Back to Journals » Risk Management and Healthcare Policy » Volume 13
Health Insurance and Long-Term Care Services for the Disabled Elderly in China: Based on CHARLS Data
Received 9 October 2019
Accepted for publication 11 February 2020
Published 25 February 2020 Volume 2020:13 Pages 155—162
DOI https://doi.org/10.2147/RMHP.S233949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Linhong Chen, 1, 2 Xiaolu Zhang, 3 Xiaocang Xu 4
1Department of Applied Statistics, School of Mathematics and Statistics, Chongqing Technology and Business University, Chongqing 400067, People’s Republic of China; 2Department of Public Administration, School of Public Administration, Sichuan University, Chengdu 610065, People’s Republic of China; 3Department of Trade Economics, School of Economics, Chongqing Technology and Business University, Chongqing 400067, People’s Republic of China; 4Department of Economics, Research Center for Economy of Upper Reaches of the Yangtse River/School of Economics, Chongqing Technology and Business University, Chongqing 400067, People’s Republic of China
Correspondence: Xiaocang Xu
Research Center for Economy of Upper Reaches of the Yangtse River/School of Economics, Chongqing Technology and Business University, Chongqing 400067, People’s Republic of China
Tel +86-15178882448
Fax +86-023-62769376
Email [email protected]
Purpose: This paper aimed to explore the relationship between the different factors, especially health insurance, and the availability of long-term care (LTC) services, among the disabled elderly.
Methods: Based on the data of China Health and Retirement Longitudinal Study (CHARLS), the logistic regression model was utilized to evaluate the influence of the different factors, especially health insurance, on the availability of long-term care services.
Results: Our findings show some interesting results. Firstly, the findings suggest that informal long-term care (LTC) services for elderly persons with disabilities heavily depend on a family member from different health insurance groups. About 80.733% of the disabled elderly depend on a family member as their primary caregivers. Secondly, other influence factors such as income and area of residence were also significantly related to the availability of long-term rental services. Thirdly, Health insurance is a very important factor influencing the availability of Long-term care services both in urban and rural areas (p< 0.001) but Income is the most interesting variable.
Conclusion: Based on our results, the growth and integration of formal long-term care (LTC) services should be facilitated. Firstly, policymakers can encourage formal long-term care (LTC) services from a variety of sources to work together to increase overall supply capability. Secondly, the long-term living security needs of people who do not have health insurance should be regulated through subsidies according to the economic status.
Keywords: long-term care, LTC, the disabled elderly, health insurance, CHARLS data, informal care, formal care
Introduction
It is necessary to improve Long-Term Care (LTC) for the disabled elderly since it affords a wide range of health care fitting the needs of people whose life-ability is restrained due to chronic disease or injury.1 The disabled elders may obtain Long-Term Care services in form of formal or informal from well-trained specialists or laypeople severally in various settings: a family health facility, family members or friends; an adult day-care center in the community; assisted-living communities in the living environment; or daily care in institutions.
LTC demands in underdeveloped countries, including China, are growing at a rate much faster than that in developed countries.2 In recent years, China has to bear the long-term labor demand pressure brought by the aging of the population. China has the largest number of elderly people in the world (over 60 years old). In 2016, the elderly population exceeded 177 million, accounting for 13.26% of the total population.3 In addition, it is divined that the elderly population will reach about 480 million in 2053 (accounting for nearly 35% of the total population).4 As shown in Figure 1, the scale of elderly disability, who has difficulties in daily living activities (ADLs) or instrumental daily living activities (IADLs), has been increasing year by year, from 10.23 million in 2003 to 15.84 million in 2016, among which the rate of mild disability has increased the fastest, from 6.77 million in 2003 to 10.48 million in 2016.5
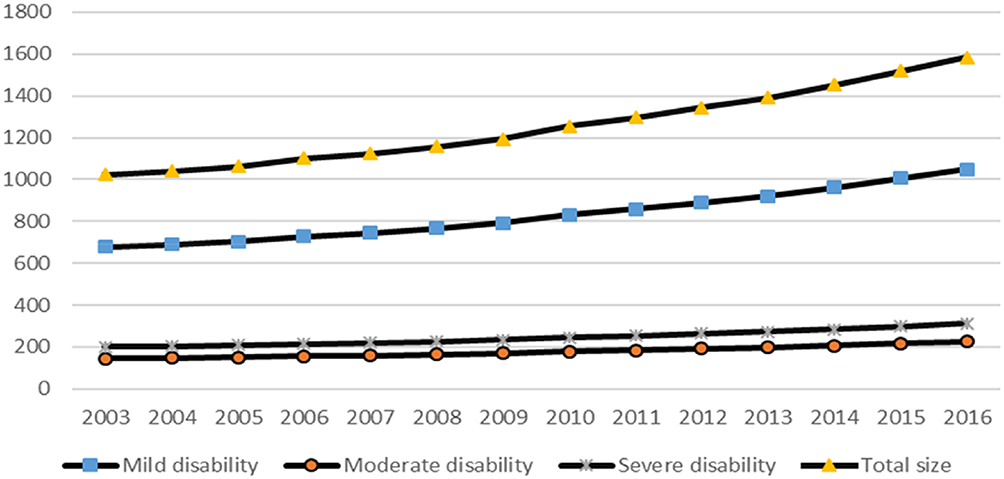 |
Figure 1 The scale of disability in the elderly over 65 in China from 2003–2016(unit:10,000). Note: Drew based on the data from “China population yearbook”. |
Previous researchers have revealed that the elderly is facing challenges to seek health care as a result of fewer caregivers.6–11 a) under the lure of the enlargement of urbanization, more and more young people migrate from rural to urban. it is challenging the family member of old people in urban or rural regions to balance their jobs and the informal support of their elderly parents;12 b) the one-child policy before 2016 in China has dramatically decreased the population extension over the past three decades and exhausted families’ ability to provide informal LTC services to fit LTC needs of the elderly.13,14 Thus, it is indicated that, as a result of the continuing trend of immigration, large numbers of the elderly may no longer depend on their children as a provenience of health care.
