Back to Journals » Risk Management and Healthcare Policy » Volume 14
Healthcare Workers’ Emotions, Stressor Experiences and Coping Strategies During the COVID-19 Pandemic in Vietnam
Authors Thai TT ![]() , Nguyen TH
, Nguyen TH ![]() , Pham PTT
, Pham PTT ![]() , Bui HHT, Bui TNM
, Bui HHT, Bui TNM
Received 1 June 2021
Accepted for publication 7 October 2021
Published 11 October 2021 Volume 2021:14 Pages 4281—4291
DOI https://doi.org/10.2147/RMHP.S322929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Truc Thanh Thai, 1 Thinh Huu Nguyen, 2 Phuong Thu Thi Pham, 3 Han Hy Thi Bui, 4 Tam Ngoc Minh Bui 2
1Faculty of Public Health, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 2Training and Scientific Research Department, University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam; 3Hospital for Rehabilitation - Occupational Diseases at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 4Woolcock Institute of Medical Research, Hanoi, Vietnam
Correspondence: Truc Thanh Thai
Faculty of Public Health, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
Tel +84 908 381 266
Email [email protected]
Tam Ngoc Minh Bui
Training and Scientific Research Department, University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam
Tel +84 906 951 668
Email [email protected]
Purpose: Healthcare workers (HCWs) are a crucial resource in the battle against the COVID-19 pandemic but are vulnerable to both SARS-CoV-2 infection and negative psychological consequences. This study evaluated HCWs’ emotions, stressor experiences and coping strategies during the pandemic.
Methods: A cross-sectional study was conducted among HCWs at the University Medical Center in Ho Chi Minh City. The questionnaire was adapted from the MERS-CoV Staff Questionnaire to measure HCWs’ emotions, stressor experiences and coping strategies during the COVID-19 pandemic.
Results: Among the 1423 participants eligible in the data analysis, the majority were female (71.1%) with a mean age of 34.2 (standard deviation 7.8) years. While most participants reported that they did their job because of their professionalism and duty as HCWs (87.4%), a high number reported feeling nervous and scared (86.0%). Most participants reported worry about transmitting SARS-CoV-2 to their families or friends (76.6%) and concern that a small mistake or lapse in concentration could infect themselves and others (76.7%). The most common coping strategies were following strict personal protective measures (95.3%), avoiding going out (92.5%) and reading about SARS-CoV-2 (92.3%). Females who had a higher educational level and less than 5-years work experience and those who worked at clinical departments and subclinical departments were more vulnerable.
Conclusion: This study indicates an urgent need for psychological support for HCWs, especially for those at high risk of having stress. Interventions and support should utilize psychological resources and approaches effectively to adapt to the new situation during the COVID-19 pandemic.
Keywords: stressor experience, coping strategy, motivational factors, health care worker, COVID-19
A Letter to the Editor has been published for this article.
Introduction
Since the first cases of the new coronavirus (SARS-CoV-2) were reported in China in late December 2019, the COVID-19 pandemic has spread to over 190 countries/regions with more than 160 million confirmed cases and 230.000 deaths in late 2020. During the pandemic, healthcare workers (HCWs) are among the most important resources for managing the crisis. However, the nature of their work leaves them vulnerable to becoming infected with SARS-CoV-2 and experiencing negative psychological consequences. In China, 3.387 HCWs were infected with SARS-CoV-2 and 22 deaths were reported by late February, 2020.1 In the US, about 9.2 thousand HCWs contracted SARS-CoV-2 and 27 had died.2 An emergency department doctor in the US has committed suicide because of the intense work pressure experienced during the COVID-19 pandemic.3 Many researchers have suggested that worry and fear about the COVID-19 may be more harmful and damaging than the physical effects of the disease.4–6 Investigations of the impact of COVID-19 on HCWs’ mental health have been reported in many countries. A recent systematic review and meta-analysis of 38 studies in 19 countries revealed that about 40% of HCWs experienced anxiety, depression or distress during the pandemic.7 However, little is known about the particular stressors HCWs experience and the coping strategies HCWs employ. Research from Saudi Arabia, India, Taiwan and Canada indicates that while HCWs are likely to experience a wide range of stressors, many HCWs lack appropriate coping strategies.8–11 Psychological interventions such as online or phone counselling for individuals or groups have been implemented in many countries to improve physical and mental health for HCWs during the pandemic.12 However, the ability to provide these initiatives has been a challenge in many resource-limited countries.
