Back to Journals » Journal of Blood Medicine » Volume 16
Haploidentical Hematopoietic Stem Cell Transplantation for Relapsed/Refractory Extramedullary Multiple Myeloma: A Conditioning Regimen Combining Selinexor and Helical Tomotherapy—A Case Report and Literature Review
Authors Chen B, Guo R, Niu Y, Guo W, Wang T ![]()
Received 16 September 2024
Accepted for publication 18 March 2025
Published 2 April 2025 Volume 2025:16 Pages 177—185
DOI https://doi.org/10.2147/JBM.S495256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Bin Chen, Rongrong Guo, Yanyan Niu, Wei Guo, Tao Wang
Department of Hematology, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China
Correspondence: Tao Wang, Email [email protected]
Abstract: Relapsed/refractory multiple myeloma (RRMM) and extramedullary multiple myeloma (EMM) present significant challenges for patients with multiple myeloma (MM) after their disease progresses.Despite notable advancements in treatments like autologous hematopoietic stem cell transplantation (ASCT) and chimeric antigen receptor (CAR)-T-cell therapy, most patients with RRMM and EMM face a short survival period. Currently, there are no effective treatments available. Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is one of the treatment options for MM. Reduced-intensity conditioning (RIC) regimens have largely replaced myeloablative conditioning (MAC) regimens. RIC is now preferred because it significantly lowers transplant-related mortality, which has dropped to 10– 20%. However, RIC regimens are linked to higher relapse rates compared to MAC. To enhance the efficacy of allo-HSCT, it is essential to identify a safer and more effective conditioning regimen. We report a case of EMM involving the breast, supraclavicular region, mediastinum, and pleural effusion, among other sites. The patient did not respond to several treatments, including a proteasome inhibitor (PI) like bortezomib, immunomodulatory drugs (IMiDs) such as lenalidomide, and a monoclonal antibody targeting CD38, like daratumumab. Consequently, we recommended haploidentical hematopoietic stem cell transplantation as a salvage treatment. After undergoing allo-HSCT with a conditioning regimen that mainly included selinexor and helical tomotherapy, the patient achieved a complete remission(CR) and enjoyed long-term disease-free survival for 11 months. Along with existing literature, this case provides encouraging insights for future research on RRMM and EMM, and we anticipate more reports on allo-HSCT cases in the future.
Keywords: allogeneic hematopoietic stem cell transplantation, relapsed/refractory multiple myeloma: extramedullary multiple myeloma, selinexor, tomotherapy
Introduction
Multiple myeloma (MM) is a malignant proliferation of plasma cells in the bone marrow.1 Relapsed/refractory multiple myeloma (RRMM) and extramedullary multiple myeloma (EMM) are aggressive subtypes.2,3 Although treatments like immunomodulatory drugs, proteasome inhibitors, and monoclonal antibodies (eg, daratumumab) have improved survival rates, most of patients eventually relapse or become refractory. EMM patients typically have an overall survival (OS) of less than 3 years.4 The lack of well-established standard treatments for RRMM and EMM creates significant challenges. Despite the use of daratumumab in later lines of therapy, the total effective rate for EMM is only 16.7%,5 with median progression-free survival (PFS) and overall survival (OS) of 2.3 and 6.6 months, respectively,6 highlighting the need for innovative treatment strategies.
Anti-BCMA CAR T-cell therapy is promising for RRMM. However, it has lower PFS and OS rates in extramedullary disease and higher occurrences of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxic syndrome (ICANS).7,8 Although it offers early remission, achieving a potential cure may require additional treatments such as stem cell transplantation and radiotherapy.
Optimizing the conditioning regimen is crucial for the success of allo-HSCT.9 RIC regimens decrease transplant-related mortality but have increased recurrence rates compared to MAC.10 Effective conditioning regimens are essential for increasing cure rates.
Exportin 1 (XPO1) is overexpressed in myeloma, which is associated with poor outcomes. Selinexor,11 an XPO1 inhibitor approved by the Food and Drug Administration (FDA) in 2019, promotes the accumulation of tumor suppressor proteins, leading to apoptosis in cancer cells. It’s used with dexamethasone for heavily pretreated MM.12
Helical tomotherapy (HT) provides accurate radiation treatment to bones and bone marrow, specifically for total marrow irradiation (TMI).13
This report discusses a patient diagnosed with RRMM and EMM affecting several locations. The patient underwent a conditioning regimen that included selinexor and HT, followed by haploidentical hematopoietic stem cell transplantation, which effectively controlled disease progression.
