Back to Journals » Drug Design, Development and Therapy » Volume 20
GLUT5-Driven Gut-Liver Axis Injury Mediating Olanzapine-Induced NAFLD and Dapagliflozin Intervention
Authors Chen X, Zhang Y, Wang J, Chen L, He SM, Wang DD ![]()
Received 10 December 2025
Accepted for publication 18 February 2026
Published 27 February 2026 Volume 2026:20 584833
DOI https://doi.org/10.2147/DDDT.S584833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiao Chen,1,* Yue Zhang,2,* Jie Wang,2,* Liang Chen,2 Su-Mei He,3 Dong-Dong Wang2
1School of Nursing, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Jiangsu Key Laboratory of New Drug Research and Clinical Pharmacy & School of Pharmacy, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Pharmacy, Suzhou Research Center of Medical School, Suzhou Hospital, Affiliated Hospital of Medical School, Nanjing University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su-Mei He, Department of Pharmacy, Suzhou Research Center of Medical School, Suzhou Hospital, Affiliated Hospital of Medical School, Nanjing University, Suzhou, Jiangsu, 215153, People’s Republic of China, Email [email protected] Dong-Dong Wang, Jiangsu Key Laboratory of New Drug Research and Clinical Pharmacy & School of Pharmacy, Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China, Email [email protected]
Objective: Drugs are an important cause of non-alcoholic fatty liver disease (NAFLD), and olanzapine is the main drug that leads to NAFLD. However, the mechanism by which this drug causes NAFLD is still unclear at present. We previously found that dapagliflozin had certain intervention effect on patients with NAFLD. This study aimed to explore the mechanism of olanzapine-induced NAFLD and the intervention effect of dapagliflozin.
Methods: Twenty-four female wistar rats were classified into control (NC) group, olanzapine (OLA) group, and dapagliflozin intervention (DAP) group for a total of 12 weeks of intervention. This study explored the specific mechanism of olanzapine-induced NAFLD and potential treatment method from dapagliflozin through transcriptomics, molecular biology, and pathological staining methods in animal models.
Results: The transcriptome and immunohistochemistry studies of the intestine and liver revealed the high expression of GLUT5 in both tissues (P < 0.01). Olanzapine induced gut-liver axis injury via GLUT5/AMPK/mTOR (P < 0.05 or P < 0.01). Dapagliflozin reversed GLUT5/AMPK/mTOR to improve intestinal barrier injury, NAFLD and hepatic fibrosis (P < 0.05 or P < 0.01).
Conclusion: The study discovered for the first time that GLUT5/AMPK/mTOR drived gut-liver axis injury mediating olanzapine-induced NAFLD and dapagliflozin intervention could reverse GLUT5/AMPK/mTOR-driven gut-liver axis injury ameliorating olanzapine-induced NAFLD. This provided a new understanding of the occurrence of olanzapine-induced NAFLD and offered a reference plan for its clinical intervention.
Keywords: GLUT5, gut-liver axis, olanzapine, NAFLD, dapagliflozin
Introduction
Schizophrenia is a serious mental disorder that mainly affects a patient’s thinking, emotions, perception and behavior, making it difficult for them to distinguish reality from illusion. It often begins in young adulthood, has a protracted course, and about half of the patients may develop mental disability, causing significant burdens on individuals, families and society.1–5 At present, the main treatment for schizophrenia is antipsychotic drugs.6,7 Second-generation antipsychotic drugs have largely replaced first-generation antipsychotic drugs due to their broad spectrum of action and fewer extrapyramidal reactions and have become the preferred drugs for treating schizophrenia. However, the risk of developing non-alcoholic fatty liver disease (NAFLD) significantly increases in patients taking second-generation antipsychotic drugs, especially olanzapine.8–14
NAFLD is a liver phenotype caused by metabolic disorders, whose global incidence rate is 559.95 per 100,000 people, with a mortality rate of 1.93 per 100,000.15 NAFLD is a liver-specific disease and an intermediary for many other diseases, which can exacerbate other chronic liver diseases, and in severe cases, it can lead to decompensated liver cirrhosis, liver cancer, and increase the risk of type 2 diabetes and cardiovascular diseases.16–26 Drugs are an important cause of NAFLD, and olanzapine is the main drug that leads to NAFLD.8–14 However, the mechanism by which this drug causes NAFLD is still unclear at present. The gut-liver axis is a system through which the intestine and the liver communicate bidirectionally via the portal vein, bile ducts, etc.27–30 It has a close interaction relationship with NAFLD.31–34 NAFLD usually accompanied by impaired intestinal barrier function, allowing bacterial endotoxins to enter the bloodstream, triggering chronic inflammation and fat accumulation in the liver.35–39 Is the occurrence of olanzapine-induced NAFLD also related to the gut-liver axis injury? What is the specific mechanism? These key questions are currently unknown.
