Back to Journals » Nursing: Research and Reviews » Volume 9
Health literacy and informed consent for clinical trials: a systematic review and implications for nurses
Authors Burks AC, Keim-Malpass J ![]()
Received 4 March 2019
Accepted for publication 20 June 2019
Published 10 July 2019 Volume 2019:9 Pages 31—40
DOI https://doi.org/10.2147/NRR.S207497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Cindy Hudson
Allison C Burks, Jessica Keim-Malpass
Department of Acute and Specialty Care, University of Virginia School of Nursing, Charlottesville, VA, USA
Abstract: The informed consent process for consideration of clinical trials is a complex process that requires the understanding of the potential trial risk, benefits, and alternatives of treatment. The aim of this systematic review was to explore the available literature related to health literacy and the informed consent process for clinical trials. Articles were included if they focused on health literacy and patient comprehension of informed consent, had perceptions related to the informed consent process, or assessed the impact of health literacy on patients’ willingness to participate in clinical trials. Eight articles were selected for this review. Limited health literacy was determined to be related to a lack of comprehension of clinical trial consent documents and heightened anxiety surrounding the informed consent process. Conflicting evidence exists around the relationship between health literacy and clinical trial enrollment. Limited health literacy levels may impact the ability for nurses to have effective informed consent processes.
Keywords: health literacy, clinical trial participation, clinical trial enrollment disparity, clinical trial consent
Health literacy refers to the ability to comprehend, as well as the ability to obtain, critically evaluate, and integrate health-related information.1 A patient’s health literacy level is an important element of high-quality care that can impact decisions and actions of patients and providers. Educational background is not always predictive of health literacy levels; as an individual’s health literacy level may be lower than his or her general literacy, meaning that even highly educated adults may have limited health literacy.2 An estimated 20–36% of all adults in the United States have limited health literacy.1,3 Limited health literacy is associated with disadvantages in health care including access to information, capacity to process and understand information, and adverse health outcomes.4 Adult patients with limited health literacy levels are at greater risk for limited comprehension in the health care setting, leading to stigma and a lack of engagement in shared decision-making.5,6
When patients are faced with a serious diagnosis with multiple treatment options they may take longer to understand information presented to them due to increased emotional stress.7 Limited health literacy levels can compound this stress, adding to the difficulty of comprehension of the extent of their illness as well as the available treatment options. Clinical trials are becoming increasingly more common as treatment options for patients with serious illnesses, but the research process is often unfamiliar to patients.8 Components of the research process that may lead to confusion include voluntary participation, freedom to withdraw, availability of alternative treatments, randomization, unclear survival benefits, unclear risk of adverse events, and the potential for receiving a study placebo in some cases. An informed consent process is required in order to ensure that patients understand the full extent of what they are agreeing to participate in prior to initiation of treatment. Limited health literacy could act as a barrier to clinical trials as clinical trial consents are often written at a high school or college reading level, impeding the ability of comprehension among patients with limited health literacy.9 Beyond reading level, informed consent documents are describing complex treatment pathways, randomization, and study procedures. Finally, clinical equipoise (ie, the concept that the investigators are hopeful that the novel therapeutic may offer benefit, but there is uncertainty surrounding the efficacy and side effects) is a complex concept to explain regardless of the patient’s health literacy.10,11 Providers must be able to assess if their patients fully comprehend the risks, benefits, and alternatives of clinical trials and ability to sign consents for clinical trials. This assessment requires an understanding of patients’ health literacy and what they understand about the clinical trial and alternative options. The relationship between health literacy and engagement in processes related to clinical trial enrollment (including informed consent, shared decision-making, general knowledge related to research participation, understanding the risks, benefits, alternatives, and links to actual clinical trial participation) has not between well established in the literature to date, and there is a defined need to elucidate these concepts. The purpose of this literature review was to evaluate the literature related to health literacy and the informed consent process in clinical trials.
