Back to Journals » Clinical Interventions in Aging » Volume 12
Grip strength as a frailty diagnostic component in geriatric inpatients
Authors Dudzińska-Griszek J, Szuster K, Szewieczek J ![]()
Received 22 April 2017
Accepted for publication 27 May 2017
Published 26 July 2017 Volume 2017:12 Pages 1151—1157
DOI https://doi.org/10.2147/CIA.S140192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Joanna Dudzińska-Griszek, Karolina Szuster, Jan Szewieczek
Department of Geriatrics, School of Health Sciences in Katowice, Medical University of Silesia, Katowice, Poland
Background: Frailty has emerged as a key medical syndrome predictive of comorbidity, disability, institutionalization and death. As a component of the five frailty phenotype diagnostic criteria, patient grip strength deserves attention as a simple and objective measure of the frailty syndrome. The aim of this study was to assess conditions that influence grip strength in geriatric inpatients.
Patients and methods: The study group consisted of 80 patients aged 78.6±7.0 years ( X ± SD), with 68.8% women, admitted to the Department of Geriatrics. A comprehensive geriatric assessment was complemented with assessment for the frailty phenotype as described by Fried et al for all patients in the study group. Functional assessment included Barthel Index of Activities of Daily Living (Barthel Index), Instrumental Activities of Daily Living Scale and Mini-Mental State Examination.
Results: Three or more frailty criteria were positive in 32 patients (40%), while 56 subjects (70%) fulfilled the frailty criterion of weakness (grip strength test). Multivariate linear regression analysis revealed that two independent measures showed positive association with grip strength – Mini-Mental State Examination score (β=0.239; P=0.001) and statin use (β=0.213; P=0.002) – and four independent measures were negatively associated with grip strength – female sex (β=–0.671; P<0.001), C-reactive protein (β=–0.253; P<0.001), prior myocardial infarction (β=–0.190; P=0.006) and use of an antidepressant (β=–0.163; P=0.018). Low physical activity was identified as the only independent qualitative frailty component associated with 2-year mortality in multivariate logistic regression analysis after adjustment for age and sex (odds ratio =6.000; 95% CI =1.357–26.536; P=0.018).
Conclusion: Cognitive function, somatic comorbidity and medical treatment affect grip strength as a measure of physical frailty in geriatric inpatients. Grip strength was not predictive of 2-year mortality in this group.
Keywords: frailty, cognitive function, statin, antidepressant, physical activity, mortality
Introduction
Frailty has emerged as a key medical syndrome that increases the risk of mortality, disability, hospitalization, falls and fractures.1 It is now recognized as an essential factor for clinical decision making.2 However, clinical criteria and operational definitions of frailty are still the subject of intense study and debate.3,4 Physical frailty phenotype is the most frequently used frailty instrument,4 originally proposed by the criteria of Fried et al.5 Despite being described for community-dwelling populations, the Fried frailty criteria proved useful for geriatric inpatient assessment.6 Physical frailty phenotype criteria include unintentional weight loss, weakness (assessment based on the hand grip strength measurement), exhaustion, slow gait and low physical activity.5 Of these five components, grip strength deserves attention as a simple and objective measure of the frailty syndrome.7,8 Reduced muscle strength, as measured by grip strength, has been associated with an increased risk of all-cause and cardiovascular mortality; therefore, grip strength is considered a simple, quick and inexpensive means of stratifying an individual’s risk of cardiovascular death.9 Weak hand grip strength in later life is a risk factor for disability, morbidity and mortality and is central to the definitions of sarcopenia and frailty.10,11 The measurement of hand grip strength may be especially useful in the context of multimorbidity to identify patients at high risk of adverse outcomes, who may benefit from closer clinical attention.12 It proved valuable as a screening tool for frailty in older patients with hematologic malignancies13 and predictive of 12-month mortality in patients after transcatheter aortic valve implantation.14 Factors associated with muscle strength in a cohort of geriatric ward inpatients have not been extensively studied. The aim of the study was to assess the determinants of grip strength in geriatric inpatients.
