Back to Journals » Substance Abuse and Rehabilitation » Volume 13
Harmful Alcohol Use Among Patients with Tuberculosis in Gedeo Zone, Southern Ethiopia
Authors Yohannes K ![]() , Ayano G, Toitole KK
, Ayano G, Toitole KK ![]() , Teferi HM, Mokona H
, Teferi HM, Mokona H ![]()
Received 3 August 2022
Accepted for publication 23 November 2022
Published 14 December 2022 Volume 2022:13 Pages 117—125
DOI https://doi.org/10.2147/SAR.S384921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Parry
Kalkidan Yohannes,1 Getinet Ayano,2,3 Kusse Koirita Toitole,4 Henok Mulatu Teferi,5 Hirbaye Mokona1,6
1Department of Psychiatry, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia; 2Research and Training Department, Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia; 3School of Population Health, Curtin University, Perth, WA, Australia; 4Arba Minch General Hospital, Arba Minch, Ethiopia; 5Mohammed Akile Memorial General Hospital, Amibara, Afar, Ethiopia; 6Department of Psychiatry, College of Medicine and Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Kalkidan Yohannes, Department of Psychiatry, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia, Email [email protected]
Introduction: Alcohol consumption among patients with tuberculosis is on the rise. There is evidence that alcohol consumption negatively affects treatment outcomes for these populations. Due to this, a substantial number of people relapse, withdraw from treatment, or even die as a result of their alcohol addiction. Despite this, little research has been conducted on the factors associated with the harmful use of alcohol by this group of people in Ethiopia. The purpose of this study was to determine the prevalence and associated factors of harmful alcohol use among patients with tuberculosis in the Gedeo Zone, southern Ethiopia.
Methods: A cross-sectional study was conducted at healthcare facilities. Four hundred and fifteen participants aged 18 and older were recruited using a systematic random sampling method. Data on sociodemographic factors, clinical factors, social support, perceptions of the stigma associated with tuberculosis, and depression were collected using structured and validated instruments. Measurement of harmful alcohol consumption was conducted using the AUDIT.
Results: The prevalence of harmful alcohol use among tuberculosis patients was 20% (95% CI; 16.1– 24.2%). There is a significant correlation between medical comorbidity (AOR = 2.44, 95% CI: 1.29– 4.62), disease duration (≥ 12 months) (AOR = 2.88, 95% CI: 1.03– 3.04), and being male (AOR = 2.10, 95% CI: 1.17– 3.77) with harmful alcohol consumption.
Conclusion: Our study revealed that alcohol consumption was high among tuberculosis patients. The presence of comorbidities, being male, and having a long-term illness were significant predictors of harmful alcohol consumption. It is imperative to screen patients who have suffered from chronic tuberculosis for an extended period of time. It is also pertinent to screen patients with comorbid medical conditions for alcohol abuse. Screening for alcohol abuse at an early stage can prevent poor treatment outcomes as well as the effects of comorbid medical conditions and harmful use of alcohol.
Keywords: harmful alcohol use, tuberculosis patients, Ethiopia, prevalence, tuberculosis, alcohol use
Background
In 2016, alcohol caused 3 million deaths worldwide (5.3% of all deaths) and 132.6 million disability-adjusted life years (DALYs)1 and it has been associated with adverse clinical outcomes among people with medical conditions.1,2 Alcohol is a psychoactive substance that has toxic and addictive properties.3,4 When used on an acute or chronic basis, it can affect a wide range of neurochemical systems.5
Harmful alcohol use is defined as
a pattern of alcohol use that has caused damage to a person’s physical or mental health or has resulted in behaviour leading to harm to the health of others.6
According to the World Health Organization,7 alcohol consumption contributed to 10% of deaths among people aged 15–49 in 2016. A higher mortality rate is associated with higher alcohol consumption.8 Approximately 5.1% of the global disease burden can be attributed to the adverse effects of harmful alcohol consumption.9 According to the World Health Organization, harmful alcohol use results in approximately 3 million deaths and 132.6 million disability-adjusted life years (DALYs).7
Furthermore, there is an increasing prevalence of alcohol consumption among patients with tuberculosis (TB), making it necessary to identify the extent and factors associated with risky alcohol consumption.7 Aside from increasing the likelihood of contracting TB threefold, excessive alcohol consumption is also associated with poor adherence to TB treatment.1 TB is one of the communicable diseases that is transmitted from person to person through tiny droplets that become airborne through coughing and sneezing.10 Mycobacterium TB is responsible for causing it.10
TB is one of the top 10 causes of death worldwide and the leading infectious cause of death (after HIV/AIDS). Globally, 9.0–11.1 million people contracted TB disease in 2017: 5.8 million men, 3.2 million women, and 1.0 million children.11 There were an estimated 1.2 million (range, 1.1–1.3 million) TB deaths among HIV-negative people in 2018 (27% reduction from 1.7 million in 2000), and an additional 25 1000 deaths (range, 223 000–281 000) among HIV positive people.12
Alcohol consumption among patients with TB has been associated with poor treatment compliance and failure, leading to treatment discontinuation, drug-resistant tuberculosis, and death.4,13–15 Alcohol consumption is also associated with a decrease in the immune system function of tuberculosis patients. Consequently, there is a much higher risk of active tuberculosis,11–17 death during treatment,18 positive smear results,19 higher rates of homelessness,20 and more treatment-resistant cases.21 As such, it is crucial to identify and treat alcohol problems as early as possible in tuberculosis patients. This will enable us to reduce and possibly prevent the adverse outcomes associated with the disease. Few studies have examined the prevalence of harmful alcohol use and its associated factors among patients with tuberculosis in Africa. There is, in particular, a paucity of data regarding alcohol use and tuberculosis in Ethiopia. The purpose of this study was to assess the prevalence and associated factors of harmful alcohol consumption among tuberculosis patients in Gedeo Zone, in the Southern Nations, Nationalities, and Peoples’ Region of Ethiopia.