Vietnam is among the first countries affected by the pandemic with the first case confirmed on January 22, 2020.13 Multiple strategies have been employed in Vietnam to control COVID-19 including intensive medical treatments for confirmed cases and contact tracing investigations. The first generation (F1) who are in close contact with a confirmed SARS-CoV-2 (F0) are tested and quarantined for at least 14 days at quarantine camps.14 Second generation (F2) contacts are required to self-isolate at home and are monitored by primary care professionals. As such, the burden of healthcare services has been increasing due to the need to manage both confirmed cases and contacts. For example, although 270 confirmed cases were reported by May 2020, more than 30,000 people were quarantined and monitored nationwide.15 Given the uncertainty at the time about how COVID-19 can be transmitted, the lack of effective medical treatments for those who become infected with the virus and the absence of vaccines to prevent infection, the fear of becoming infected and severely ill or dying has been a significant concern for HCWs. HCWs are in contact with many patients with a variety of different health conditions, and some of these patients may be infected with COVID-19. This means HCWs have a significant risk of being infected, being quarantined and transmitting SARS-CoV-2 to others, including staff at the hospital and family at home. For example, Bach Mai Hospital has become a hot-spot of SARS-CoV-2 infection in Vietnam, and hundreds of HCWs working there have been quarantined inside the hospital. Given the high level of burnout among HCWs16 and the multiple types of mental health problems17 reported in studies prior to the pandemic, the effect of the COVID-19 pandemic on burnout rates and mental health problems is likely to be even more pronounced in HCWs. However, to date, little is known about the psychological effects of COVID-19 on HCWs in Vietnam and other countries.
Therefore, this study aimed to evaluate the effect of SARS-CoV-2 on HCWs’ emotions, stressor experiences and coping strategies during the COVID-19 pandemic. Findings from this study might be helpful in targeting psychological supports for this population.
Methods
Settings and Study Design
During a two-week period in March and April 2020, a cross-sectional study was conducted at a university hospital in Vietnam. The hospital has approximately 3000 HCWs and provides healthcare services for both inpatients and outpatients throughout Vietnam. There are an average of 8000 visits to the hospital per day. Of the 2003 HCWs who agreed to participate in the survey, 1423 HCWs completed the survey and were included in this analysis.
Study Procedures
All study procedures were approved by the Research Ethics Committee at the University Medical Center Ho Chi Minh City, Vietnam (No: 08/GCN-HDDD). All the participation was voluntary. From an existing list of all staff at the hospital, an invitation email was sent to each individual staff member after a consensus introducing about the study. LimeSurvey, a free and open-source platform, was used to host the online survey. A token was embedded in a unique link with an access code to the online form so that only invited persons could access the survey. The use of the token also ensured each staff member completed the survey only once and thus multiple entry was avoided. Five days after the initial invitation email, a reminder email was sent to those who did not complete the survey.
Measurement
The online questionnaire for this study was adapted from the MERS-CoV Staff Questionnaire8,9 with the replacement of “MERS-CoV” by “SARS-CoV-2” to focus on the COVID-19 pandemic. Our questionnaire contained information about background characteristics, staff emotion during the pandemic, factors causing stress, factors that helped to reduce stress, coping strategies used and motivational factors during the outbreak. Background characteristics included sex, age, highest education completed, profession, number of years working as a HCW, number of years working at the hospital, place of work, marital status and having children.
Staff emotion during the COVID-19 pandemic was measured using 15 questions using a Likert-type rating scale including 0 (not at all), 1 (slightly), 2 (moderately) and 3 (very much). The experience of factors causing stress was measured based on a list of 20 questions/events using 4-point rating scale including 0 (very minimally stressed), 1 (slightly stressed), 2 (moderately stressed), 3 (very much stressed). Perception of factors that helped to reduce stress was evaluated through 14 items on a 4-point scale from 0 (not at all effective) to 3 (extremely effective). Coping strategies were explored using 13 questions/statements based on a 4-point scale including 0=never used, 1=sometimes used, 2=often used and 3=always used. Perception of motivational factors was captured by 10 questions using a Likert-type rating scale from 0 (not important at all) to 3 (extremely important). These measures have been reported to be reliable with Cronbach’s alpha from 0.76 to 0.86.8 This adapted questionnaire was translated into Vietnamese independently by two researchers, and discrepancies were discussed to come up with a final version. A pilot study among a convenient sample of five HCWs was also carried out to double-check the wording of the questionnaire. In the main survey, the questionnaire had good to excellent reliability with Cronbach’s alpha ranging from 0.75 to 0.91.