Methods
A review of the literature was completed in November 2017 through June 2019 using a systematic approach. Combinations of the terms “health literacy,” “clinical trial participation,” and “clinical trial enrollment disparity” were used to search the bibliographical databases CINAHL, Cochrane, PubMed, Web of Science, PsycNET, and Google Scholar for English language articles. Figure 1 illustrates the search strategy during each phase of the literature review.
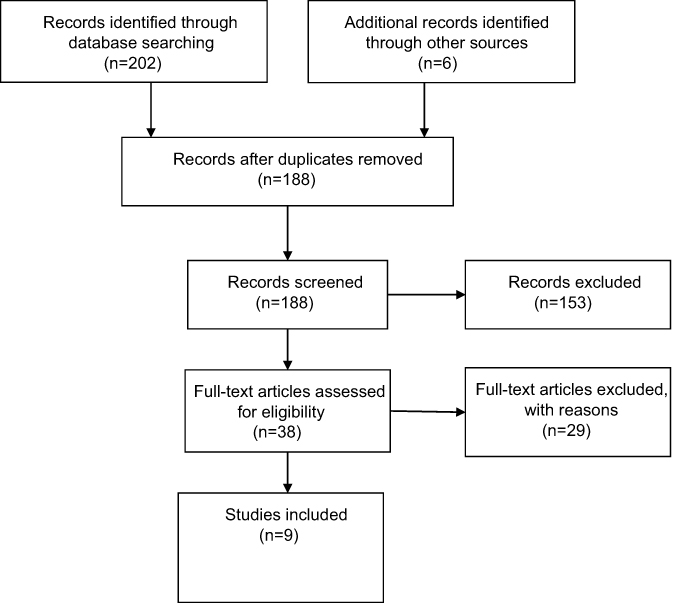 |
Figure 1 Methods diagram. |
Articles were included in this literature review if they investigated the consent process for clinical trials. Specifically, relevant articles focused on informed consent comprehension, patient perceptions of consents, and the impacts of health literacy on patient’s willingness to participate in clinical trials were also included. Exclusion criteria included studies focused on children and/or adolescents due to the ethical differences of the assent process and obtaining consent for specific procedures or treatments. Finally, studies completed outside of the United States were not included due to differences in national clinical trial regulations under the Common Rule.12 Studies completed prior to 1990 were excluded.
The initial search resulted in a total of 188 abstracts for review. At this stage, papers that failed to meet inclusion criteria based on the abstract alone were excluded, leaving 38 articles for full-text review. Twenty-nine articles were then excluded according to the inclusion and exclusion criteria, leaving 9 articles meeting the inclusion criteria and two systematic reviews (see Figure 1). The systematic reviews were read for overall context, and individual articles that were cited were reviewed for potential eligibility. The final sample included 9, and each was abstracted using a template, analyzed to determine the purpose, sample population, health literacy assessment used, outcomes measured in each study, and study results as summarized in Table 1. Verification of paper eligibility and abstraction of key data elements were conducted using two independent reviewers (AB and JKM). After key elements related to study predictors and outcomes were abstracted from each of the included studies, the two authors conducted a directed thematic analysis to identify cross-cutting themes. A formal quality assessment was not able to be performed because the studies were all observational and cross-sectional, with convenience samples so all articles would have been deemed as low quality lacking the ability for broad generalization.