Methods
Study Design and Setting
The study was conducted between November 1, 2018, and December 30, 2018, in Yirgacheffe, Wonago, and Dilla Zuriya districts in the Gedeo Zone. The Gedeo Zone is located in the Southern Ethiopia region, 359 kilometers southeast of Addis Ababa (the capital of Ethiopia). The Zone has 42 public health facilities, including a referral hospital, 2 primary hospitals, and 39 health centers.
Study Population
The study population consisted of all patients with TB who presented to the TB clinic. All individuals with tuberculosis who were available during the survey were included in the sample. This study included patients who had been taking TB medications for at least two weeks. Those patients who were seriously ill at the time of the study were excluded from the study.
Sample Size Determination and Sampling Procedure
The study was part of a more extensive study that examined depressive symptoms and their associated factors among patients with tuberculosis who presented to public health facilities in the Gedeo district, southern Ethiopia. In this study, we used the sample size calculated for depression based on the following assumptions: 95% confidence level, 5% margin of error, and 43.3% prevalence depression in Ethiopia.22
A total sample size of 415 was calculated based on a 10% non-response rate. Participants were assigned to each health facility proportionally based on the number of patients reported in the previous year’s annual reports. The participants were selected through a systematic random selection process.
Instruments and Procedures
Data was collected through face-to-face interviews using a structured, standardized questionnaire. The questionnaires included sociodemographic data, the Patient Health Questionnaire-9 (PHQ-9),23 the Oslo Social Support Scale-3,24 and structured questions to examine related factors. Nurses and public health workers in the tuberculosis clinic collected the data.
The Oslo Social Support Scale-3 was used to measure the level of social support. The OSSS-3 consists of three items: the number of close confidants you have, the sense of concern that other people have for you, and the connection that you have with your neighbors. There is a range of scores ranging from 3 to 14, with a high score representing a high level of social support and a low score representing a low level of social support. According to the OSSS-3 sum score, we classified the different types of social support into three broad categories based on the type of social support they provided. Among the ranges are: From 3 to 8, poor social support; from 9 to 11, moderate social support; and from 12 to 14, strong social support.25
In order to gather information on the perceived stigma of tuberculosis, 11-item perceived tuberculosis stigma scale composed of Likert scale questions regarding the perception of loneliness, guilt, shame, and the disclosure of the patient’s tuberculosis status was used in the current study. Perceived TB stigma scale is composed of 11 items, which are rated on a Likert scale of one to four, with 1 being strongly disagree and 4 being strongly agree.26
We collected data on depression using the Patient Health Questionnaire (PHQ-9) to gather information about the condition. There are nine items in the PHQ-9 that can be used to screen depression based on the Diagnostic Statistical Manual-IV criteria. The PHQ-9 has been found to have a sensitivity value of 67% and a specificity value of 86%. Depression is indicated by a score of 10 or more out of 27 on the scale.23
We measured harmful alcohol use using AUDIT items, with a cut-off point of eight or higher.27 Alcohol Disorder Identification Test (AUDIT) is a ten-item assessment tool designed to assess the extent of alcohol consumption, alcohol dependence symptoms, and problems associated with alcohol consumption. The AUDIT contains ten items, each scored on a Likert scale from 0 to 4, with a maximum score of 40. An AUDIT score of eight or higher indicates a tendency to use alcohol in a hazardous or harmful manner. A score of more than eight indicates harmful alcohol consumption in patients with tuberculosis. Two language experts translated the AUDIT into Amharic and back into English, and mental health professionals checked the consistency of the questionnaire. Data quality was ensured through the design and modification of the questionnaire. A pre-test was conducted on 5% of the sample. The principal investigator and supervisors monitored the data collection daily.