Patients and methods
Patients
The study group consisted of 80 consecutive patients aged 78.6±7.0 years ( ± SD; in the range of 60–92 years), with 68.8% women, admitted to the Department of Geriatrics at University Hospital, No 7 SUM, Uppersilesian Medical Center in Katowice, Poland between October 2014 and December 2014, who provided informed consent for participation in the study. Exclusion criteria included patients unable to provide informed consent because of cognitive impairment.
± SD; in the range of 60–92 years), with 68.8% women, admitted to the Department of Geriatrics at University Hospital, No 7 SUM, Uppersilesian Medical Center in Katowice, Poland between October 2014 and December 2014, who provided informed consent for participation in the study. Exclusion criteria included patients unable to provide informed consent because of cognitive impairment.
Measurements
Comprehensive geriatric assessment (CGA) complemented with tests for frailty and body mass assessment was performed for all patients. CGA included a structured interview, physical examination, geriatric functional assessment, blood sampling, electrocardiogram, abdominal ultrasound and chest X-ray. Barthel Index of Activities of Daily Living (Barthel Index)15 and Instrumental Activities of Daily Living Scale (IADL)16 were used to determine functional status. Mini-Mental State Examination (MMSE)17 was used to assess global cognitive performance. Geriatric Depression Scale-Short Form (GDS-SF) was used to screen for depression.18 Barthel Index scores range from 0 to 100, IADL from 9 to 27 and MMSE from 0 to 30; higher scores indicate better functional status. GDS-SF scores range from 0 to 15, with higher scores indicating higher depression probability. Modified Get-up and Go Test (scored from 0 to 10, with lower values suggesting increased ambulatory disability) was used to evaluate patient fall risk.19,20 Frailty was diagnosed according to the criteria of Fried et al.5 A Kern digital dynamometer was used for grip strength measurement. Low physical activity (weekly energy expenditure) was calculated on the basis of the modified “Minnesota Leisure Time Activity Questionnaire”.21,22 A Polish language version of the “Frailty Assessment Components: Standardized Protocols” was used. Dementia was diagnosed according to the recommendations of the National Institute on Aging–Alzheimer’s Association.23 Pain intensity was assessed with the Visual Analog Scale (VAS)24,25 scored from 0 to 10. Body mass index was calculated for all subjects. Patient survival 2 years after hospital discharge was assessed by making phone calls to patient caregivers.
Statistical analysis
Data were analyzed using STATISTICA version 12 (Stat Soft Polska; Stat Soft, Inc., Tulsa, OK, USA). Chi-square test, V-square test and Fisher’s exact test were used for categorical variables and the nonparametric Mann–Whitney U test for quantitative variables to compare patients with frailty to those without frailty and to compare grip strength in subgroups of patients with various clinical and functional characteristics. The nonparametric Spearman’s rank correlation coefficient was used to assess relationships between clinical, functional and laboratory measures and grip strength. Multivariate linear regression was used to assess measures associated with grip strength. Analysis with backward elimination included variables that yielded P-values of 0.1 or lower in the initial univariate analysis. To adjust for sex, male grip strength values were multiplied by a factor of (1−SP2), where SP denotes a semipartial correlation coefficient for female sex in the multivariate linear regression analysis (Table 1). The squared semipartial correlation coefficient determines the specific portion of variance explained by a given independent variable in a multivariate linear regression analysis. Multivariate binary logistic regression was performed to assess the association between quantitative and qualitative physical frailty measures and 2-year mortality. The variables were adjusted for age and sex. Multivariate analysis with backward elimination included variables that yielded P-values of ≤0.1 in the initial univariate analysis. P-values <0.05 were considered statistically significant.
 | Table 1 Standardized coefficients for measures associated with grip strength in geriatric inpatients in the multivariate linear regression model (corrected R2=0.686), N=80 |
Ethics
The study protocol was approved by the Bioethical Committee of the Medical University of Silesia in Katowice, Poland (Letter KNW/0022/KB1/1/14).