Therefore, the role of health insurance in long-term care services has come under increasing scrutiny. First, the public health departments, emphasizing that treatment spending is too expensive rather than cost-effective healthcare, is impossible to provide coordinated and seamless patient-centered services.15 Second, the rural population and urban residents without formal labor contracts are not entitled to any government-subsidized medical or social insurance.16,17 In recent years, the central government has made efforts to narrow the gap between different population groups in terms of health insurance. Some local governments have taken measures to abolish the free public medical care system and establish a unified social medical insurance system for employees, regardless of whether their employers are public or private. To reduce potential resistance.18 However, inequality still exists. Health insurance, as the main source of health and social care costs for older persons with varying intensity, frequency, and skilled care, and rehabilitation, have historically and contemptuously been unequal to different population groups. Therefore, in the process of using LTC services, depending on the level of health insurance enjoyed by the elderly, there may be a situation of co-existence of shortage and waste.19,20
In conclusion, growing number of the disabled elderly are incapable to meet the LTC services they need, which due to population aging, rapid urbanization, and the shortcomings of the medical insurance system. Therefore, it is of great significance to study the long-term care services, especially the role of health insurance in it. However, related studies are rare.21 The aim of this paper is to assess the influencing factors (especially health insurance) associated with the availability of Long-term care services for the disabled elderly in China. At the end of the paper, we also analyzed the differences between urban and rural areas.
Materials and Methods
Data Source and Variable Selection
China Health and Retirement Longitudinal Study (CHARLS), funded by Peking University (China), World Bank, and National Institute on Aging (China), is the raw data source for our research. It is a longitudinal questionnaire of national representativeness for the adults who over the age of 45 and covered their social, economic and health situation. CHARLS adopts multi-stage stratified Probability Proportionate to Size sampling (PPS) to generate a sampling framework. Many indicators were contained in the questionnaire of CHARLS: population structure and layout, family composition, health situation, and health service utilization, working situation, and insurance benefits, Household consumption level, and assets situation, etc. The latest data of CHARLS (2015) covered more than 10,000 families and 17,500 individuals from 150 districts of 28 provinces.22 The ethical approval is not required in this paper since CHARLS data is publicly available. Of course, registration application on its website (http://charls.pku.edu.cn) is required. Our account name is [email protected].
In this study, two dependent variables were used to represent the two main concepts of LTC availability in disabled elderly people.23 LTC availability includes: a) “the availability of social care” represents the extent to how disabled elderly people receive help to meet their daily needs. (Question: Are you satisfied with the help you receive when you encounter difficulties in your daily needs? All the answers are processed into two levels: Mild satisfied /dissatisfied; Highly satisfied). b) “the availability of health care” represents the primary source of care for elderly people once they become ill. (Question: Who do you get help from when you are sick?) The answers included three types: no health care at all, informal care providers such as a family member or friend, and formal care such as public or private social care suppliers need to pay for. It should be pointed out that the dependent variable was only included the availability of social care and not included the availability of health care due to the design of survey questions and the characteristics of the answers when we did multivariate logistic regression analysis of factors associated with the availability of Long-Term Care Services.
The core independent variable was health insurance, which was divided into three levels: a) health insurance with free public medical services (generous), b) public medical insurance (moderate), c) health insurance without medical insurance (no). In China, only the elderly who used to work as civil servants or public institutions can receive the pension paid in full by the central government. Their pension income replacement rate can be reached to 100%; The pension benefits of people with public pension insurance depend on the average income in the area where they live.