Case Report
A 56-year-old female patient visited the doctor in July 2021 because her lower back pain had been worsening progressively for three months. CT scans showed reduced bone density in the ribs, thoracic spine, lumbar spine, pelvis, and femoral head. The vertebral MRI revealed abnormal signals in the thoracic, lumbar, and sacral regions, as well as in the facet joints, along with a pathological fracture of the L1 vertebra. Laboratory results included hemoglobin at 90 g/L, IgA at 0.259 g/L, IgG at 2.88 g/L, IgM at 0.166 g/L, IgE at 17.1 IU/mL, serum albumin at 37 g/L, lactate dehydrogenase at 164 U/L, β2 microglobulin at 4.63 mg/L, blood creatinine at 58.2 μmol/L, and blood calcium at 2.11 mmol/L. Serum protein electrophoresis did not detect M protein. However, serum immunofixation electrophoresis revealed a monoclonal κ band. The serum kappa light chain was 0.74 g/L, lambda light chain was 0.36 g/L, and rFLC (κFLC:λFLC) was 2.0556. Urinary free kappa light chain was 21.30 mg/L, urinary free lambda light chain was 5.35 g/L, and urinary rFLC (κFLC:λFLC) was 3.9813. Bone marrow cytology and biopsy indicated an 80% infiltration of kappa-restricted clonal plasma cells expressing various markers: CD38 positive, CD138 positive (poly), sporadic CD56 positive, K positive (poly), lambda negative (poly), slightly positive CD20, small clusters of E-CAD positive, and less scattered MPO positive. Additionally, flow cytometry revealed that approximately 17.62% of the plasma cells were monoclonal. The karyotype analysis (according to ISCN) revealed the following results: 42, XX, del(1)(p34), del(6)(q21), add(9)(q34), 10, del(11)(q23), 12, 13, del(14), t(11;14)(q13;q32), add(20)(p13), and 2213/46, XX.4 She was diagnosed with kappa multiple myeloma, classified as DS stage IIIA, ISS stage II, R-ISS stage II, and assessed as intermediate risk according to mSMART2.0. The patient is of Asian ethnicity, highly educated, and has no occupational exposure risks, smoking, or alcohol consumption. She resides in quality housing and has no family history of similar diseases. The patient has had a history of allergic asthma for 20 years.
After completing four cycles of the bortezomib and dexamethasone treatment, her response was classified as a very good partial response (VGPR). In November 2021, a presternal mass developed, which was treated with PVD chemotherapy (pomalidomide, bortezomib, and dexamethasone) and 46 Gy of local radiation, leading to its complete disappearance. A February 2022 PET-CT scan revealed multiple regions of bone destruction in the ribs, scapula, spine, sacrum, pelvis, and upper femurs, along with soft tissue masses. Increased FDG metabolism was observed in the lateral and right acetabulum, right femoral head, left supraclavicular region, bilateral subclavian areas, mediastinal 2L region, and in several enlarged lymph nodes near the 10th thoracic vertebra. She continued her treatment with PVD chemotherapy (pomalidomide, bortezomib, and dexamethasone).
In April 2022, the patient reported increased lower back pain along with a supraclavicular mass and swelling in her left arm. Chest CT revealed multiple swollen lymph nodes in the left supraclavicular region and mediastinum, and significant pleural effusion on the left side. A biopsy of the left supraclavicular lymph node revealed plasma cells, with immunohistochemistry results showing CD38(+), CD138(+), Kappa(+), Lambda(-), and Ki-67 at 90%. The patient’s condition was evaluated for disease progression and extramedullary infiltration of multiple myeloma. She underwent the DRD regimen (daratumumab, lenalidomide, and dexamethasone) followed by DRD+PACE chemotherapy (cisplatin, doxorubicin, cyclophosphamide, and etoposide), which led to a reduction in lymph nodes and pleural effusion. Another course of DRD followed. In September 2022, a left breast mass was biopsied, confirming myeloma. Immunohistochemistry results indicated the following: CD138(+), CD38(+), LCA(+) in low amounts, CD20(-), CD3 (partially positive), CD5(-), Pax-5(-), P120(-), E-cad(-), GATA-3(-), CK(-), and Ki-67 at 70%. She received another course of DRD+PACE chemotherapy.
