Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Hearing status in patients with vitiligo
Authors Rahimi H, Mozafari N ![]() , Bastaninejad S
, Bastaninejad S ![]() , Tehranchinia Z, Samani NA
, Tehranchinia Z, Samani NA
Received 9 January 2019
Accepted for publication 10 April 2019
Published 21 June 2019 Volume 2019:12 Pages 445—450
DOI https://doi.org/10.2147/CCID.S201012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Hoda Rahimi,1 Nikoo Mozafari,1 Shahin Bastaninejad,2 Zohreh Tehranchinia,1 Nourullah Aghaebrahimi Samani2
1Skin Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Otorhinolaryngology Research Center, Tehran University of Medical Sciences, Tehran, Iran
Background: Vitiligo is an acquired disorder characterized by depigmented macules and patches that result from a progressive loss of functional melanocytes. During embryogenesis, precursor cells of melanocytes (melanoblasts) migrate not only to the epidermis and hair follicles but also to the leptomeninges, uveal tract of the eye, and inner ear. Thus, it has been proposed that these organs may be involved in vitiligo, as well.
Objective: This study was designed to evaluate the frequency and characteristics of hearing loss by means of audiometry and distortion product otoaucostic emission (DPOAE) in patients with vitiligo.
Methods: Fifty-three patients with vitiligo and 52 age- and sex-matched healthy subjects were enrolled in this case–control study. After a complete otological examination, comprehensive audiological evaluations including pure tone audiometry (PTA) and DPOAE were performed for all participants and the results were compared between the two groups.
Results: Neither PTA nor DPOAE showed significant difference between the two groups in any of the evaluated frequencies (0.75–8 KHz). Furthermore, in patient group, there was no association between PTA/DPOAE and age, gender, duration of the disease, presence of halo nevus, type of vitiligo, extent of involvement, and positive family history of vitiligo.
Conclusion: Vitiligo patients have normal hearing status.
Keywords: vitiligo, hearing, hypoacusis, OAE, melanocyte
Introduction
Vitiligo is an acquired disorder characterized by depigmented macules and patches that result from a progressive loss of functional melanocytes.1 This disorder affects approximately 0.5–2% of the general population worldwide with no gender or race predominance. It may appear at any age; however, the average age of onset is almost 20 years.2 The precise etiology of vitiligo is still unknown, but several hypotheses, including autoimmunity, cytotoxicity, neural-chemical mediators, and free radicals, have been proposed to date.1 Regardless of the etiology, the final outcome of this disorder is the destruction of the melanocytes. This destruction may occur not only in the skin, but also in other organs that contain melanocytes, including the uveal tract and the retinal pigment epithelium, the inner ear, and the leptomeninges.3,4
The inner ear contains many melanocytes, especially in the base of the cochlea, which is responsible for hearing high frequencies.5 Melanin is believed to have several roles in the inner ear. It can bind to ototoxic drugs and inhibit their adverse effects on the cochlea.6 Many authors have also reported that melanocytes of the inner ear can protect the cochlea against various stresses, especially loud noise.7,8 Melanocytes are also essential for creating endolymphatic potential, which is very important for cochlear hair cell function and normal hearing.8,9
Otoacoustic emissions (OAEs) are sounds produced by the outer hair cells (OHC) of the cochlea. The existence of normal OAEs is an indicator of healthy OHCs with normal function and other essential structures, such as stria vascularis. Abnormal OAEs reveal the dysfunction of OHCs and consequently the dysfunction of the cochlea.10 Distortion product otoacoustic emissions (DPOAEs) are a section of OAEs. The evaluation of DPOAEs is an easy, prompt, non-invasive technique to determine cochlear function, directly. Demonstrating even an asymptomatic dysfunction of the cochlea in its early stages is a major advantage of this method.11,12
Based on this belief that the destruction of melanocytes may cause hearing abnormalities, several studies have been planned to evaluate hearing loss in vitiligo,13 most of which have reported only audiological and brain stem auditory evoked responses. To our knowledge, only few studies have assessed OAEs.13 The present research, therefore, aimed to evaluate the frequency and characteristics of hearing loss using audiometry and DPOAE in patients with vitiligo.
Methods
Fifty-three patients (20 males, 33 females) with vitiligo and 52 age- and sex-matched healthy subjects were enrolled in this case–control study. Those with a history or evidence of definite otologic diseases (eg, chronic otitis media or tympanic perforation), chronic noise exposure, positive family history of hearing loss, ototoxic drug intake and vascular, neurological, autoimmune or metabolic diseases were excluded. The study protocol was approved by the Ethics Committee of the Skin Research Center. The study is being conducted according to the principles of the Declaration of Helsinki. Written consent was obtained from all the participants.