Other related control variables included gender (Question: What’s your gender?), family income (Question: What is the approximate annual income of your family? All the answers were processed into four levels:<50,000; 50,000–150,000; 150,000–300,000;>300,000 RMB), education (Question: How many years have you studied? There are three answer options: 0 years, 1–9 years, 10+ years), and living arrangements (Question: Who are you living with now? All the answers were processed into three categories: With family, Alone, In rest homes (or sanatoriums)).
For these variables, we processed the corresponding data of the CHARLS database samples. For example, in terms of missing values, we simply removed the samples with missing values since the CHARLS samples are large enough. Finally, 7787 valid samples were formed. of which 3945 come from urban and 3842 come from rural.
Empirical Method and Research Process
The empirical research method of this paper is Logistic regression, which is a generalized linear regression analysis model, often used in data mining, automatic disease diagnosis, economic prediction and other fields. For example, discussing the influencing factors that cause a certain variable, and predicting the probability of the occurrence of such variable according to the influencing factors. All the empirical analysis of data was performed by R software.
The research was conducted in four steps. First, descriptive statistics of dependent and independent variables were conducted. It should be noted that the samples selected in this paper are all above 60 age groups. Second, Apply each dependent variable to the weight of different Health insurance groups. Third, Multivariate logistic regression analysis of factors associated with the availability of social care and health care. Finally, we did the sub-regression analysis by urban and rural to discuss the different between them.
Results
Statistical Characteristics Analysis
Table 1 gives descriptive univariate information of all variables which filtered and processed from the 2015 CHARLS data according to the above processing methods and requirements.
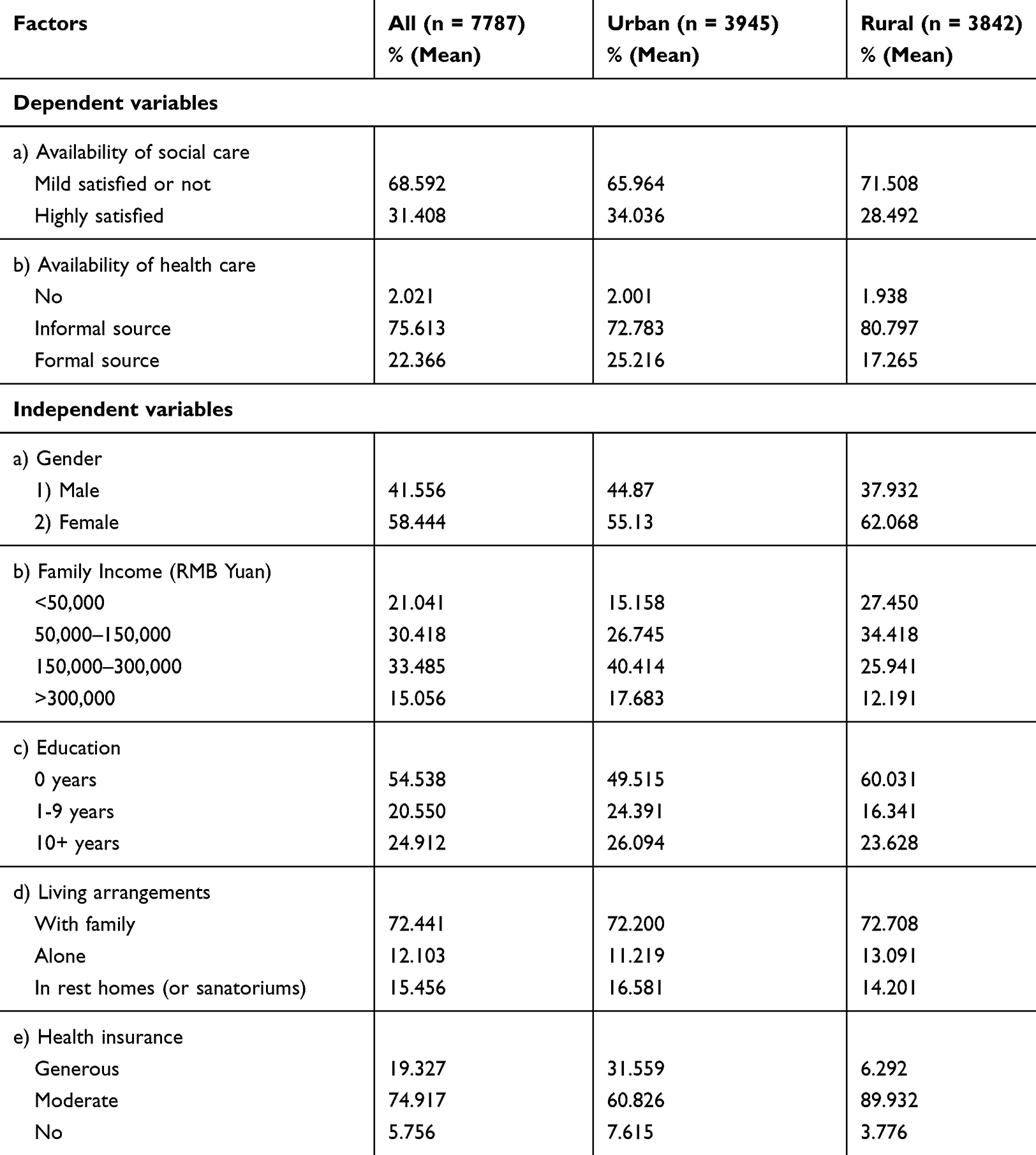 |
Table 1 Descriptive Univariate Information in the 2015 CHARLS Data |
In terms of dependent variables, about 68.592% of the disabled elderly think that the help received not fully meets their needs. About 75.613% of the disabled elderly have access to health care through informal channels, while about 22.366% have access to formal channels. In rural regions, about 80.797% of the disability elderly depend on informal sources and less than 20% receive formal sources of long-term health care.
