Back to Journals » Patient Preference and Adherence » Volume 15
Health System Responsiveness for HIV/AIDS Treatment and Care Services in Shewarobit, North Shewa Zone, Ethiopia
Authors Asefa G, Atnafu A ![]() , Dellie E
, Dellie E ![]() , Gebremedhin T
, Gebremedhin T ![]() , Aschalew AY, Tsehay CT
, Aschalew AY, Tsehay CT ![]()
Received 7 January 2021
Accepted for publication 25 February 2021
Published 9 March 2021 Volume 2021:15 Pages 581—588
DOI https://doi.org/10.2147/PPA.S300825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Getachew Asefa,1 Asmamaw Atnafu,2 Endalkachew Dellie,2 Tsegaye Gebremedhin,2 Andualem Yalew Aschalew,2 Chalie Tadie Tsehay2
1Shewarobit Primary Hospital, Shewarobit, North Shewa Zone Administration, Amhara National Regional State, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Chalie Tadie Tsehay
University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Email [email protected]
Purpose: Health System Responsiveness is the key objective of the health system used to fulfil patients’ universal legitimate expectations. However, the health system’s responsiveness to HIV/AIDS was not assessed in Ethiopia. Therefore, this study aimed at assessing the health system responsiveness of HIV/AIDS treatment and care services and associated factors in the public health facilities of Shewarobit town, Ethiopia.
Patients and Methods: An institution-based cross-sectional study was employed from 15 February to 15 April 2020 in the public health facilities of Shewarobit town. The data were collected among 416 randomly selected Anti-Retroviral Therapy (ART) users using an interviewer-administered questionnaire. Responsiveness was measured using 27 Likert scale questions across seven responsiveness domains. A binary logistic regression model was fitted. A p-value of less than 0.05 and AOR with a 95% confidence interval (CI) was used to declare the associated factors in the final multivariable logistic regression analysis.
Results: The overall health system responsiveness was 55.3% (95% CI: 50.6– 59.8). High performance of responsiveness was found on confidentiality, respect, and communication domains, whereas poor responsiveness was achieved in prompt attention and choice domains. Participants aged 50+ years (AOR:2.48, 95% CI, 1.12– 5.54), perceived good health (AOR: 3.10, 95% CI: 1.75– 5.48), patients’ satisfaction with care (AOR: 2.98, 95% CI: 1.35– 6.54) and history of visiting traditional healers (AOR: 2.50, 95% CI:1.51– 4.17) were factors associated with health system responsiveness of HIV/AIDS treatment and care services in the study area.
Conclusions: Unacceptable responsive performance was found in choice and prompt attention domains. Participants’ age, perceived health status, history of visiting traditional healers, and patient satisfaction were factors that affect responsiveness in the study area. Thus, providing training, frequent supportive supervision, improving community awareness, and incorporating traditional healers in the modern health system would enhance the health system responsiveness in Ethiopia.
Keywords: responsiveness, HIV/AIDS, health systems, Ethiopia
Background
A health system consists of organizations, people, and activities whose primary purpose is to promote, restore, or maintain health.1,2 Health care provision involves many interrelated processes and interactions between care providers and clients that influence healthcare provision’s patient-centeredness.3 World Health Organization (WHO) has identified three main goals for the health system: improving the health of the population, improving the health system’s responsiveness to the population it serves, and financial protection from catastrophic health expenditure.2
Health system responsiveness (HSR) was introduced in the world health report in 2000 and nowadays it is a well-recognized key objective of national health systems.1,2 HSR is a promising measure of the quality of a health system and focuses on a health care system’s ability to satisfy patients as per the service standards and ethical principles in terms of nonfinancial and non-clinical aspects of health care.4–6 This encompasses autonomy, attention, dignity, choice, confidentiality, communication, amenities, and access to social supports domains, which measure how the healthcare has to be client-centered and to what extent the clients’ legitimate expectations are being met.4,7,8
In Ethiopia, about 722,248 people were living with HIV by the year 2018.9 Most of the deaths are related to poor treatment adherence leading to opportunistic infections,10,11 which can be significantly reduced by maintaining patients’ universal expectations.3,12–14 The recent universal scale-up of HIV/AIDS treatment and care services (HATCS) has saved many lives.11,15 Medical conditions like HIV/AIDS require lifelong care; the quality of care should meet clients’ expectations to encourage treatment adherence and achieve better health outcomes.16,17
The WHO survey highlighted that prompt attention, dignity, and communication had the highest importance-rates across 35 to 41 countries, whereas the summary of the responsiveness-score highlighted a large variability worldwide.2,18–21 It is higher in developed counties such as European countries; however, HSR in Africa remains low.7,22–25 In Ethiopia, lower HSR performance was observed in the choice, attention, and autonomy domains of HATCS.26
Studies showed that healthcare facilities lack adequate financing, trained and motivated health workforce, and essential logistics. Besides, poor quality of care, socio-demographic and cultural factors (stigma and discrimination), the inability of the health systems to create better care climates, patients’ experience of visiting traditional healers, the type of health facility in which the service is provided, the direct and indirect cost of treatment and comorbidity status and other factors contribute for the poor responsiveness performance in Ethiopia.21,22,27–32 The recent evidence has shown that the higher the HSR, the greater the chances of treatment successes, meeting the clients’ expectations, and contentment with the services.10,25
However, empirical data are limited in Ethiopia. Therefore, this study aimed at assessing the performance of HSR on HATS and associated factors among patients who were on ART in Shewarobit town public health facilities. Further, it is believed that the evidence generated from this study would give a strong suggestion to the concerned bodies and trigger the policymakers in the field to design evidence-based strategies to tackle the burden of the problem.