Data Analysis
To facilitate data analysis, Likert-type scale was dichotomized into yes (score of 1 or above) and no (score of 0). The overall measure of each domain was computed based on the total number of feelings, experiences and strategies measured. t-tests or ANOVA tests were used to compare these overall measures among participants with different characteristics. All statistical tests were two-sided. Type one error rate was set at 0.05.
Results
Among the 1423 participants eligible in the data analysis, the majority were female (71.1%) with a mean age of 34.2 (standard deviation 7.8) years old. Most of the participants had a college (42.2%) or undergraduate degree (39.6%). More than one-fourth of participants were physicians and about one-third were nurses. Approximately half of participants had worked for at least 10 years. The majority worked at clinical departments (63.0%), were married (58.5%) and had children (55.8%) (Table 1).
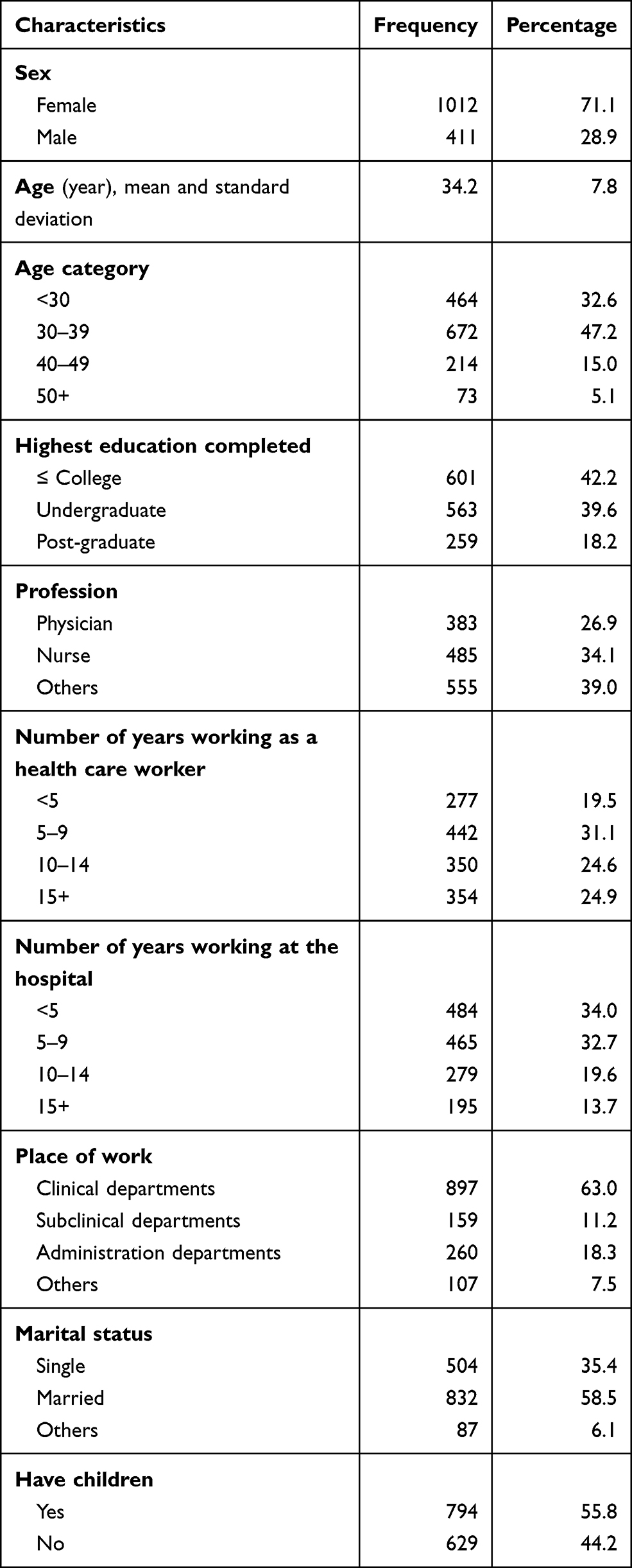 |
Table 1 Background Characteristics of Participants (N=1423) |
Table 2 presents staff's feelings and experiences of factors causing stress during the COVID-19 pandemic. Most participants felt that they did their job because of their professionalism and duty (87.4%). However, a high number of participants reported feeling nervous and scared during the pandemic (86.0%). Most participants felt that special recognition (90.7%) or financial compensation (81.3%) was needed during the outbreak. Very few participants thought of quitting their job (9.9%) or calling in sick (11.0%). For factors causing stress during the pandemic, more than three quarters reported worry about transmitting SARS-CoV-2 to their family or friends (76.6%) and concern that a small mistake or lapse in concentration could infect themself and others (76.7%). A large number of participants experienced stress because they did not know when the pandemic would be under control (69.7%) and when learning of news of new cases of SARS-CoV-2 that were reported in TV/newspaper (71.2%).