In terms of independent variables, 58.444% of the disabled elderly are women and 54.538% of the disabled elderly have no higher education, and above 72.441% of the disabled elderly live with their families. 19.327% of the elderly disabled enjoy relatively high health insurance, and about 5.756% of the elderly disabled do not have endowment insurance and medical insurance. There are big differences in health insurance between urban and rural areas. Twenty-eight percent of the city disabled elderly enjoy generous health insurance. Only 6.292% of disabled old people in rural regions receive generous health insurance.
Availability of LTC Services in Different Health Insurance Groups
The previous analysis tells us that the role of health insurance in long-term care services has come under increasing scrutiny. Therefore, this part of the analysis is meaningful. As Table 2 shows, some of the results are very interesting.
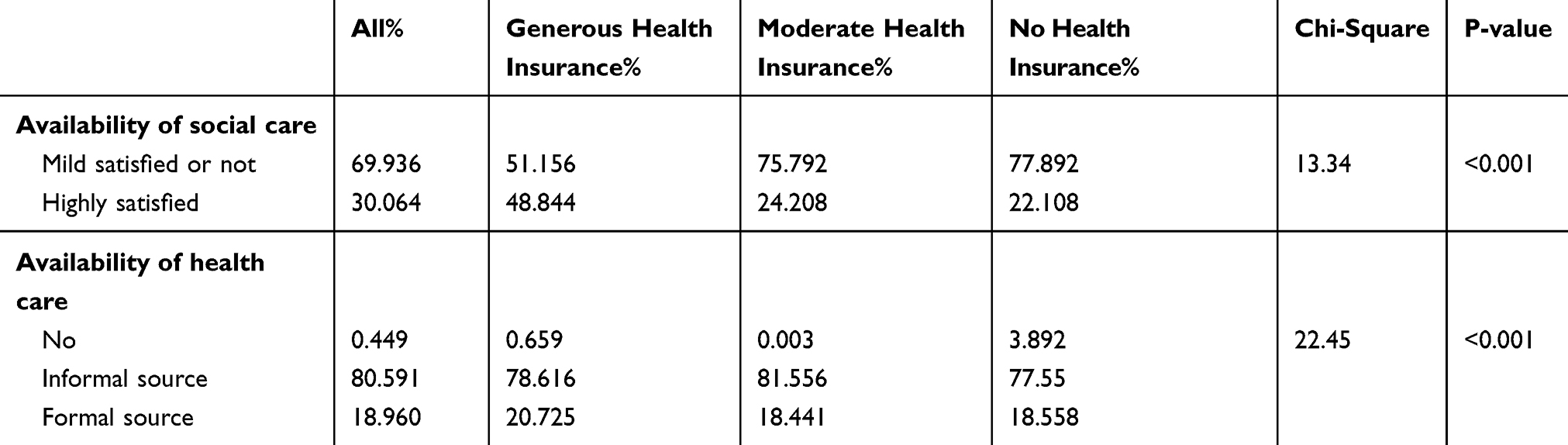 |
Table 2 Availability of LTC Services by Health Insurance (Weighted Percentages) |
In Table 2, key differences in the availability of social care can be able to compare between different Health insurance groups. Less than 70% of the disabled elderly received health insurance believe that social care slightly meets only or fails to meet their needs. Less than 25% of the disabled elderly with moderate (24.208%) or no (22.108%) health insurance think the help they received fully meet their needs. On the other hand, in terms of health care availability, Approximate 80% of the disabled elderly in these three groups must depend on informal sources to seek healthcare. About 3.892% of the disabled elderly who are not eligible for health insurance do not receive medical care.