Patients and Methods
Study Design and Settings
An institution-based cross-sectional study was employed from 15 February to 15 April 2020 in the public health facilities of Shewarobit town, Ethiopia. Shewarobit town is under Kewet district, north Shewa zone with 9 kebeles (the smallest administrative units). The town is located at 225kms in the north of Addis Ababa, the capital of Ethiopia. Based on the 2007 national census report, about 17,575 (14.85%) of the district’s population was residing in the Shewarobit town.33 The town had one governmental, and one private hospital, one health center, 6 private medium clinics, and 10 pharmacies. The primary hospital and health center have been providing HIV/AIDS care, treatment, and support services for 1646 seropositive patients (1436 at the health center and 210 at the hospital). Of these, 1589 (96.5%) individuals were over 18 years of age.34
Population and Sampling Procedures
All people living with HIV in Shewarobit town were the source population, whereas individuals who were attending the hospital and health center were the study population. Patients aged older than 18 years who were on treatment for at least six months in Shewarobit primary hospital and health center were included in the study, whereas patients who were critically ill and unable to communicate were excluded from the study.
The sample size was determined using single population proportion formula (n= (z α/2)2 *p(1-p)/d2) considering a 95% confidence interval, 50% proportion (p), 5% margin of error (d), and 10% nonresponse rate, yielding a final sample size of 424.
The sample was proportionally allocated to the primary hospital and health center, based on the past three-month average client flow reports (using the ART registries). The first participant was selected by simple random sampling and then using systematic random sampling at every 4th interval, 369 clients from Shewarobit health center, and 55 clients from Shewarobit primary hospital were selected.
Variables and Measurements
Health system responsiveness of HIV/AIDS treatment services was the dependent variable of the study. It was measured using the seven responsiveness domains with a total of 27 items of questions: prompt attention (4 items), respect (4 items), communication (3 items), autonomy (4 items), confidentiality (3 items), choice (3 items), and quality of basic amenities (6 items).35 Each question was rated with four and five-point Likert scale options (responses code 1–4, and 1–5) depending on the type of questions presented from never to always, from very bad to very good, or from strongly disagree to strongly agree.26,35 The outcome variable’s overall value was dichotomized as acceptable and unacceptable based on the threshold, which was determined using the demarcation threshold formula: (total highest score – total lowest score)/2) + total lowest score.36,37 Accordingly, those who scored 78 and above were considered the HSR as “acceptable” otherwise “unacceptable”. Likewise, each domain was also determined by the demarcation threshold formula as to the main outcome variable.36,37
Perceived quality of care was measured by 12 questions of the clients’ response about the quality of care and rated from strongly disagree to strongly agree,38 and dichotomized as low or high.36,37 Consequently, those who scored below 66.5 were considered “low” otherwise considered “high”.
Patient health questions; the assessment of depression using nine questions ranged from “Not at all to almost every day” and dichotomized as low or high. Accordingly, those who got below 22.5 were considered “low” and otherwise considered “high”.
Client satisfaction was measured by six satisfaction-related questions rated from very dissatisfied to very satisfied, strongly disagree to strongly agree and none of the time to all of the time,39 and categorized as poor or good. Distance to reach the health facility is the amount of kms taken to reach the health facility on foot and was determined as greater and equal to 5 km or less than 5 kms. Type of health facility; The type of health facilities for this study were hospital and health center. Visiting a traditional practitioner; It is the clients’ exposure status to traditional healers before coming to public health facilities and measured as “Yes” or “No”.
Data Collection Tools and Procedures
An interviewer-administered structured questionnaire was developed from the WHO multi-country studies.26,35 The questionnaire consists of the socio-demographic characteristics, clinical, perceived health, service accessibility, perceived quality of care, satisfaction, patient health questions (PHQ-9), and HSR related questions. For perceived service quality, the SERVQUAL tool was used,38 patient satisfaction assessment,39 PHQ 9 was used to assess whether the patients have depression or not.40 Moreover, chart reviews were employed for viral load, HIV clinical stage, and other chronic diseases.
The data collection tools were prepared in English, then translated to Amharic (local language) and back to English to ensure consistency. The overall internal reliability of the tools was checked using Cronbach’s alpha reliability test. Hence, the Cronbach’s alpha values for HSR, PHQ-9, satisfaction with care and perceived quality of care were 0.97, 0.96, 0.97, and 0.99, respectively, which showed high reliability.3 The questionnaire was pre-tested on 24 clients (5% of the sample size) attending HATCS at Ataye health center (the nearby health center) to check the completeness, clarity, and consistency. Three diploma nurses for data collection and one BSc holder health officer for supervision, who were not working in the study areas, were recruited. A one-day training was given to data collectors and the supervisor on the objectives of the study, data collection tools, procedures, and handling of participant’s concerns without introducing biases.