Dapagliflozin, as an SGLT2 inhibitor, not only lowers blood sugar but also has various important functions such as promoting weight loss, protecting the heart, and protecting the liver and kidneys.40–44 Importantly, we previously found that dapagliflozin had certain intervention effect on patients with NAFLD.43 Therefore, in this study, we designed a dapagliflozin administration group to observe the intervention effect of dapagliflozin on olanzapine-induced NAFLD. Based on these, this study aimed to explore the mechanism of olanzapine-induced NAFLD and the intervention effect of dapagliflozin.
Materials and Methods
Animal Experiment
Given sex difference in NAFLD susceptibility, random 24 female wistar rats (aged about 4 weeks) grouping as control (NC) group (n=8), olanzapine (OLA) group (n=8), and dapagliflozin intervention (DAP) group (n=8), who were bought from Vital River Laboratory Animal Technology Co., Ltd. Based on the preceding discussion, the animals were housed in standard cages under controlled environmental conditions, with ambient temperature maintained at 20–25°C, relative humidity regulated between 40% and 70%, and a 12-hour light/dark cycle. The animals had ad libitum access to standard laboratory chow and drinking water. OLA and DAP groups were intervened by gavage with 5 mg/kg/day olanzapine (Lot number: 231106, EASTON BIOPHARMACEUTICALS) and NC group was intervened by gavage with equal volume of CMCNa. Furthermore, DAP group was intervened by gavage with 1 mg/kg/day dapagliflozin (Lot number: TC2508, AstraZeneca) and NC, OLA groups were intervened by gavage with equal volume of CMCNa. This experiment was conducted for a total of 12 weeks of intervention. In this study, humane endpoints were established for animal experiments. The criteria for triggering humane endpoints included: labored breathing, uncontrolled hemorrhage, convulsions or paralysis, inability to self-feed or drink for >24 hours, weakness leading to inability to stand upright. Animals meeting any of these criteria were euthanized promptly to minimize suffering. They were sacrificed via dislocation of the cervical spine. These procedures were carried out in accordance with applicable veterinary guideline of American Veterinary Medical Association. Animal protocols and procedures were approved by The Animal Care and Use Committee of Xuzhou Medical University (No.202401T029). In addition, we complied with Guideline for Ethical Review of Animal Welfare (GB/T 35892-2018) to ensure the welfare of the experimental animals used in our research.
Sample Collection
After a 12-week experimental intervention, sacrificing all the animals and extracting samples such as intestines, livers and blood for later testing. The fresh intestines and livers were fixed using tissue fixation fluid, and the residual intestines and livers were rapidly freezed using liquid nitrogen.
Pathological Staining
Pathological staining incorporated oil red, masson, sirius red, AB-PAS, PAS. Oil red dye kit (G1015), masson dye kit (G1006), sirius red dye kit (G1018), PAS dye kit (G1008), AB-PAS dye kit (G1049) were bought from Servicebio Biotechnology (Wuhan) Co., Ltd. Take pictures with the pathological section scanner (3DHISTECH Pannoramic, version: Pannoramic MIDI) and mean of integral optical density (IOD) was used to analyze the results.
Transcriptomic Analysis
Transcriptome sequencing included RNA extraction, quality detection, library construction, library quality control, sequencing, gene expression quantitative analysis, gene differential expression analysis, functional enrichment analysis, et al.
Immunohistochemical Staining
Immunohistochemical staining was used to explore GLUT5 expression. Antibody against GLUT5 (TD13545) was bought from Abmart Medical Technology (Shanghai) Co., Ltd. Take pictures with the pathological section scanner and mean of IOD was used to analyze the results.