Results of Logistic Regression
Table 3 presented the results of multiple regression about life-related factors related to the availability of Long-term care services.
- After controlling for the potential confounding effects of income, living arrangement and other factors, the availability of Long-term care services was obviously correlated with the health insurance. Compared with the generous health insurance group, the moderate and non-health insurance groups were 1.848 and 2.148 times more possibly to only meet the needs of LTC daily care, respectively.
- Compared with the first family income group (<50,000), other groups are 1.428, 1.632 and 1.884 times, respectively. But the gap between them was not statistically meaningful.
- Elderly people living alone was 1.536 times and in rest homes (or sanatoriums) was 2.496 times more possibly to be just moderately satisfied compared to those living with their families. Notably, there was no statistical meaningful between elderly people living alone and with their families.
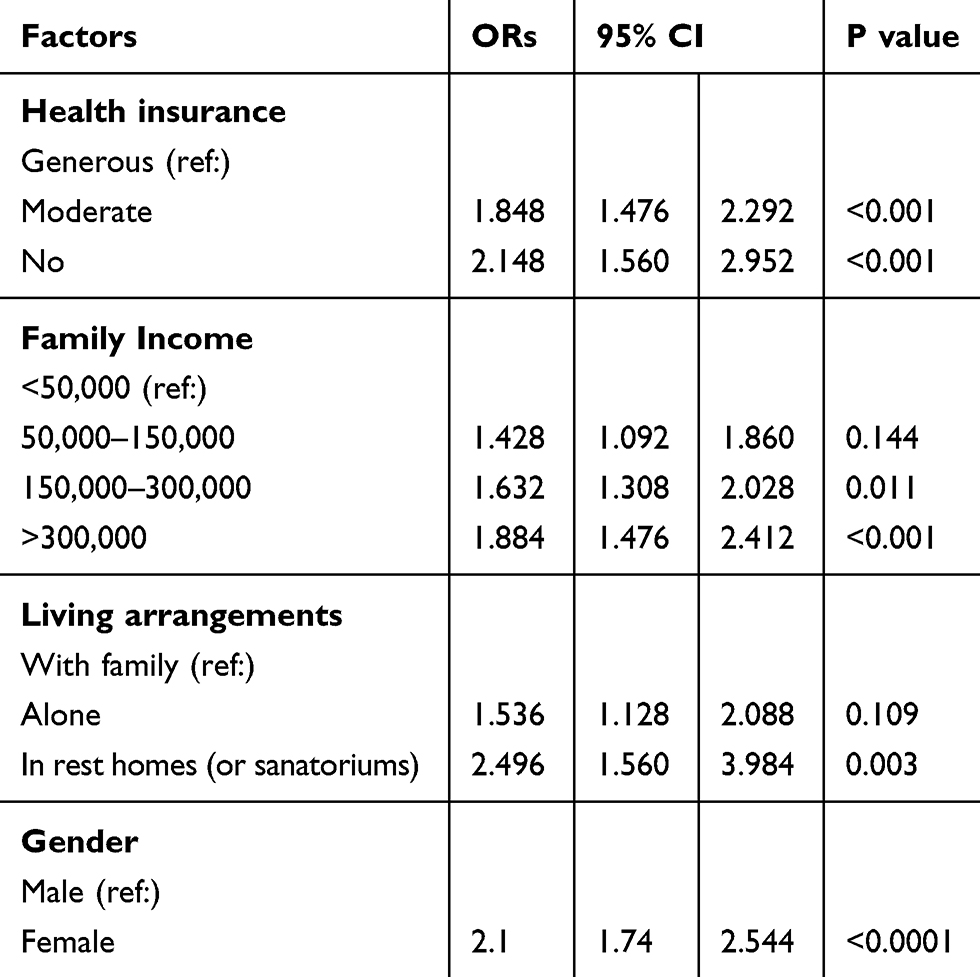 |
Table 3 Multivariate Analysis of Factors Associated with the Availability of Long-Term Care Services |
Table 3 also shows the factors related to generous health insurance and the availability of Long-term care services for gender. Women were significantly more satisfied with the availability of Long-term care services than men.
Sub-Regression Analysis by Urban and Rural
As shown in Table 1 above, it occurs some difference between urban and rural areas about the descriptive information of variables in CHARLS data. Therefore, it is necessary and meaningful to perform sub-regression analysis by urban and rural.
Table 4 reveals some interesting information. For instance, a) Health insurance is a very important factor influencing the availability of Long-term care services both in urban and rural areas(p<0.001) while the effect of other factors is not significant especially Living arrangements. b) Income is the most interesting variable influencing the availability of Long-term care services. In both urban and rural areas, the other family income three groups showed greater satisfaction with the availability of Long-term care services than the first group (<50,000). But it is not significant in the urban and very significant in the rural areas.