Ethical Considerations
Dilla University College of Health and Medical Science Institutional Review Board has approved this study. In each of the districts (Yirgacheffe District, Wonago District, and Dilla Zuriya District), the health departments and health centers authorized the conduct of the interviews. Participants were informed of the purpose of the study. Each interview was preceded by the participants’ written informed consent form. Reports and other documents did not include the names of participants. We followed the Helsinki Declaration in the conduct of this study.
Data Analysis
Data were prepared, coded, and entered into SPSS-20. The data were summarized using means, frequencies, and percentages. A bivariate and multivariable logistic regression analysis was conducted in this study to assess the factors associated with harmful alcohol consumption. The odds ratio, as well as their 95% confidence intervals, were calculated to determine the strength of the association. A significance level of P<0.05 was used.
Results
Sociodemographic and Economic Characteristics
A total of 409 participants were interviewed, of whom 252 (61.6%) were males. More than fifty percent of the participants lived in rural areas. Sixty-six percent of the participants were employed by the government or were in private business. More than half of the participants were under the age of 30 years, and more than 50% were married. Among the participants, 22.5% had not attended formal education, 40.3% had primary education, while more than a third, 37.2%, had secondary education or higher. The majority of participants earned an income of approximately 1539 ETB per month, and 21.8% earned more than 1539 ETB per month (Table 1).
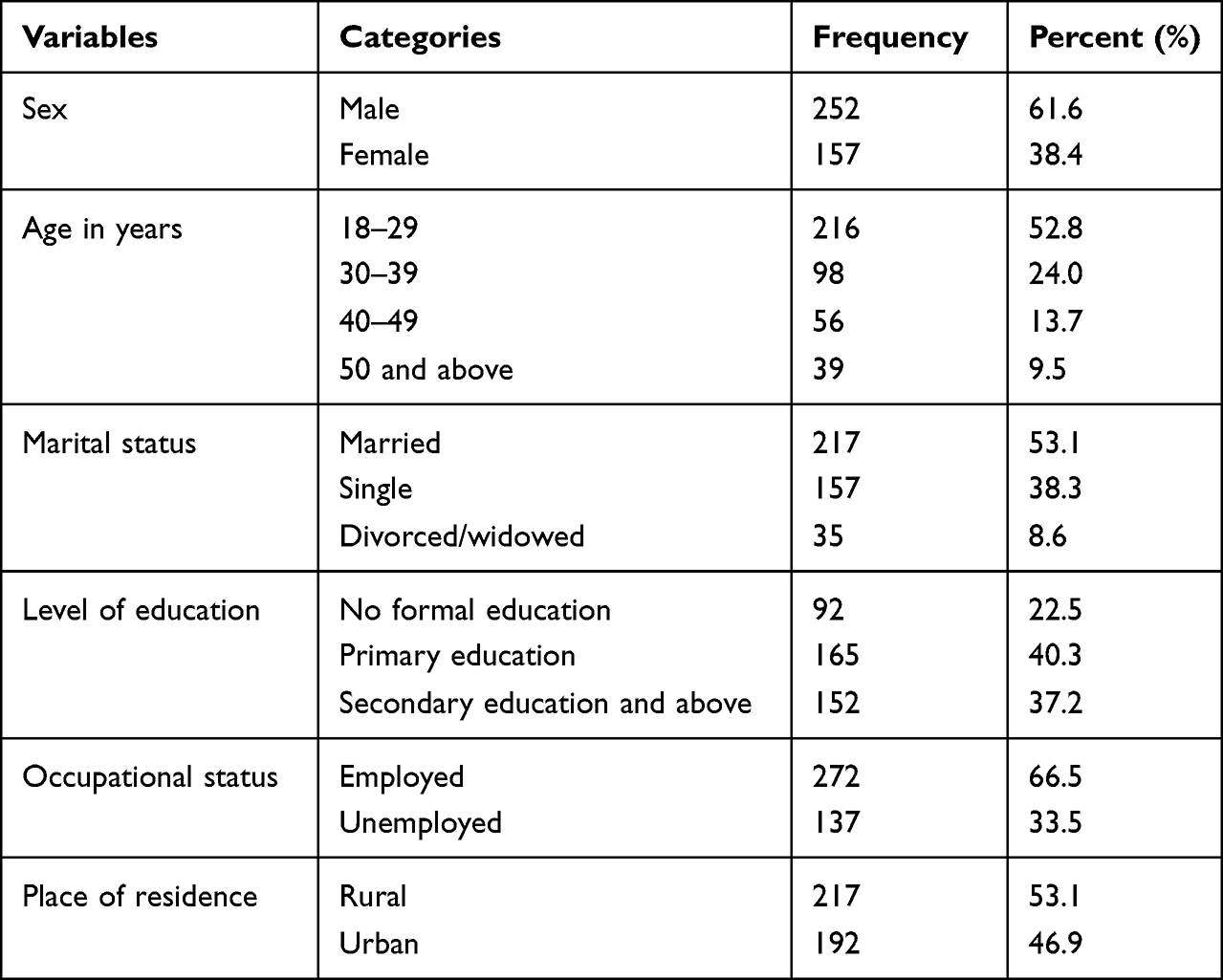 |
Table 1 Socio-Demographic Characteristics of Patients Attending Tuberculosis Unit of Public Health Facilities, Gedeo Zone, Southern Ethiopia, 2018 (n = 409) |
The Respondents’ Psychosocial and Clinical Characteristics