In October 2022, an evaluation following multiline treatment revealed recurrent extramedullary lesions, a decrease in white blood cells and hemoglobin, and an increase in bone marrow monoclonal plasma cells (3.66%). The treatment included proteasome inhibitors (Bortezomib), immunomodulators (Lenalidomide, Pomalidomide), and the CD38 monoclonal antibody (Daratumumab). Immunofixation identified IgG κ type M protein, and fluorescence in situ hybridization (FISH) detected a 6% abnormal amplification of the 1q21 signal, which surpasses the 3% threshold. She was diagnosed with progressive disease (PD) and classified as high-risk according to mSMART 3.0. The patient chose to undergo allo-HSCT, with her son serving as a 6/12 hLA-matched donor who is DSA-negative.
The conditioning regimen (Figure 1) consisted of several treatments: selinexor (60 mg on days −10 and −7), TMI (8 Gy on days −8 to −5), Vp16 (20 mg/kg on days −5 to −2), CTX (90 mg/kg on days −5 to −2), and ATG (10 mg/kg on days −5 to −2). CSA combined with MMF and short-term MTX were used to prevent acute graft-versus-host disease (aGvHD); ganciclovir was administered for viral prophylaxis, and defibrotide was employed to prevent veno-occlusive disease (VOD). The patient received allo-HSCT using both bone marrow and peripheral blood stem cells, yielding a mononuclear cell count of 9.66×10^8/kg and a CD34+ cell count of 3.02×10^6/kg.
 |
Figure 1 The flow chart of RIC Selinexor (60 mg on days −10 and −7), TMI (total dose of 8 Gy on days −8 to −5), Vp16 (total dose of 20 mg/kg on days −5 to −2), CTX (total dose of 90 mg/kg on days −5 to −2), and ATG (total dose of 10 mg/kg on days −5 to −2). RIC,Reduced intensity conditioning TMI,Total marrow irradiation HSC,Haematopoietic stem cell. |