Immunofluorescent Staining
Immunofluorescent staining was used to analyze the expression of occludin, claudin-1, ZO-1, COLI, COLIII, fibronectin, E-cadherin, α-SMA. Antibodies against occludin (GB111401), COLI (GB11022-3), COLIII (GB111629), fibronectin (GB114491), E-cadherin (GB12083), α-SMA (GB111364) were bought from Servicebio Biotechnology (Wuhan) Co., Ltd. Antibodies against claudin-1 (TD6919), ZO-1 (TA5145) were bought from Abmart Medical Technology (Shanghai) Co., Ltd. Take pictures with the pathological section scanner and mean of IOD was used to analyze the results.
Western Blotting
Western blotting was used for exploring the expression of occludin, claudin-1, ZO-1, E-cadherin, α-SMA, GLUT5, p-AMPK, p-mTOR. Antibodies against occludin (GB11149), ZO-1 (GB115686) were bought from Servicebio Biotechnology (Wuhan) Co., Ltd. Antibodies against claudin-1 (TD6919), GLUT5 (TD13545), E-cadherin (TA0131), α-SMA (T55295) were bought from Abmart Medical Technology (Shanghai) Co., Ltd. Antibody against p-mTOR (ab137133) was bought from Abcam. Antibody against p-AMPK (P17273) was bought from ProMab biotechnologies, Inc. Antibodies against β-actin (66009-1-Ig), GAPDH (60004-1-Ig) were bought from Proteintech Group, Inc. Western blotting was tested via chemiluminescence gel imager (Tanon, Tanon-4600) and results were used for semi-quantitative analysis.
Statistical Analysis
The comparison between the two groups was conducted using the T-test, while the comparison among the three groups was performed using the ANOVA analysis. P < 0.05 or P < 0.01 was considered as statistically significant difference.
Results
Olanzapine Induced Gut-Liver Axis Injury
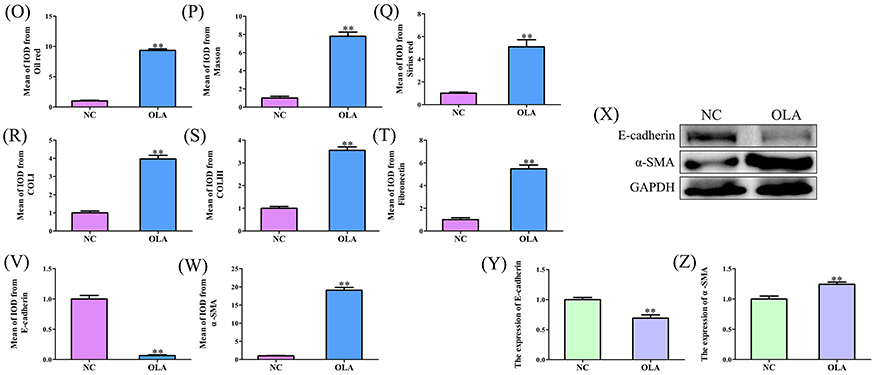
Figure 1A–F were immunofluorescent staining of occludin, claudin-1, ZO-1 in ileum and colon, respectively. Figure 1G was Western blotting of occludin, claudin-1, ZO-1. Figure 1H–J were corresponding statistical analysis of occludin, claudin-1, ZO-1 from Western blotting, respectively, in which compared with NC group the expression of occludin, claudin-1, ZO-1 were reduced in OLA group (P < 0.05 or P < 0.01). These results suggested that olanzapine induced intestinal barrier injury. Figure 1K was oil red staining, masson staining, sirius red staining of liver. Figure 1L–N were immunofluorescent staining of COLI, COLIII, fibronectin in liver. Figure 1O–Q were corresponding statistical analysis of oil red staining, masson staining, sirius red staining in liver, in which compared with NC group, the results of oil red staining, masson staining, sirius red staining in liver were deteriorative in OLA group (P < 0.01). Figure 1R–T were corresponding statistical analysis of COLI, COLIII, fibronectin in liver, in which compared with NC group, the expression of COLI, COLIII, fibronectin in liver were increased in OLA group (P < 0.01). Figure 1U–W were immunofluorescent staining of E-cadherin/α-SMA and corresponding statistical analysis of E-cadherin/α-SMA from immunofluorescent staining in liver, where compared with NC group, the expression of E-cadherin in liver from immunofluorescent staining was reduced in OLA group (P < 0.01), on the other hand the expression of α-SMA in liver from immunofluorescent staining was increased in OLA group (P < 0.01). Figure 1X–Z were Western blotting of E-cadherin/α-SMA and corresponding statistical analysis of E-cadherin/α-SMA from Western blotting in liver, where compared with NC group, the expression of E-cadherin in liver from Western blotting was reduced in OLA group (P < 0.01), on the other hand the expression of α-SMA in liver from Western blotting was increased in OLA group (P < 0.01). These results suggested that olanzapine induced NAFLD and hepatic fibrosis.
