(2):13–17. doi:10.3949/ccjm.76.s2.03
2. Freedland KE, Carney RM. Depression as a risk factor for adverse outcomes in coronary heart disease. BMC Med. 2013;11:131. doi:10.1186/1741-7015-11-131
3. Nemeroff CB, Goldschmidt-Clermont PJ. Heartache and heartbreak – the link between depression and cardiovascular disease. Nat Rev Cardiol. 2012;9:526–539. doi:10.1038/nrcardio.2012.91
4. Kemp AH, Quintana DS, Felmingham KL, Matthews S, Jelinek HF. Depression, comorbid anxiety disorders, and heart rate variability in physically healthy, unmedicated patients: implications for cardiovascular risk. PLoS One. 2012;7(2):e30777. doi:10.1371/journal.pone.0030777
5. Hartmann R, Schmidt FM, Sander C, Hegerl U. Heart rate variability as indicator of clinical state in depression. Front Psychiatry. 2019;9:735. doi:10.3389/fpsyt.2018.00735
6. Koschke M, Boettger MK, Schulz S, et al. Autonomy of autonomic dysfunction in major depression. Psychosom Med. 2009;71:852–860. doi:10.1097/PSY.0b013e3181b8bb7a
7. Kidwell M, Ellenbroek BA. Heart and soul: heart rate variability and major depression. Behav Pharmacol. 2018;29(2 and 3–Spec Issue):152–164. doi:10.1097/FBP.0000000000000387
8. Simula S, Vanninen E, Lehto S, et al. Heart rate variability associates with asymptomatic coronary atherosclerosis. Clin Auton Res. 2014;24(1):31–37. doi:10.1007/s10286-013-0220-z
9. Bonnemeier H, Hartmann F, Wiegand UK, et al. Heart rate variability in patients with acute myocardial infarction undergoing primary coronary angioplasty. Am J Cardiol. 2000;85(7):815–820. doi:10.1016/S0002-9149(99)00873-5
10. Erdogan A, Coch M, Bilgin M, et al. Prognostic value of heart rate variability after acute myocardial infarction in the era of immediate reperfusion. Herzschrittmacherther Elektrophysiol. 2008;19(4):161–168. doi:10.1007/s00399-008-0024-3
11. Ortak J, Weitz G, Wiegand UK, et al. Changes in heart rate, heart rate variability, and heart rate turbulence during evolving reperfused myocardial infarction. Pacing Clin Electrophysiol. 2005;28(Suppl 1):227–232. doi:10.1111/j.1540-8159.2005.00015.x
12. Sunbul EA, Sunbul M, Gulec H. The impact of major depression on heart rate variability and endothelial dysfunction in patients with stable coronary artery disease. Gen Hosp Psychiatry. 2017;44:4–9. doi:10.1016/j.genhosppsych.2016.10.006
13. de Guevara MSL, Schauffele SI, Nicola-Siri LC, et al. Worsening of depressive symptoms 6 months after an acute coronary event in older adults is associated with impairment of cardiac autonomic function. J Affect Disord. 2004;80:257–262. doi:10.1016/S0165-0327(03)00105-8
14. Wilkowska A, Rynkiewicz A, Wdowczyk J, Landowski J. Morning and afternoon serum cortisol level in patients with post-myocardial infarction depression. Cardiol J. 2017;24.
15. First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV). Washington, D.C.: American Psychiatric Press, Inc.; 1996.
16. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571.
17. Martens EJ, Nyklícek I, Szabó BM, Kupper N. Depression and anxiety as predictors of heart rate variability after myocardial infarction. Psychol Med. 2008;38(3):375–383. Epub 2007 Nov 8. doi:10.1017/S0033291707002097
18. Guinjoan SM, de Guevara MS, Correa C, et al. Cardiac parasympathetic dysfunction related to depression in older adults with acute coronary syndromes. J Psychosom Res. 2004;56(1):83–88. doi:10.1016/S0022-3999(03)00043-6
19. Catipovic´-Veselica K, Galic´ A, Jelic´ K, et al. Relation between major and minor depression and heart rate, heart-rate variability, and clinical characteristics of patients with acute coronary syndrome. Psychol Rep. 2007;100(3 Pt 2):1245–1254. doi:10.2466/PR0.100.3.1245-1254
20. Carney RM, Blumenthal JA, Freedland KE, et al. Low heart rate variability and the effect of depression on post-myocardial infarction mortality. Arch Intern Med. 2005;165(13):1486–1491. doi:10.1001/archinte.165.13.1486
21. Drago S, Bergerone S, Anselmino M, et al. Depression in patients with acute myocardial infarction: influence on autonomic nervous system and prognostic role. Results of a five-year follow-up study. Int J Cardiol. 2007;115(1):46–51. doi:10.1016/j.ijcard.2006.04.029
22. van Den Berg MP, Spijkerman TA, van Melle JP, et al. Depression as an independent determinant of decreased heart rate variability in patients’ post myocardial infarction. Neth Heart J. 2005;13(5):165–169.