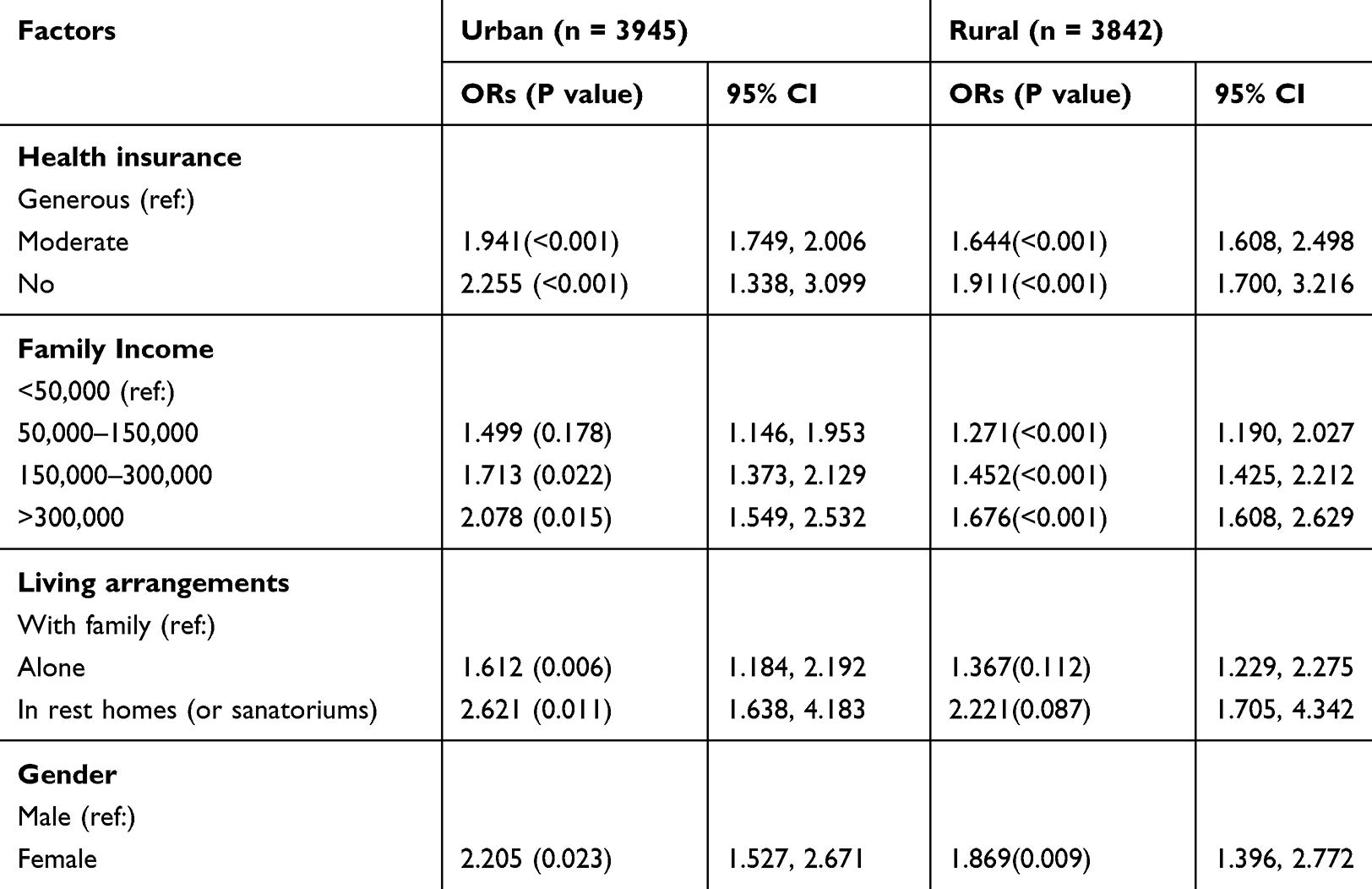 |
Table 4 Sub-Multivariate Analysis of Factors Associated with the Availability of Long-Term Care Services by the Differences Between Urban and Rural Areas |
Discussion
The aging population and rapid urbanization pose serious challenges to the long-term care services for the elderly in China. There are many factors that affect long term care services, such as gender, family income, living arrangements, etc. But buying health insurance is definitely one of the key factors. This paper is to explore the relationship between them and long-term care services.