Data Processing and Analysis
The data were entered and cleaned using Epi-data version 4.6 and analyzed using SPSS Version 20. Descriptive statistics and binary logistic regression analysis were done. In the bivariable analysis, a p-value of less than 0.2 was used to select the candidate variables for the multivariable analysis. In the final model, a p-value of less than 0.05 and adjusted odds ratio (AOR) with a 95% confidence interval (CI) were used to declare the factors significantly associated with the health system’s performance. The Hosmer and Lemeshow test result of model fitness was 0.35.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) of the University of Gondar, College of Medicine and Health Sciences, Institute of Public Health (Ref. No: IPH/8768/2012). Permission was obtained from Shewarobit primary hospital, district health office, and health center before data collection. Informed written consent was obtained from each study participant. The purpose and benefits of the study were explained to the respondents. Confidentiality was maintained by avoiding personal identifiers and keeping the participants’ privacy during the interview. The study was done according to the Helsinki declaration.
Results
Socio-Demographic Characteristics of Participants
A total of 416 clients were invited and participated in the study, with a response rate of 98.1%. The majority (88.0%) were from the health center, more than half (52.2% were females, and 34.6% were in the age group of 30–39 years. Regarding marital status, 60.1% were not married; 66.4% were Christian followers religiously; 34.9% were merchants (Table 1).
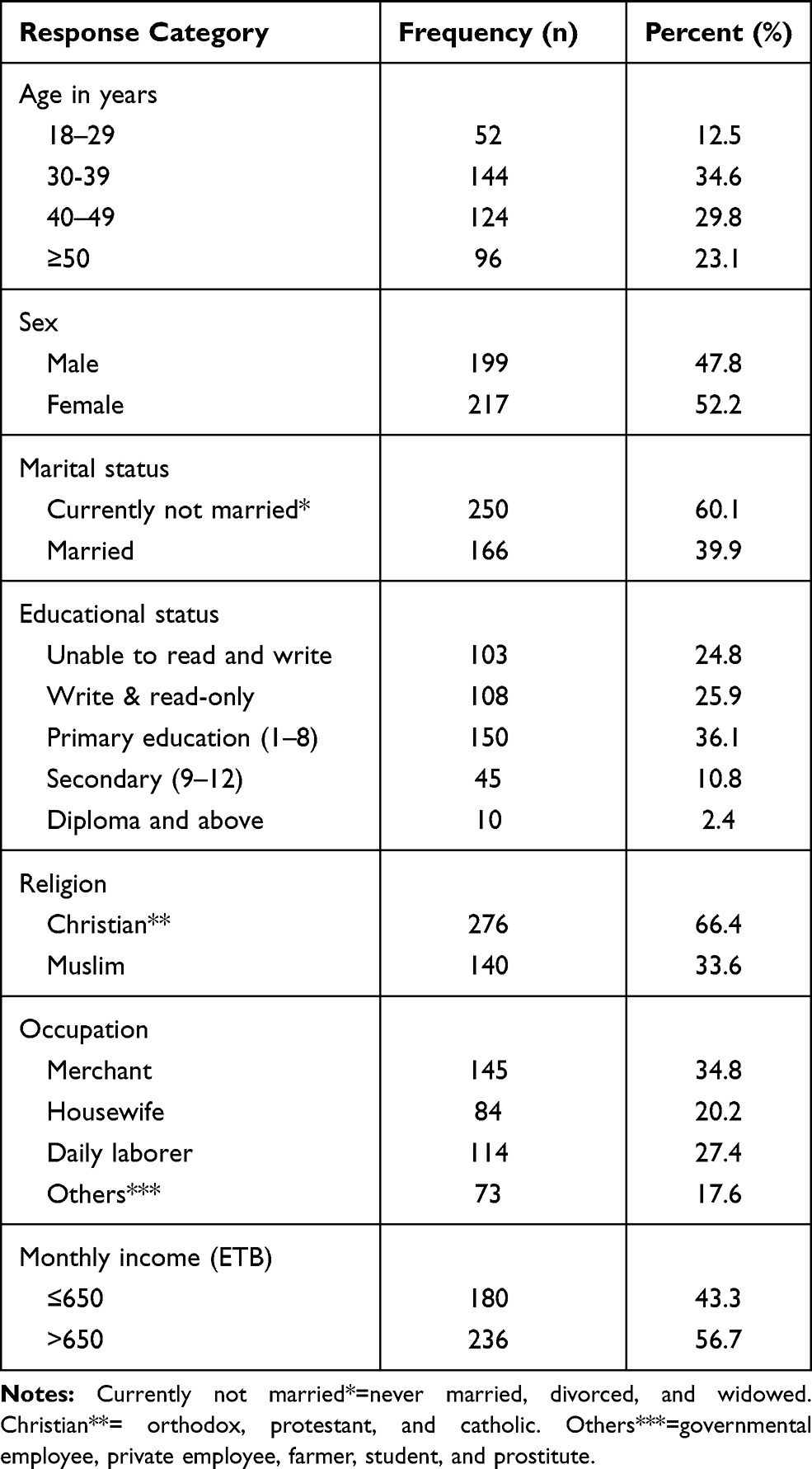 |
Table 1 Socio-Demographic Characteristics of the Participants in Shewarobit Town Public Health Facilities, North Shewa Zone, Ethiopia, 2020 (n=416) |
Clinical Characteristics of the Participants
Regarding their health status, the majority (97.6%) of the respondents’ viral load was below 1000 copies/cm3 and (98.3%) were in the first HIV clinical-stage, 7.7% have had other chronic diseases in addition to HIV/AIDS, and almost three fourth (73.1%) have had perceived good health. Moreover, 92.1% and 55.5% of the participants had high PHQ-9 and good satisfaction with care, respectively (Table 2).