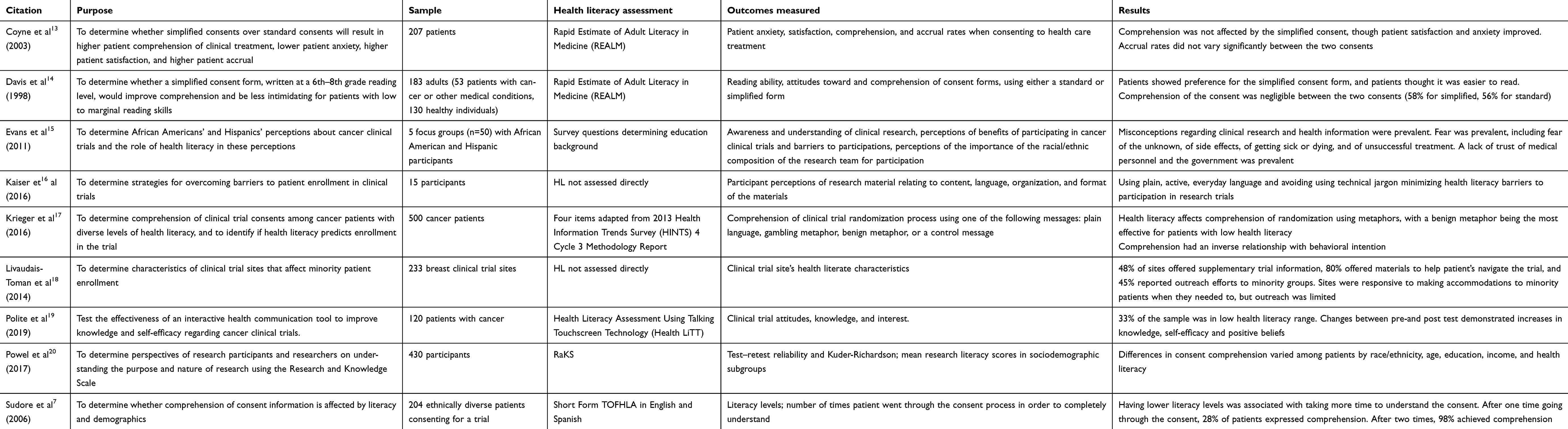 |
Table 1 Literature search review matrix |
Results
Several studies used a validated assessment of health literacy in their studies to measure health literacy among their participants. The health literacy assessment tools used included the Rapid Estimate of Adult Literacy in Medicine (REALM), the Test of Functional Health Literacy in Adults (TOFHLA), and Health Literacy Assessment Using Talking Touchscreen Technology (Health LiTT). Two articles compared health literacy levels in participants with informed consent documents for hypothetical clinical trials as opposed to clinical trials they were actually considering for themselves. All of the studies were observational in nature, and only one of the studies included development or testing of an intervention for those with limited health literacy.19 Researchers collected outcome data through surveys, questionnaires, and in-person or telephone interviews.
Three common themes were apparent within the articles including the relationship between health literacy and 1) patient comprehension of informed consent documents, 2) patient perceptions of clinical trial consent processes, and 3) patient willingness to participate in clinical trials. The following sections describe these themes in depth.
Health literacy and patient comprehension of informed consent documents
Varying health literacy levels affects patients’ comprehension of clinical trial informed consent documents, with lower literacy levels associated with lower comprehension. Studies that addressed health literacy by using modified or simplified consents improved comprehension among patients of all literacy levels.14,13 Standard informed consent documents are often written above the population’s average literacy level, indicating a gap between health literacy and the ability of patients or families to understand information about clinical trials.
Davis et al14 conducted a study to assess adults’ comprehension of informed consent documents for a Phase III breast cancer clinical trial. Study participants were first screened for health literacy levels using REALM, which determined the average reading level of participants to be at a 7th–8th grade level. Forty-six of the 183 adults tested (25%) scored below a 6th grade level, meaning they could be considered to have marginal health literacy. The participants were given either a standard informed consent document or a simplified booklet-style form. Comprehension of the clinical trial was assessed using a questionnaire developed by the researchers. The average comprehension of the standard informed consent document was 58%. The average comprehension of the simplified informed consent document was 56%, indicating no significant difference between both forms (p=0.0033). The researchers noted a correlation between comprehension scores and health literacy levels. Participants who scored at or above a 9th grade level had significantly higher comprehension scores for both consents at 72% comprehension than those reading on or below an 8th grade level. The average comprehension score for participants reading at or below a 3rd grade level was 21%, 39% for those at a 4th–6th grade level, and 54% for those reading at a 7th–8th grade level. Overall, comprehension of basic treatment information was low for all participants in this study.