23. Frasure-Smith N, Lespérance F, Irwin MR, Talajic M, Pollock BG. The relationships among heart rate variability, inflammatory markers and depression in coronary heart disease patients. Brain Behav Immun. 2009;23(8):1140–1147. doi:10.1016/j.bbi.2009.07.005
24. Glassman AH, Bigger JT, Gaffney M, Van Zyl LT. Heart rate variability in acute coronary syndrome patients with major depression: influence of sertraline and mood improvement. Arch Gen Psychiatry. 2007;64(9):1025–1031. doi:10.1001/archpsyc.64.9.1025
25. Lichtman JH, Bigger JT
26. Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations – a scientific statement from the American Heart Association. Circulation. 2014;129:1350–1369. doi:10.1161/CIR.0000000000000019
27. Carney RM, Blumenthal JA, Stein PK, et al. Depression, heart rate variability, and acute myocardial infarction. Circulation. 2001;104:2024–2028. doi:10.1161/hc4201.097834
28. Stein PK, Domitrovich PP, Kleiger RE, Schechtman KB, Rottman JN. Clinical and demographic determinants of heart rate variability in patients post myocardial infarction: insights from the cardiac arrhythmia suppression trial (CAST). Clin Cardiol. 2000;23:187–194. doi:10.1002/clc.4960230311
29. Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol. 2010;141:122–131. doi:10.1016/j.ijcard.2009.09.543
30. Harris PR, Sommargren CE, Stein PK, Fung GL, Drew BJ. Heart rate variability measurement and clinical depression in acute coronary syndrome patients: narrative review of recent literature. Neuropsychiatr Dis Treat. 2014;10:1335–1347. doi:10.2147/NDT.S57523
31. Stapelberg NJ, Hamilton-Craig I, Neumann DL, Shum DH, McConnell H. Mind and heart: heart rate variability in major depressive disorder and coronary heart disease – a review and recommendations. Aust N Z J Psychiatry. 2012;46:946–957. doi:10.1177/0004867412444624
32. Taylor CB. Depression, heart rate related variables and cardiovascular disease. Int J Psychophysiol. 2010;78:80–88. doi:10.1016/j.ijpsycho.2010.04.006
33. Thayer J, Lane R. The role of vagal function in the risk for cardiovascular disease and mortality. Biol Psychol. 2007;74:224–242. doi:10.1016/j.biopsycho.2005.11.013
34. Keller MB, Hirschfeld RMA, Demyttenaere K, Baldwin DS. Optimizing outcomes in depression: focus on antidepressant compliance. Int Clin Psychopharmacol. 2002;17:265–271. doi:10.1097/00004850-200211000-00001
35. Kronish IM, Ross JS, Zhao H, Muntner P. The impact of hospitalization for acute myocardial infarction on adherence to statins among older adults. Circ Cardiovasc Qual Outcomes. 2016;9:364–371. doi:10.1161/CIRCOUTCOMES.115.002418
36. Gehi A, Haas D, Pipkin S, Whooley MA. Depression and medication adherence in outpatients with coronary heart disease: findings from the heart and soul study. Arch Intern Med. 2005;165(21):2508–2513. doi:10.1001/archinte.165.21.2508
37. Ottaviani C, Watson DR, Meeten F, Makovac E, Garfinkel SN, Critchley H. Neurobiological substrates of cognitive rigidity and autonomic inflexibility in generalized anxiety disorder. Biol Psychol. 2016;119:31–41. doi:10.1016/j.biopsycho.2016.06.009
38. Balzarotti S, Biassoni F, Colombo B, Ciceri MR. Cardiac vagal control as a marker of emotion regulation in healthy adults: a review. Biol Psychol. 2017;130:54–66. doi:10.1016/j.biopsycho.2017.10.008
39. Vargas ER, Soros P, Shoemaker JK, Hachinski V. Human cerebral circuitry related to cardiac control: a neuroimaging meta-analysis. Ann Neurol. 2016;79:709–716. doi:10.1002/ana.24642
40. Bush DE, Ziegelstein RC, Tayback M, et al. Even minimal symptoms of depression increase mortality risk after acute myocardial infarction. Am J Cardiol. 2001;88:337–341. doi:10.1016/S0002-9149(01)01675-7
41. Carney RM, Blumenthal JA, Catellier D, et al. Depression as a risk factor for mortality after acute myocardial infarction. Am J Cardiol. 2003;92:1277–1281.
42. Stein PK, Domitrovich PP, Huikuri HV, Kleiger RE; Cast Investigators. Traditional and nonlinear heart rate variability are each independently associated with mortality after myocardial infarction. J Cardiovasc Electrophysiol. 2005;16:13–20. doi:10.1046/j.1540-8167.2005.04358.x
43. Herrmann C, Brand-Driehorst S, Buss U, Ruger U. Effects of anxiety and depression on 5-year mortality in 5,057 patients referred for exercise testing. J Psychosom Res. 2000;48:455–462. doi:10.1016/S0022-3999(99)00086-0
44. Carney RM, Freedland KE, Stein PK, Skala JA, Hoffman P, Jaffe AS. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med. 2000;62(5):639–647. doi:10.1097/00006842-200009000-00007
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.