Figure 1 Continued. Figure 1 Olanzapine induced gut-liver axis injury. (A) Immunofluorescent staining of occludin in ileum. (B) Immunofluorescent staining of claudin-1 in ileum. (C) Immunofluorescent staining of ZO-1 in ileum. (D) Immunofluorescent staining of occludin in colon. (E) Immunofluorescent staining of claudin-1 in colon. (F) Immunofluorescent staining of ZO-1 in colon. (G) Western blotting of occludin, claudin-1, ZO-1. (H) Corresponding statistical analysis of occludin from Western blotting. (I) Corresponding statistical analysis of claudin-1 from Western blotting. (J) Corresponding statistical analysis of ZO-1 from Western blotting. (K) Oil red staining, masson staining, sirius red staining of liver. (L) Immunofluorescent staining of COLI in liver. (M) Immunofluorescent staining of COLIII in liver. (N) Immunofluorescent staining of fibronectin in liver. (O) Corresponding statistical analysis of oil red staining in liver. (P) Corresponding statistical analysis of masson staining in liver. (Q) Corresponding statistical analysis of sirius red staining in liver. (R) Corresponding statistical analysis of COLI in liver. (S) Corresponding statistical analysis of COLIII in liver. (T) Corresponding statistical analysis of fibronectin in liver. (U) Immunofluorescent staining of E-cadherin/α-SMA in liver. (V) Corresponding statistical analysis of E-cadherin from immunofluorescent