The patient tolerated the conditioning regimen well and experienced no significant adverse reactions. Neutropenic fever was managed effectively with routine anti-infection treatment. Granulocyte engraftment occurred 28 days after the transplant, followed by platelet engraftment on Day 52, resulting in complete donor chimerism. Four months after the transplant, the patient developed chronic graft-versus-host disease (cGvHD), presenting with scattered rashes and mild oral ulcers. This condition was managed with topical hydrocortisone. Ten months after the transplant, she is undergoing maintenance therapy with selinexor and lenalidomide, taking selinexor 40 mg twice a week and lenalidomide 25 mg from Day 1 to Day 14 every three months. A dynamic evaluation shows that the patient’s multiple myeloma is in complete remission (CR), with no new extramedullary lesions and normal results from blood cell analysis (Figure 2–4).
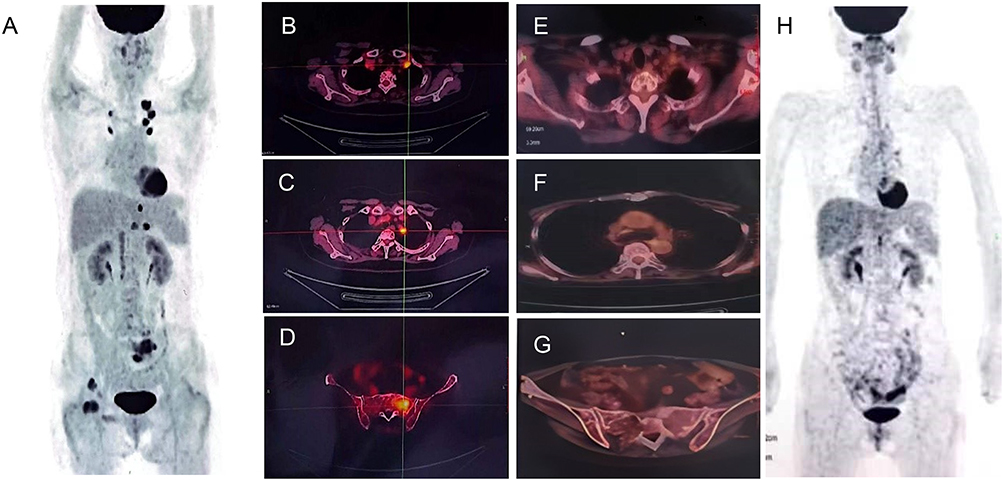 |
Figure 2 FDG PET/CT shows Multiple myeloma extramedullary lesions. (A)2022-2-10 PET image, (B) Swollen lymph nodes under clavicle, SUVmax 7.8, (C) Paraspinal soft tissue nodules in T10 pyramid, Size about 1.3cm×0.7cm,SUVmax 8.6, (D) left side of sacrum, SUVmax 9.1, (E) 2023-5-8 After-HSCT,no subclavian hypermetabolic lymph nodes, (F) 2023-5-8 After-HSCT,no hypermetabolic lesions were found in the mediastinum or hilus, (F) 2023-5-8 no hypermetabolic lesions were found in the sacrum and pelvis, (H)2023-5-8 PET image. |
 |
Figure 3 Treatment history and efficacy evaluation. Abbreviations: VD, Bortezomib and Dexamethasone; PVD, Pomalidomide, Bortezomib and Dexamethasone; DRD, Daratumumab,Lenalidomide and Dexamethasone; PACE, Cisplatin, Doxorubicin, Cyclophosphamide and Etoposide; CR, complete response; VGPR, very good partial response; PD, progressive disease. |
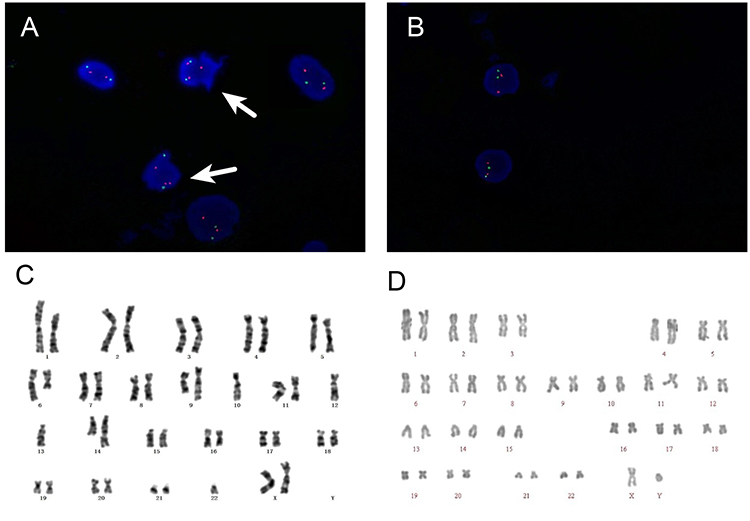 |
Figure 4 Fluorescence in situ hybridization and chromosome. (A)Before allogeneic hematopoietic stem cell transplantation:CKS1B (1q21-22) amplification abnormality is 6% (interval 3%). The white arrow indicates an abnormal signal. A normal signal consists of two green dots and two red dots, whereas the marked area shows an additional red dot. (B) After allogeneic hematopoietic stem cell transplantation: Normal signal, (C) Before allogeneic hematopoietic stem cell transplantation: complex karyotype, (D)After allogeneic hematopoietic stem cell transplantation: normal karyotype. |