Results
Thirty-two patients (40%) fulfilled the frailty criteria. Thirty patients (37.5%) were classified as prefrail and 18 (22.5%) as nonfrail. As compared to patients without frailty, patients with frailty used more medications, had lower MMSE, Barthel Index, IADL scores and Modified Get-Up and Go Test results; higher GDS scores; lower values of red blood cells (RBCs) and lymphocytes; and lower concentrations of hemoglobin, albumin, total cholesterol and high-density lipoprotein-cholesterol (Table 2). The frailty weakness criterion (assessed using hand grip strength measurement) was fulfilled in 56 subjects (70%). Grip strength correlated positively with IADL, MMSE, Barthel Index, growth, body mass, hemoglobin concentration, hematocrit, RBC and lymphocyte count, and the concentration of sodium and bilirubin, while it correlated negatively with the number of used medications, GDS, VAS and C-reactive protein (CRP) concentration (Table 3). MMSE and statin use were independent measures positively associated with grip strength, while female sex, CRP, prior myocardial infarction and use of antidepressants were inversely associated with grip strength in the multivariate linear regression model adjusted for demographic and clinical characteristics, and these factors accounted for 68.6% of the grip strength variance in the study group (Tables 1 and 4). Ten patients (12.5%) died within 2 years of hospital discharge. Low physical activity was the only independent qualitative frailty component (odds ratio =6.000; 95% CI =1.357–26.536; P=0.018) and physical activity level was the only quantitative frailty measure (odds ratio =0.998; 95% CI =0.997–1.000; P=0.016) associated with 2-year mortality in multivariate logistic regression analysis after adjustment for age and sex.
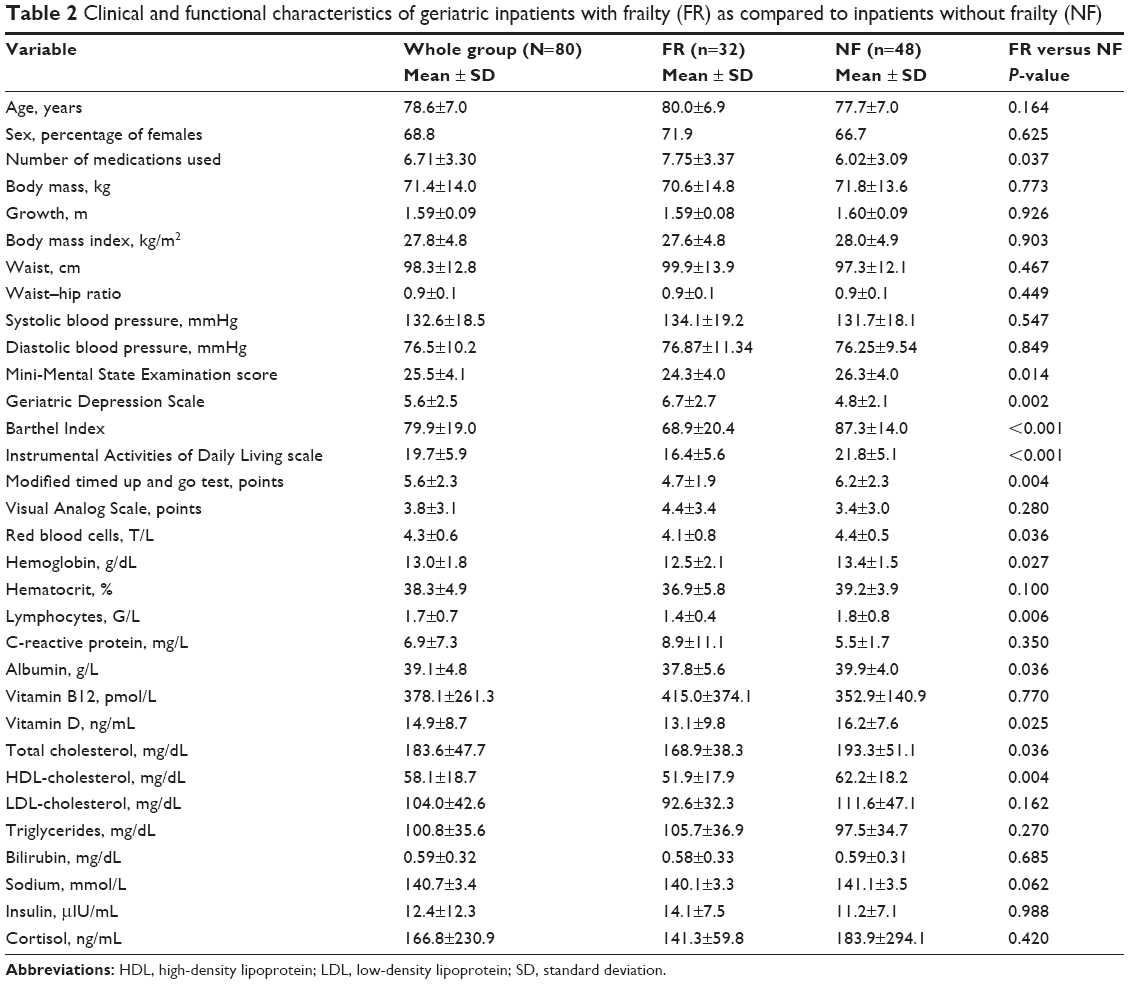 | Table 2 Clinical and functional characteristics of geriatric inpatients with frailty (FR) as compared to inpatients without frailty (NF) |
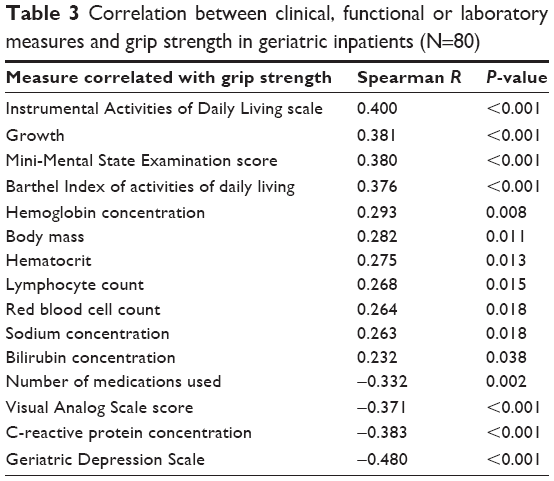 | Table 3 Correlation between clinical, functional or laboratory measures and grip strength in geriatric inpatients (N=80) |
 | Table 4 Comparison of GS between groups of geriatric inpatients with different demographic, clinical and functional characteristics with and without adjustment for sex |
Discussion
Our observations confirm the multidimensional scope of frailty – a syndrome that includes both physical and cognitive conditions.26 Frailty diagnosed on the basis of physical phenotype criteria was associated with worse MMSE and GDS scores (Table 2). More advanced functional deterioration in this group is confirmed by the work of other authors indicating that frailty is a major risk factor for disability.1 In addition to lower hemoglobin, albumin and vitamin D levels, as compared to subjects without frailty, patients with frailty had lower total cholesterol and high-density lipoprotein-cholesterol. While attention toward the treatment of hypercholesterolemia is emphasized in many guidelines, low total cholesterol may be a marker of