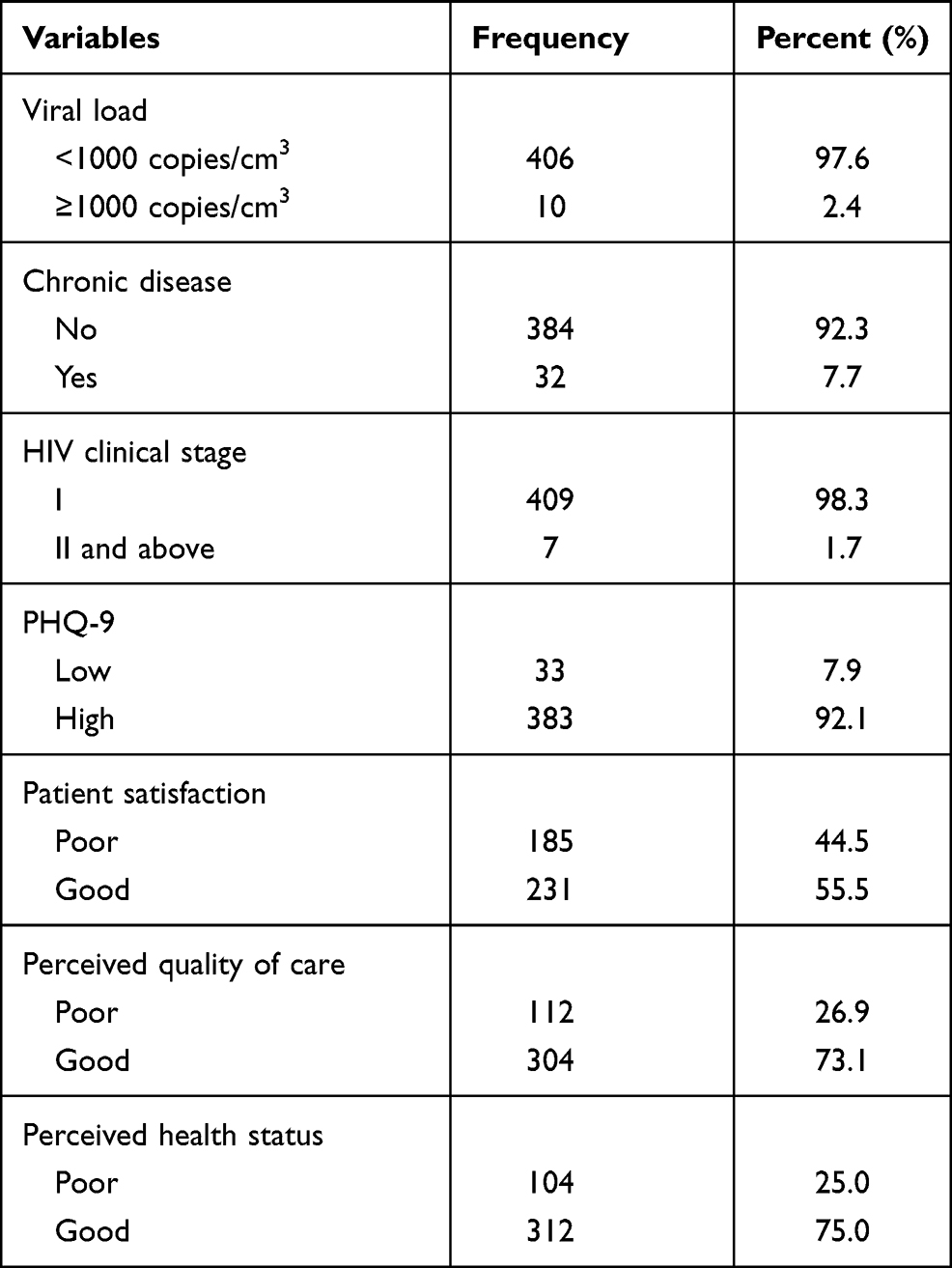 |
Table 2 Clinical Characteristics of the Participants in Shewarobit Town Public Health Facilities, North Shewa Zone, Ethiopia, 2020 (n=416) |
Health Services Accessibility-Related Characteristics
Nearly eight three percent of the participants were travelling less than 5kms on foot to get the care, and 87.98% were treated at HC. Moreover, 70.43% had no history of visiting traditional healers for care (Table 3).