staining in liver. (W) Corresponding statistical analysis of α-SMA from immunofluorescent staining in liver. (X) Western blotting of E-cadherin/α-SMA in liver. (Y) Corresponding statistical analysis of E-cadherin from Western blotting in liver. (Z) Corresponding statistical analysis of α-SMA from Western blotting in liver. *P < 0.05, **P < 0.01 vs NC. Scale bar was 200 µm. Abbreviations: NC, control group; OLA, olanzapine group; FN, fibronectin; E-ca, E-cadherin.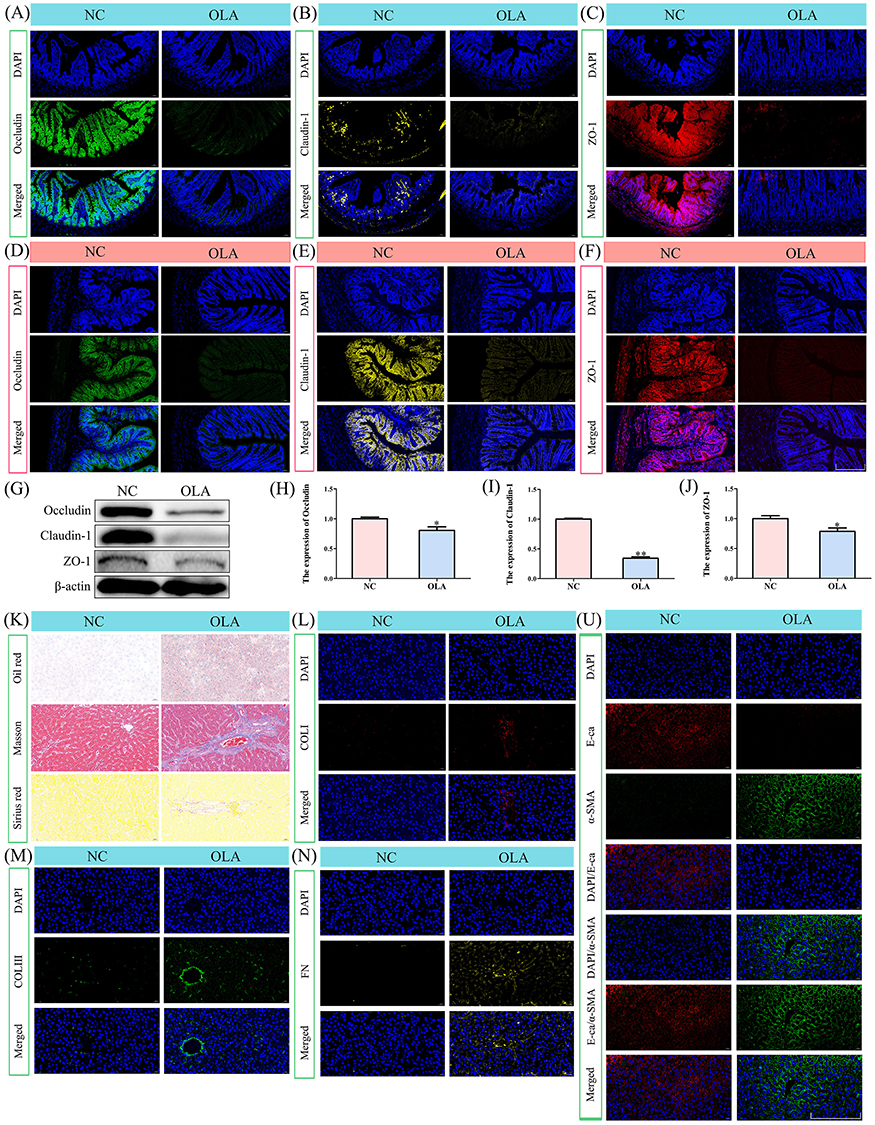
GLUT5 Was Increased in Intestinal Tract
Figure 2A–F were violin plot, heatmap, genome circus, volcano map, KEGG pathways enrichment, and carbohydrate digestion and absorption, where these transcriptomic results indicated that GLUT5 was highly expressed in intestinal barrier injury. Figure 2G–I were immunohistochemical staining and corresponding statistical analysis of GLUT5 in ileum and colon, respectively, where compared with NC group, the expression of GLUT5 in ileum and colon from immunohistochemical staining were increased in OLA group (P < 0.01). These results proved again that GLUT5 was highly expressed in intestinal barrier injury.
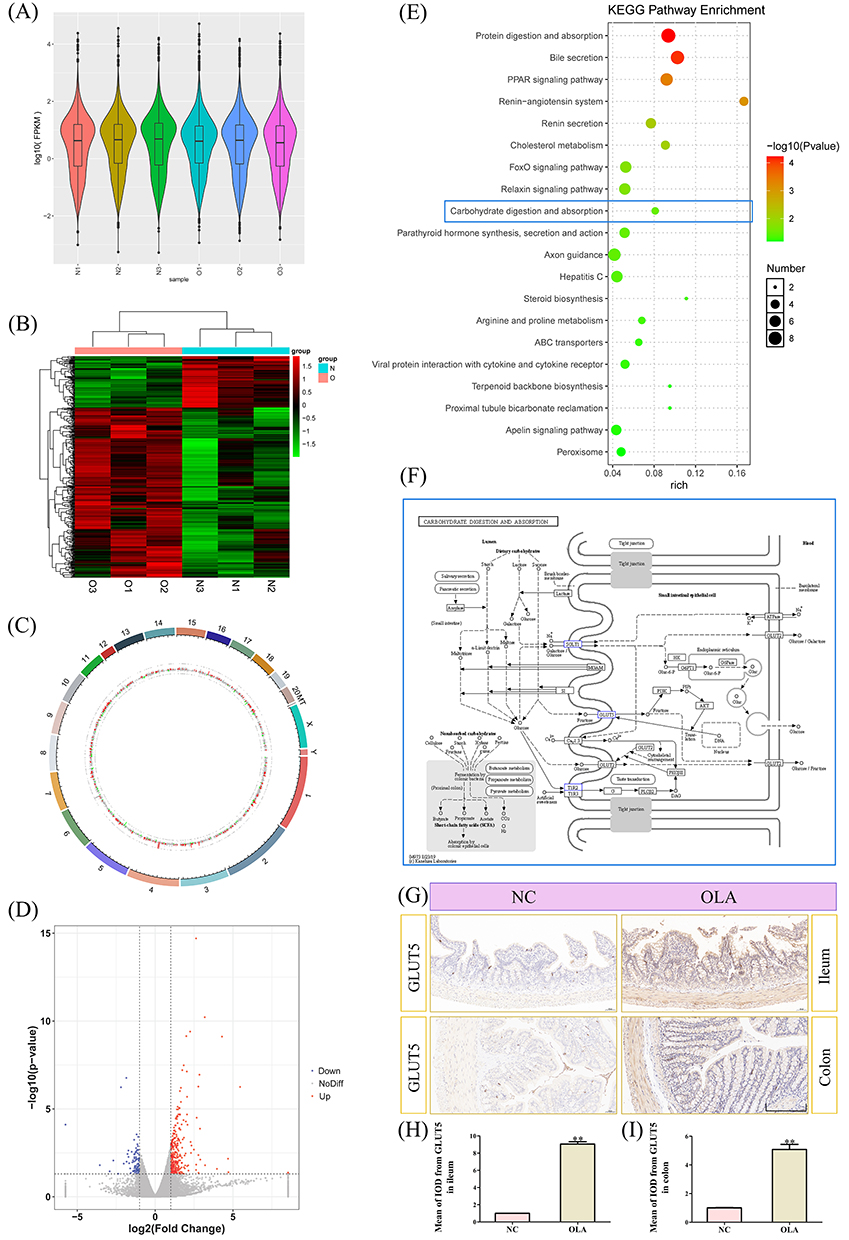 |