Discussion
This 56-year-old patient shows signs of both RRMM and EMM, which poses a significant treatment challenge. Although proteasome inhibitors, immunomodulators, and monoclonal antibodies are commonly used to treat multiple myeloma, most patients eventually relapse and develop refractory disease (Figure 3). The incidence of tertiary refractory multiple myeloma, which does not respond to these treatments, is on the rise, particularly among patients who have received all five major therapies: carfilzomib, bortezomib, lenalidomide, pomalidomide, and daratumumab.1,2
EMM occurs when myeloma cells invade organs outside the bone marrow. It can be diagnosed through imaging, biopsy, or physical examination.1,2,4 Patients with EMM often exhibit high-risk gene expression and cytogenetics, along with elevated LDH levels, and reduced hemoglobin and platelet counts.4 Although there have been advances in proteasome inhibitors, IMiDs, monoclonal antibodies, and CAR-T-cell therapies, the treatment standards for RRMM and EMM primarily rely on retrospective studies (Table 1).11,14–19
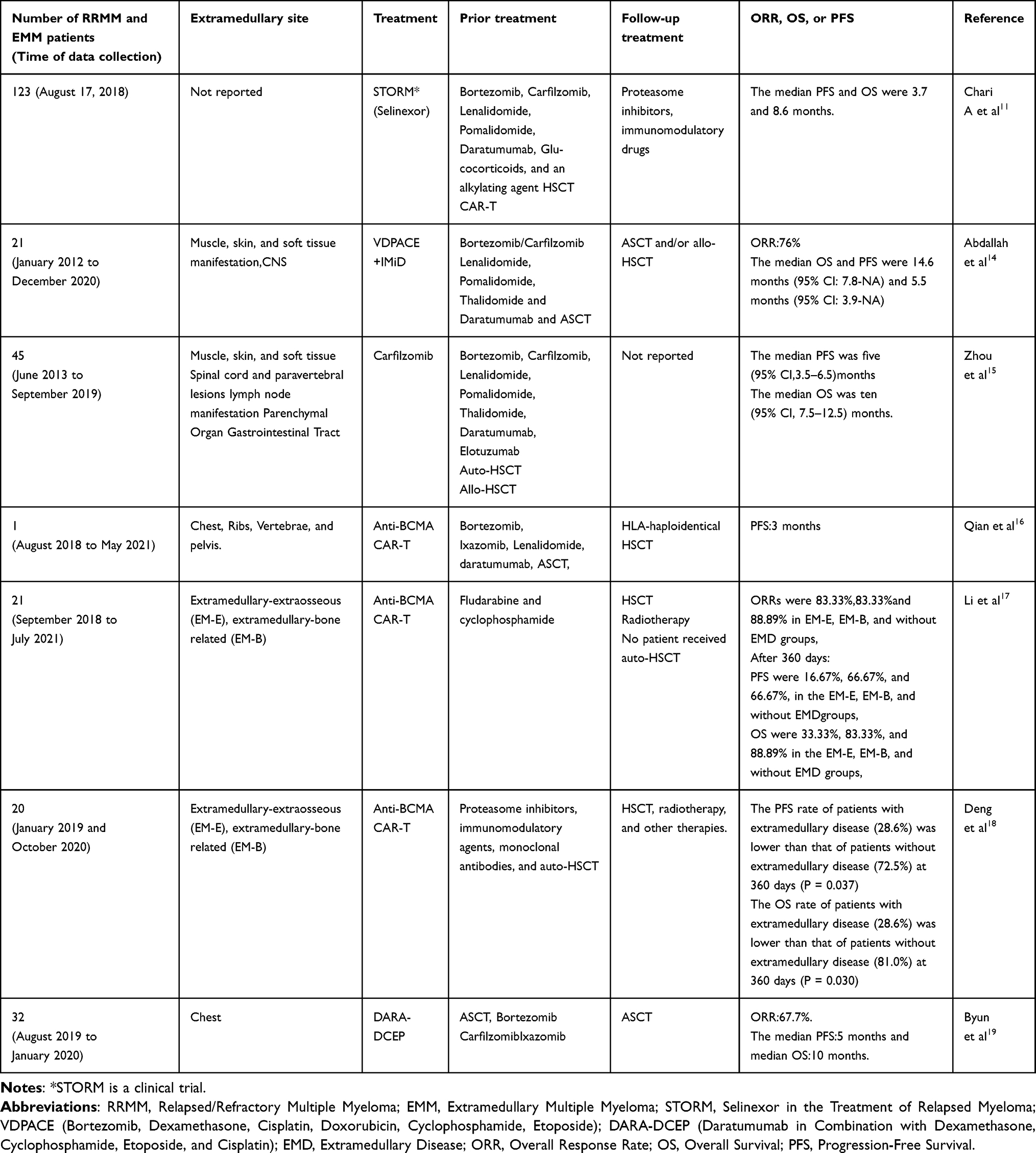 |
Table 1 Outcomes of Patients with RRMM and EMM After Treatment with Novel Agents, CAR-T Cell Therapy and Stem Cell Transplant |
Allogeneic stem cell transplantation is still a valuable option for treating of RRMM and EMM those with high-risk characteristics, thanks to its graft-versus-myeloma effect.20 There are three common conditioning regimens: treosulfan (Treo), non-Treo myeloablative conditioning (MAC), and non-Treo reduced-intensity conditioning (RIC). In a study, the five-year non-relapse mortality (NRM) rates were 10% for Treo, 17% for non-Treo RIC, and 19% for non-Treo MAC.21 However, it is still unclear which conditioning regimen is more effective for RRMM and EMM.
