Back to Journals » International Medical Case Reports Journal » Volume 19
Hashimoto’s Thyroiditis with Subclinical Hypothyroidism and Multi-System Symptoms: A Case of a Middle-Aged Male
Authors Ahmed WA
Received 12 August 2025
Accepted for publication 30 December 2025
Published 8 January 2026 Volume 2026:19 558479
DOI https://doi.org/10.2147/IMCRJ.S558479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Waled AM Ahmed1,2
1Community Medicine Department, Faculty of Medicine, Al-Saeeda University, Sanaa, Yemen; 2Community Health Nursing Department, Faculty of Nursing, Al-Baha University, Al-Baha, Saudi Arabia
Correspondence: Waled AM Ahmed, Email [email protected]
Abstract: Hashimoto’s thyroiditis (HT) is a chronic autoimmune disease with lymphocytic infiltration of the thyroid gland and autoantibodies against endogenous components. A 45-year-old male professor at an academic institution with positive family history for autoimmune diseases among his brother and sister came to clinical hospital because of unspecific systemic symptoms, elevated TSH, low normal Free T4 (fT4), positivity autoantibodies against the thyroid gland. The biochemical signs of inflammatory process were shown in a report and image form ultrasound of thyroid gland, this indicates enlargement and thyroiditis. The case was diagnosed by elevated TSH, positive anti-TPO and thyroid ultrasound as subclinical stage of HT. The treating physician had prescribed 50 micrograms levothyroxine per day with selenium and zinc supplements. The case emphasizes early detection and integrative management based on our experience about importance for interdisciplinary diagnostics when it comes to autoimmune thyroiditis together with multi-system involvement and non-specific complaints.
Keywords: Hashimoto’s thyroiditis, anti-TPO antibodies, subclinical hypothyroidism, autoimmune disease, vitamin D deficiency, TSH, functional symptoms, HT
Introduction
Hashimoto’s thyroiditis (HT) is a chronic inflammatory autoimmune disorder associated with producing antithyroid antibodies.1,2 It is the most common cause of hypothyroidism in iodine-sufficient regions.3,4 It is often underdiagnosed in its early stages due to the nonspecific nature of symptoms.5,6 The disease has a strong autoimmune origin, with a high prevalence of antithyroid peroxidase (TPO) and antithyroglobulin (TG) antibodies.3,7
The previous studies have reported that the thyroid autoimmune disease is prevalent in women compared to men,8,9 non-alcoholic liver disease is prevalent among males compared to females with subclinical hypothyroidism.10 This highlights that the thyroid autoimmune conditions are most common in females while fatty liver associated disorders are commonly reported in males. However, the HT is prevalent in females,11 our case was a male middle aged. The unique features include that the case had presented typical subclinical symptoms with difficulty diagnosing the case.
In Arab communities, vitamin D deficiency is common due to several factors including limited exposure sun, dietary insufficiency, and cultural clothing practices.12 Recent studies have shown a significant link between vitamin D deficiency and occurrence of autoimmune thyroiditis, indicating that vitamin D plays a role in controlling immune system and thyroid function.9,13 In our case, the coincidence of vitamin D deficiency may have contributed to the occurrence of autoimmune thyroiditis.
As presented in recent systematic review investigated the local symptoms of HT, highlighted the gap in research on the HT, and indicated the early symptoms reported were thyroid discomfort, dysphagia, neck pain and throat discomfort.14 These reviews highlight the importance of early detection of the condition before further deterioration to late stages. In the light of previous knowledge, we presented this case study of HT in an attempt to define the clinical features and any potent association of with other autoimmune conditions.
Case Description
A middle-aged male with a positive family history of undiagnosed autoimmune conditions was presented in this case study. The case complains of overweight, fatty liver, high lipid profile and allergy for unknown reasons for three years. Antihistamine and anti-lipid medications were prescribed for previous year with no significant improvement. Recently he presented with low back pain, persistent fatigue, gastrointestinal disturbances, chronic allergic symptoms (sinusitis, itching), anxiety and cognitive fog.