The diagnosis of vitiligo was made clinically by expert dermatologists. The demographic details and clinical characteristics of all patients, including the duration and extension of the disease, the presence of leucotrichia (pylosis) and halo nevi and family history of vitiligo, were recorded. Vitiligo was classified as generalized (disseminated macules), focal (one or more macules in one area), and acrofacial (involvement of the face or distal parts of the extremities). The vitiligo patients were subdivided into a group with active and a group with stable disease, depending on whether new lesions had appeared on their skin within the last six months. The percentage of the body surface area (BSA) involved by the disease was calculated using the rule of nines. After a complete otological examination to exclude patients with evidence of other otologic diseases, a comprehensive audiological evaluation including pure tone audiometry (PTA) and DPOAE was also performed for all the participants by the same audiologist, who was blinded to the project.
(PTA)
Pure tone thresholds were determined for each ear separately at frequencies of 750, 1000, 1500, 2000, 3000, 4000, 6000, and 8000 Hz for air conduction using a pure tone audiometer (Capella; Otodynamics Ltd, Herts, UK) in a silent standard cabin. The mean threshold level was defined as the mean of hearing levels at frequencies of 2000 and 4000 Hz. The normal value was defined as a hearing level <25 db.
DPOAE
DPOAE was measured using the MADSEN Capella computer-based analyzer (Otometrics A/S Taastrup, Denmark). An asymmetric protocol was used, and L1 was taken as 65-dB sound pressure level (SPL) and L2 as 55-dB SPL, with a frequency ratio (f2/f1) of 1.2. Both the amplitude of response of the distortion product (DP) at f1–f2 and background noise (Ns) were obtained as DP-grams at eight points corresponding to f2 frequencies of 750, 1000, 1500, 2000, 3000, 4000, 6000, and 8000 Hz. The signal-to-noise ratio (SNR) was measured (SNR=DP–Ns) at each of these eight points. If the SNR was ≥3 dB SPL on at least 70% of the tested frequencies, DPOAE was considered normal.
Statistical analysis
The statistical analysis was performed for each ear, rather than for the patients per se, because the results were independent between each individual’s two ears. All the analyses were performed using SPSS software (version 16.0, SPSS Inc., Chicago, IL). P-values less than 0.05 were considered statistically significant. The nonparametric Mann–Whitney test was applied for comparing the quantitative variables, and the χ2 test was used to compare the categorical variables between the study groups.
Results
This study included 53 vitiligo patients (106 ears) and 52 controls (104 ears). The mean±SD of age was 35.09±14.01 years in the case group and 39.63±18.05 years in the control group. There was no statistically significant difference in age and sex between the two groups (Table 1). In the case group, the mean duration of disease was 9.57±7.66 years (range; 0.5–30). Generalized vitiligo was the most common type of vitiligo in the subjects, followed by focal and acrofacial types. Table 1 summarizes the complete demographic and clinical characteristics of the patients.