About one-third of the respondents had poor social support, while 177 (43.1%) had intermediate support. More than one-third of the participants in the study (159, 38.9%) perceived TB stigma, while a significantly larger group (61.6%, n = 250) perceived no stigma associated with TB. The proportion of participants with pulmonary tuberculosis (73.8%, n = 302) in the intensive phase of treatment (61.6%, n = 250) was 73.8%.
Most participants (77%, n = 315) adhered moderately to their tuberculosis treatment. Most of the sample consisted of newly diagnosed tuberculosis cases, while 15.2% required re-treatment.
Additionally to TB, 71 (17.4%) participants were HIV positive, and 22 had co-morbid chronic illnesses, such as hypertension (n = 6), heart disease (n = 10), diabetes mellitus (n = 2), and kidney disease (n = 4). Only 5.1% of the population had a family history of mental illness. Two hundred thirty-six (57.7%) were interviewed within 6–12 months of their illness. In addition, nearly half of the participants reported symptoms of depression (Table 2).
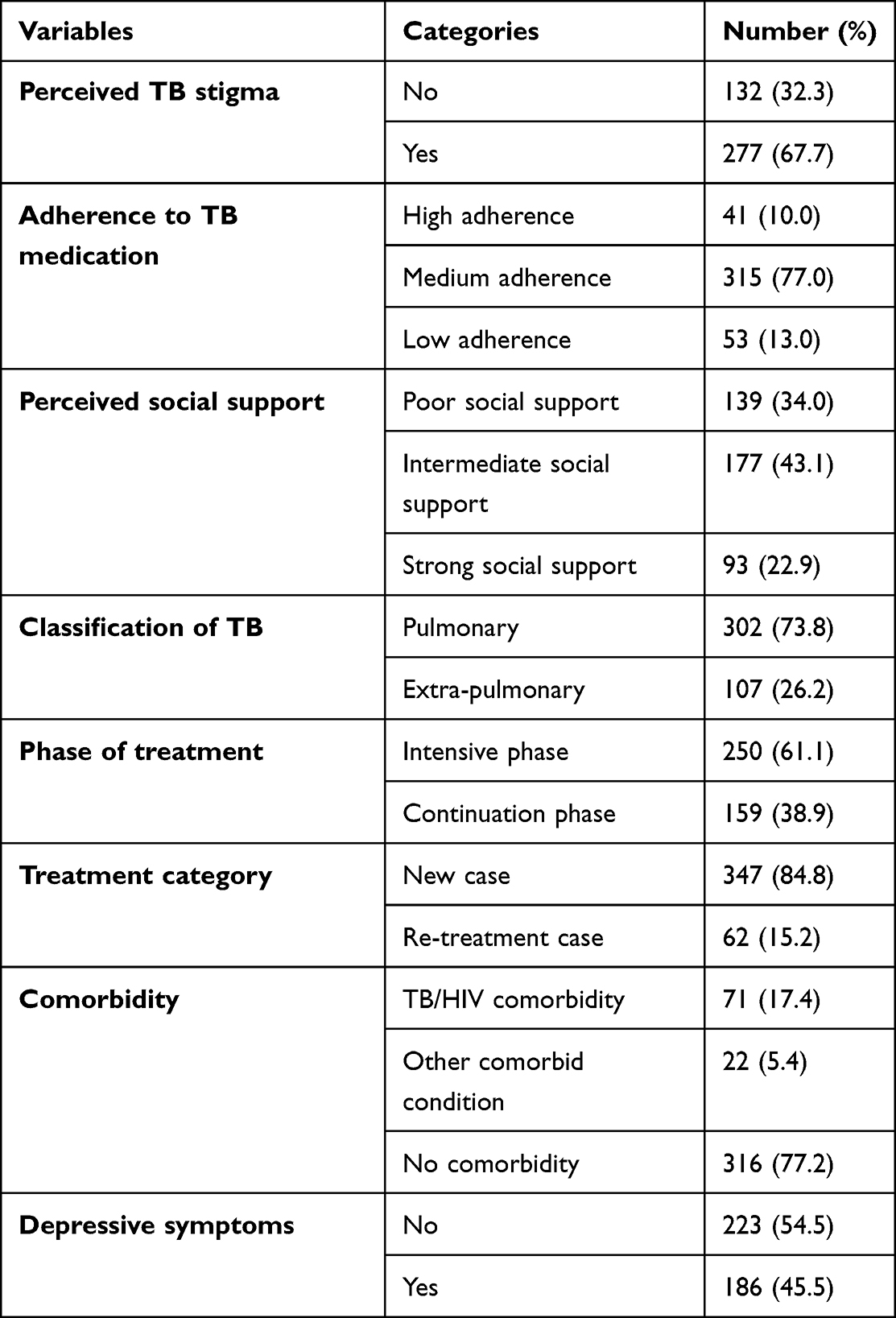 |
Table 2 A Description of Psychosocial and Clinical Characteristics of Patients with Tuberculosis, Gedeo Zone, South Ethiopia, 2018, (n = 409) |
Prevalence of Harmful Alcohol Use
Ten items from the Alcohol Disorder Identification Test (AUDIT) were summed up to produce a single variable (1) (AUDIT 8 and above).
Eighty-two (20%) of the tuberculosis patients were harmful alcohol consumers.
Factors Associated with Harmful Alcohol Use
We conducted statistical analysis to determine whether socio-demographic, clinical, and psychosocial factors were associated with harmful alcohol use. Age, gender, marital status, depression, medical comorbidity, duration of illness, social support, and TB category had p-values less than 0.2 in bi-variate logistic regression and were considered in multiple logistic regression analysis. Using the Hosmer and Lemeshow test, the model goodness of fit was determined to be 0.64, which indicates that the model is sound.