In 2019, selinexor, an XPO1 inhibitor, was approved for patients with RRMM who had not responded to at least two proteasome inhibitors (PIs), immunomodulatory drugs (IMiDs), and an anti-CD38 monoclonal antibody.12 Research involving 817 patients with RRMM demonstrated that selinexor combinations achieved higher objective response rates (65.9% vs 23.4%) and longer progression-free survival (12.5 months vs 2.9 months) compared to fifth-line treatments.22 Nevertheless, there are few studies that have investigated the use of selinexor in conditioning regimens for allo-HSCT in either RRMM or EMM.
Total body irradiation (TBI) plays a critical role in hematopoietic cell transplantation (HCT). It effectively eradicates malignant cells and prevents the rejection of donor cells. TBI’s effectiveness is not influenced by blood supply or patient variability, allowing it to target sanctuary sites such as the testicular tissues and the central nervous system(CNS). Numerous trials indicate that TBI significantly outperforms non-TBI treatment options.23
Helical tomotherapy (HT) combines CT image-guided radiotherapy and intensity-modulated radiation therapy into one device. It has a maximum target size of about 60 cm in width and 160 cm in length. HT is well-suited for delivering conformal targeted TBI to large, complex target shapes while minimizing the dose to critical normal organs.13,24,25
Historically, HT was primarily utilized for autologous stem cell transplantation in the treatment of RRMM.13,24,25 Some researchers administered HT in combination with melphalan at a dose of 140 mg/m², followed by autologous stem cell transplantation as a consolidation treatment during the first relapse of MM. Among these 13 patients, 38.5% achieved a very good partial response, while 30.8% attained a complete response. Out of the 13 patients, three remained progression-free at the time of assessment. Six patients were long-term survivors, remaining alive after 55 months of follow-up. This study confirms that the use of TMI yields favorable outcomes and demonstrates an excellent tolerance profile during the first relapse of MM.24
Other relevant studies have confirmed that TMI, employing 8 Gy as a conditioning regimen, is a viable alternative to TBI for autologous stem cell transplantation in RRMM.13,25 However, there are few reports on the use of HT as a conditioning regimen in haploidentical HSCT for the treatment of RRMM and EMM.
There are two primary prophylaxis methods for aGvHD. These methods are post-transplant cyclophosphamide (PTCy) and anti-thymocyte globulin (ATG). ATG plays a vital role in the “Beijing Protocol”, which is essential for preventing GvHD effectively. It reduces the incidence of aGvHD and significantly lowers the occurrence of cGvHD after HLA-matched transplantation. The “Beijing Protocol” is widely applied and has been included in the 5th edition of Thomas’ Hematopoietic Cell Transplantation. Furthermore, domestic data show that the “Beijing Protocol” promotes faster hematopoietic recovery and improves non-relapse mortality (NRM), disease-free survival (DFS), and overall survival (OS) rates compared to the PTCy method. For this patient, we have more experience in using CsA + MTX + MMF based on ATG for the prevention of aGvHD, and the success rate is also encouraging.
In this case, the patient showed high compliance during treatment. After several treatment lines, the disease progressed, leading to RRMM and EMM in the breast, supraclavicular area, mediastinum, and pleural cavity. She received a conditioning regimen that combining selinexor and HT, followed by haploidentical HSCT. The patient tolerated the regimen well without any adverse reactions and achieved CR after ten months.
To our knowledge, our patient is the first case of selinexor combined with helical tomotherapy as a conditioning regimen for RRMM and EMM using haploidentical HSCT. Given the positive outcome, this approach appears to effectively control disease progression in RRMM and EMM, thus warranting further investigation.
Abbreviations
RRMM, Relapsed/refractory multiple myeloma; EMME, extramedullary multiple myeloma; MM, Multiple myeloma; ASCT, Autologous hematopoietic stem cell transplantation; CAR, Chimeric antigen receptor; allo-HSCT, Allogeneic hematopoietic stem cell transplantation; RIC, Reduced-intensity conditioning; MAC, Myeloablative conditioning; PI, Proteasome inhibitor; IMiDs, Immunomodulatory drugs; CR, Complete remission; OS, Overall survival; PFS, Progression-free survival; CRS, Cytokine release syndrome; ICANS, Immune effector cell-associated neurotoxic syndrome; XPO1, Exportin 1; FDA, Food and drug administration; HT, Helical tomotherapy; TMI, Total marrow irradiation; VGPR, Very good partial response; FISH, Fluorescence in situ hybridization; PD, Progressive disease; Vp16, Etoposide; CTX, Cyclophosphamide; ATG, Anti-thymocyte globulin; CSA, Cyclosporine A; MMF, Mycophenolate mofetil; MTX, Methotrexate; aGvHD, Acute graft-versus-host disease; VOD, Veno-occlusive disease; cGvHD, Chronic graft-versus-host disease; Treo, Treosulfan; TBI, Total body irradiation; HCT, Hematopoietic cell transplantation; CNS, Central nervous system; PTCy, Post-transplant cyclophosphamide; NRM, Non-relapse mortality; DFS, Disease-free survival.