Coyne et al13 conducted a study to assess whether easy-to-read consent statements compared with standard informed consent documents for cancer clinical trials resulted in greater patient comprehension. Study participants were screened using REALM to determine health literacy level, and the results indicated that the average reading level for this sample was at or above a 9th grade level. Comprehension of the consents was measured using 23 true/false and multiple-choice questions about the treatment regimens presented in the consents. The results showed a comprehension rate of 69% for the standard consent and 72% for the simplified consent. Researchers also noted that participant’s REALM scores were positively associated with comprehension of consents, regardless of whether they were reading the standard or simplified versions, meaning the higher the health literacy level, the better the participants were able to comprehend. Results from this study limit generalizability to broader populations given the high levels of health literacy in the study sample.
Sudore et al7 conducted a qualitative study to assess whether and how health literacy affected the understanding of consent information. Literacy levels of the 208 participants were first assessed using the Short Form Test of TOFHLA. Comprehension of the informed consent document was assessed using a true/false questionnaire focusing on the participant’s understanding of study procedures, risk, and confidentiality when enrolling in a clinical trial. Participants were required to answer every question correctly prior to enrollment, and researchers noted the number of passes it took for participants to achieve this goal. Lower health literacy levels were significantly associated with requiring more passes through the consent process and missing more comprehension questions on the questionnaire. Results of this study showed that with each 1-point decrease in individual’s TOFHLA score, the odds of requiring more passes and missing more comprehension statements on the first pass increased.
Evans et al15 conducted a qualitative study to determine awareness and understanding of cancer clinical trial research process, specifically among African Americans and Hispanics/Latinos. Health literacy was assessed using survey questions regarding education background. Participants were asked to discuss their understanding of the clinical trial process, including the randomization process. Misconceptions regarding cancer clinical trial research were prevalent, and researchers concluded that limited health literacy contributes to poor comprehension as evidenced by the inaccuracies and misconceptions of information among their participants.
Krieger et al17 addressed how health literacy affected comprehension of randomization during the cancer clinical trial consent process. Researchers used three different methods of delivering information in consents including plain language, a gambling metaphor, and a benign metaphor. Comprehension among these three presentations as well as to participant’s health literacy levels was compared. Health literacy was assessed using four questions from the 2013 Health Information Trends Survey (HINT) 4 Cycle 3 Methodology Report. Health literacy was determined to have a statistically significant effect on comprehension of randomization during the consent process, with participants with lower health literacy levels comprehending less. The benign metaphor was shown to increase comprehension among participants with low health literacy levels, while the gambling metaphor increased comprehension among patients with higher health literacy levels. Use of the metaphors to explain information during the consent process improved comprehension for all participants compared to using plain language alone.
Powell et al20 developed the Research and Knowledge Scale (RaKS) in order to measure health literacy and determine how literacy levels affect comprehension of consents for research trials. The study used survey questions involving aspects of clinical trials such as randomization, risks associated with studies, and informed consents and determined participants' understanding of the information. Researchers determined that research understanding of the survey was lower among participants with lower health literacy levels.
Simonds et al21 assessed 97 informed consent documents to determine readability, suitability, and comprehensibility. By using the Simple Measure of Gobbledygook, the results showed that the average reading level of the consents was grade 12. By using the Suitability and Comprehensibility Assessment of Materials, the researchers showed that 29% of the consents adequately met literacy demands of the population. Researchers determined that consents are often above the average literacy level of the population, impeding participants’ comprehension of study information.
Health literacy and patient perceptions of the informed consent process
Patients’ perceptions of the informed consent process varied depending on literacy levels and readability of consents. When researchers provided simplified versions of their consents, participants were identified as being more satisfied with the consent process. Fear and anxiety were common feelings during the consent process among participants of all health literacy levels. Those with higher health literacy levels were more likely to have lower levels of fear and greater satisfaction of consents.
