Back to Journals » International Journal of Women's Health » Volume 17
GnRH-a Pretreatment Doses and Frozen-Thawed Blastocyst Transfer Outcomes in PCOS Patients: A Retrospective Cohort Study
Authors Li X ![]() , Zhou Y, Qiu Y
, Zhou Y, Qiu Y ![]() , Wu J
, Wu J ![]() , Song Q
, Song Q ![]() , Li R
, Li R ![]() , Liang X
, Liang X ![]()
Received 27 August 2025
Accepted for publication 4 November 2025
Published 15 November 2025 Volume 2025:17 Pages 4519—4527
DOI https://doi.org/10.2147/IJWH.S563596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Xi Li, Yanqun Zhou, Ying Qiu, Jingjing Wu, Qiulan Song, Rong Li, Xinhong Liang
The Nanning Second People’s Hospital/The Third Affiliated Hospital of Guangxi Medical University (Guangxi Clinical Research Center for Reproductive Medicine), Nanning, Guangxi Zhuang Autonomous Region, 530031, People’s Republic of China
Correspondence: Xinhong Liang, The Nanning Second People’s Hospital/The Third Affiliated Hospital of Guangxi Medical University (Guangxi Clinical Research Center for Reproductive Medicine), Nanning, Guangxi Zhuang Autonomous Region, 530031, People’s Republic of China, Tel +86 13481012810, Email [email protected] Rong Li, The Nanning Second People’s Hospital/The Third Affiliated Hospital of Guangxi Medical University (Guangxi Clinical Research Center for Reproductive Medicine), Nanning, Guangxi Zhuang Autonomous Region, 530031, People’s Republic of China, Tel +86 13517887398, Email [email protected]
Objective: To evaluate the effects of GnRH-a pretreatment with 1.5 mg or 3.75 mg, in combination with hormone replacement therapy (HRT), on pregnancy outcomes in women with polycystic ovary syndrome (PCOS) undergoing frozen embryo transfer (FET).
Methods: We conducted a retrospective analysis of 555 FET cycles in PCOS patients treated at our center between July 2022 and June 2024. Based on endometrial preparation regimens, participants were allocated into three groups: HRT alone, GnRH-a (1.5 mg) + HRT, and GnRH-a (3.75 mg) + HRT. Baseline characteristics and pregnancy outcomes were compared among the groups. Multivariable logistic regression was used to adjust for potential confounders.
Results: Baseline characteristics were comparable among groups in age, duration of infertility, body mass index (BMI), endometrial thickness on the start day, estradiol (E2) and luteinizing hormone (LH) on the start day, endometrial thickness on the day of embryo transfer (ET), E2 on the ET day, and days of estradiol valerate administration (all P > 0.05). The proportion of double-embryo transfer cycles was higher in the 1.5 mg GnRH-a + HRT group than in the other two groups (P < 0.001). Pregnancy outcomes, including implantation rate (54.17% vs 46.81% vs 56.73%), clinical pregnancy rate (57.68% vs 57.43% vs 63.70%), early pregnancy loss rate (11.41% vs 13.24% vs 9.30%), and ectopic pregnancy rate (1.09% vs 0.00% vs 1.16%), did not differ significantly among groups (P > 0.05). Multivariable analysis identified the number of embryos transferred as the only factor significantly associated with pregnancy outcome (P < 0.001).
Conclusion: GnRH-a pretreatment at either 1.5 mg or 3.75 mg did not confer a clear benefit over HRT alone in PCOS patients undergoing FET. The number of embryos transferred remains the primary determinant of pregnancy outcome. Larger prospective studies are warranted to validate these findings.