 |
Table 3 Health Service-Related Characteristics of Participants in Shewarobit Town Public Health Facilities, North Shewa Zone, Ethiopia,2020 (n=416) |
Health System Responsiveness of HATCS
The magnitude of HSR performance was 55.3% (95% CI, 50.6%-59.8%). Across the domains the responsiveness score was respect (83.1%), communication (82.5%), confidentiality (91.1%), amenity (72.4%), autonomy (58.4%), prompt attention (24.3%), and choice (26.9%) (Table 4).
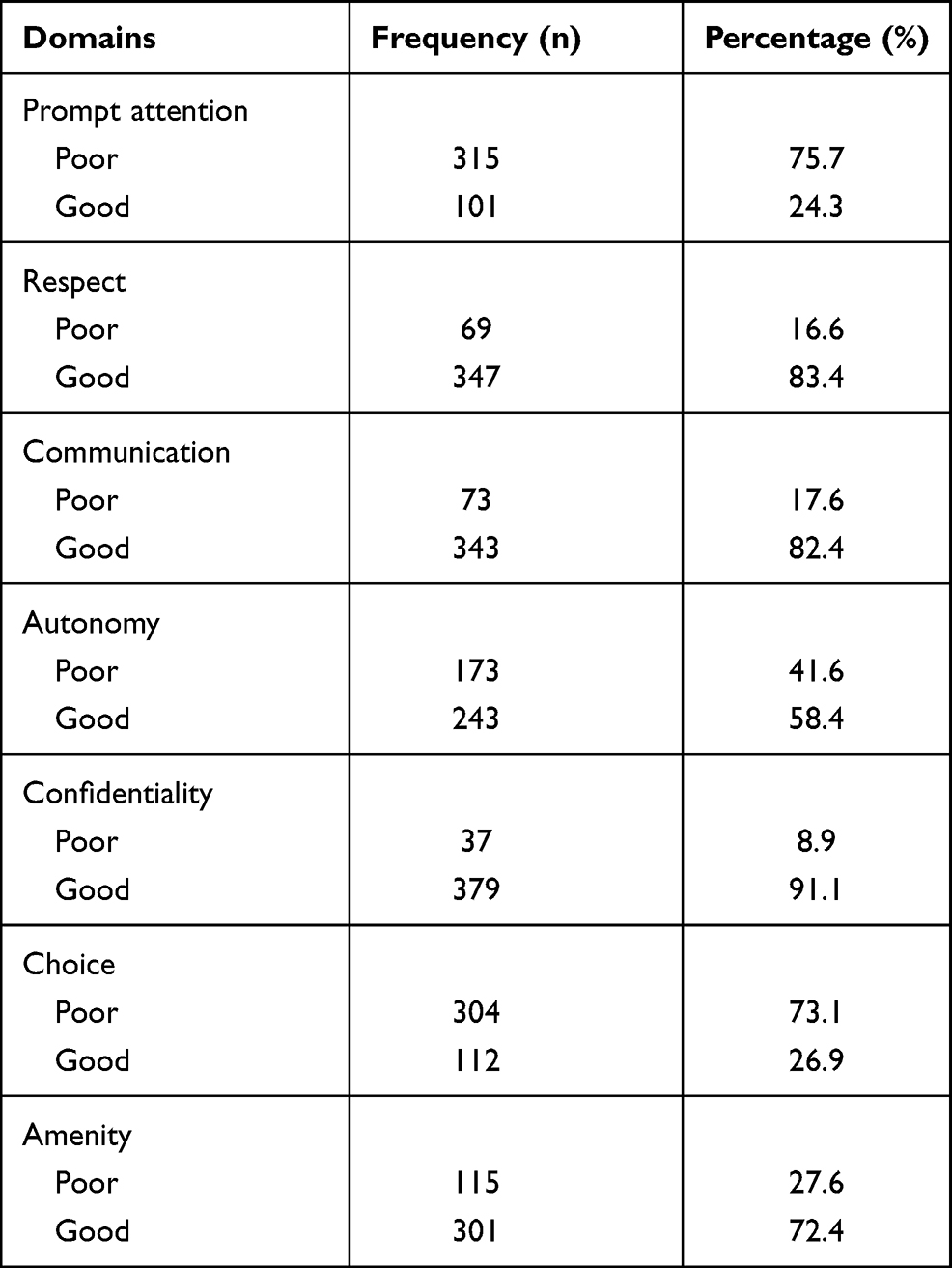 |
Table 4 Performance of HSR Domains for HATCS in Shewarobit Town Public Health Facilities, North Shewa Zone, Ethiopia, 2020 (n = 416) |
Factors Associated with the HSR of HATCS
In the final multivariable logistic regression analysis, age, satisfaction, perceived health status and visiting traditional healers were significantly associated with HSR.