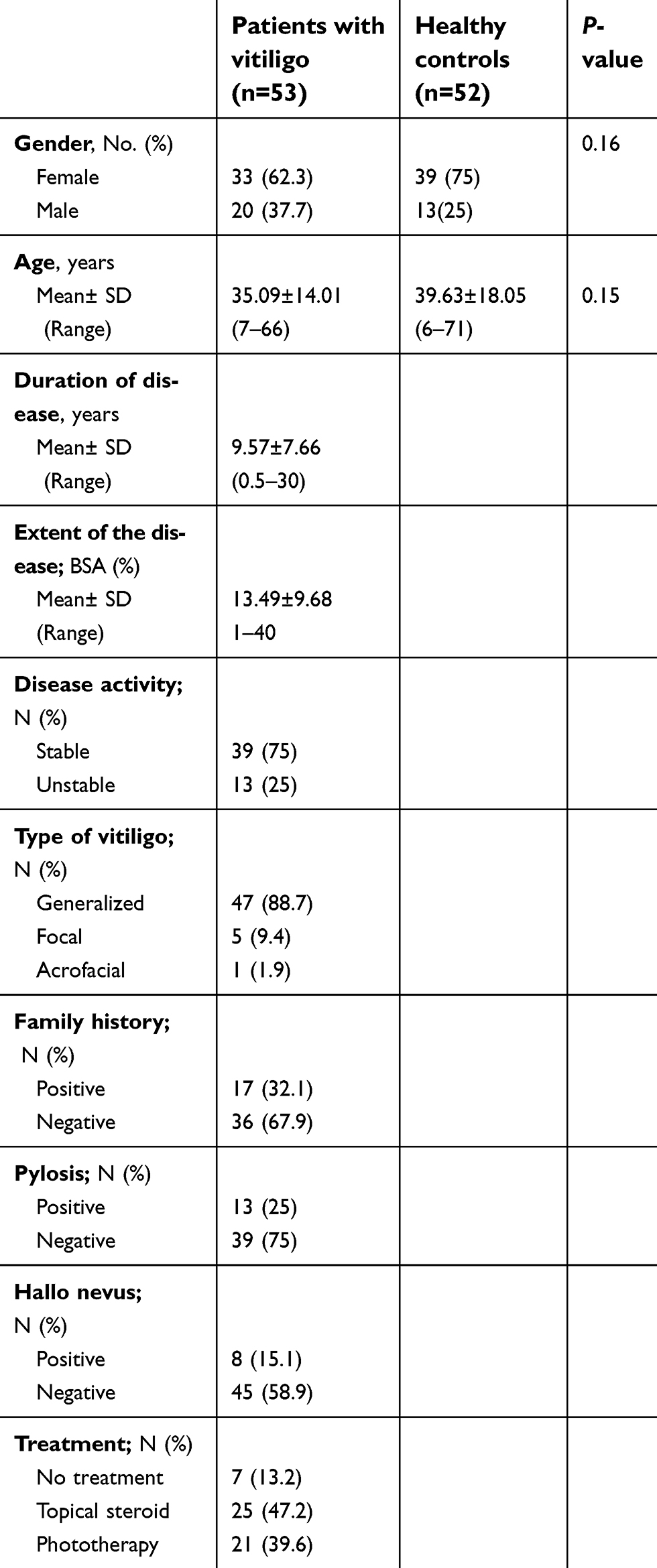 | Table 1 Baseline demographics and clinical characteristics of the study participants |
Comparing the means of pure tone thresholds, we found no significant difference between the case and control groups in any of the evaluated frequencies (Table 2). Furthermore, in the case group, there was no association between PTA and age, sex, duration of the disease, presence of halo nevus, type of vitiligo, extent of the disease, and positive family history of vitiligo.
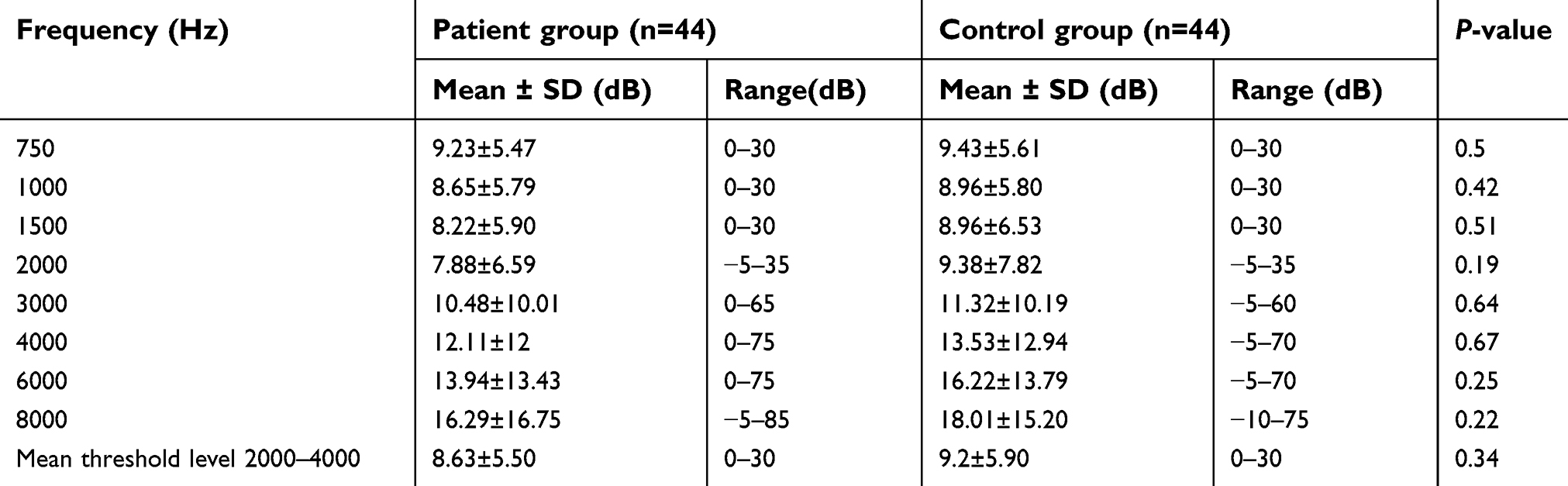 | Table 2 Mean, standard deviation, and range of pure tone thresholds in different frequencies (dB) |
Table 3 shows the DPOAE findings in the patients and controls. Similarly, no statistically significant difference was found in DPOAE between the case and control groups. Moreover, in the case group, there was no correlation between DPOAE and age, gender, duration of the disease, presence of halo nevus, type of vitiligo, extent of the disease, and positive family history of vitiligo.