Keywords: polycystic ovary syndrome, frozen-thawed blastocyst transfer, GnRH agonist, artificial cycle
Introduction
PCOS is a common endocrine-metabolic disorder affecting women of reproductive age, characterized by anovulation or oligo-ovulation, hyperandrogenism, and insulin resistance with accompanying metabolic abnormalities. These endocrine-metabolic features contribute to ovulatory dysfunction and impaired endometrial receptivity.1 Globally, PCOS affects approximately 11–13% of women of reproductive age, making it a leading cause of anovulatory infertility.2 The associated endocrine and metabolic dysregulation not only reduces pregnancy rates but also increases the risk of miscarriage.3 Reflecting these challenges, international evidence-based guidelines for PCOS recommended embryo cryopreservation when ART is planned, aiming to reduce the risk of ovarian hyperstimulation syndrome (OHSS) while preserving cumulative live birth rates.4 Recent evidence suggests that FET can avoid hyperestrogenic states and promote better embryo-endometrial synchrony, potentially improving pregnancy outcomes in PCOS patients.5 Therefore, optimizing endometrial preparation protocols during FET remains a critical step in enhancing reproductive outcomes for this population. The optimal strategy for endometrial preparation in PCOS, however, continues to be debated. Several studies support gonadotropin-releasing hormone agonist (GnRH-a) downregulation followed by HRT over HRT alone, reporting improved clinical outcomes.6–9 In contrast, other analyses have found no significant differences in clinical outcomes between pretreatment with 3.75 mg GnRH-a followed by artificial cycles and HRT alone,10–12 highlighting the persistent uncertainty regarding optimal GnRH-a dosing regimens. Given these conflicting findings and the clinical interest in minimizing drug exposure and side effects, the potential value of lower-dose GnRH-a pretreatment has attracted considerable attention. Nevertheless, evidence regarding the impact of low-dose (1.5 mg) GnRH-a pretreatment on FET outcomes in PCOS patients remains lacking. Therefore, this study aims to compare three endometrial preparation regimens—HRT alone, 1.5 mg GnRH-a + HRT, and 3.75 mg GnRH-a + HRT—in PCOS patients undergoing FET to address this evidence gap and provide evidence-based guidance for individualized treatment strategies.
Materials and Methods
General Information
This medical study is a retrospective observational study. According to the Declaration of Helsinki (World Medical Association Inc, 2009), this research requires ethical review and approval. The study received ethical approval from the Ethics Committee of the Nanning Second People’s Hospital, which agreed to waive the requirement for informed consent from the participants.
The need for written informed consent was waived by the Ethics Committee due to the retrospective, observational nature of this study. The analysis utilized exclusively anonymized clinical and laboratory data that were originally collected for routine diagnosis and treatment purposes. The use of this de-identified data for research posed no more than minimal risk to the patients, and it was impracticable to obtain consent from all individuals given the large cohort and the fact that data were fully anonymized, preventing re-contact. All data were handled in strict confidentiality and in compliance with the principles of the Declaration of Helsinki.
Data analysis will be conducted using coded information, ensuring that no personal details (such as contact information, addresses, etc.) of the participants will be collected. All samples will be de-identified to fully protect the privacy rights of the participants. Furthermore, the data selected for this study will only be used for research purposes and will not be utilized for any other purposes. The public reporting of research results will not disclose any personal identities of the participants.
Study subjects and grouping From July 2022 to June 2024, PCOS patients undergoing frozen embryo transfer (FET) at the Reproductive Center of the Third Affiliated Hospital of Guangxi Medical University were enrolled, for a total of 555 cycles. Based on endometrial preparation regimens, participants were divided into three groups: HRT alone; artificial cycle after pretreatment with GnRH agonist at 1.5 mg (1.5 mg GnRH-a + HRT); artificial cycle after pretreatment with GnRH agonist at 3.75 mg (3.75 mg GnRH-a + HRT). Inclusion criteria followed the Rotterdam criteria for PCOS diagnosis (2003). Exclusion criteria included: (1) adenomyosis; (2) endometriosis; (3) intrauterine adhesions, endometrial polyps, or uterine malformations; (4) planned preimplantation genetic testing/PGT-PGS. Embryo transfer procedures were performed by physicians at our center with more than 20 years of experience. The study protocol was approved by the Ethics Committee of the Nanning Second People’s Hospital [Y2022100]. Flowchart of Study Population Selection (Figure 1).