Figure 2 GLUT5 was increased in intestinal tract. (A) Violin plot. (B) Heatmap. (C) Genome circos. (D) Volcano map. (E) KEGG pathways enrichment. (F) Carbohydrate digestion and absorption. (G) Immunohistochemical staining of GLUT5 in ileum and colon. (H) Corresponding statistical analysis of GLUT5 in ileum. (I) Corresponding statistical analysis of GLUT5 in colon. Highlighted box represented the changed pathway or protein. **P < 0.01 vs NC. N1, N2, N3 were from NC group. O1, O2, O3 were from OLA group. Scale bar was 200 µm. Abbreviations: NC, control group; OLA, olanzapine group. |
GLUT5 Was Increased in Liver
Figure 3A–F were violin plot, heatmap, genome circus, volcano map, KEGG pathways enrichment, and carbohydrate digestion and absorption, where these transcriptomic results indicated that GLUT5 was highly expressed in NAFLD and hepatic fibrosis. Figure 3G and H were immunohistochemical staining and corresponding statistical analysis of GLUT5 in liver, where compared with NC group, the expression of GLUT5 in liver from immunohistochemical staining was increased in OLA group (P < 0.01). These results proved again that GLUT5 was highly expressed in NAFLD and hepatic fibrosis.
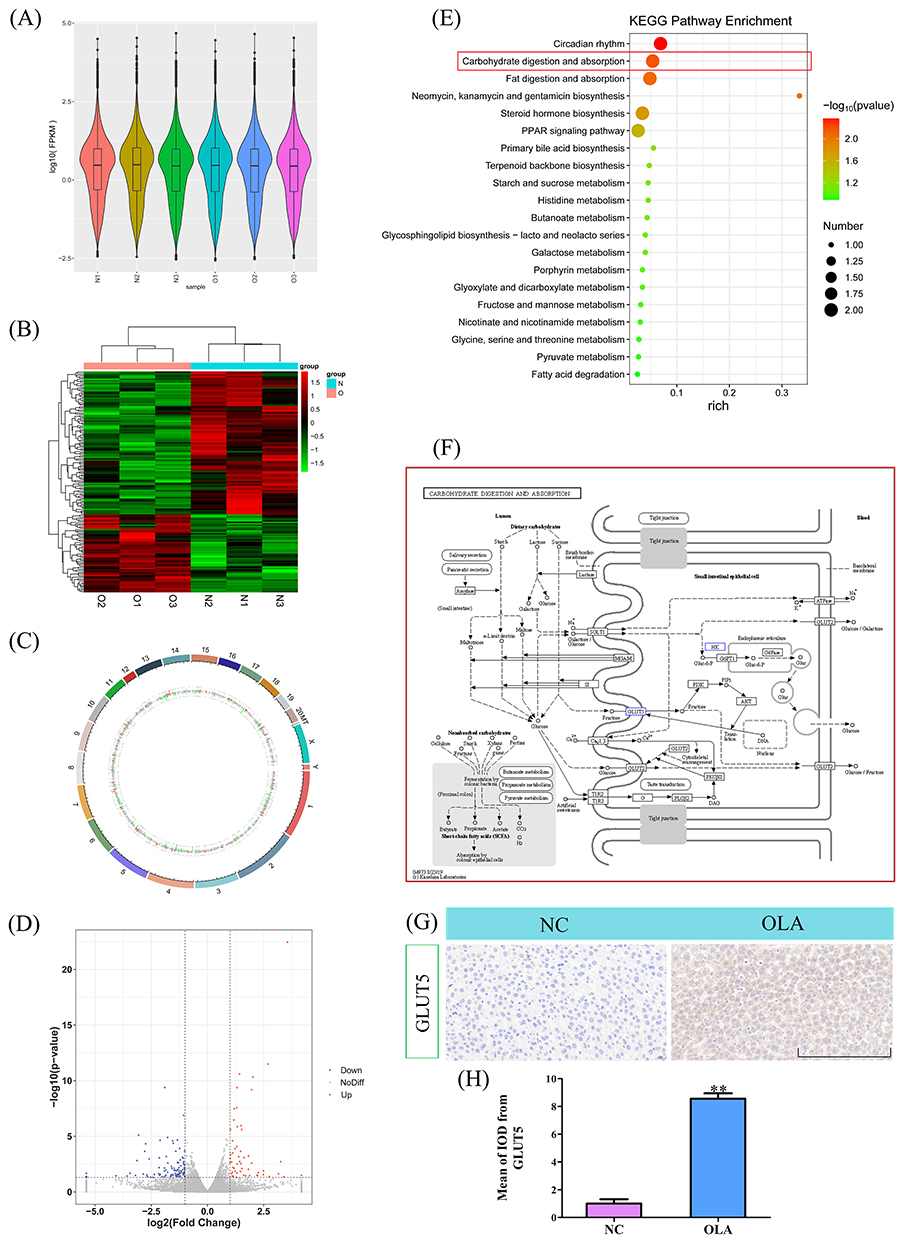 |
Figure 3 GLUT5 was increased in liver. (A) Violin plot. (B) Heatmap. (C) Genome circos. (D) Volcano map. (E) KEGG pathways enrichment. (F) Carbohydrate digestion and absorption. (G) Immunohistochemical staining of GLUT5 in liver. (H) Corresponding statistical analysis of GLUT5 in liver. Highlighted box represented the changed pathway or protein. **P < 0.01 vs NC. N1, N2, N3 were from NC group. O1, O2, O3 were from OLA group. Scale bar was 200 µm. Abbreviations: NC, control group; OLA, olanzapine group. |