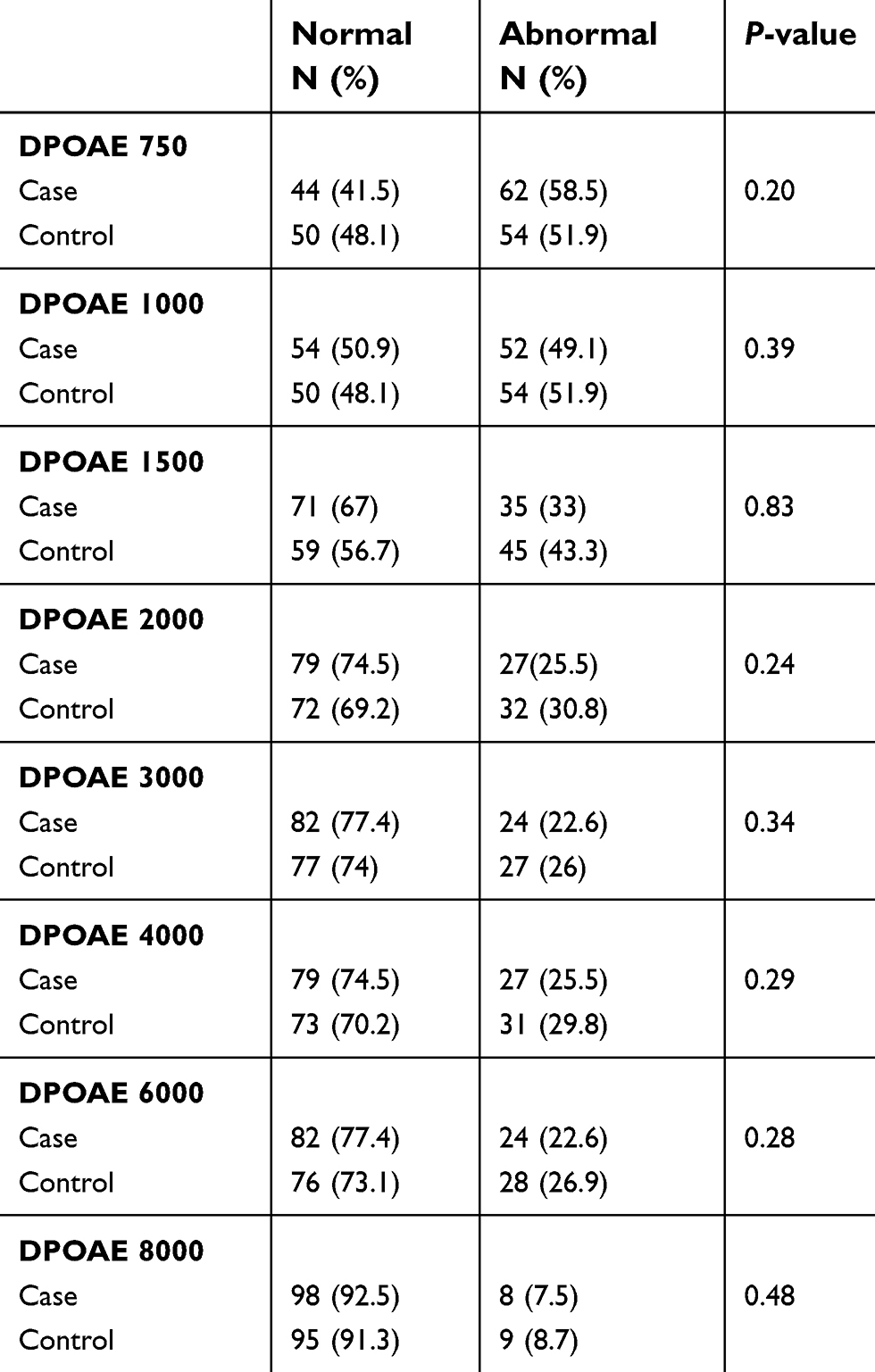 | Table 3 Comparison of distortion product otoacoustic emission (DPOAE) in different frequencies in case and control groups |
Discussion
Melanocytes are neural crest-derived cells. During embryogenesis, precursor cells (melanoblasts) migrate not only to the epidermis and hair follicles, but also to the uveal tract of the eye, leptomeninges, and the inner ear. Although the function of the melanocytes in the inner ear is not thoroughly understood, it has been recently proposed that they potentially play a role in the protection of cochlear hair cells against ototoxic drugs and noise injury, and some studies have been conducted to evaluate hearing status in vitiligo patients.