There was a 2.10 times (95% CI: 1.17, 3.77) more significant risk of harmful alcohol use among males than in TB patients with comorbid medical conditions. Patients with medical comorbidity were about 2.44 times more likely to engage in harmful alcohol use (AOR = 2.44, 95% CI: 1.29–4.62) than those without comorbid medical condition.
There was an association between harmful alcohol use and the duration of illness among TB patients. A more prolonged illness duration (>12 months) is associated with a 2.88 times higher risk of harmful alcohol use compared to shorter illness duration (<6 months) (Table 3).
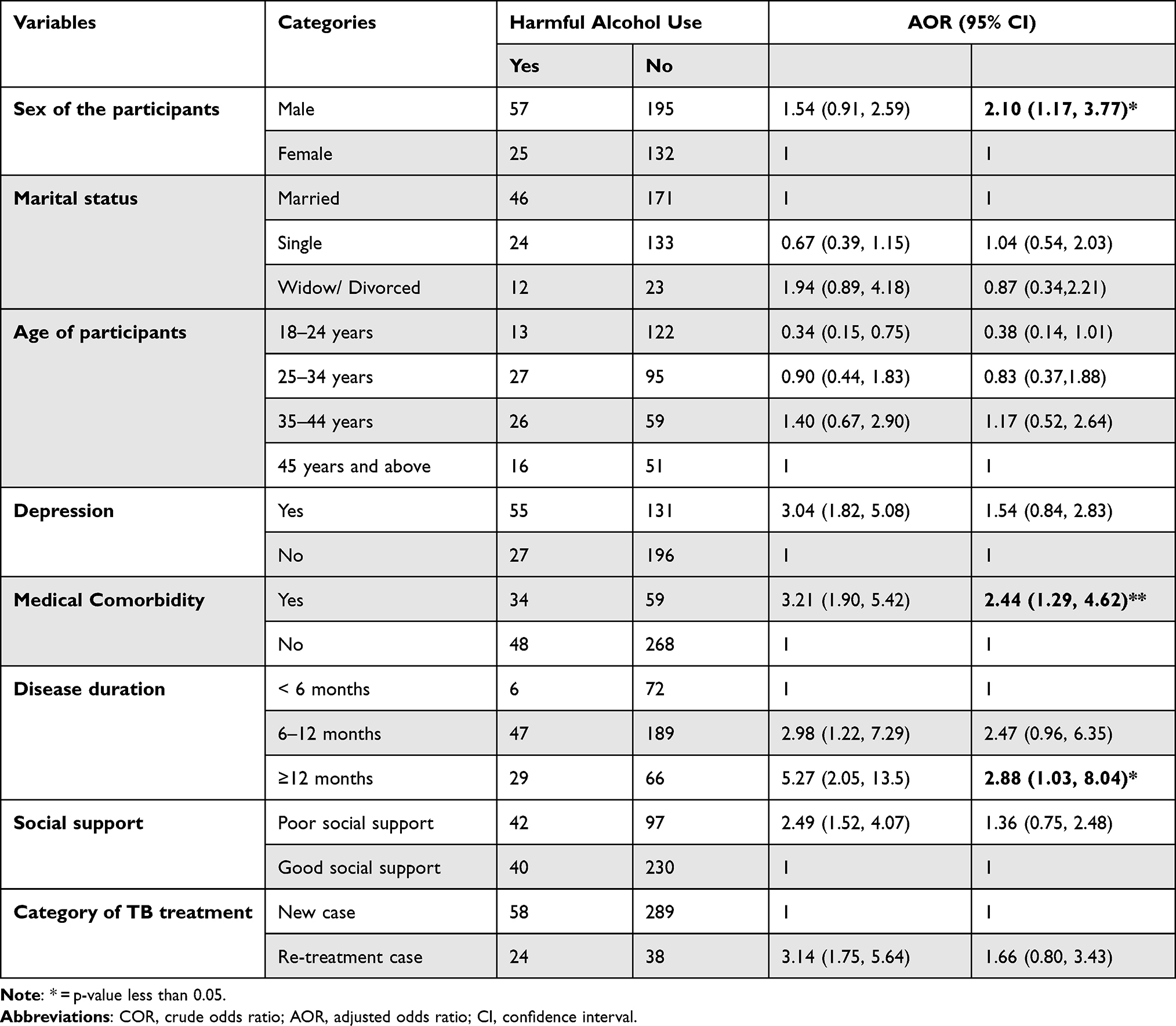 |
Table 3 Bivariate and Multivariate Analysis of Factors Associated with Harmful Alcohol Use Among Patients with Tuberculosis at Tuberculosis Units of Health Facilities, Gedeo Zone, Southern Ethiopia, 2018 (n = 409) |
Discussion
The prevalence of harmful alcohol use among patients with tuberculosis was 20% (95% CI = 16.1–24.2). This is lower than the findings in Botswana, Lesotho, India, and Thailand (24.7%, 35.1%, 29%, 32%, and 24.4%).2,13,14,28,29 Variations in study settings, study designs, study years, sociodemographic data, and screening methods may account for this.
The findings of this study are similar to those of studies conducted in South Africa, Scotland, and the United States (23.3%, 23.2%, 18%, and 17.9%, respectively).4,30–32 AUDIT was used in all studies conducted in Botswana, South India, and Lesotho. Their characteristics may be similar to those of this study. Different populations, study years, and sociodemographic factors may cause differences.
This study, however, suggests a significantly higher rate of inflated estimates than a study conducted in the United States (15.1%).33 This study used a different tool for measuring hazardous drinking and a different cut-off point for categorizing the patients’ alcohol use behavior. Furthermore, the design, duration, and setting of the current study may have also contributed to the variation in results.