health deterioration. Grip strength, a component of the five physical frailty criteria,5 is also considered a biomarker of aging and a predictor of disability, morbidity and mortality.27 Grip strength was a better predictor of all-cause and cardiovascular mortality than systolic blood pressure in more than 140,000 participants aged 35–70 years from the PURE Study.9 In primary care outpatients aged 60 years or more, without IADL impairment, grip strength was associated with age, female sex, height, depression and mobility problems.28 Others have shown that physical inactivity, body fat, diabetes, depression, sleeping disturbances, number of medications and falls were identified as factors associated with grip strength in community-dwelling elderly patients,29 although a Spanish study suggests that the grip strength poorly discriminates prefrail from frail individuals.30 It reveals a linear age-dependent decline in very old men (aged ≥85) and a curvilinear decline in very old women; in both sexes, better values were observed in subjects with higher baseline physical activity, height, fat-free mass, better self-rated health and not having arthritis of the hand(s).31 In our group of geriatric inpatients, grip strength correlated with anthropometric, clinical and functional measures (Table 3). However, it is difficult to determine the cause-and-effect dependence between muscle strength and other functional measures. In the Spearman’s rank correlation analysis, grip strength correlated positively with IADL, MMSE and Barthel Index and negatively with GDS and VAS. Grip strength appears to influence both physical and mental functioning, between which there exists a bidirectional relationship. As expected, grip strength rose with higher body growth and mass. Similar to Joosten et al,32 we did not observe a significant association between anemia and low grip strength. However, correlations with hemoglobin concentration and RBC count suggest possible treatment for improving the muscle strength and, therefore, susceptibility to frailty. Sex had the strongest influence on grip strength in a multivariate linear regression analysis. Grip strength was higher in men than in women (23.1±9.8 versus 14.7±7.4 kg; P<0.001) in a sample of 209 geriatric inpatients examined by Joosten et al.32 We observed that the CRP concentration was an independent negative determinant of grip strength in our sample of patients, which confirms the deleterious impact of inflammation on muscle function. A meta-analysis by Soysal et al revealed that frailty and prefrailty were associated with higher inflammatory parameters, although higher serum CRP and interleukin-6 (IL-6) levels were not associated with frailty in three longitudinal studies.33 However, IL-6 and CRP levels were inversely associated with physical and cognitive performance as well as survival in a large cohort of community-dwelling older individuals.34 Prior myocardial infarction was another independent factor associated negatively with grip strength in our patients. This factor was found to be