In the present study, neither PTA nor DPOAE showed significant difference between the two groups in any of the evaluated frequencies. These results are comparable with the results reported by Orecchia et al, which revealed hypoacusis only in 2% of the patients, which was not statistically significant.14 Ozuer et al investigated evoked potentials and PTA in 50 vitiligo patients and 50 healthy controls and found no significant difference between two groups either.15 One of the largest similar studies was performed by Al-Mutairi et al on 197 vitiligo patients; they showed no correlation between vitiligo and hearing loss.16 Nonetheless, a comprehensive review of literature reveals a few more studies on hearing status in vitiligo with diverse and even conflicting results (Table 4). For example, Escalante-Ugalde et al did not find any hearing loss in their vitiligo patients and stated that the dark-skinned composition of their study group might be associated with their better hearing status.17 Conversely, Ardic et al observed a significant hypoacusis in their dark-skinned vitiligo group.5 There seems to be an inconsistency even between the studies which have confirmed the association of audiological abnormalities and vitiligo; the frequency of hypoacusis has been reported from16% to 68% in different studies (Table 4).18–29 It is likely that these inconsistencies are due to the very diverse methodologies used in these studies. For example, only one study presented an exact definition of hearing loss as a difference of ≥25 dB in at least two consecutive frequencies.20 Another explanation for such vast dissimilarities is the different ethnicities and populations included in these studies. Furthermore, some studies did not exclude patients with other systemic diseases and their reported