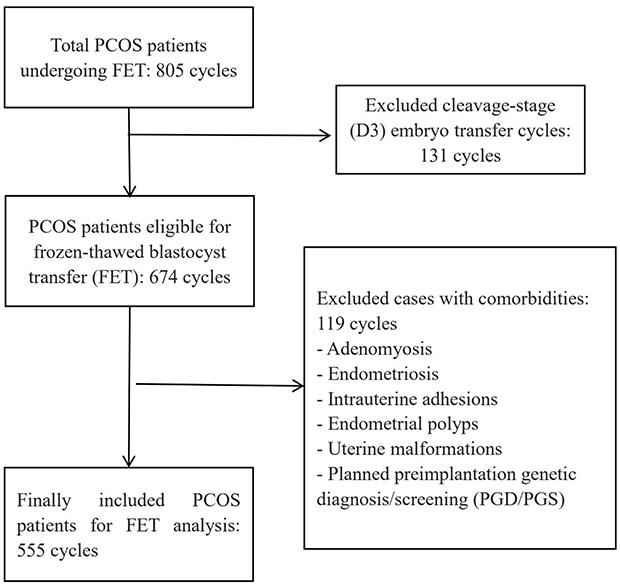 |
Figure 1 Flowchart of Study Population Selection. |
Regarding the unit of analysis, this study included all eligible FET cycles between July 2022 and June 2024. For some patients, multiple independent treatment cycles were included in the analysis. This approach was taken to fully reflect the clinical practice and cumulative pregnancy outcomes in this real-world cohort. We acknowledge that cycles from the same patient are not entirely independent; however, the primary aim of this analysis was to evaluate the treatment protocol’s effectiveness at the cycle level, which is a common and clinically relevant approach in reproductive medicine research.
Endometrial Preparation Methods
HRT group: On days 2–3 of the menstrual cycle, baseline hormonal assessment and transvaginal ultrasound (TVUS) were performed. Patients with estradiol (E2) < 50 pg/mL, progesterone (P) < 1 ng/mL, and no ovarian cysts on TVUS were administered oral estradiol valerate tablets (Bayer, Germany) at 2 mg twice daily for 5 days, after which the dose was increased to 3 mg twice daily. After 10–12 days of estradiol valerate administration, a follow-up TVUS was performed to monitor endometrial thickness and hormone levels. If the endometrial thickness was < 7 mm, vaginal estrogen tablets (Femoston, estradiol tablet/estradiol dydrogesterone tablet, Abbott, Netherlands) at 1 mg/day were added. When the endometrial thickness reached ≥ 7 mm, endometrial transformation was initiated using either intramuscular progesterone injections (60 mg/day) or vaginal progesterone gel (Crinone, 90 mg/day) plus dydrogesterone (20 mg twice daily). Frozen-thawed blastocyst transfer was performed on the 6th day after progesterone initiation. The dosages of estrogen and progesterone remained unchanged until 12–14 days after transfer.
1.5 mg GnRH-a + HRT Group
On menstrual cycle days 2–3, patients were administered oral Femoston (1 mg/day) for 21 days, followed by an intramuscular injection of 1.5 mg GnRH-a (Triptorelin acetate, Diphereline, IPSEN; from a 3.75 mg vial) for pituitary down-regulation. Twenty-eight days after commencing Femoston, awaiting the onset of menstruation. On days 2–3 of this subsequent cycle, serum hormone levels and TVUS were re-evaluated. Down-regulation criteria were defined as FSH < 5 mIU/mL, LH < 5 mIU/mL, E2 < 50 pg/mL, P < 1 ng/mL, and the absence of ovarian cysts on TVUS. Upon meeting these criteria, the oral estradiol valerate regimen, identical to that used in the HRT group, was initiated.
3.75 mg GnRH-a + HRT Group
On menstrual cycle days 2–3, patients received an intramuscular injection of 3.75 mg GnRH-a (Triptorelin acetate, Diphereline, IPSEN) for pituitary down-regulation. After 28 days, serum hormone levels and TVUS were reassessed. The same down-regulation criteria as in the 1.5 mg GnRH-a + HRT group were applied. Once these criteria were met, the oral estradiol valerate regimen, identical to that used in the HRT group, was initiated.