a determinant of lower physical function in 51 community-dwelling patients aged 65+ years with established chronic coronary heart disease.35 Many other clinical conditions, including diabetes36 and anorexia,37 may drive sarcopenia and decrease in muscle strength, increasing the risk of frailty. Treatment with the use of antidepressants also revealed a negative association with muscle strength (Tables 1 and 4). Depression and the presence of comorbidities that interact with depressive symptomatology increase the risk of incident frailty.38 Depression combined with inappropriate nutrition predisposes to muscle strength decrease.39 Lakey et al demonstrated an association between antidepressant treatment (regardless of depression status) and increased incidence of frailty in older women.40 It is unclear whether all antidepressant classes carry a similar relationship with frailty. Therefore, further research is needed to explain the possible role of antidepressants in the depression–frailty relationship. In contrast to other studies,41–44 in our observation, statin use was positively associated with muscle strength (Tables 1 and 4). This finding needs confirmation in further studies. We assume, that a beneficial impact of statins on the cardiovascular system, and therefore, their positive effect on organ perfusion may outweigh their direct deleterious effect on skeletal muscles in some patients. However, Rengo et al found that chronic statin therapy in healthy asymptomatic individuals does not promote deleterious myofilament structural or functional adaptations.45 Our observation of the association between grip strength and MMSE scores (Tables 1 and 3), as well as the GDS (Table 3), support the concept of a psychologic dimension of physical frailty in geriatric inpatients. The prognostic value of an assessment that accounts for both physical and mental components of frailty is superior to the separate values of these components.46 Grip strength was not predictive of survival prognosis in our group; low physical activity was the only frailty component associated with 2-year mortality. In another study performed in geriatric inpatients in Poland, that did not include frailty assessment, 5.5-year mortality was associated with age, cognitive function, IADL score, Charlson comorbidity index, body mass index, cholesterol and hemoglobin levels.47 Despite the limitations of our study, especially a relatively low number of participants and short follow-up period, this analysis confirmed that grip strength is influenced by multiple factors of patient health status. Frailty emerged as one of the top predictors of adverse health outcomes, disability and mortality in older patients with multiple chronic conditions,48,49 including patients with COPD,50 diabetes,51 cancer,52 liver cirrhosis,53 end-stage renal disease,54 heart failure55 and patients who underwent transcatheter aortic valve implantation.14 Although not included in all frailty models, grip strength constitutes a valuable diagnostic component of this clinical syndrome.