Additionally, the current study identified several factors associated with harmful alcohol consumption among patients with TB. A significant association was found between the sex of the participant and harmful alcohol use. Men had a higher risk of harmful alcohol use than women did. The study’s results are consistent with cross-sectional studies conducted in Namibia, Lesotho, India, and Scotland.4,11,14,28 According to a systematic review of alcohol use and tuberculosis, alcohol use is associated with poorer treatment outcomes.34 There was also a significant association between harmful alcohol consumption and disease duration. Compared to those with a shorter duration of disease, those with a longer duration had a 2.88-fold higher probability of using harmful alcohol.16 Alcohol adversely affects the clinical course of tuberculosis.15,17 Alcohol consumption increases the chances of relapsing, deteriorating clinical outcomes, and developing multi-drug resistant tuberculosis (MDR-TB).
Furthermore, medical comorbidity, HIV/AIDS, and other chronic diseases increased the odds ratio of harmful alcohol use. Those with comorbid physical conditions have a 2.44-fold higher risk of harmful alcohol use than those without these conditions.35 Possibly, this is because individuals with medical comorbidities are more likely to experience stress and other psychological problems. Thus, the current finding in line with the 2018 WHO Global Status Report on Alcohol and Health.7
Unlike other studies, this study did not find any association between the harmful use of alcohol and several factors, including age, marital status, anxiety symptoms, social support, and TB treatment category.
The Strengths and Limitations of the Study
A strength of the study was the use of validated and standardized tools to assess harmful alcohol use and independent variables. However, it is not possible to establish causality based on a cross-sectional study, and, for example, patients with co-morbid medical conditions may be more likely to drink heavily.