Embryo Vitrification, Thawing, and Selection
Vitrification and thawing were performed using standard vitrification protocols. Thawed blastocysts were graded on the day of transfer according to the Gardner scoring system. Blastocysts were classified into 6 stages based on the degree of expansion: Stage 1 (early blastocyst, blastocoel less than half the volume of the embryo); Stage 2 (blastocoel greater than or equal to half the volume of the embryo); Stage 3 (full blastocyst, blastocoel completely filling the embryo); Stage 4 (expanded blastocyst, blastocoel larger than the early embryo with a thinning zone); Stage 5 (hatching blastocyst, trophectoderm starting to herniate through the zone pellucida); Stage 6 (hatched blastocyst, blastocyst has completely escaped from the zone pellucida). Blastocysts at stages 3–6 were further graded for the quality of the inner cell mass (ICM) and trophectoderm (TE). ICM grading: A (tightly packed, many cells); B (loosely grouped, several cells); C (very few cells, may appear degenerate); D (no visible ICM). TE grading: A (many cells forming a cohesive epithelium); B (fewer cells forming a loose epithelium); C (very few large cells, often degenerate). Blastocysts achieving Stage 3 or higher with an ICM grade of C or better were considered viable for transfer. Those with a combined ICM/TE score of 3BB or higher were defined as high-quality blastocysts.
Assessment of Pregnancy Outcomes
Serum β-hCG levels were measured 12 days after blastocyst transfer. If pregnancy was confirmed, hormonal supplementation was maintained. Clinical pregnancy was confirmed by TVUS on day 28 after transfer, indicated by the presence of a gestational sac and primitive cardiac activity. Following confirmation of clinical pregnancy, estradiol valerate was gradually reduced and discontinued, and progesterone supplementation began to be tapered at 9 weeks of gestation, with complete discontinuation by 10–11 weeks.
Observational Indicators
This study reports data from 555 FET cycles. The following parameters were compared among the HRT-alone, 1.5 mg GnRH-a + HRT, and 3.75 mg GnRH-a + HRT groups: age, duration of infertility, body mass index (BMI), E2 level on the initiation day, LH level on the initiation day, endometrial thickness on the initiation day, endometrial thickness on the transformation day, E2 level on the transformation day, duration of estradiol valerate administration, number of embryos transferred, embryo implantation rate, clinical pregnancy rate, early miscarriage rate, and ectopic pregnancy rate.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics, version 26.0. For normally distributed continuous data, results are presented as mean ± standard deviation and compared by analysis of variance with LSD post hoc tests. Categorical variables were compared using the chi-square test or Fisher’s exact test as appropriate. A two-sided P value < 0.05 was considered statistically significant. For multiple comparisons across the three groups, a Bonferroni-adjusted significance level of 0.05/3 = 0.017 was applied (P < 0.017 considered significant). Variables potentially influencing pregnancy outcomes were entered into multivariate logistic regression analyses.
Results
Comparison of Baseline Characteristics Among the Three Groups
The comparison of baseline characteristics among the three groups showed no statistically significant differences in age, duration of infertility, BMI, E2 and LH levels at treatment initiation, endometrial thickness at initiation, endometrial thickness at progesterone transformation, serum E2 on the transformation day, or duration of estradiol valerate administration (P > 0.05).
Embryo Transfer Parameters
The proportion of double-embryo transfer (DET) cycles was significantly higher in the 1.5 mg GnRH-a + HRT group compared to the HRT-alone group (P < 0.001). No significant differences were observed in DET proportions between the following groups: 1.5 mg GnRH-a + HRT vs 3.75 mg GnRH-a + HRT groups (P > 0.05), HRT-alone vs 3.75 mg GnRH-a + HRT groups (P > 0.05), (Table 1).