Conclusion
Cognitive function, somatic comorbidity and medical treatment affect grip strength as a measure of physical frailty in geriatric inpatients. Grip strength was not predictive of 2-year mortality in this group.
Acknowledgments
The authors express their acknowledgments to Dr Krzysztof Wilczyński for the language review of the paper. This project was funded by the Medical University of Silesia grants to statutory work (contracts KNW-1–011/N/5/0 and KNW-1–014/K/6/Z) and young scientist research agreement (KNW-2–013/N/4/N).
Disclosure
The authors report no conflicts of interest in this work.
References
Vermeiren S, Vella-Azzopardi R, Beckwée D, et al; Gerontopole Brussels Study group. Frailty and the prediction of negative health outcomes: a meta-analysis. J Am Med Dir Assoc. 2016;17(12):1163.e1–1163.e17. | ||
Farcet A, de Decker L, Pauly V, et al. Frailty markers and treatment decisions in patients seen in oncogeriatric clinics: results from the ASRO pilot study. PLoS One. 2016;11:e0149732. | ||
Ruan Q, D’Onofrio G, Sancarlo D, et al. Emerging biomarkers and screening for cognitive frailty. Aging Clin Exp Res. Epub 2017 Mar 4. | ||
Buta BJ, Walston JD, Godino JG, et al. Frailty assessment instruments: systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res Rev. 2016;26:53–61. | ||
Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol Med Sci. 2001;56(3):M146–M156. | ||
Bieniek J, Wilczyński K, Szewieczek J. Fried frailty phenotype assessment components as applied to geriatric inpatients. Clin Interv Aging. 2016;11:453–459. | ||
Mijnarends DM, Schols JM, Meijers JM, et al. Instruments to assess sarcopenia and physical frailty in older people living in a community (care) setting: similarities and discrepancies. J Am Med Dir Assoc. 2015;16(4):301–308. | ||
Chainani V, Shaharyar S, Dave K, et al. Objective measures of the frailty syndrome (hand grip strength and gait speed) and cardiovascular mortality: a systematic review. Int J Cardiol. 2016;215:487–493. | ||
Leong DP, Teo KK, Rangarajan S, et al; Prospective Urban Rural Epidemiology (PURE) Study investigators. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015;386(9990):266–273. | ||
Syddall HE, Westbury LD, Dodds R, Dennison E, Cooper C, Sayer AA. Mortality in the Hertfordshire Ageing Study: association with level and loss of hand grip strength in later life. Age and Ageing. Epub 2016 Dec 7. | ||
Dodds RM, Syddall HE, Cooper R, Kuh D, Cooper C, Sayer AA. Global variation in grip strength: a systematic review and meta-analysis of normative data. Age Ageing. 2016;45(2):209–216. | ||
Leong DP, Teo KK. Predicting cardiovascular disease from handgrip strength: the potential clinical implications. Expert Rev Cardiovasc Ther. 2015;13(12):1277–1279. | ||
Velghe A, De Buyser S, Noens L, Demuynck R, Petrovic M. Hand grip strength as a screening tool for frailty in older patients with haematological malignancies. Acta Clin Belg. 2016;71(4):227–230. | ||
Kleczynski P, Dziewierz A, Bagienski M, et al. Impact of frailty on mortality after transcatheter aortic valve implantation. Am Heart J. 2017;185:52–58. | ||
Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65. | ||
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. | ||
Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. | ||
Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1–2):165–173. | ||
Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil. 1986;67(6):387–389. | ||