Compliance with Ethical Standards
This study was funded by Key Research and Development Projects of Shanxi Province (201803d31144) and the Natural Science Foundation General Project of Shanxi Province (202203021211070). Written informed consent to publish case details and any accompanying images was provided by the patient. Third Hospital of Shanxi Medical University:Shanxi Bethune Hospital Ethics Committee approved this consent process and institutional approval was required to publish the case details.
Written Informed Consent
In this manuscript, we present a case report on the use of Selinexor in combination with helical tomotherapy as a conditioning regimen for the treatment of relapsed/refractory extramedullary multiple myeloma via haploidentical haematopoietic stem cell transplantation, along with a review of the contemporary literature. Prior to submission to the Journal of Blood Medicine, we have obtained written consent from the patient/study participant for the publication of their identifiable details, including photographs, videos, case history, and/or details within the text (“Material”). The patient/study participant has confirmed that they have read and had the opportunity to review the Material and the Article.
Patient Consent
Obtained.
Acknowledgment
The authors would like to thank the patient and their family for their cooperation and willingness to share their experience.
Disclosure
Conflict of interest not exists in the submission of this manuscript, and the manuscript is approved by all authors for publication.
References
1. Donk van de NWCJ, Pawlyn C, Yong KL. Multiple myeloma. Lancet. 2021;397(10272):410–427. doi:10.1016/S0140-6736(21)00135-5
2. Bhutani M, Foureau DM, Atrash S, et al. Extramedullary multiple myeloma. Leukemia. 2020;34(1):1–20. doi:10.1038/s41375-019-0660-0
3. Hindié E. Teclistamab in relapsed or refractory multiple myeloma. N Engl J Med. 2022;387(18):1721–1723. doi:10.1056/NEJMc2211969
4. Bladé J, Beksac M, Caers J, et al. Extramedullary disease in multiple myeloma: a systematic literature review. Blood Cancer J. 2022;12(3):45. doi:10.1038/s41408-022-00643-3
5. Usmani SZ, Weiss BM, Plesner T, et al. Clinical efficacy of daratumumab monotherapy in patients with heavily pretreated relapsed or refractory multiple myeloma. Blood. 2016;128(1):37–44. doi:10.1182/blood-2016-03-705210
6. Pick M, Vainstein V, Goldschmidt N, et al. Daratumumab resistance is frequent in advanced-stage multiple myeloma patients irrespective of CD 38 expression and is related to dismal prognosis. Eur J Haematol. 2018;100(5):494–501. doi:10.1111/ejh.13046
7. Wu JF, Dhakal B. BCMA-targeted CAR-T cell therapies in relapsed and/or refractory multiple myeloma: latest updates from 2023 ASCO annual meeting. J Hematol Oncol. 2023;16(1):86. doi:10.1186/s13045-023-01479-5
8. Neelapu SS, Tummala S, Kebriaei P, et al. Chimeric antigen receptor T-cell therapy - assessment and management of toxicities. Nat Rev Clin Oncol. 2018;15(1):47–62. doi:10.1038/nrclinonc.2017.148
9. Sobh M, Michallet M, Dubois V, et al. Salvage use of allogeneic hematopoietic stem cell transplantation after reduced-intensity conditioning from unrelated donors in multiple myeloma. A study by the plasma cell disorders subcommittee of the European group for blood and marrow transplant chronic malignancies working party. Haematologica. 2017;102(7):e271–e274. doi:10.3324/haematol.2017.165399
10. Hayden PJ, Iacobelli S, Pérez-Simón JA, et al. Conditioning-based outcomes after allogeneic transplantation for myeloma following a prior autologous transplant (1991–2012) on behalf of EBMT CMWP. Eur J Haematol. 2020;104(3):181–189. doi:10.1111/ejh.13352
11. Chari A, Vogl DT, Gavriatopoulou M, et al. Oral selinexor-dexamethasone for triple-class refractory multiple myeloma. N Engl J Med. 2019;381(8):727–738. doi:10.1056/NEJMoa1903455