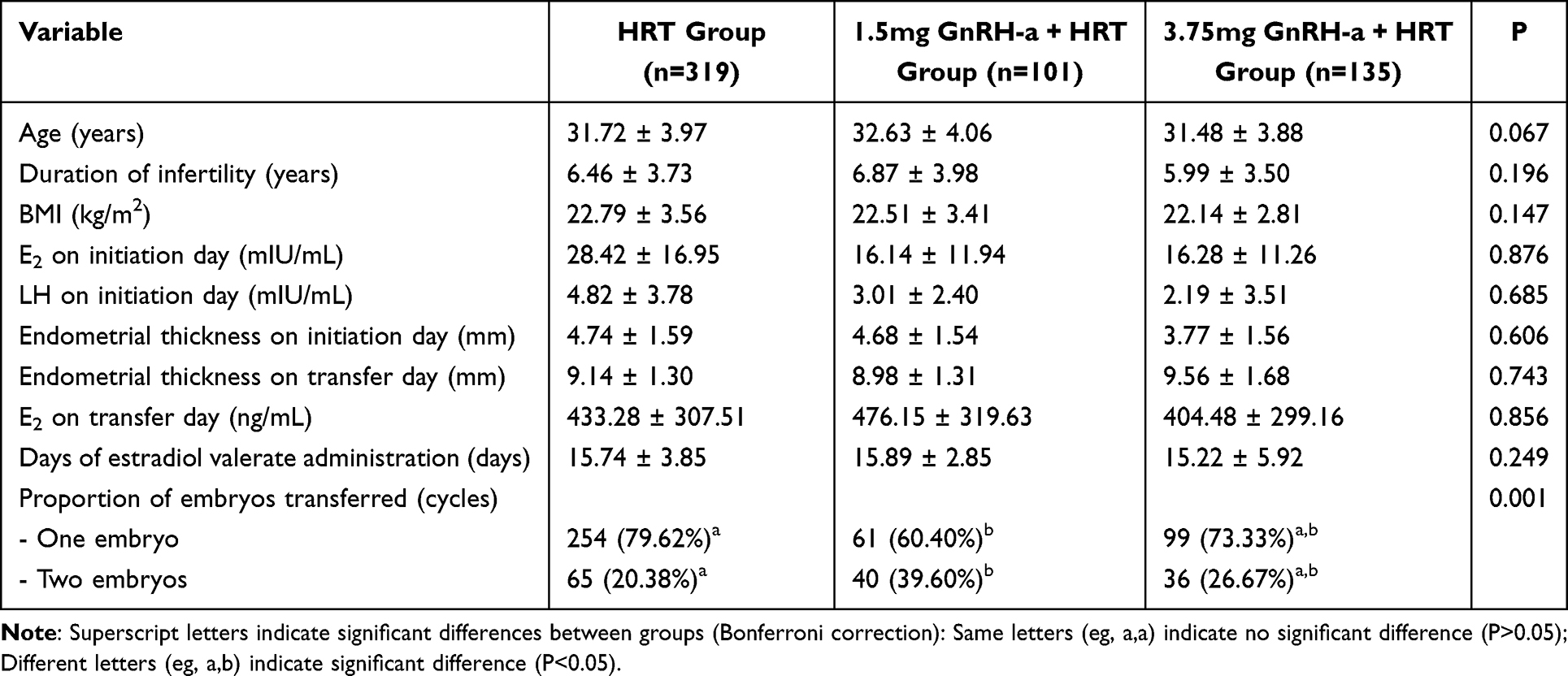 |
Table 1 Comparison of General Characteristics Among Groups |
Comparative Analysis of Embryo Implantation and Pregnancy Outcomes
No statistically significant differences were observed among the three groups for the following key outcomes (all P > 0.05): Embryo Implantation Rates:Group 1: 54.17%, Group 2: 46.81%, Group 3: 56.73%. Clinical Pregnancy Rates (CPR): Group 1: 57.68%, Group 2: 57.43%, Group 3: 63.70%. Early Miscarriage Rates: Group 1: 11.41%, Group 2: 13.24%, Group 3: 9.30%. Ectopic Pregnancy Rates: Group 1: 1.09%, Group 2: <0.01% (revised from 0.00%), Group 3: 1.16%, (Table 2).
 |
Table 2 Comparison of Pregnancy Outcomes Among Groups |
Logistic Regression Analysis
Adjusted for maternal age and BMI, the analysis confirmed that the transfer of two embryos (DET) significantly increased the probability of clinical pregnancy (aOR 2.68 [1.75–4.69], P < 0.001; Table 3).