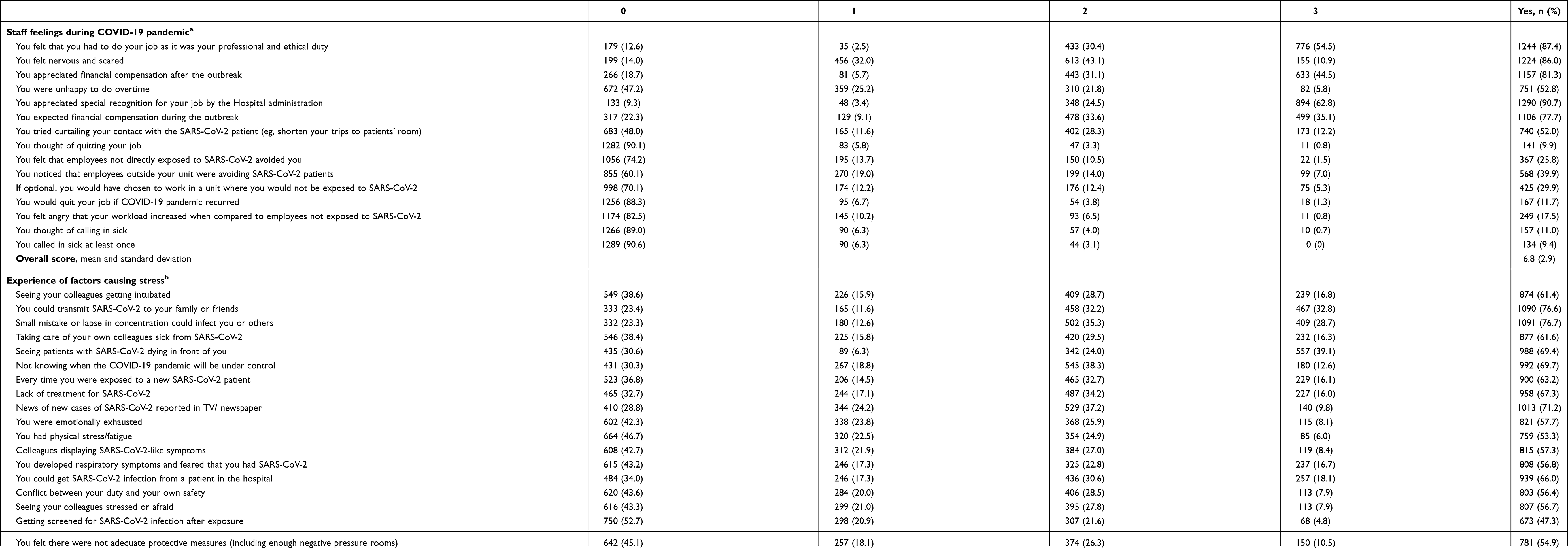 |
Table 2 Staff Feelings and Experience of Factors Causing Stress During COVID-19 Pandemic |
Factors that helped to reduce stress, coping strategies used by staff and their experiences of motivation factors are shown in Table 3. The most common factors that helped to reduce stress were positive attitudes from colleagues (89.9%), none of their fellow staff being infected with SARS-CoV-2 (82.2%), clear guidelines from the hospital for infection prevention (90.4%) and protective equipment provided by the hospital (88.3%). The most common coping strategies included following strict personal protective measures (95.3%), avoiding going out in public places (92.5%), reading about SARS-CoV-2, its prevention and mechanism of transmission (92.3%) and talking to self and motivating one’s self to face the pandemic with a positive attitude (90.9%). Only 13.1% reported venting emotions through crying or screaming to cope with stress. In terms of motivational factors, most participants reported adequate personal protective equipment supplied by the hospital (92.3%), family support (89.8%), available cure or vaccine for the disease (84.1%) and psychiatric help and therapy made available in the workplace would help reduce stress and anxiety (84.8%).