Accordingly, HSR among participants whose age was 50+ was 2.48 times higher than those in the age group 18 to 29 years (AOR: 2.48, 95% CI, 1.12–5.54). Responsiveness among participants who had good perceived health status was more than three times higher compared to their counterparts (AOR: 3.10, 95% CI: 1.75–5.48). Participants having a history of visiting traditional healers before joining the public health facility were 2.5 times more likely to receive acceptable health system responsiveness than those who had no history of visiting traditional healers (AOR: 2.50, 95% CI:1.51–4.17). Moreover, HSR among participants who had good satisfaction with care was nearly three times higher than those who had poor satisfaction (AOR: 2.98, 95% CI:1.35–6.54) (Table 5).
 |
Table 5 Bivariable and Multivariable Linear Regression Analysis of Potential Factors Associated with HSR of HATCS in Shewarobit Town Public Health Facilities, North Shewa Zone, Ethiopia, 2020 (n = 416) |
Discussion
This study investigated the HSR HIV/AIDS treatment and care service users in Shewarobit town public health facilities. The WHO multi-country studies questionnaire was used to measure HSR. The overall HSR of HATCS in Shewarobit public health facilities was 55.3%. Moreover, age, satisfaction with services, perceived health status and visiting traditional healers were variables significantly associated with HSR.
The finding lower than that of a study conducted in Wolayta zone, Ethiopia (68.3%).26 This could be a difference in the study period; the previous study was carried out three years ago when non-governmental organizations actively engaged, there was also a high provision of training and professional benefit packages that increased health workers’ motivation, nevertheless, in the current time, most of the partners leave without handing over to the government. Similarly, this finding was lower than the finding of studies in Brazil (80%) and European countries (81%).41 It may be attributed to socio-cultural and economic disparities such as skilled manpower, health care availability and accessibility, access to transport, and differences in the clients’ perception.
The performance of responsiveness of HATCS differed in each domain. The finding is supported by a study conducted in Brazil where the adequate responsiveness of choice (24.4%) and prompt attention (22%).42 Our study revealed that there were high unacceptable responsiveness performance in prompt attention (75.72%) and choice (73.08%) domains while high acceptable responsiveness performed in confidentiality (91.11%), respect (83.41%), and communication (82.45%). This result was in line with that of a study conducted in the Wolayta zone in which confidentiality (92.4%) and respect (94.9%) were high scored domains,26 This highest achievement might be the attention given to compassion, respect, caring in Ethiopia which is one of the transformational agendas of health sector transformational plan of the country,43 Iran,19,44 and Tanzania by which confidentiality (86.7%) and respect (81.4%) were the highest acceptably responsive domains.45 In Europe, respect, and communication were the highest performed domains in overall services,21 and Cameron.24
In this study, the likely hood of HSR among participants aged 50 years and above was 2.48 times higher compared to those aged 18 up to 29 years. This is consistent with a study in South Africa.46 The study showed that HSR was increased by more than three times among participants who perceived good health than those who perceived poor health status. This study was consistent with studies in southern Ethiopia,26 South Africa,46 and Europe.21 This means that the likelihood of commitment to therapy and compliance with the program often increases as good health perception increases.47
Compared to those who had poor satisfaction with care, those patients who had good satisfaction with the services offered had 2.98 times higher HSR. This result was supported by a study in southern Ethiopia26 and Vietnam.48 Furthermore, WHO evidence showed that all responsiveness domains, except confidentiality, were positively and significantly linked to recorded satisfaction with the health care system.5 This represents the presence of the high patient and professional interactions that meets the needs of patients, which should be an absolute priority for patients with HIV/AIDS.49
In this study, the odds of HSR among participants with a history of visiting traditional healers before joining the public health facility was 2.5 times higher compared to their counterparts. This is the fact that traditional healers give no treatment for HIV/AIDS. Therefore, the patients’ confirmation of care given by traditional healers is certainly unmatched with care from public health facilities that improve HSR.
Strength and Limitations
For the result to be considered representative of HATCS in the study area, relatively large sample size was used. The study used primary and secondary data sources to improve the credibility of the results. As for the limitation, the performance of responsiveness was assessed based on the client’s experience and perceptions, most of the health facility-related factors were not assessed, if the research was performed with a mixed approach, it could be better.
Conclusions
HIV/AIDS treatment and care’s overall responsiveness performance was 55.3%. Although some domains such as confidentiality, respect, and communication domains were in high acceptable performance, the choice and prompt attention domains were in high unacceptable response performance.
The age of participants’, perceived health status, the history of patients visiting traditional healers before entering public health facilities, and patients’ satisfaction with the services were factors significantly correlated with HSR in public health facilities in Shewarobit city administration. Thus, providing training, proactive supervision, community awareness, and including traditional healers in the modern health system and increasing the responsiveness of choice and prompt attention domains, would enhance the health system’s responsiveness in the study area.