As shown in Table 1 the case of HT with subclinical hypothyroidism was diagnosed by positive anti-TPO and thyroid ultrasound associated with vitamin D deficiency and mild systemic inflammation (elevated CRP, ESR), and positive h. pylori, additionally with coexisting ANA positivity (AC-4/5 pattern) indicating possible poly autoimmunity.
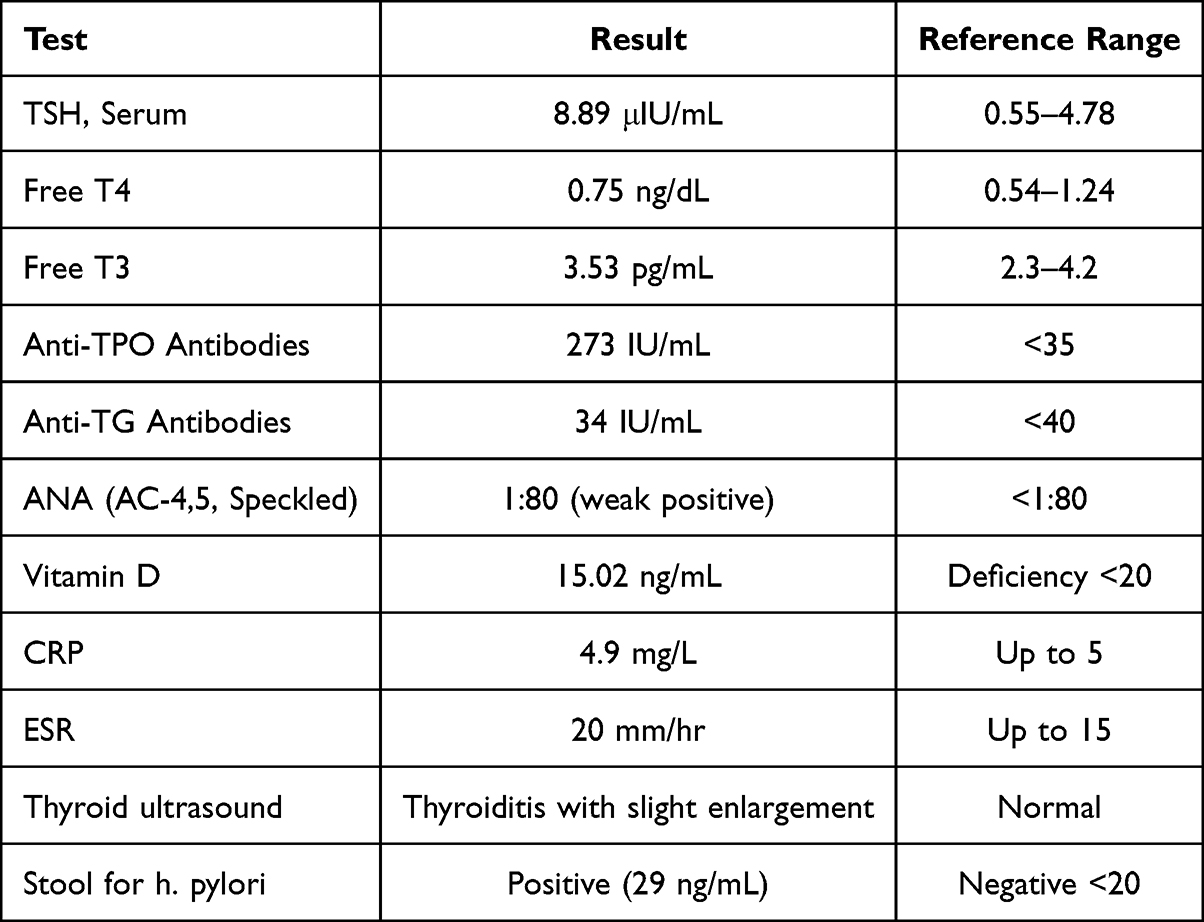 |
Table 1 Laboratory Investigations of the Case of HT |
The thyroid ultrasound was conducted for this case to confirm the diagnosis and to be the baseline for frequent follow up. As shown in Figure 1, the case has thyroiditis with slight enlargement. It also indicates that the case is active and the deterioration of thyroid function has been detected.