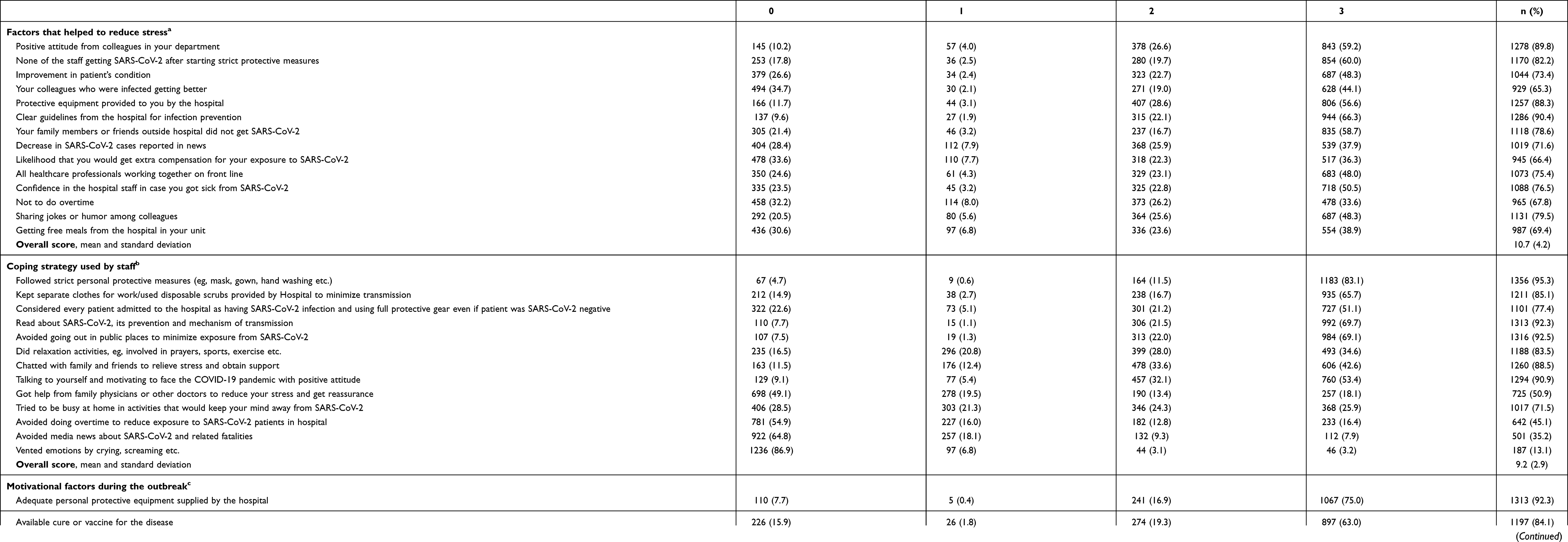 |
Table 3 Factors That Helped to Reduce Stress, Coping Strategies Used by Staff and Experience of Motivation Factor |
Table 4 presents the distribution of feelings, factors causing stress, factors that helped to reduce stress, coping strategies used and motivational factors across participants’ characteristics. Females experienced more factors causing stress and less factors that helped to reduce stress than males. Participants with a higher educational level had a significantly higher number of all feelings and factors measured. Participants who had less than a 5-year working experience reported more factors causing stress but also experienced more factors that helped to reduce stress. Participants who worked at clinical departments and subclinical departments had significantly higher number of stress feelings, factors causing stress and used more strategies to cope with stress during the pandemic. There was no statistically significant association between age, profession, marital status and having children and the five outcomes.
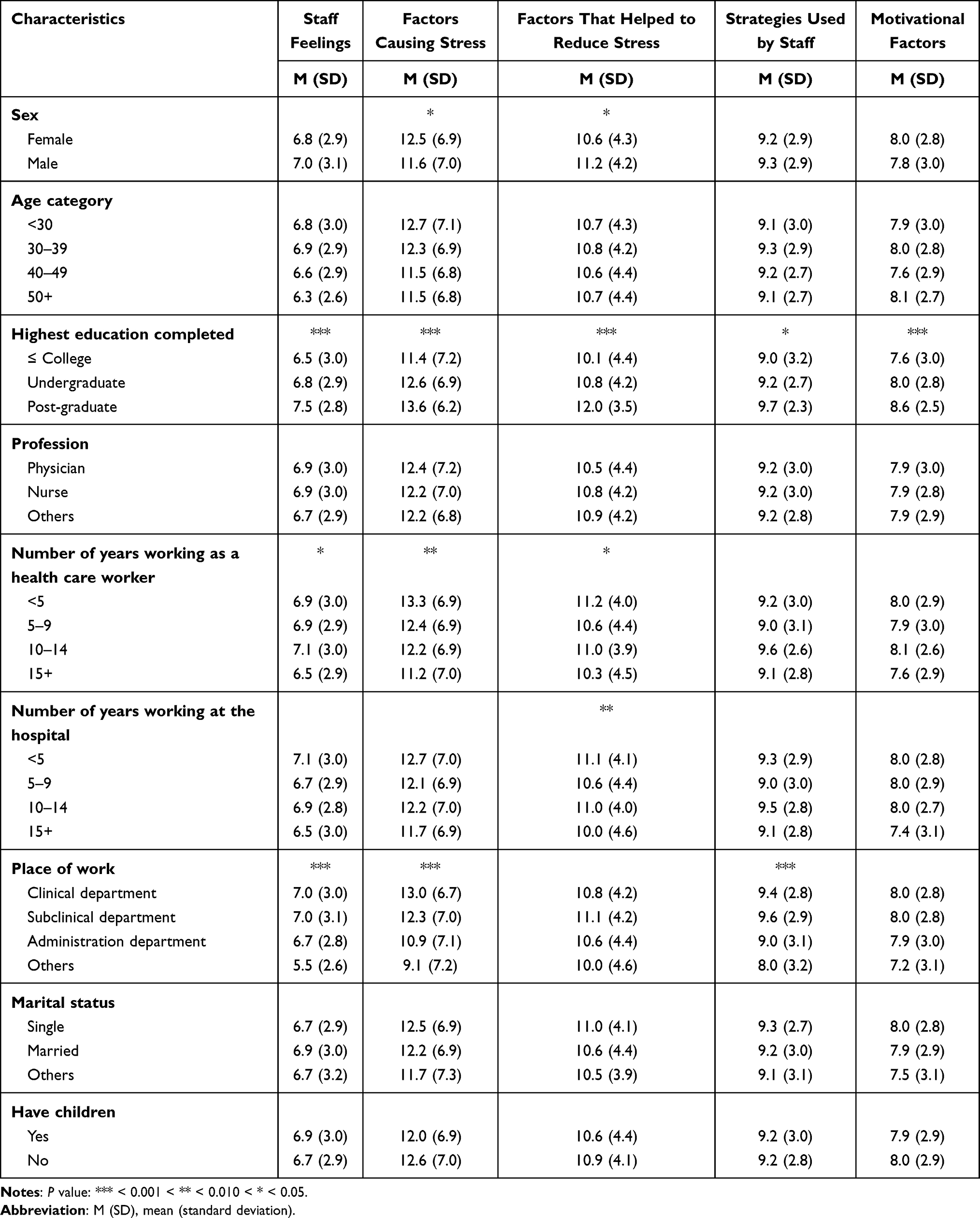 |
Table 4 Distribution of Feelings, Stress and Strategies Used Across Participants’ Characteristics |
Discussion
Our study is among the first in Vietnam to investigate the psychological effects of COVID-19 pandemic among HCWs. We found that almost all participants had the willingness to work during the pandemic because of their professionalism and duty as HCWs. However, a great number of participants (86%) felt nervous and scared due to their fear of being infected and transmitting the virus to their family and friends, as well as not knowing when the COVID-19 pandemic would be under control. These findings are consistent with HCWs in other countries from previous studies. For example, a study among 117 HCWs in Saudi Arabia during the MERS-CoV outbreak8 revealed that while 94% had to do their job as HCWs, 96% felt nervous and scared. A survey among 26 female nurses during the SARS outbreak in 2003 in Taiwan showed that the most prevalent feelings were worrying about endangering coworkers (92.3%) and uncertainty about when the pandemic will be under control (92.3%).9 Lee et al9 also reported a high level of conflict between duty and safety among HCWs in Taiwan. Another qualitative study in Canada showed that while no HCWs refused to perform their duties during the SARS pandemic in 2003, their anxiety and fear were paramount.10 However, these figures are much higher than that reported in a recent study among a convenience sample of 150 healthcare workers in India where 43.3% indicated feeling nervous and scared during the COVID-19 pandemic.11 These findings confirm the important role of the unpredictability and uncertainty of the disease, misinformation from media and social isolation in explaining adverse feelings among HCWs.18 While at present it is not possible to provide HCWs with certainty about when the COVID-19 pandemic will end, the provision of psychological support for HCWs is clearly needed.