Davis et al14 assessed participants’ preference for either the standard consent form or the simplified consent using a questionnaire. Overall, participants preferred the simplified consent form over the standard consent, indicating on the questionnaires that it was easier to read, less frightening, and more comfortable. Participant preference varied by the reading level, with those who scored lower on the REALM assessment preferring the simplified consent to a greater extent. Of participants reading at or above an 8th grade level, 70% preferred the simplified consent over the standard consent, while 52% of those reading at a 9th grade level or above showed preference for the simplified consent. Of the 183 participants, 115 (63%) indicated that they would prefer to be given both forms when consenting for a clinical trial.
Coyne et al13 also assessed for patient satisfaction of the simplified consent over the standard consent. Participants were more satisfied and less anxious with the easy-to-read consent statement rather than the standard consent form. Higher satisfaction was correlated with higher comprehension, which was positively associated to higher REALM scores, indicating that the higher a patient’s health literacy level, the more likely they are able to understand the consent and therefore be satisfied with the consent process.
Evans et al15 addressed the participants’ attitudes toward the informed consent process compared to the participants’ health literacy levels. The researchers focused discussions on perceptions of clinical trials. A common theme during the discussions was that participants were fearful of research and had a mistrust of medical personnel. A limited health-literacy level was associated with the misconception that participants in clinical trials are guinea pigs. The researchers urged health care providers to address literacy levels in the creation of their consents in order to decrease negative perceptions of clinical trials.
Health literacy and patient willingness to participate in clinical trials
Health literacy is a likely a common barrier to clinical trial enrollment and clinical trial completion, but has yet to be systematically studied.22 Health literacy impacts patient comprehension of consents and the research process, and comprehension is associated with participant intention to participate in studies. Limited health literacy levels can lead to fear and misunderstanding of clinical trials, impeding enrollment rates. The relationship between high levels of health literacy and clinical trial enrollment is also not clear. There has been empirical evidence to suggest high health literacy levels are also associated with less intent to enroll due to the perception that clinical trials are individualized treatment options.17
Coyne et al13 assessed if the use of an easy-to-read consent would result in higher patient accrual rates. Accrual rates did not vary significantly between the two consents, with over 85% of all patients deciding to participate, regardless of which consent they read. REALM scores were not noted to be associated with accrual rates.
Krieger et al17 assessed the relationship between comprehension of the informed consent process and participant intention to participate in the trial. The results showed that comprehension had an inverse relationship with participant intention. Comprehension was determined to positively correlate with health literacy levels in this same study, indicating that higher health literacy levels were associated with less intention of participation in the clinical trial. Researchers noted that higher comprehension of randomization after the consent process likely leads to the belief for patients that clinical trials are not individualized in their treatment regimens, making these participants less willing to enroll in the study. Similarly, Polite et al19 tested the effectiveness of an intervention focused on clinical trial knowledge and self-efficacy targeted toward individuals with varying levels of health literacy. They found that a tailored intervention delivered via iPad can change attitudes and self-efficacy related to clinical trial enrollment for cancer patients.19
Livaudais-Toman et al18 conducted a qualitative study involving 233 breast clinical trials to assess barriers to enrollment including health literacy. The study assessed how consents were presented to patients, including assessment of how clinical trial information was presented to patients (for example, written or verbal consents; available in languages beyond English; the use of summaries or fact sheets; and the availability of consents to be reviewed by community members). Researchers specifically addressed the presentation of these consents among populations with limited health literacy levels, though they did not include how health literacy was assessed. Results of the study showed that a lack of supplemental information in the consent process impedes the understanding of clinical trials among patients with limited health literacy, acting as a barrier to enrollment in the trial. Researchers encouraged acknowledgment of health literate characteristics of clinical trials in order to improve enrollment rates among populations with limited health literacy.