12. Richter J, Madduri D, Richard S, et al. Selinexor in relapsed/refractory multiple myeloma. Therape Adv Hematol. 2020;11:2040620720930629. doi:10.1177/2040620720930629
13. Shueng PW, Lin SC, Chong NS, et al. Total marrow irradiation with helical tomotherapy for bone marrow transplantation of multiple myeloma: first experience in Asia. Technol Cancer Res Treat. 2009;8(1):29–38. doi:10.1177/153303460900800105
14. Abdallah AO, Mohyuddin GR, Ahmed N, et al. Outcomes of VDPACE with an immunomodulatory agent as a salvage therapy in relapsed/refractory multiple myeloma with extramedullary disease. EJHaem. 2021;2(4):757–764. doi:10.1002/jha2.275
15. Zhou X, Flüchter P, Nickel K, et al. Carfilzomib based treatment strategies in the management of relapsed/refractory multiple myeloma with extramedullary disease. Cancers. 2020;12(4):1035. doi:10.3390/cancers12041035
16. Qian Y, Qian Z, Zhao X, et al. Successful treatment of relapsed/refractory extramedullary multiple myeloma with anti-BCMA CAR-T cell therapy followed by haploidentical hematopoietic stem cell transplantation: a case report and a review of the contemporary literature. Front Med. 2021;8:649824. doi:10.3389/fmed.2021.649824
17. Li W, Liu M, Yuan T, et al. Efficacy and follow-up of humanized anti-BCMA CAR-T cell therapy in relapsed/refractory multiple myeloma patients with extramedullary-extraosseous, extramedullary-bone related, and without extramedullary disease. Hematological Oncol. 2022;40(2):223–232. doi:10.1002/hon.2958
18. Deng H, Liu M, Yuan T, et al. Efficacy of humanized anti-BCMA CAR T cell therapy in relapsed/refractory multiple myeloma patients with and without extramedullary disease. Front Immunol. 2021;12:720571. doi:10.3389/fimmu.2021.720571
19. Byun JM, Min CK, Kim K, et al. Phase II trial of daratumumab with DCEP in relapsed/refractory multiple myeloma patients with extramedullary disease. J Hematol Oncol. 2022;15(1):150. doi:10.1186/s13045-022-01374-5
20. Tricot G, Vesole DH, Jagannath S, Hilton J, Munshi N, Barlogie B. Graft-versus-myeloma effect: proof of principle. Blood. 1996;87(3):1196–1198. doi:10.1182/blood.V87.3.1196.bloodjournal8731196
21. Gran C, Wang J, Nahi H, et al. Treosulfan conditioning for allogeneic transplantation in multiple myeloma - improved overall survival in first line hematopoietic stem cell transplantation—a large retrospective study by the chronic malignancies working party of the EBMT. Br J Haematol. 2020;189(5):e213–e217. doi:10.1111/bjh.16642
22. Gu X, Sun C, Xu J, et al. Optimal timing and drug combination of selinexor in multiple myeloma: a systematic review and meta-analysis. Hematology. 2023;28(1):2187972. doi:10.1080/16078454.2023.2187972
23. Rodrigues CA, Sanz G, Brunstein CG, et al. Analysis of risk factors for outcomes after unrelated cord blood transplantation in adults with lymphoid malignancies: a study by the Eurocord-Netcord and lymphoma working party of the European group for blood and marrow transplantation. J Clin Oncol. 2009;27(2):256–263. doi:10.1200/JCO.2007.15.8865
24. Wong JYC, Rosenthal J, Liu A, Schultheiss T, Forman S, Somlo G. Image-guided total-marrow irradiation using helical tomotherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation. Int J Radiat Oncol Biol Phys. 2009;73(1):273–279. doi:10.1016/j.ijrobp.2008.04.071
25. Cailleteau A, Maingon P, Choquet S, et al. Phase 1 study of the combination of escalated total marrow irradiation using helical tomotherapy and fixed high-dose melphalan (140 mg/m2) followed by autologous stem cell transplantation at first relapse in multiple myeloma. Int J Radiat Oncol Biol Phys. 2023;115(3):677–685. doi:10.1016/j.ijrobp.2022.09.069
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.