In the current study, a diversity of factors causing stress were reported as well as the multiple coping strategies used. Notably, while only 52.8% of HCWs were unhappy to do overtime, this figure was significantly higher in Saudi Arabia and India with 93% and 96% of HCWs having this feeling, respectively.8,11 Moreover, while about 10% thought of quitting their job or calling in sick in our study, HCWs in Saudi Arabia during the MERS-CoV outbreak intended to quit jobs (92%) or to take sick leave (62%). These differences are possibly due to the situation of the study hospitals. Hospitals in both of these two studies are accredited to treat patients with MERS-CoV and SARS-CoV-2 and HCWs are at high risk of contracting coronavirus. However, while our study hospital had no infection cases, there were 40 confirmed cases in the hospital in Saudi Arabia.8 Our findings suggest that higher levels of stress, fear, and actual severe adverse effects of COVID-19 exist in other hospitals in Vietnam where new cases of SARS-CoV-2 were confirmed and admitted. Although psychological support is essential for HCWs at hospitals with confirmed cases, such support should also be available for other hospitals to prevent adverse psychological indirect effects of COVID-19 on the well-being of HCWs.
Despite the high prevalence of stressors, most of our participants reported positive approaches to coping with COVID-19 and very few chose avoidant-coping strategies. Similar to previous studies,8,9,11 the most common coping strategies used included following strict personal protective measures, avoiding going out in public places, reading about SARS-CoV-2, its prevention and mechanism of transmission. In contrast, while only 13% of our participants coped with COVID-19 by venting emotions such as crying and screaming, which is similar in the study by Srivastava et al (10.7%),11 this figure was almost double in the study by Lee et al9 and triple in the study by Khalid et al.8 Our study is also in line with the literature where positive attitudes from colleagues, sufficient protective equipment and clear guidelines provided by the hospital were reported by HCWs as the most important strategic and motivational factors to help them to cope with stress during the pandemic.19 Importantly, although no SARS-CoV-2 case was under care and treatment at the study hospital, nearly 85% indicated the need for psychiatric help and therapy made available in the workplace to help reduce stress and anxiety.
Although it is ideal to provide psychological support for all HCWs, doing so would result in another challenge and burden particularly for resource limited countries. Therefore, identifying those who are at high risk of having psychological problems is an important strategy so that psychological resources can be utilized effectively. In our study, females who had a higher educational level and less than 5-year work experience and those who worked at clinical departments and subclinical departments appeared to be the most vulnerable population. This finding is in line with current literature. For example, a study of 34 hospitals in China, across which 1257 HCWs were exposed to COVID-19 revealed that females had approximately 1.5 to 2.0 times higher odds of having depression, anxiety and distress.20 The level of severity of these conditions was also higher in females. However, it is interesting that while a high level of stress has been consistently reported in female HCWs during the COVID-19 outbreak,20 about three quarters of our participants and in the samples of previous studies were female.8,20 Our findings and others indicate an urgent need for immediate psychological support targeting those who have these risk factors.
There are several implications of our study. Firstly, the COVID-19 pandemic has highlighted substantial gaps in mental health services for HSWs. In Vietnam and possibly other resource-limited countries where mental health receives little attention from health sectors, the lack of such support may lead to both immediate and long-term consequences as observed in previous studies, such as depression, anxiety, suicide and chronic post-trauma psychiatric problems. This in turn reduces the effectiveness of the healthcare system in managing the COVID-19 pandemic. Secondly, while the majority of appropriate healthcare resources have been utilized during the outbreaks such as personal protective equipment, more attention needs to be directed to the provision of psychological support. With regard to the need for social distancing, tele-mental health as suggested by Whaibeh et al21 may be a good option whereby information and communication technologies can be used to deliver psychological support and monitor the early detection of adverse psychological effects among HCWs.
This study has some limitations. First, our study was conducted at a single hospital, which had no cases of COVID-19. This limits the generalization of our findings. It is expected that higher levels of stress might be observed among other hospitals in different settings, particularly hospitals where SARS-CoV-2 cases are being treated. Secondly, while we employed a cross-sectional survey in this study, the nature of stress and coping strategies might be influenced by the real situation of the COVID-19 pandemic. The effect of COVID-19 would be more pronounced in settings where COVID-19 is not under control and there are a high number of confirmed cases and deaths. However, since COVID-19 is unpredictable and effective treatment and vaccines were not available at the time of the study, the findings from our study might be temporary. Mental health surveillance systems and more studies are needed to understand the psychological effects of this pandemic. Moreover, although the scale used in our study is frequently used in similar studies, information about its psychometric properties is limited. Due to resource and time constraints, we were unable to validate this scale in Vietnam. Therefore, the validity of this scale requires further evaluation.