Firstly, the findings suggest that informal LTC services for elderly persons with disabilities heavily depend on a family member from different health insurance groups. About 80.733% of the disabled elderly depend on a family member as their primary caregivers. The traditional informal LTC given by a family member may be more fragile or unsustainable because of the change in family construction Caused by the China child policy13 or the migration from rural to urban regions, and the shortage crisis is likely to worsen in the coming decades. In addition, our study found that those eligible for generous health insurance were more capable of affording long-term care services than those with modest health insurance or no health insurance at all. The disabled elderly does not have any health insurance, and the ability to pay for LTC services has been challenged, especially the vulnerable groups such as those without formal employment in their working life, and ordinary workers in rural areas.
Secondly, other influence factors such as income and area of residence were also significantly related to the availability of long-term rental services. Elderly people at a socio-economic disadvantage, that is, those with lower family incomes or rural people were more possibly to be unable to access satisfactory social daily care because they cannot afford them. This result is consistent with the imbalance of health insurance, which also reveals the unfairness of LTC provisions. In addition, Traditional values of filial piety have long meant that old parents should be cared for by their children24 and other houses, in general, pay more attention to the physical rather than psychological needs of the elderly.25
Thirdly, a sub-regression analysis by urban and rural was carried out at the end of empirical analysis. Some interesting information was revealed. For example, Health insurance is a very important factor influencing the availability of Long-term care services both in urban and rural areas (p<0.001) but Income is the most interesting variable. In both urban and rural areas, the other family income three groups showed greater satisfaction with the availability of Long-term care services than the first group (<50,000). But it is not significant in the urban and very significant in the rural areas.
To sum up, the development of LTC service in China has restricted by a lack of human resources the fragmentation of public services.26 In addition, long-term care services, particularly home-based healthcare and community-based day-care, are not directly covered by social medical insurance; As a result, disabled seniors must either depend on themselves or a family member to pay for long-term care or be forced to seek other potential resolutions. unnecessary hospitalizations and inappropriate delays in discharge are common throughout the country, especially in community health centers, as there are few high-quality and affordable LTC services for the disabled elderly with multiple chronic diseases.27 Therefore, without proper policy intervention, the sustainability of LTC systems may suffer severe challenges in the near future.
Therefore, governments should carry out relative policies endeavored to promote the development of LTC services in different styles and improve supply capability and quality by strengthening various services providers. Private capital should also be encouraged to play a significant role, in addition to public services organized and provided directly by government departments in the ministries of health and civil affairs. Fiscal subsidies, public procurement, and private supply through public-private partnerships, schooling or -job-training should be a policy option to promote the long-term credit sector.
Moreover, due to the influence of the one-child policy before 2016, the supply of informal LTC is possible to continue to decrease in the coming decades.12 Although the central government has issued the two-child policy after 2016, it seems that guaranteeing citizens freedom to choose the two-child policy without any conditions is not enough to stimulate the society desire to have more children.28,29
Conclusion
Based on our results, the growth and integration of formal LTC services should be facilitated. Firstly, policymakers can encourage formal LTC services from a variety of sources to work together to increase overall supply capability. At the same time, different types of long-term care services managed by different government departments, such as the ministry of health and civil affairs, should be integrated to afford coordinated and continuous healthcare for the disabled elderly. To improve the and accessibility of long-term care services for the elderly with disabilities, policymakers may consider instituting special social insurance for long-term care services or adding additional insurance to existing social medical insurance. Secondly, the long-term living security needs of people who do not fall within the scope of social security should be regulated through subsidies according to the economic status.
Acknowledgments
We thank the support by China Chongqing Education Commission Humanities and Social Sciences Research Project, grant number No: 19SKGH089; the MOE Project of Key Research Institute of Humanities and Social Sciences of Research Center for Economy of Upper Reaches of the Yangtse River “Research on agricultural modernization and industrial innovation and development”, grant number CJSYTD201710; Open subject of Collaborative Innovation Center for Urban Industries Development in Chengdu-Chongqing Economic Zone ”Study on spatiotemporal differences and influencing factors of low carbon agricultural productivity in China”, grant number KFJJ2019029; and thank Professor Timothy Kyng and Professor Fei Guo at Macquarie university, Feng Wei at University of Electronic Science and Technology of China for their thoughtful guidance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. United Nations. DESA/Population Division “World Population Prospects: The 2017 Revision, Key Findings and Advance Tables”; ESA/P/WP/248. San Francisco, CA, USA: United Nations; 2017.