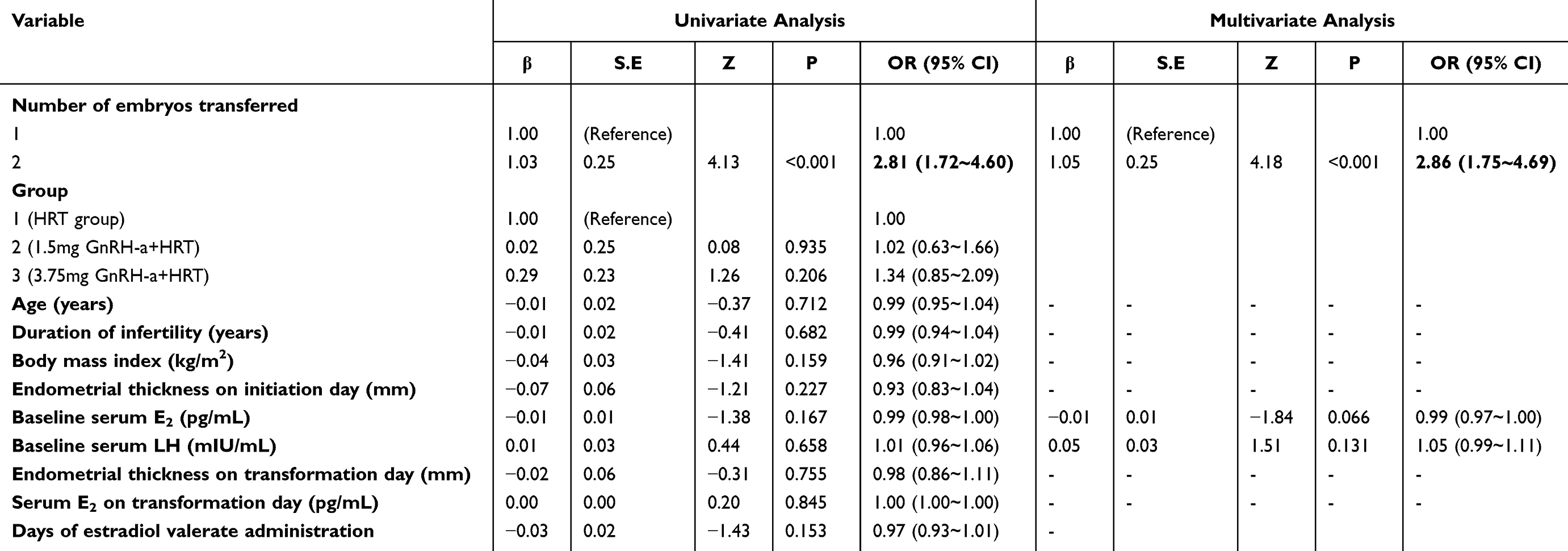 |
Table 3 Univariate and Multivariate Logistic Regression Results |
Discussion
This study compared 555 FET cycles and found that neither the 1.5 mg nor the 3.75 mg doses of GnRH-a pretreatment significantly improved the embryo implantation rate, clinical pregnancy rate, or early miscarriage rate in patients with PCOS. These findings suggest that GnRH-a pretreatment may not provide substantial benefit over HRT alone in this population. The artificial cycle regimen is commonly used for FET in PCOS patients due to its simplicity and flexibility. However, a key limitation of HRT is the risk of spontaneous follicular development, which can lead to cycle cancellation. Furthermore, the hyperandrogenic environment and elevated LH levels in PCOS may cause premature progesterone receptor expression, advancing the endometrium into a secretory phase and potentially shifting the implantation window, which could lower clinical pregnancy rates.13 While the pituitary downregulation induced by GnRH-a can suppress spontaneous ovulation and stabilize endometrial development,14 its clinical efficacy in improving pregnancy outcomes in this context remains inconsistent across studies. Previous reports on the utility of GnRH-a pretreatment are conflicting. Some studies support the use of GnRH-a downregulation combined with HRT, suggesting better clinical outcomes for PCOS patients compared to HRT alone.6–9 For example, Wang et al6 reported that this protocol was associated with significantly lower miscarriage rates and higher live birth rates. The potential mechanism may involve the modulation of endometrial receptivity. Experimental evidence indicates that endometrial function may be compromised in PCOS patients. A distinct aberrant inflammatory and immune signature observed in the PCOS endometrium potentially constitutes a primary mechanism underlying reduced fertility in this population.15 Both systemic circulation and local endometrial tissues in PCOS exhibit elevated inflammatory mediators, including IL-6 and TNF-α.16 Concurrent pathological processes such as enhanced oxidative stress and impaired angiogenesis further disrupt embryo implantation.17 Notably, GnRH-a administration during artificial cycle preparation for FET has been shown to regulate the expression of cytokines such as IL-6 and IL-11 in endometrial stromal cells,18 suggesting a potential pathway through which it could improve endometrial receptivity. Conversely, other studies align with our findings. A meta-analysis by Wu et al11 concluded that GnRH-a pretreatment showed no advantage for PCOS patients undergoing FET, and a randomized controlled trial by Luo et al12 involving 328 cycles found no differences in pregnancy outcomes but highlighted a significant increase in patient costs with GnRH-a downregulation. In our study, the 1.5 mg GnRH-a + HRT group exhibited the lowest numerical values for both embryo implantation rate and clinical pregnancy rate (46.81% vs 54.17%/56.73% and 57.43% vs 57.68%/63.70%, respectively), although these differences were not statistically significant. This may suggest that the 1.5 mg dose is insufficient to fully suppress elevated LH levels or adequately modulate the local inflammatory environment in some PCOS patients, thereby failing to optimize endometrial receptivity. A notable confounding factor was the significantly higher proportion of double-embryo transfer (DET) cycles in the 1.5 mg group (39.6%, P < 0.001), which may have partially offset a potential negative effect of the low-dose regimen. Our logistic regression analysis confirmed that the number of embryos transferred was the only factor significantly associated with clinical pregnancy (aOR 2.68 [1.75–4.69], P < 