 |
Figure 1 Thyroid ultrasound for as case of HT. It shows a case of thyroiditis with slight enlargement. |
Management and Follow-Up
The patient was then started on a gluten-free, anti-inflammatory, elimination diet specific for autoimmune and histamine intolerance. He also was advised to start levothyroxine 50 microgram tablets as early morning. The monitoring of the thyroid function should be done every 6–8 weeks to measure the progress of the condition.
Initially the treatment was to address H. pylori infection with gastroenterologist consultation with a combination of metronidazole, tetracycline hydrochloride, bismuth subcitrate potassium and Xanprazan 20mg. The treating doctor also prescribed a vitamin D supplementation (50,000 IU weekly for 8 weeks), selenium 200 microgram daily for three months in addition to other supplements including zinc, vitamin b complex and ferrus sulphate.
Discussion
In this case, there were markedly elevation of anti‑TPO level (273 IU/mL), and TSH (8.89 μIU/mL), and associated with borderline anti‑Tg (34 IU/mL), is criteria for diagnosis of a case of HT. In more than 90% of patients exhibit anti‑TPO positivity in case of autoimmune thyroiditis.15 The pattern of elevated TSH (8.89 μIU/mL) with low‑normal Free T4 suggests a stage of subclinical hypothyroidism, consistent with typical characteristics in Hashimoto’s conditions.
Despite normal Free T3 (3.53 pg/mL), immunoassay testing of free hormones can overestimate levels, particularly at lower concentrations. This highlights the significance of using TSH level as the most sensitive screening tool and monitoring for Hashimoto’s cases and indicates that tissue-level thyroid activity may already be inadequate. The diagnosis of HT was usually done by high level of TSH and Anti-TPO in addition to alteration in thyroid using thyroid ultrasound.3
The vitamin D level of our patient of 15 ng/mL (deficient) aligns with previous findings linking vitamin D deficiency to HT.9,12,13,16 A systematic review on the association between vitamin D deficiency and HT had indicated that vitamin D deficiency could increase the risk of developing of HT.13 In addition to the association, vitamin D deficiency was found in other autoimmune conditions.16 Although autoimmunity is significantly linked with deficiency of vitamin D,16 a systematic review of randomized controlled trials have yielded that vitamin D supplementation is not significantly associated with improvement in thyroid hormones and TSH levels.17
In the Arab communities, specifically in Saudi Arabia, United Arab Emirates and Yemen, several studies have been conducted, they reported a high prevalence of vitamin D deficiency,18–21 which may play an essential role in the development of autoimmune diseases, including HT. Vitamin D also linked to autoimmune thyroiditis, influencing the thyroid and autoimmune functions.8,13,16,22,23 A previous review has reported that patients with HT have significantly lower levels of vitamin D compared to people with normal vitamin D levels, highlighting its role in developing HT.24–26
Levothyroxine therapy may decrease anti‑TPO antibody titers in long-term, although the restoration is complete in only a minority of patients. With the modest level of antibody while still in early-stage hypothyroidism, it seems appropriate to keep an eye on such and expect a gradual decline with treatment. Previous studies have shown that autoantibodies declines with levothyroxine long term treatment,27 and with selenium supplementation.28 This underscores the role of thyroid hormones and nutritional supplementations are essential for treating autoimmune thyroiditis.
The findings reported in this case were consistent with literature and represent the importance of early detection and appropriate management of autoimmune conditions. Generalizability may be less as this case was a male whereas HT is prevalent among females, another limitation was that this case was observed for short period of time, a need for follow up report to assess the long-term effect of early interventions with vitamin D, zinc, and selenium supplements with levothyroxine in minimizing thyroid antibodies.