Scientific Hypothesis of Olanzapine Activated GLUT5/AMPK/mTOR Driving Gut-Liver Axis Injury
Figure 4A–D were Western blotting of GLUT5, p-AMPK, p-mTOR and corresponding statistical analysis of GLUT5, p-AMPK, p-mTOR from Western blotting in intestinal tract, where compared with NC group, the expression of GLUT5, p-mTOR in intestinal tract from Western blotting were increased in OLA group (P < 0.05 or P < 0.01), on the other hand the expression of p-AMPK in intestinal tract from Western blotting was reduced in OLA group (P < 0.01). These results suggested that olanzapine activated GLUT5/AMPK/mTOR in intestinal barrier injury. Figure 4E–H were Western blotting of GLUT5, p-AMPK, p-mTOR and corresponding statistical analysis of GLUT5, p-AMPK, p-mTOR from Western blotting in liver, where compared with NC group, the expression of GLUT5, p-mTOR in liver from Western blotting were increased in OLA group (P < 0.05 or P < 0.01), on the other hand the expression of p-AMPK in liver from Western blotting was reduced in OLA group (P < 0.01). These results suggested that olanzapine activated GLUT5/AMPK/mTOR in NAFLD and hepatic fibrosis. Figure 4I was scientific hypothesis of olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury.