hearing loss may be the result of other diseases coexisting with vitiligo, such as diabetes mellitus and hypothyroidism. In the present study, patients with any systemic diseases were excluded so as to obtain more accurate and reliable results. The only common finding of almost all these studies is that the vitiligo patients reported to show audiological disturbances were asymptomatic.13 Therefore, it appears that even if any audiological changes occur in vitiligo patients, they are of no clinical significance and may be of more interest to biologists and physiologists. It should be noted, however, that no study had evaluated the presence of melanocytes in the inner ear of vitiligo patients directly, and definite evidence is still missing on melanocyte destruction in the inner ear of vitiligo patients. Abad et al also failed to find any melanocyte-derived autoantigen in their vitiligo patients with overt hearing loss.21
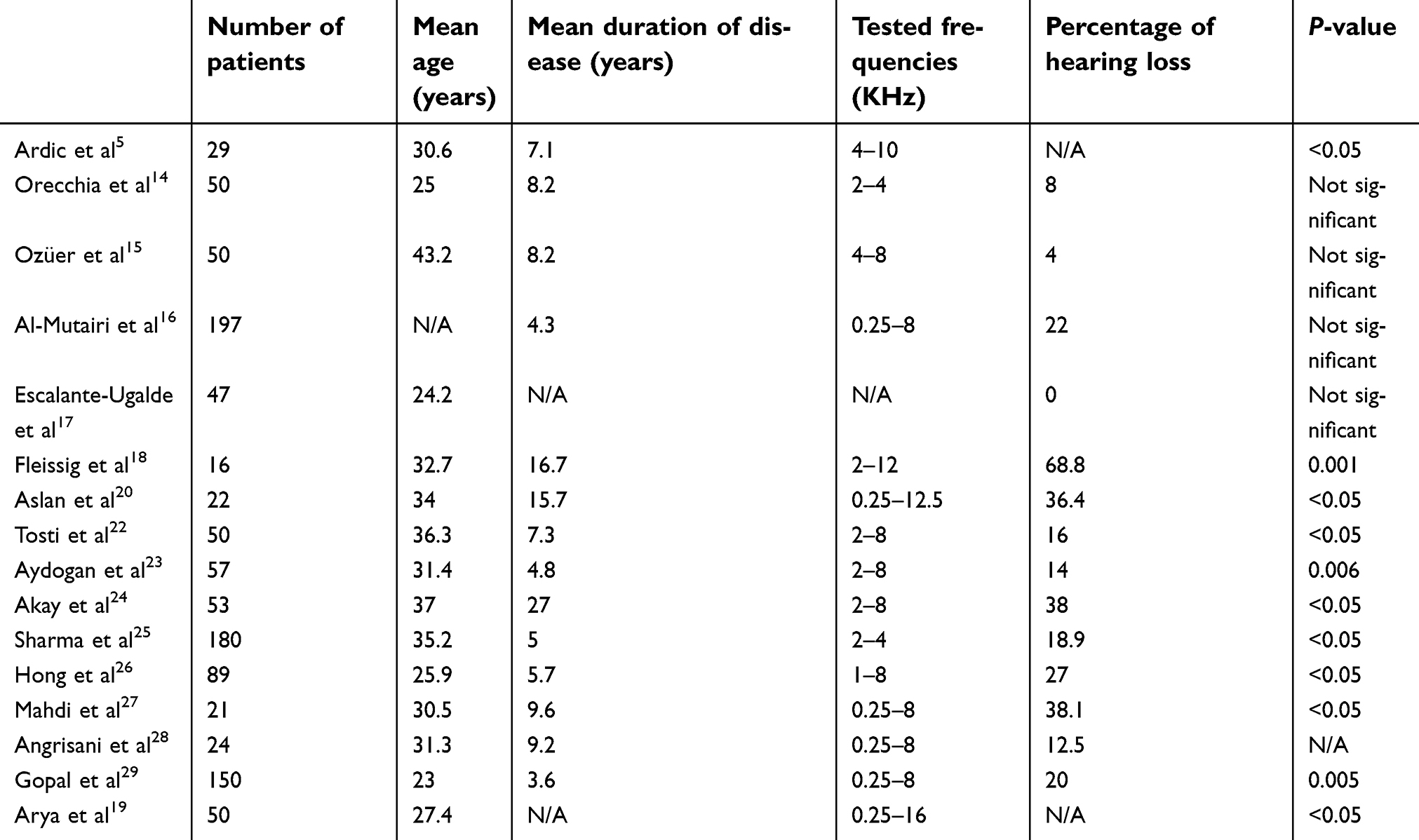 | Table 4 Features of studies about hearing loss in vitiligo |
The present study found no correlation between hypoaucosis and age, gender, duration of the disease, presence of halo nevus, type of vitiligo, extent of the disease and positive family history of vitiligo. Table 5 summarizes the results of other studies concerning these factors.
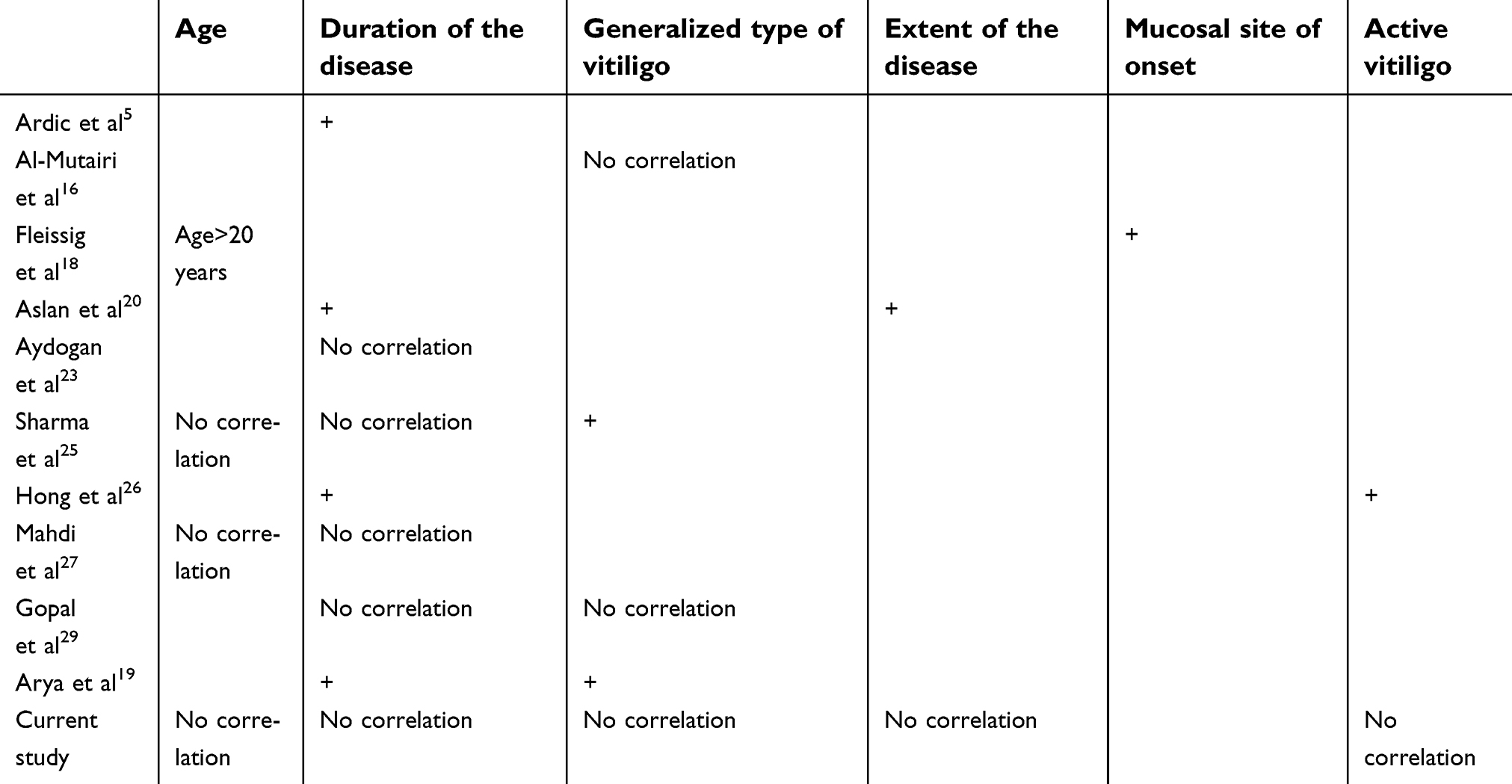 | Table 5 Correlation of clinical characteristics of vitiligo patients with hypoacusis |
The main limitation of the present study was its relatively small sample size.
Conclusion
Obtaining accurate results about the hearing status of patients with vitiligo requires large multi-centric and multi-ethnicity studies conducted with standard methodologies. Also, the direct evaluation of the presence or absence of melanocytes in the inner ear of vitiligo patients (eg, by postmortem histopathological studies) could be of great value.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mirnezami M, Rahimi H. Serum zinc level in patients with vitiligo: a case-control study. Indian J Dermatol. 2018;63;227–230.