Kaiser et al16 assessed the strategies for overcoming barriers to patient enrollment in clinical trials by using a specific community advisor board known as the Community Advisors of Research Design and Strategies (CARDS). The CARDS identified four characteristics of consents that may affect enrollment in clinical trials among patients with limited health literacy levels. The use of readability tools, every day, active language, non-judgmental tones, and minimal requests for demographic information in consents made community members more willing to participate in the study. Health literacy levels were not assessed among the members of CARDS, though consents were determined to be at a college reading level, and members of the CARDS identified that technical jargon in the consents was confusing and hindered enrollment in the trial.
Discussion
The articles analyzed in this review of the literature discussed the relationship between health literacy and the informed consent process for clinical trials. Limited health literacy was associated with limited comprehension of consents, leading to increased anxiety and decreased satisfaction with the consent process for clinical trials. Misperceptions about clinical trials were common among patients with limited health literacy. The existing research literature has predominantly focused on health literacy and knowledge and/or perceptions regarding the informed consent document only. There is less existing literature focused on the relationship between health literacy and the informed consent process, which also includes an understanding of clinical trial procedures, potential risks, benefits, and alternatives. Additionally, a central component to a clear understanding of risks and benefits of clinical trial participation that should be elicited during the informed consent process is clinical equipoise, and none of the studies specifically focused on the relationship between health literacy and this key concept.
Health care providers must empower patients to make decisions regarding their health particularly during points of additional stress such as a new diagnosis, or a worsening clinical trajectory. The informed consent process can assist patients with shared decision-making, though they must first be able to understand the extent of the consent.23 Based on the evidence presented in this literature review, clinical trial consents are often written above the average health literacy level, prohibiting patients from being able to fully understand what they are signing.21 Several of the articles presented the use of modified or simplified consents to aid in this process in order to attempt to increase comprehension levels among all patients.7,14,13 Comprehension improved when information was simplified, increasing patients’ satisfaction and confidence in their decisions. Comprehension was associated with intent to participate in the trials, though the articles presented conflicting evidence as to whether higher or lower comprehension leads to greater likelihood of enrollment. More research must be done to determine the full effects of health literacy and clinical trial enrollment.
Gaps in current knowledge
The majority of research studies used qualitative interviews to obtain their data, which could have impacted patients’ responses if they answered in ways that they thought health care providers wanted to hear. While this methodological approach is appropriate in eliciting experiences, preferences, and understanding regarding clinical trials, the informed consent process, and consent documents, it does not allow for assessment of the specific relationship between health literacy and these outcomes. Additionally, the measurements used to assess health literacy varied among the articles. Several of the articles either did not assess health literacy at all, or did not use a standardized quantitative measure to assess health literacy. Researchers cannot rely on health literacy assessment that only includes education level as a proxy for health literacy, as it has been well understood that education alone is not indicative of functional health literacy.24 Nonstandardized health literacy assessment may limit the generalizability of the studies to broader populations where it is estimated that upward of 36% of the population have limited health literacy.3
Another important gap in the literature is the lack of evidence supporting the relationship between health literacy and actual clinical trial enrollment or completion. The conceptual basis for this relationship is mixed with some preliminary evidence suggesting that limited health literacy is associated with a lack of comprehension and stigma which may impede clinical trial enrollment.5,6 Alternatively, there is also evidence suggesting that patients with high levels of health literacy and routine access to health information might view clinical trials as nonindividualized plans of care, although this relationship depends on the severity and type of illness.17 For instance, patients with many treatment options available to them might feel more inclined to defer clinical trial enrollment after acquiring additional knowledge.25 Thus, more studies are needed to 1) fully investigate the relationship between health literacy and clinical trial participation and 2) develop subsequent interventions that can be used to tailor informed consent and clinical trial materials for patients with limited health literacy.