Conclusion and Recommendation
Twenty percent of tuberculosis patients used harmful alcohol. Medical comorbidities, being male, and having a long-term illness were significant predictors of harmful alcohol use. In addition, those who delay seeking treatment or who have a prolonged illness duration should be screened for harmful alcohol use. Furthermore, patients with comorbid medical conditions should be screened for alcohol use. By screening early for alcohol abuse, we may avoid poor treatment outcomes as well as the effects of comorbid medical conditions and alcohol abuse. A prospective study will also be required to determine whether there is a relationship between factors that predict harmful alcohol consumption among tuberculosis patients.
Abbreviations
AUDIT, Alcohol Use Disorders Identification Test; DALYs, Disability Adjusted Life Years; PHQ-9, nine-item Patient Health Questionnaire; TB, Tuberculosis.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The researchers would like to thank all of the staff of the public health institutions in the Gedeo region who provided information. We sincerely thank Dilla University, the College of Medicine and Health Sciences, Research and Dissemination Office for funding this study. All authors of the article wish to acknowledge Dilla University’s Research Directorate office for its support. In addition, we are grateful to the data collectors, study participants, and the Gedeo Zone Health Department.
Author Contributions
Kalkidan Yohannes and Hirbaye Mokona conceived the study and were part of the whole study process. Getinet Ayano, Kussie Koirita, and Henok Mulatu participated in the study’s design, reviewed all versions, and made corrections. Kalkidan Yohannes has access to raw data, and she is responsible for it. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research work was funded by Dilla University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Status Report on Alcohol and Health 2018. World Health Organization; 2018.
2. Zetola NM, Modongo C, Kip E, Gross R, Bisson G, Collman R. Alcohol use and abuse among patients with multidrug-resistant tuberculosis in Botswana. Int J Tuberculosis Lung Dis. 2012;16(11):1529–1534. doi:10.5588/ijtld.12.0026
3. Sadock BJ, Sadock VA. Kaplan & Sadock’s Concise Textbook of Clinical Psychiatry. Lippincott Williams & Wilkins; 2008.
4. De la Haye B, Wild S, Stevenson J, Johnston F, Blatchford O, Laurenson I. Tuberculosis and alcohol misuse in Scotland: a population-based study using enhanced surveillance data. Int J Tuberculosis Lung Dis. 2012;16(7):886–890. doi:10.5588/ijtld.11.0624
5. Chatterjee D, Shams S, Gerlai R. Chronic and acute alcohol administration induced neurochemical changes in the brain: comparison of distinct zebrafish populations. Amino Acids. 2014;46(4):921–930. doi:10.1007/s00726-013-1658-y
6. Kaplan BJ. Kaplan and sadock’s synopsis of psychiatry. Behav Sci Clin Psychiatry. 2016;58(1):78–79.
7. World Health Organization. Global Status Report on Alcohol and Health 2018. World Health Organization; 2019.
8. Roerecke M, Gual A, Rehm J. Reduction of alcohol consumption and subsequent mortality in alcohol use disorders: systematic review and meta-analyses. J Clin Psychiatry. 2013;74(12):17165. doi:10.4088/JCP.13r08379
9. Eashwar VA, Umadevi R, Gopalakrishnan S. Alcohol consumption in India–An epidemiological review. J Fam Med Primary Care. 2020;9(1):49. doi:10.4103/jfmpc.jfmpc_873_19
10. Fauci AS. Harrison’s Principles of Internal Medicine. McGraw-Hill Education; 2015.
11. O’Connell R, Chishinga N, Kinyanda E, et al. Prevalence and correlates of alcohol dependence disorder among TB and HIV infected patients in Zambia. PLoS One. 2013;8(9):e74406. doi:10.1371/journal.pone.0074406
12. World Health Organization. Global Tuberculosis Report 2019. World Health Organization; 2019.
13. Suhadev M, Thomas BE, Charles N, Mathew TA, Wares F. Alcohol use disorders (AUD) among tuberculosis patients: a study from Chennai, South India. PLoS One. 2011;6(5):e19485.
14. Thapa P, Kamath R, Shetty B, Monteiro A, Sekaran V. Prevalence and associated factors of alcoholism among tuberculosis patients in Udupi Taluk, Karnataka, India: a cross sectional study. J Nepal Health Res Counc. 2014;12(28):177–181.
15. Jakubowiak W, Bogorodskaya E, Borisov E, Danilova D, Kourbatova E. Risk factors associated with default among new pulmonary TB patients and social support in six Russian regions. Int J Tuberculosis Lung Dis. 2007;11(1):46–53.