Acknowledgment
The authors would like to thank all respondents for their willingness to participate in the study and gave valuable information. We are also thankful to the Shewarobit administration town health office, hospital, and health center for their permission. And the University of Gondar, Institute of Public Health staff, for their technical supports. Finally, our appreciation should go to data collectors and supervisors for their unreserved contribution to the data collection process.
Disclosure
The authors declared that they have no conflicts of interest for this work and that no funding was obtained for this study.
References
1. WHO. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes. WHO’s Framework for Action. Geneva: World Health Organization; 2007.
2. WHO. The World Health Report 2000: Health Systems: Improving Performance. Geneva: World Health Organization; 2000.
3. A. D. An Introduction to Quality Assurance in Health Care. New York: Oxford University Press; 2003.
4. Valentine N, de Silva A, Kawabata K, Darby C, Murray C, Evans D. Health system responsiveness: concepts, domains and operationalization. Health Syst Performance Debates Methods Empiricism. 2003.
5. Bleich SN. How does satisfaction with the health-care system relate to patient experience? Bull World Health Organ. 2009;87(4):271–278. doi:10.2471/BLT.07.050401
6. Blumenthal D. Quality of care–what is it? N Engl J Med. 1996;335(12):891–894. doi:10.1056/NEJM199609193351213
7. De Silva A, Valentine N. A Framework for Measuring Responsiveness. Geneva: World Health Organization; 2000.
8. Üstün TB, Chatterji S, Mechbal A, Murray C. Methods, Empiricism. The world health surveys. Geneva: WHO; 2003:797.
9. UNAIDS. Global HIV & AIDS statistics — 2019 fact sheet. 2019.
10. Allen H, Wright BJ, Harding K, Broffman L. The role of stigma in access to health care for the poor. Milbank Q. 2014;92(2):289–318. doi:10.1111/1468-0009.12059
11. Rankin WW, Brennan S, Schell E, Laviwa J, Rankin SH. The stigma of being HIV-positive in Africa. PLoS Med. 2005;2(8):. doi:10.1371/journal.pmed.0020247.
12. Murray CJ, Frenk J. A framework for assessing the performance of health systems. Bull World Health Organ. 2000;78(6):717–731.
13. Fan VS, Burman M, McDonell MB, Fihn SD. Continuity of care and other determinants of patient satisfaction with primary care. J Gen Intern Med. 2005;20(3):226–233. doi:10.1111/j.1525-1497.2005.40135.x
14. Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q. 2005;83(4):691–729. doi:10.1111/j.1468-0009.2005.00397.x
15. Hw J. Universal access to HIV/AIDS treatment: promise and problems. JAMA. 2008;300(5):2008.
16. Dang BN, Westbrook RA, Black WC, Rodriguez-Barradas MC, Giordano TP. Examining the link between patient satisfaction and adherence to HIV care: a structural equation model. PLoS One. 2013;8(1):e54729–e54729.
17. Assefa Y, Lynen L, Wouters E, Rasschaert F, Peeters K, Van Damme W. How to improve patient retention in an antiretroviral treatment program in Ethiopia: a mixed-methods study. BMC Health Serv Res. 2014;14(1):45. doi:10.1186/1472-6963-14-45
18. Valentine N, Darby C, Bonsel GJ. Which aspects of non-clinical quality of care are most important? Results from WHO’s general population surveys of “health systems responsiveness” in 41 countries. Soc Sci Med. 2008;66(9):1939–1950. doi:10.1016/j.socscimed.2007.12.002
19. Bazzaz MM, Taghvaee MRE, Salehi M, Bakhtiari M. Health system’s responsiveness of inpatients: hospitals of Iran. Glob J Health Sci. 2015;7(7):106–117. doi:10.5539/gjhs.v7n7p106
20. Li J, Chongsuvivatwong V, Assanangkornchai S, McNeil EB, Cai L. Comparison of health system responsiveness between HIV and non-HIV patients at infectious disease clinics in Yunnan, China. Patient Prefer Adherence. 2018;12:1129–1137. doi:10.2147/PPA.S163416
21. Murante AM, Seghieri C, Vainieri M, Schäfer WLA. Patient-perceived responsiveness of primary care systems across Europe and the relationship with the health expenditure and remuneration systems of primary care doctors. Soc Sci Med. 2017;186:139–147. doi:10.1016/j.socscimed.2017.06.005
22. Miller JS, Mhalu A, Chalamilla G, et al. Patient satisfaction with HIV/AIDS care at private clinics in Dar es Salaam, Tanzania. AIDS Care. 2014;26(9):1150–1154. doi:10.1080/09540121.2014.882487
23. Mohammed S, Bermejo J, Souares A, Sauerborn R, Dong H. Assessing responsiveness of health care services within a health insurance scheme in Nigeria: users’ perspectives. BMC Health Serv Res. 2013;13:502. doi:10.1186/1472-6963-13-502
24. Wung BA, Peter NF, Atashili J. Clients’ satisfaction with HIV treatment services in Bamenda, Cameroon: a cross-sectional study. BMC Health Serv Res. 2016;16(1):280. doi:10.1186/s12913-016-1512-5
25. Peltzer K, Phaswana-Mafuya N. Patient experiences and health system responsiveness among older adults in South Africa. Glob Health Action. 2012;5(1):18545.