Mazur K, Wilczyński K, Szewieczek J. Geriatric falls in the context of a hospital fall prevention program: delirium, low body mass index, and other risk factors. Clin Interv Aging. 2016;11:1253–1261. | ||
Taylor HL, Jacobs DR Jr, Schucker B, Knudsen J, Leon AS, Debacker G. A questionnaire for the assessment of leisure time physical activities. J Chronic Dis. 1978;31(12):741–755. | ||
Siscovick DS, Fried L, Mittelmark M, Rutan G, Bild D, O’Leary DH. Exercise intensity and subclinical cardiovascular disease in the elderly. The Cardiovascular Health Study. Am J Epidemiol. 1997;145(11):977–986. | ||
McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263–269. | ||
Joyce CR, Zutshi DW, Hrubes V, Mason RM. Comparison of fixed interval and visual analogue scales for rating chronic pain. Eur J Clin Pharmacol. 1975;8(6):415–420. | ||
Hjermstad MJ, Fayers PM, Haugen DF, et al; European Palliative Care Research Collaborative (EPCRC). Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. | ||
Halil M, Cemal Kizilarslanoglu M, Emin Kuyumcu M, Yesil Y, Cruz Jentoft AJ. Cognitive aspects of frailty: mechanisms behind the link between frailty and cognitive impairment. J Nutr Health Aging. 2015;19(3):276–283. | ||
Sayer AA, Kirkwood TB. Grip strength and mortality: a biomarker of ageing? Lancet. 2015;386(9990):226–227. | ||
Lino VT, Rodrigues NC, O’Dwyer G, Andrade MK, Mattos IE, Portela MC. Handgrip strength and factors associated in poor elderly assisted at a primary care unit in Rio de Janeiro, Brazil. PLoS One. 2016;11:e0166373. | ||
Vasconcelos KS, Dias JM, Bastone Ade C, et al. Handgrip strength cutoff points to identify mobility limitation in community-dwelling older people and associated factors. J Nutr Health Aging. 2016;20(3):306–315. | ||
Lorenzo-López L, López-López R, Maseda A, Diego-Díez C, Gómez-Caamaño S, Millán-Calenti JC. Prevalence and clinical characteristics of prefrailty in elderly adults: differences according to degree of urbanization. J Am Geriatr Soc. 2016;64(1):221–223. | ||
Granic A, Davies K, Jagger C, Kirkwood TB, Syddall HE, Sayer AA. Grip strength decline and its determinants in the very old: longitudinal findings from the Newcastle 85+ Study. PLoS One. 2016;11(9):e0163183. | ||
Joosten E, Detroyer E, Milisen K. Effect of anaemia on hand grip strength, walking speed, functionality and 1 year mortality in older hospitalized patients. BMC Geriatr. 2016;16(1):153. | ||
Soysal P, Stubbs B, Lucato P, et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res Rev. 2016;31:1–8. | ||
Puzianowska-Kuźnicka M, Owczarz M, Wieczorowska-Tobis K, et al. Interleukin-6 and C-reactive protein, successful aging, and mortality: the PolSenior study. Immun Ageing. 2016;13:21. | ||
Ades PA, Savage PD, Tischler MD, Poehlman ET, Dee J, Niggel J. Determinants of disability in older coronary patients. Am Heart J. 2002;143(1):151–156. | ||
Park SW, Goodpaster BH, Strotmeyer ES, et al. Decreased muscle strength and quality in older adults with type 2 diabetes: the health, aging, and body composition study. Diabetes. 2006;55(6):1813–1818. | ||
Landi F, Liperoti R, Russo A, et al. Association of anorexia with sarcopenia in a community-dwelling elderly population: results from the ilSIRENTE study. Eur J Nutr. 2013;52(3):1261–1268. | ||
Vaughan L, Corbin AL, Goveas JS. Depression and frailty in later life: a systematic review. Clin Interv Aging. 2015;10:1947–1958. | ||
Guligowska A, Pigłowska M, Fife E, et al. Inappropriate nutrients intake is associated with lower functional status and inferior quality of life in older adults with depression. Clin Interv Aging. 2016;11:1505–1517. | ||