16. Rehm J, Samokhvalov AV, Neuman MG, et al. The association between alcohol use, alcohol use disorders and tuberculosis (TB). A Systematic Review BMC Public Health. 2009;9(1):1–12.
17. Moran A, Harbour DV, Teeter LD, Musser JM, Graviss EA. Is alcohol use associated with cavitary disease in tuberculosis? Alcohol Clin Exp Res. 2007;31(1):33–38. doi:10.1111/j.1530-0277.2006.00262.x
18. Mathew T, Ovsyanikova T, Shin S, et al. Causes of death during tuberculosis treatment in Tomsk Oblast, Russia. Int J Tuberculosis Lung Dis. 2006;10(8):857–863.
19. Lönnroth K, Williams BG, Stadlin S, Jaramillo E, Dye C. Alcohol use as a risk factor for tuberculosis–a systematic review. BMC Public Health. 2008;8(1):1–12. doi:10.1186/1471-2458-8-289
20. Haddad MB, Wilson TW, Ijaz K, Marks SM, Moore M. Tuberculosis and homelessness in the United States, 1994–2003. JAMA. 2005;293(22):2762–2766. doi:10.1001/jama.293.22.2762
21. Kendall EA, Theron D, Franke MF, et al. Alcohol, hospital discharge, and socioeconomic risk factors for default from multidrug resistant tuberculosis treatment in rural South Africa: a retrospective cohort study. PLoS One. 2013;8(12):e83480. doi:10.1371/journal.pone.0083480
22. Duko B, Gebeyehu A, Ayano G. Prevalence and correlates of depression and anxiety among patients with tuberculosis at WolaitaSodo University Hospital and Sodo Health Center, WolaitaSodo, South Ethiopia, Cross sectional study. BMC Psychiatry. 2015;15(1):1–7. doi:10.1186/s12888-015-0598-3
23. Gelaye B, Williams MA, Lemma S, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–661. doi:10.1016/j.psychres.2013.07.015
24. Abiola T, Udofia O, Zakari M. Psychometric properties of the 3-item Oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malays J Psychiatry. 2013;22(2):32–41.
25. Bøen H, Dalgard OS, Bjertness E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 2012;12(1):1–12. doi:10.1186/1471-2318-12-27
26. Abebe G, Deribew A, Apers L, et al. Knowledge, health seeking behavior and perceived stigma towards tuberculosis among tuberculosis suspects in a rural community in southwest Ethiopia. PLoS One. 2010;5(10):e13339. doi:10.1371/journal.pone.0013339
27. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test. Geneva: World Health Organization; 2001.
28. Hayes-Larson E, Hirsch-Moverman Y, Saito S, et al. Depressive symptoms and hazardous/harmful alcohol use are prevalent and correlate with stigma among TB-HIV patients in Lesotho. Int J Tuberculosis Lung Dis. 2017;21(11):S34–S41. doi:10.5588/ijtld.17.0062
29. Laprawat S, Peltzer K, Pansila W, Tansakul C. Alcohol use disorder and tuberculosis treatment: a longitudinal mixed method study in Thailand. South Afr J Psychiatry. 2017;23(1):1–5. doi:10.4102/sajpsychiatry.v23i0.1074
30. Peltzer K, Naidoo P, Matseke G, Louw J, Mchunu G, Tutshana B. Prevalence of psychological distress and associated factors in tuberculosis patients in public primary care clinics in South Africa. BMC Psychiatry. 2012;12(1):1–9. doi:10.1186/1471-244X-12-89
31. Peltzer K, Louw J, Mchunu G, Naidoo P, Matseke G, Tutshana B. Hazardous and harmful alcohol use and associated factors in tuberculosis public primary care patients in South Africa. Int J Environ Res Public Health. 2012;9(9):3245–3257. doi:10.3390/ijerph9093245
32. Fiske CT, Hamilton CD, Stout JE. Alcohol use and clinical manifestations of tuberculosis. J Infect. 2009;58(5):395–401. doi:10.1016/j.jinf.2009.02.015
33. Oeltmann JE, Kammerer JS, Pevzner ES, Moonan PK. Tuberculosis and substance abuse in the United States, 1997–2006. Arch Intern Med. 2009;169(2):189–197. doi:10.1001/archinternmed.2008.535
34. Johnston JC, Shahidi NC, Sadatsafavi M, Fitzgerald JM, Pai M. Treatment outcomes of multidrug-resistant tuberculosis: a systematic review and meta-analysis. PLoS One. 2009;4(9):e6914. doi:10.1371/journal.pone.0006914
35. Macintyre K, Bloss E. Alcohol brewing and the African tuberculosis epidemic. Med Anthropol. 2011;30(2):126–135. doi:10.1080/01459740.2011.552457
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.