2. Zokaei S, Farhud DD, Keykhaei M, et al. Cultured epidermal melanocyte transplantation in vitiligo: a review article. Iran J Public Health. 2019;3:388–399.
3. Goldgeie MH, Klein LE, Klein-Angerer S, et al. The distribution of melanocyte in the leptomeninges of the human brain. J Invest Dermatol. 1984;82:235–238.
4. Araki S, Mizuta K, Takeshita T, et al. Degeneration of the stria vascularis during development in melanocyte deficient mutant rats (Ws/Ws rats). Eur Arch Otorhinolaryngol. 2002;259:309–315.
5. Ardiç FN, Aktan S, Kara CO, Sanli B. High-frequency hearing and reflex latency in patients with pigment disorder. Am J Otolaryngol. 1998;19:365–369.
6. Conlee JW, Bennett ML, Creel DJ. Differential effects of gentamicin on the distribution of cochlear function in albino and pigmented guinea pigs. Acta Otolaryngol. 1995;115:367–374.
7. Tachibana M. Sound needs sound melanocytes to be heard. Pigment Cell Res. 1999;12:344–354.
8. Steel KP, Barkway C. Another role for melanocytes: their importance for normal stria vascularis development in the mammalian inner ear. Development. 1989;107:453–463.
9. Nin F, Yoshida T, Sawamura S, et al. The unique electrical properties in an extracellular fluid of the mammalian cochlea; their functional roles, homeostatic processes, and pathological significance. Pflugers Arch. 2016;468:1637–1649. doi:10.1007/s00424-016-1871-0
10. Prieve B, Fitzgerald S. Otoacoustic emissions. In: Katz J, editor. Handbook of Clinical Audiology. Baltimore, MD: Lippincot Williams and Wilkins; 2003:440–460.