26. Yakob B, Ncama BP. Measuring health system responsiveness at facility level in Ethiopia: performance correlates and implications. BMC Health Serv Res. 2017;17(1):263. doi:10.1186/s12913-017-2224-1
27. Alemayehu YK, Bushen OY, Muluneh AT. Evaluation of HIV/AIDS clinical care quality: the case of a referral hospital in North West Ethiopia. Int J Qual Health Care. 2009;21(5):356–362. doi:10.1093/intqhc/mzp030
28. Posse M, Meheus F, van Asten H, van der Ven A, Baltussen R. Barriers to access to antiretroviral treatment in developing countries: a review. Trop Med Int Health. 2008;13(7):904–913. doi:10.1111/j.1365-3156.2008.02091.x
29. Yakob B, Purity ncama B. Client satisfaction: correlates and implications for improving HIV/AIDS treatment and care services in southern Ethiopia. Int Health. 2016;8(4):292–298. doi:10.1093/inthealth/ihw008
30. Liabsuetrakul T, Petmanee P, Sanguanchua S, Oumudee N. Health system responsiveness for delivery care in Southern Thailand. Int J Qual Health Care. 2012;24(2):169–175. doi:10.1093/intqhc/mzr085
31. Kayombo EJ, Uiso FC, Mbwambo ZH, Mahunnah RL, Moshi MJ, Mgonda YH. Experience in initiating collaboration of traditional healers in managing HIV and AIDS in Tanzania. J Ethnobiol Ethnomed. 2007;3(1):6. doi:10.1186/1746-4269-3-6
32. WHO. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. In: Recommendations for a Public Health Approach. Geneva; 2013.
33. (CSA) CSA. National census; Amhara region population distribution by city. 2007.
34. office sh. Annual Health Facilities Performance; 2019.
35. Üstün TB, Chatterji S, Villanueva M, et al. WHO multi-country survey study on health and responsiveness. 2001.
36. Hailemariam S, Genetu A, Sahile E. Mother’s satisfaction towards childbirth care at public health centers in Bench-Maji Zone, Ethiopia: a facility-based cross-sectional study. Int J Reprod Med. 2020;2020:6746459. doi:10.1155/2020/6746459
37. Mindaye T, Taye B. Patients satisfaction with laboratory services at antiretroviral therapy clinics in public hospitals, Addis Ababa, Ethiopia. BMC Res Notes. 2012;5(1):184. doi:10.1186/1756-0500-5-184
38. Daniel CN, Berinyuy LP. Using the SERVQUAL Model to assess service quality and customer satisfaction. 2010.
39. Hawthorne G, Sansoni J, Marosszeky N. An update on the development of the short assessment of patient satisfaction (SAPS). 2009.
40. Löwe B, Kroenke K, Herzog W, Gräfe K. Measuring depression outcome with a brief self-report instrument: sensitivity to change of the Patient Health Questionnaire (PHQ-9). 2004;81(1):61–66. doi:10.1016/S0165-0327(03)00198-8
41. Valentine N, de Silva A, Murray C Estimating responsiveness level and distribution for 191 countries: methods and results. GPE Discussion Paper Series: No22. 2000.
42. DdS M, Martins RD, RPFSd J, Samico IC, Santo A. Assessment of the responsiveness of a public health service from the perspective of older adults. Revista De Saúde Pública. 2017;51:51. doi:10.1590/S1518-8787.2017051006854
43. Wassihun B, Zeleke S. Compassionate and respectful maternity care during facility based child birth and women’s intent to use maternity service in Bahir Dar, Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):294. doi:10.1186/s12884-018-1909-8
44. Karami-Tanha F, Moradi-Lakeh M, Fallah-Abadi H. Health system responsiveness for care of patients with heart failure: evidence from a university hospital. Arch Iran Med. 2014;17(11):736–740.
45. Kapologwe NA, Kibusi SM, Borghi J, Gwajima DO, Kalolo A. Assessing health system responsiveness in primary health care facilities in Tanzania. BMC Health Serv Res. 2020;20(1):104. doi:10.1186/s12913-020-4961-9
46. Peltzer K, Phaswana-Mafuya N. Patient experiences and health system responsiveness among older adults in South Africa. Glob Health Action. 2012;5:1–11.
47. Dang BN, Westbrook RA, Black WC, Rodriguez-Barradas MC, Giordano TP. Examining the link between patient satisfaction and adherence to HIV care: a structural equation model. PLoS One. 2013;8(1):e54729.
48. Tran BX, Dang AK, Vu GT, et al. Patient satisfaction with HIV services in Vietnam: status, service models and association with treatment outcome. PLoS One. 2019;14(11):e0223723. doi:10.1371/journal.pone.0223723
49. Roberts KJ. Physician-patient relationships, patient satisfaction, and antiretroviral medication adherence among HIV-infected adults attending a public health clinic. AIDS Patient Care STDS. 2002;16(1):43–50. doi:10.1089/108729102753429398
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.