0.001). This underscores that embryo number, rather than GnRH-a pretreatment, was the primary determinant of success in our cohort and highlights the critical importance of controlling for this variable when evaluating different endometrial preparation protocols. In conclusion, our findings, consistent with several recent studies,10–12 indicate that GnRH-a downregulation pretreatment does not confer a significant benefit for clinical outcomes in PCOS patients undergoing FET. The potential to simplify the pretreatment protocol to a standard HRT regimen could reduce medical costs, minimize drug exposure, and avoid potential side effects for patients. This refocuses clinical emphasis towards optimizing embryo quality and transfer techniques rather than reliance on pharmacological pretreatments.
Conclusions
Clinical Implications of the Study
In summary, based on our data findings, for patients with PCOS undergoing FET, GnRH-a pretreatment (either 1.5 mg or 3.75 mg) may not have a significant advantage over simple HRT in improving pregnancy outcomes. The number of transferred embryos is a key factor affecting the success of pregnancy. This finding supports prioritizing a simple HRT regimen in FET for PCOS patients, which can simplify the treatment process, reduce medical costs and medication burden, and minimize potential adverse reactions. Therefore, it is recommended that clinical practice pay more attention to optimizing embryo quality and transfer techniques, rather than relying on routine GnRH-a pretreatment.
Limitations of the Study
However, the conclusions of this study should be interpreted in the context of its limitations. Given the retrospective nature of this study and its single-center design, the possibility of residual confounding cannot be excluded. Therefore, larger, multicenter randomized controlled trials are needed to further validate this conclusion and to explore specific PCOS patient subgroups that may benefit from GnRH-a pretreatment.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study received approval from the Ethics Committee of the Nanning Second People’s Hospital [Y2022100].
Acknowledgments
We acknowledge the clinical support provided by the Guangxi Clinical Research Center for Reproductive Medicine team during data collection. All researchers maintained independence in study design, data analysis, and interpretation. We would like to thank the funding which gave us financial support: The Self-funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region and the Guangxi Key Research and Development Program.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by The Self-funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region [grant number: Z-A20221144] and the Guangxi Key Research and Development Program [grant number: Guike AB25069053].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Expert Group of Consensus on Infertility Treatment and Fertility Preservation in Polycystic Ovary Syndrome, Subgroup of Reproductive Endocrinology and Fertility Preservation, Fertility Preservation Branch, Chinese Preventive Medicine Association. Consensus on infertility treatment and fertility preservation in polycystic ovary syndrome. J Reprod Med. 2020;29:843–851.
2. Stener-Victorin E, Teede H, Norman RJ, et al. Polycystic ovary syndrome. Nat Rev Dis Primers. 2024;10:27. doi:10.1038/s41572-024-00511-3
3. Hoeger KM, Dokras A, Piltonen TT. Update on PCOS consequences, challenges and guiding treatment. J Clin Endocrinol Metabolism. 2021;106:1071–1083. doi:10.1210/clinem/dgaa839
4. Yin JW, Yang W, Yu D, et al. International evidence-based guideline recommendations for assessment and management of polycystic ovary syndrome (2023 update). Chin J Reprod Contracept. 2023;43:1099–1113.