2. Xu X, Chen L. Projection of long-term care costs in China, 2020–2050: based on the Bayesian quantile regression method. Sustainability. 2019;11(13):3530. doi:10.3390/su11133530
3. Xu X, Chen L. Influencing factors of disability among the elderly in China, 2003–2016: application of Bayesian quantile regression. J Med Econ. 2019;22(6):605–611. doi:10.1080/13696998.2019.1600525
4. Xu X, Xu Z, Chen L, Li C. How does industrial waste gas emission affect health care expenditure in different regions of china: an application of Bayesian quantile regression. Int J Environ Res Public Health. 2019;16(15):2748. doi:10.3390/ijerph16152748
5. Zeng L, Xu X, Zhang C, Chen L. Factors influencing long-term care service needs among the elderly based on the latest anderson model: a case study from the middle and upper reaches of the yangtze river. Healthcare. 2019;7(4):157. doi:10.3390/healthcare7040157
6. Xie H, Wang Z, Hou S, Jin X, Wang M, Shang S.The status of elderly care service needs and long-term care services strategies in China. Chin J Nurs. 2012;47(1):14–16.
7. Du J, Du X.Rural-urban migration and its impacts on familial old- support systems in sending areas. Popul Res. 2002;26(2):49–53.
8. Sun J. The issues in the long-term care for the left behind elders in rural areas during the work force migration. Popul J. 2006;4:14–18.
9. Zhang W, Li S. An analysis of the effects of labor emigration on supporting the aged family folks in rural China. China Soft Sci. 2004;8:34–39.
10. National Bureau of Statistics of the People’s Republic of China. Report on the survey of migrant workers in 2013. 2014; Available from: http://www.stats.gov.cn/tjsj/zxfb/201405/t20140512_551585.html.
11. Wu L. Inequality of pension arrangements among different segments of the labor force in China. J Aging Soc Policy. 2013;25:181–196. doi:10.1080/08959420.2012.735159
12. Phillips DR, Feng Z. Challenges for the ageing family in the People’s Republic of China. Can J Aging. 2015;34(3):290–304.
13. Zhan H, Liu G, Guan X. Willingness and availability: explaining new attitudes toward institutional elder care among Chinese elderly parents and their adult children. J Aging Stud. 2006;20:279–290. doi:10.1016/j.jaging.2005.09.006
14. Wu B, Mao Z-F, Zhong R. Long-term care arrangements in rural China: review of recent developments. J Am Med Dir Assoc. 2009;10:472–477. doi:10.1016/j.jamda.2009.07.008
15. Tang Y, Xu Y.Challenge, response and reflection: practice of long-term care for the oldest-old in China. Sci Res Aging. 2013;1(6):28–35.
16. Du F, Zhang T. Equity and efficiency issues of social security system in China. Study Explor. 2008;1:1–22.
17. Guan X. Analysis on the equity of the social security system in contemporary China. J Soochow Univ. 2013;3:1–9.
18. The Central People’s Government of the People’s Republic of China. Decision about the reform of the old age insurance for the public sector employees; 2015. Available from: http://www.gov.cn/zhengce/content/2015-01/14/content_9394.htm.
19. Liu N, Zeng L, Li Z, Wang J. Health-related quality of life and long-term care needs among elderly individuals living alone: a cross-sectional study in rural areas of Shaanxi Province, China. BMC Public Health. 2013;13:313. doi:10.1186/1471-2458-13-313
20. Kane RA. Long-term care and a good quality of life: bringing them closer together. Gerontologist. 2001;41(3):293–304. doi:10.1093/geront/41.3.293
21. Peng L, Zhixin F, Zhuochun W. The availability and affordability of long-term care for disabled older people in China: the issues related to inequalities in social security benefits. Arch Gerontol Geriatr. 2016;67:21–27. doi:10.1016/j.archger.2016.06.018
22. Xu X, Huang X, Zhang X, Chen L. Family economic burden of elderly chronic diseases: evidence from China. Healthcare. 2019;7(3):99. doi:10.3390/healthcare7030099
23. Chatterji S, Byles J, Cutler D, Seeman T, Verdes E. Health, functioning, and disability in older adults—present status and future implications. Lancet. 2015;385:563–575. doi:10.1016/S0140-6736(14)61462-8
24. Qu J, Wu X. Living arrangements and living willingness of the elderly in China. Sci Res Aging. 2013;1(2):[in Chinese].
25. Tang J, Li H, You J, Chen L, Zhao N. Counter measures and suggestion for improving the life quality of old people in nursing homes. Chin Gen Pract. 2009;12(1A):31–33.
26. Huang J, Meng F. Integrating pension service with medical service for the elderly: necessity, dilemmas and solutions. Chin J Health Policy. 2014;7(6):63–68.
27. Jiang J, Huang W, Wang Z, Zhang G. The effect of health on labour supply of rural elderly People in China—An empirical analysis using CHARLS data. Int J Environ Res Public Health. 2019;16:1195. doi:10.3390/ijerph16071195
28. Zhang L, Wang G. A research on the second childbirth expectation and the birth plan for the fertility age population of Chinese. Popul Economics. 2015;6:43–51.
29. Feng X, Li F. To have a second child or not?: the choice and its determinants of the urban population of childbearing age. J China Nat Sch Adm. 2016;1:94–101.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.