Conclusion
Although positive coping strategies were used, a high level of stress was observed among HCWs in Vietnam even in a hospital with no SARS-CoV-2 infection. However, most HCWs reported a willingness to continue their work because of their professionalism. This study indicates an urgent need for psychological support, especially for those who are more vulnerable during the pandemic. Such interventions and support should utilize psychological resources and approaches to effectively adapt to new situations during the COVID-19 pandemic.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Research Ethics Committee at the University Medical Center Ho Chi Minh City, Vietnam (No.: 08/GCN-HDDD) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors would like to thank the director board at the University Medical Center Ho Chi Minh City for continuous support during the study and all health care workers who participated in this study.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Wang J, Zhou M, Liu F. Exploring the reasons for healthcare workers infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020. doi:10.1016/j.jhin.2020.03.002
2. Burrer SL, de Perio MA, Hughes MM, et al.; Centers for Disease Control and Prevention. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. Morb Mortal Wkly Rep. 2020;69:477–481. doi:10.15585/mmwr.mm6915e6
3. The Guardian. New York ER doctor who treated coronavirus patients dies by suicide. The Guardian. Available from: https://www.theguardian.com/us-news/2020/apr/28/dr-lorna-breen-new-york-er-coronavirus.
4. Ren SY, Gao RD, Chen YL. Fear can be more harmful than the severe acute respiratory syndrome coronavirus 2 in controlling the Corona virus disease 2019 epidemic. World J Clin Cases. 2020;8(4):652–657. doi:10.12998/wjcc.v8.i4.652
5. Kelvin DJ, Rubino S. Fear of the novel coronavirus. J Infect Dev Ctries. 2020;14(1):1–2. doi:10.3855/jidc.12496
6. Asmundson GJG, Taylor S. Coronaphobia: fear and the 2019-nCoV outbreak. J Anxiety Disord. 2020;70:102196. doi:10.1016/j.janxdis.2020.102196
7. Saragih ID, Tonapa SI, Saragih IS, et al. Global prevalence of mental health problems among healthcare workers during the Covid-19 pandemic: a systematic review and meta-analysis. Int J Nurs Stud. 2021;121:104002. doi:10.1016/j.ijnurstu.2021.104002
8. Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin Med Res. 2016;14(1):7–14. doi:10.3121/cmr.2016.1303
9. Lee SH, Juang YY, Su YJ, Lee HL, Lin YH, Chao CC. Facing SARS: psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen Hosp Psychiatry. 2005;27(5):352–358. doi:10.1016/j.genhosppsych.2005.04.007
10. Robertson E, Hershenfield K, Grace SL, Stewart DE. The psychosocial effects of being quarantined following exposure to SARS: a qualitative study of Toronto health care workers. Can J Psychiatry. 2004;49(6):403–407. doi:10.1177/070674370404900612
11. Srivastava A, Srivastava S, Upadhyay R, Gupta R, Jakhar K, Pandey R. Stressor combat strategies and motivating factors among health care service providers during COVID-19 pandemic. Cureus. 2021;13(4):e14726. doi:10.7759/cureus.14726
12. Chen Q, Liang M, Li Y, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4):e15–e16. doi:10.1016/s2215-0366(20)30078-x
13. Phan LT, Nguyen TV, Luong QC, et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N Engl J Med. 2020;382(9):872–874. doi:10.1056/NEJMc2001272
14. Nguyen TA, Cuong QN, Kim ALT, et al. Adapting a TB contact investigation strategy for COVID-19. Int J Tuberc Lung Dis. 2020. doi:10.5588/ijtld.20.0169
15. Vietnam Ministry of Health. Information page about COVID-19. May 02, 2020. Available from: https://ncov.moh.gov.vn/web/guest/trang-chu.
16. Nguyen HTT, Kitaoka K, Sukigara M, Thai AL. Burnout study of clinical nurses in Vietnam: development of job burnout model based on Leiter and Maslach’s theory. Asian Nurs Res. 2018;12(1):42–49. doi:10.1016/j.anr.2018.01.003
17. Tran TTT, Nguyen NB, Luong MA, et al. Stress, anxiety and depression in clinical nurses in Vietnam: a cross-sectional survey and cluster analysis. Int J Ment Health Syst. 2019;13:3. doi:10.1186/s13033-018-0257-4
18. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. 2020;52:102066. doi:10.1016/j.ajp.2020.102066
19. Klein J, Frie KG, Blum K, von Dem Knesebeck O. Psychosocial stress at work and perceived quality of care among clinicians in surgery. BMC Health Serv Res. 2011;11(1):109. doi:10.1186/1472-6963-11-109
20. Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976
21. Whaibeh E, Mahmoud H, Naal H. Telemental health in the context of a pandemic: the COVID-19 experience. Curr Treat Options Psychiatry. 2020;1–5. doi:10.1007/s40501-020-00210-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.