The results of this literature review revealed that while studies suggest a relationship between comprehension and health literacy in clinical trial consents and the informed consent process, there is a lack of sufficient evidence elucidating these complex relationships and preventing these findings from being generalizable. Additionally, there was a real lack of attention to the context of family/caregiver health literacy beyond just health literacy assessment at the patient level only. While some of the articles used modified or simplified versions of consents, these informed consent processes have not been standardized, and more research must be done to identify the most appropriate intervention to tailor consents for all literacy levels. More information on patients’ perceptions of the consent process is needed to provide adequate input on ways to improve the consent process to make it better suited to fit the needs of all patients.
Implications for nurses
Health literacy plays an important role in patients’ experience in considering and participating in clinical trials. Literacy levels can impact the amount of information patients and families comprehend when consenting for clinical trials, impacting the ability for researchers to have an effective informed consent process. Patients are likely more satisfied and less anxious about participating in clinical trials when they are able to more fully understand the forms they are signing and can repeat back their own understanding of the potential risks, benefits, and alternatives. When developing consents, nurses must understand this impact in order to ameliorate health literacy as a barrier to health care.
Nurses must be aware of the role of health literacy in health care and specifically when assisting patients in the informed consent process. Prior to initiating the informed consent process for clinical trials, nurses should routinely assess the patient and caregiver/family’s health literacy level.26 There are validated and brief three health literacy screening questions that have been shown to be feasible when implemented in busy clinical environments.26 This routine and brief assessment can empower nurses to tailor approaches to the informed consent process by offering diagrams, pictures and other graphical representations instead of densely worded documents and truly integrate family-centered care during all phases.6 These alternative strategies can be used to tailor discussions related to clinical trial risk and benefit. Finally, techniques such as the teach-back method should be employed by nurses to ensure that explanations were effective.27
Acknowledgments
Jessica Keim-Malpass is a Translational Health Institute of Virginia (THRIV) scholar.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. IOM. Health Literacy: A Prescription to End Confusion. In: Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Washington, DC: The National Academies Press; 2004.
2. Davis TC, Williams MV, Marin E, Parker RM, Glass J. Health literacy and cancer communication. CA Cancer J Clin. 2002;52(3):134–149.
3. Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175–184. doi:10.1111/j.1525-1497.2005.40245.x
4. DeWalt D, Berkman N, Sheridan S, Lohr K, Pignone M. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004;19:1228–1239. doi:10.1111/j.1525-1497.2004.40153.x
5. Easton P, Entwistle VA, Williams B. How the stigma of low literacy can impair patient-professional spoken interactions and affect health: insights from a qualitative investigation. BMC Health Serv Res. 2013;13(1):319. doi:10.1186/1472-6963-13-319
6. Lambert V, Keogh D. Health literacy and its importance for effective communication. Part 2. Nurs Child Young People. 2014;26(4):32–36. doi:10.7748/ncyp2014.05.26.4.32.e387
7. Sudore R, Landefeld C, Williams B, Barnes B, Lindquist K, Schillinger D. Use of a modified informed consent process among vulnerable patients: a descriptive study. J Gen Intern Med. 2006;21(8):867–873. doi:10.1111/j.1525-1497.2006.00535.x
8. Tam N, Huy N, Thoa L, et al. Participants’ understanding of informed consent in clinical trials over three decades: systematic review and meta-analysis. Bull World Health Organ. 2015;93(3):1. doi:10.2471/BLT.14.141390
9. Dormandy E, Tsui EYL, Marteau TM. Development of a measure of informed choice suitable for use in low literacy populations. Patient Educ Couns. 2007;66(3):278–295. doi:10.1016/j.pec.2007.01.001
10. Doab A, Topp L, Day CA, Dore GJ, Maher L. Clinical trial literacy among injecting drug users in Sydney, Australia: a pilot study. Contemp Clin Trials. 2009;30(5):431–435. doi:10.1016/j.cct.2009.04.002
11. Kalkman S, van Thiel GJMW, Grobbee DE, Meinecke A-K, Zuidgeest MGP, van Delden JJM. Stakeholders’ views on the ethical challenges of pragmatic trials investigating pharmaceutical drugs. Trials. 2016;17(1):419. doi:10.1186/s13063-016-1546-3
12. Lantos JD, Wendler D, Septimus E, Wahba S, Madigan R, Bliss G. Considerations in the evaluation and determination of minimal risk in pragmatic clinical trials. Clin Trials. 2015;12(5):485–493. doi:10.1177/1740774515597687
13. Coyne C, Xu R, Raich P, et al. Randomized, controlled trial of an easy-to-read informed consent statement for clincial trial participation. J Clincial Oncol. 2003;21(5):836–842. doi:10.1200/JCO.2003.07.022
14. Davis T, Berkel H, Holcombe R, Pramanik S, Divers S. Informed consent for clincial trials: a comparative study of standard versus simplified forms. J Natl Cancer Inst. 1998;90(9):668–674. doi:10.1093/jnci/90.9.668
15. Evans K, Lewis M, Hudson S. The role of health literacy on African Amercan and Hispanic/Latino perspectives on cancer clincial trials. J Cancer Educ. 2011;27(2):1.