11. Brown AM, McDowell B, Forge A. Acoustic distortion product can be used to monitor the effects of chronic gentamicin treatment. Hear Res. 1989;42:143–156. doi:10.1016/0378-5955(89)90140-8
12. Vinck BM, Van Cauwenberge PB, Leroy L, Corthals P. Sensitivity of transient evoked and distortion product otoacoustic emissions to direct effects of noise on the human cochlear. Audiology. 1999;38:44–52. doi:10.3109/00206099909073001
13. De Jong MA, Adelman C, Gross M. Hearing loss in vitiligo: current concepts and review. Eur Arch Otorhinolaryngol. 2017;274:2367–2372. doi:10.1007/s00405-017-4452-8
14. Orecchia G, Marelli MA, Fresa D, Robiolio L. Audiologic disturbances in vitiligo. J Am Acad Dermatol. 1989;21:1317–1318.
15. Ozüer MZ, Sahiner T, Aktan S, Sanli B, Bayramoğlu I. Auditory evoked potentials in vitiligo patients. Scand Audiol. 1998;27:255–258.
16. Al-Mutairi N, Al-Sebeih KH. Late onset vitiligo and audiological abnormalities: is there any association? Indian J Dermatol Venereol Leprol. 2011;77(5):571–576. doi:10.4103/0378-6323.84059
17. Escalante-Ugalde C, Poblano A, Montes de Oca E, et al. No evidence of hearing loss in patients with vitiligo. Arch Dermatol. 1991;127:1240. doi:10.1001/archderm.1991.01680070142026
18. Fleissig E, Gross M, Ophir I, et al. Risk of sensorineural hearing loss in patients with vitiligo. Audiol Neurootol. 2013;18:240–246. doi:10.1159/000350337
19. Arya R, Kumar Munjal S, Panda NK, Prasad D. Audiological and electrophysiological changes in patients with vitiligo. Indian J Otolaryngol Head Neck Surg. 2016;68:417–423. doi:10.1007/s12070-015-0889-5
20. Aslan S, Serarslan G, Teksoz E, Dagli S. Audiological and transient evoked otoacoustic emission findings in patients with vitiligo. Otolaryngol Head Neck Surg. 2010;142:409–414. doi:10.1016/j.otohns.2009.11.007
21. Abad S, Wieërs G, Colau D, et al. Absence of recognition of common melanocytic antigens by T cells isolated from the cerebrospinal fluid of a Vogt-Koyanagi-Harada patient. Mol Vis. 2014;20:956–969.
22. Tosti A, Bardazzi F, Tosti G, Monti L. Audiologic abnormalities in cases of vitiligo. J Am Acad Dermatol. 1987;17:230–233.
23. Aydogan K, Turan OF, Onart S, Karadogan SK, Tunali S. Audiological abnormalities in patients with vitiligo. Clin Exp Dermatol. 2006;31:110–113. doi:10.1111/j.1365-2230.2005.02004.x
24. Akay BN, Bozkir M, Anadolu Y, Gullu S. Epidemiology of vitiligo, associated autoimmune diseases and audiological abnormalities: ankara study of 80 patients in Turkey. J Eur Acad Dermatol Venereol. 2010;24:1144–1150. doi:10.1111/j.1468-3083.2010.03605.x
25. Sharma L, Bhawan R, Jain RK. Hypoacusis in vitiligo. Indian J Dermatol Venereol Leprol. 2004;70:162–164.
26. Hong CK, Lee MH, Jeong KH, Cha CI, Yeo SG. Clinical analysis of hearing levels in vitiligo patients. Eur J Dermatol. 2009;19:50–56. doi:10.1684/ejd.2008.0563
27. Mahdi P, Rouzbahani M, Amali A, Rezaii Khiabanlu S, Kamali M. Audiological manifestations in vitiligo patients. Iran J Otorhinolaryngol. 2012;24:35–40.
28. Angrisani RM, Azevedo MF, Pereira LD, et al. A study on otoacoustic emissions and supression effects in patients with vitiligo. Braz J Otorhinolaryngol. 2009;75:111–115.
29. Gopal KV, Rama Rao GR, Kumar YH, Appa Rao MV, Vasudev P. Vitiligo: a part of a systemic autoimmune process.Indian. J Dermatol Venereol Leprol. 2007;73:162–165. doi:10.4103/0378-6323.32710
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.