Conclusion
This case of male HT illustrates the diagnostic difficulty in detecting TH from other conditions of hypothyroidism in men and underscores the importance of a routine comprehensive metabolic and hormonal assessment of middle age population. The improvement in subclinical symptoms and laboratory investigations after starting vitamin D supplementation with thyroid hormone replacement further highlights the relationship between vitamin D deficiency and thyroid autoimmune diseases. The case highlights that males could also have a risk of developing HT.
Ethical Considerations
The author did not get approval from ethical board because the case has provided signed consent to publish the information, and the hospital provided permission for studying the case details and a written permission from the hospital to study the case was obtained. The author also adhered to the guidelines of Helsinki.
Consent for Publication
The adult patient of this case had provided written consent for publication of the case details.
Informed Consent Statement
Informed written consent was obtained from the case involved in the study.
Acknowledgments
The author expresses his gratitude to the included patient for his cooperation and support.
Funding
This work is not funded by any agency or institution.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Li J, Huang Q, Sun S, et al. Thyroid antibodies in Hashimoto’s thyroiditis patients are positively associated with inflammation and multiple symptoms. Sci Rep. 2024;14(1):27902. doi:10.1038/s41598-024-78938-7
2. Weetman A. An update on the pathogenesis of Hashimoto’s thyroiditis. J Endocrinol Investigation. 2021;44(5):883–5. doi:10.1007/s40618-020-01477-1
3. Ragusa F, Fallahi P, Elia G, et al. Hashimotos’ thyroiditis: epidemiology, pathogenesis, clinic and therapy. Best Pract Res Clin Endocrinol Metabolism. 2019;33(6):101367. doi:10.1016/j.beem.2019.101367
4. Wiersinga WM. Hashimoto’s thyroiditis. In: Thyroid Diseases. Springer; 2016:1–44.
5. Gottwald-Hostalek U, Schulte B. Low awareness and under-diagnosis of hypothyroidism. Curr Med Res Opin. 2022;38(1):59–64. doi:10.1080/03007995.2021.1997258
6. Chiovato L, Magri F, Carlé A. Hypothyroidism in context: where we’ve been and where we’re going. Adv Ther. 2019;36(Suppl 2):47–58. doi:10.1007/s12325-019-01080-8
7. Boutzios G, Koukoulioti E, Goules AV, et al. Hashimoto thyroiditis, anti-parietal cell antibodies: associations with autoimmune diseases and malignancies. Front Endocrinol. 2022;13:860880. doi:10.3389/fendo.2022.860880
8. Luca Chiovato PL, Fiore E, Tonacchera M, Pinchera A. Thyroid autoimmunity and female gender. J Endocrinol Investigation. 2014;16:384–391. doi:10.1007/BF03348863
9. Turashvili N, Javashvili L, Giorgadze E. Vitamin D deficiency is more common in women with autoimmune thyroiditis: a retrospective study. Int J Endocrinol. 2021;2021(1):4465563. doi:10.1155/2021/4465563
10. Lee J, Ha J, Jo K, et al. Male-specific association between subclinical hypothyroidism and the risk of non-alcoholic fatty liver disease estimated by hepatic steatosis index: Korea National Health and Nutrition Examination Survey 2013 to 2015. Sci Rep. 2018;8(1):15145. doi:10.1038/s41598-018-32245-0
11. Hu X, Chen Y, Shen Y, Tian R, Sheng Y, Que H. Global prevalence and epidemiological trends of Hashimoto’s thyroiditis in adults: a systematic review and meta-analysis. Front Public Health. 2022;10:1020709. doi:10.3389/fpubh.2022.1020709
12. Hassan AB, Alamien SH, Khalil NA, et al. Prevalence of vitamin D deficiency in the Arab countries: a systematic review and meta-analysis. Discov Public Health. 2025;22(1):1–27. doi:10.1186/s12982-025-00993-w
13. Khozam SA, Sumaili AM, Alflan MA, RAaS S, Sumaili A. Association between vitamin D deficiency and autoimmune thyroid disorder: a systematic review. Cureus. 2022;14(6). doi:10.7759/cureus.25869
14. Yuan J, Qi S, Zhang X, et al. Local symptoms of Hashimoto’s thyroiditis: a systematic review. Front Endocrinol. 2023;13:1076793. doi:10.3389/fendo.2022.1076793
15. Mohamed AI, Ali AE, Abdrabo AA. Prevalence of positive thyroid peroxidase antibodies (anti-TPO) in patients diagnosed with hypothyroidism. J Med Life Sci. 2025;7(2):270–280.