5. Palomba S, Costanzi F, Caserta D, et al. Pharmacological and non-pharmacological interventions for improving endometrial receptivity in infertile patients with polycystic ovary syndrome a comprehensive review of the available evidence. Reprod Biomed Online. 2024;49:104381. doi:10.1016/j.rbmo.2024.104381
6. Wang Y, Hu W-H, Wan Q, et al. Effect of artificial cycle with or without GnRH-a pretreatment on pregnancy and neonatal outcomes in women with PCOS after frozen embryo transfer a propensity score matching study. Reprod Biol Endocrinol. 2022;20:56. doi:10.1186/s12958-022-00929-y
7. Wei L, Tian B, Wang S, et al. Gonadotropin releasing hormone agonists combined with hormone replacement therapy significantly improves reproductive outcomes for patients with thin endometrium and intramural fibroids in frozen embryo transfer cycles. Drug Design Develop Ther. 2025;19:173–183. doi:10.2147/DDDT.S501809
8. Qi Q, Luo J, Wang Y, et al. Effects of artificial cycles with and without gonadotropin-releasing hormone agonist pretreatment on frozen embryo transfer outcomes. J Int Med Res. 2020;48:1–8. doi:10.1177/0300060520918474
9. Xu B, Hou Z, Liu N, et al. Pretreatment with a long-acting GnRH agonist for frozen-thawed embryo transfer cycles:how to improve live birth? J Ovarian Res. 2023;16:197. doi:10.1186/s13048-023-01277-0
10. Salemi S, Yahyaei A, Vesali S, et al. Endometrial preparation for vitrified–warmed embryo transfer with or without GnRH-agonist pre-treatment in patients with polycystic ovary syndrome: a randomized controlled trial. Reprod BioMed Online. 2021;43:446–452. doi:10.1016/j.rbmo.2021.06.006
11. Wu Y, Tu M, Liu Y, et al. GnRH agonist pretreatment for frozen embryo transfer among women with polycystic ovary syndrome: a narrow systematic review and meta-analysis of randomized controlled trials. Reprod Biol Endocrinol. 2024;22:121. doi:10.1186/s12958-024-01293-9
12. Luo L, Chen M, Wen Y, et al. Pregnancy outcome and cost‐effectiveness comparisons of artificial cycle‐prepared frozen embryo transfer with or without GnRH agonist pretreatment for polycystic ovary syndrome: a randomised controlled trial. BJOG. 2020;128:667–674. doi:10.1111/1471-0528.16461
13. Kanamarlapudi V, Gordon UD, Bernal AL. Luteinizing hormonechorionic gonadotrophin receptor overexpressed in granulosa cells from polycystic ovary syndrome ovaries is functionally active. Reprod Biomed Online. 2016;6:635–641. doi:10.1016/j.rbmo.2016.03.003
14. Groenewoud ER, Cantineau AEP, Kollen BJ, et al. What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? A systematic review and meta-analysis. Human Reprod Update. 2017;19:458–470. doi:10.1093/humupd/dmt030
15. Palomba S. Is fertility reduced in ovulatory women with polycystic ovary syndrome? An opinion paper. Human Reprod. 2021;36:2421–2428. doi:10.1093/humrep/deab181
16. Di Pietro C, Cicinelli E, Guglielmino MR. Altered transcriptional regulation of cytokines, growth factors, and apoptotic proteins in the endometrium of infertile women with chronic endometritis. Am J Reprod Immunol. 2013;69:509–517. doi:10.1111/aji.12076
17. Guo F, Huang Y, Fernando T, et al. Altered molecular pathways and biomarkers of endometrial receptivity in infertile women with polycystic ovary syndrome. Reprod Sci. 2022;29:3335–3345. doi:10.1007/s43032-022-00845-x
18. Li L, Liu L, Kou Z, et al. GnRH agonist treatment regulates IL-6 and IL-11 expression in endometrial stromal cells for patients with HRT regiment in frozen embryo transfer cycles. Reprod Biol. 2022;22:100608. doi:10.1016/j.repbio.2022.100608
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.