16. Kaiser B, Thomas G, Bowers B. A case study of engaging hard-to-reach participants in the research process: Community Advisors on Research Design and Strategies (CARDS). Res Nurs Health. 2016;40(1):70–79. doi:10.1002/nur.21753
17. Krieger JL, Neil JM, Strekalova YA, Sarge MA. Linguistic strategies for improving informed consent in clinical trials among low health literacy patients. J Natl Cancer Inst. 2017;109(3):djw233. doi:10.1093/jnci/djw233
18. Livaudis-Toman J, Burke N, Napoles A, Kaplan C. Health literate organizations: are clincial trial sites equipped to recruit minority and limited health literacy patients? J Heal Disparties Res Pract. 2014;7(4):1.
19. Polite BN, Cipriano-Steffens TM, Liao C, Miller EL, Arndt NL, Hahn EA. Investigation of a multimedia, computer-based approach to improve knowledge, attitudes, self-efficacy, and receptivity to cancer clinical trials among newly diagnosed patients with diverse health literacy skills. Cancer. 2019;125:2066–2075. doi:10.1002/cncr.31991
20. Powell L, Ojukwu E, Person S, Allison J, Rosal M, Lemon S. Psychometric development of the research and knowledge scale. Med Care. 2017;55(2):117–124. doi:10.1097/MLR.0000000000000629
21. Simonds V, Garroutte E, Buchwald D. Health literacy and informed consent materials: designed for documentation, not comprehension of health research. J Health Commun. 2017;22(8):682–691. doi:10.1080/10810730.2017.1341565
22. Kaplan CP, Nápoles AM, Narine S, et al. Knowledge and attitudes regarding clinical trials and willingness to participate among prostate cancer patients. Contemp Clin Trials. 2015;45:443–448. doi:10.1016/j.cct.2015.09.023
23. Andronis L, Billingham LJ, Bryan S, James ND, Barton PM. A practical application of value of information and prospective payback of research to prioritize evaluative research. Med Decis Making. 2016;36(3):321–334. doi:10.1177/0272989X15594369
24. Chinn D, McCarthy C. All Aspects of Health Literacy Scale (AAHLS): developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ Couns. 2013;90(2):247–253. doi:10.1016/j.pec.2012.10.019
25. Walsh MC, Trentham-Dietz A, Schroepfer TA, et al. Cancer information sources used by patients to inform and influence treatment decisions. J Health Commun. 2010;15(4):445–463. doi:10.1080/10810731003753109
26. Keim-Malpass J, Doede A, Kennedy C, Showalter S. Health literacy assessment: feasibility in a breast surgical oncology clinic. Clin J Oncol Nurs. 2017;21(3):384–386. doi:10.1188/17.CJON.384-386
27. Ballard D, Hill J. The nurse’s role in health literacy of patients with cancer. Clin J Oncol Nurs. 2016;20(3):232–234. doi:10.1188/16.CJON.232-234
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.