Lakey SL, LaCroix AZ, Gray SL, et al. Antidepressant use, depressive symptoms, and incident frailty in women aged 65 and older from the Women’s Health Initiative Observational Study. J Am Geriatr Soc. 2012;60(5):854–861. | ||
Bruckert E, Hayem G, Dejager S, Yau C, Bégaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients – the PRIMO study. Cardiovasc Drugs Ther. 2005;19(6):403–414. | ||
Stroes E, Thompson PD, Corsini A, et al. Statin-associated muscle symptoms: impact on statin therapy – European Atherosclerosis Society Consensus Panel Statement on Assessment, Etiology and Management. Eur Heart J. 2015;36(17):1012–1022. | ||
Loenneke JP, Loprinzi PD. Statin use may reduce lower extremity peak force via reduced engagement in muscle-strengthening activities. Clin Physiol Funct Imaging. Epub 2016 Jun 10. | ||
Campins L, Camps M, Riera A, Pleguezuelos E, Yebenes JC, Serra-Prat M. Oral drugs related with muscle wasting and sarcopenia. A review. Pharmacology. 2017;99(1–2):1–8. | ||
Rengo JL, Callahan DM, Savage PD, Ades PA, Toth MJ. Skeletal muscle ultrastructure and function in statin-tolerant individuals. Muscle Nerve. 2016;53(2):242–251. | ||
Matusik P, Tomaszewski K, Chmielowska K, et al. Severe frailty and cognitive impairment are related to higher mortality in 12-month follow-up of nursing home residents. Arch Gerontol Geriatr. 2012;55(1):22–24. | ||
Bień B, Bień-Barkowska K, Wojskowicz A, Kasiukiewicz A, Wojszel ZB. Prognostic factors of long-term survival in geriatric inpatients. Should we change the recommendations for the oldest people? J Nutr Health Aging. 2015;19(4):481–488. | ||
Ritt M, Schwarz C, Kronawitter V, et al. Analysis of Rockwood et Al’s Clinical Frailty Scale and Fried et Al’s Frailty Phenotype as Predictors of Mortality and Other Clinical Outcomes in Older Patients Who Were Admitted to a Geriatric Ward. J Nutr Health Aging. 2015;19(10):1043–1048. | ||
Romero-Ortuno R, Wallis S, Biram R, Keevil V. Clinical frailty adds to acute illness severity in predicting mortality in hospitalized older adults: an observational study. Eur J Intern Med. 2016;35:24–34. | ||
Galizia G, Cacciatore F, Testa G, et al. Role of clinical frailty on long-term mortality of elderly subjects with and without chronic obstructive pulmonary disease. Aging Clin Exp Res. 2011;23(2):118–125. | ||
Cacciatore F, Testa G, Galizia G, et al. Clinical frailty and long-term mortality in elderly subjects with diabetes. Acta Diabetol. 2013;50(2):251–260. | ||
Handforth C, Clegg A, Young C, et al. The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol. 2015;26(6):1091–1101. | ||
Tandon P, Tangri N, Thomas L, et al. A rapid bedside screen to predict unplanned hospitalization and death in outpatients with cirrhosis: a prospective evaluation of the clinical frailty scale. Am J Gastroenterol. 2016;111(12):1759–1767. | ||
Kallenberg MH, Kleinveld HA, Dekker FW, et al. Functional and cognitive impairment, frailty, and adverse health outcomes in older patients reaching ESRD-A systematic review. Clin J Am Soc Nephrol. 2016;11(9):1624–1639. | ||
Rodríguez-Pascual C, Paredes-Galán E, Ferrero-Martínez AI, et al. The frailty syndrome is associated with adverse health outcomes in very old patients with stable heart failure: a prospective study in six Spanish hospitals. Int J Cardiol. 2017;236:296–303. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.