16. Durá-Travé T, Gallinas-Victoriano F. Autoimmune thyroiditis and vitamin D. Int J Mol Sci. 2024;25(6):3154. doi:10.3390/ijms25063154
17. Safari S, Shojaei-Zarghani S, Molani-Gol R, Rafraf M, Malekian M. Effects of vitamin D supplementation on TSH and thyroid hormones: a systematic review of randomized controlled trials. Endocrinología, Diabetes y Nutrición. 2025;72(1):37–46. doi:10.1016/j.endinu.2024.07.007
18. Alharbi HF, Rezq KA. Vitamin D supplementation in Saudi Arabia: mothers’ knowledge, practices, and attitudes. PeerJ. 2025;
19. Madkhali Y, Janakiraman B, Alsubaie F, et al. Prevalence and trends of vitamin D deficiency in a Saudi Arabian population: a five-years retrospective study from 2017 to 2021. Front Public Health. 2025;13:1535980. doi:10.3389/fpubh.2025.1535980
20. Al-Shami AS, Omar A. Association between thyroid disorder and vitamin D among Yemeni patients; 2025.
21. Tahir H, Nazir N, Tanvir S. Effect of vitamin D supplementation on thyroid function tests in hypothyroid patients: a six-month study at Pakistan Emirates Military Hospital Rawalpindi. Pak J Med Cardiol Rev. 2025;4(1):18–28.
22. Czarnywojtek A, Florek E, Pietrończyk K, et al. The role of vitamin D in autoimmune thyroid diseases: a narrative review. J Clin Med. 2023;12(4):1452. doi:10.3390/jcm12041452
23. Kivity S, Agmon-Levin N, Zisappl M, et al. Vitamin D and autoimmune thyroid diseases. Cell Mol Immunol. 2011;8(3):243–247. doi:10.1038/cmi.2010.73
24. Zhang J, Chen Y, Li H, Li H. Effects of vitamin D on thyroid autoimmunity markers in Hashimoto’s thyroiditis: systematic review and meta-analysis. J Int Med Res. 2021;49(12):03000605211060675. doi:10.1177/03000605211060675
25. Kim D. The role of vitamin D in thyroid diseases. Int J Mol Sci. 2017;18(9):1949. doi:10.3390/ijms18091949
26. Krysiak R, Szkróbka W, Okopień B. The effect of vitamin D on thyroid autoimmunity in levothyroxine-treated women with Hashimoto’s thyroiditis and normal vitamin D status. Exp Clin Endocrinol Diabetes. 2017;125(04):229–233. doi:10.1055/s-0042-123038
27. Schmidt M, Voell M, Rahlff I, et al. Long-term follow-up of antithyroid peroxidase antibodies in patients with chronic autoimmune thyroiditis (Hashimoto’s thyroiditis) treated with levothyroxine. Thyroid. 2008;18(7):755–760. doi:10.1089/thy.2008.0008
28. Wichman J, Winther KH, Bonnema SJ, Hegedüs L. Selenium supplementation significantly reduces thyroid autoantibody levels in patients with chronic autoimmune thyroiditis: a systematic review and meta-analysis. Thyroid. 2016;26(12):1681–1692. doi:10.1089/thy.2016.0256
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.