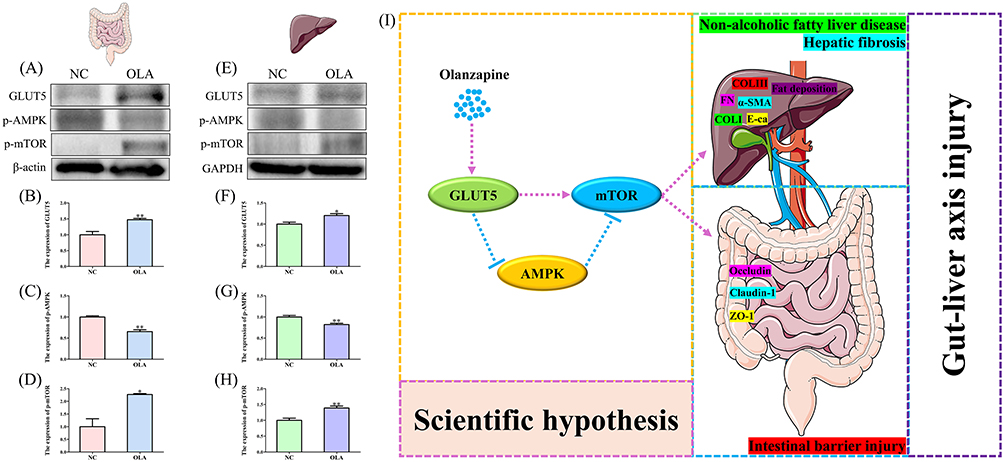 |
Figure 4 Scientific hypothesis of olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury. (A) Western blotting of GLUT5, p-AMPK, p-mTOR in intestinal tract. (B) Corresponding statistical analysis of GLUT5 from Western blotting in intestinal tract. (C) Corresponding statistical analysis of p-AMPK from Western blotting in intestinal tract. (D) Corresponding statistical analysis of p-mTOR from Western blotting in intestinal tract. (E) Western blotting of GLUT5, p-AMPK, p-mTOR in liver. (F) Corresponding statistical analysis of GLUT5 from Western blotting in liver. (G) Corresponding statistical analysis of p-AMPK from Western blotting in liver. (H) Corresponding statistical analysis of p-mTOR from Western blotting in liver. (I) Scientific hypothesis of olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury. *P < 0.05, **P < 0.01 vs NC. Abbreviations: NC, control group; OLA, olanzapine group. |
Dapagliflozin Reversed GLUT5/AMPK/mTOR to Improve Intestinal Barrier Injury
Figure 5A was flow chart. Figure 5B–D were AB-PAS/PAS staining in ileum and colon and corresponding statistical analysis of PAS staining in ileum and colon, where compared with NC group, the expression of PAS staining in ileum and colon were increased in OLA group (P < 0.01), compared with OLA group, the expression of PAS staining in ileum and colon were reduced in DAP group (P < 0.01). Figure 5E–H were Western blotting of GLUT5, p-AMPK, p-mTOR and corresponding statistical analysis of GLUT5, p-AMPK, p-mTOR from Western blotting in intestinal tract, where compared with NC group, the expression of GLUT5, p-mTOR in intestinal tract from Western blotting were increased in OLA group (P < 0.01), on the other hand the expression of p-AMPK in intestinal tract from Western blotting was reduced in OLA group (P < 0.01). Compared with OLA group, the expression of GLUT5, p-mTOR in intestinal tract from Western blotting were reduced in DAP group (P < 0.05 or P < 0.01), on the other hand the expression of p-AMPK in intestinal tract from Western blotting was increased in DAP group (P < 0.05). These results suggested that olanzapine activated GLUT5/AMPK/mTOR in intestinal barrier injury, and dapagliflozin could reverse GLUT5/AMPK/mTOR. Figure 5I–L were Western blotting of occludin, claudin-1, ZO-1 and corresponding statistical analysis of occludin, claudin-1, ZO-1 from Western blotting, respectively, in which compared with NC group the expression of occludin, claudin-1, ZO-1 were reduced in OLA group (P < 0.05 or P < 0.01), and compared with OLA group the expression of occludin, claudin-1, ZO-1 were increased in DAP group (P < 0.05 or P < 0.01). Figure 5M–O were immunofluorescent staining of occludin, claudin-1, ZO-1 in ileum. Figure 5P–R were immunofluorescent staining of occludin, claudin-1, ZO-1 in colon. These results suggested that dapagliflozin reversed GLUT5/AMPK/mTOR to improve intestinal barrier injury.
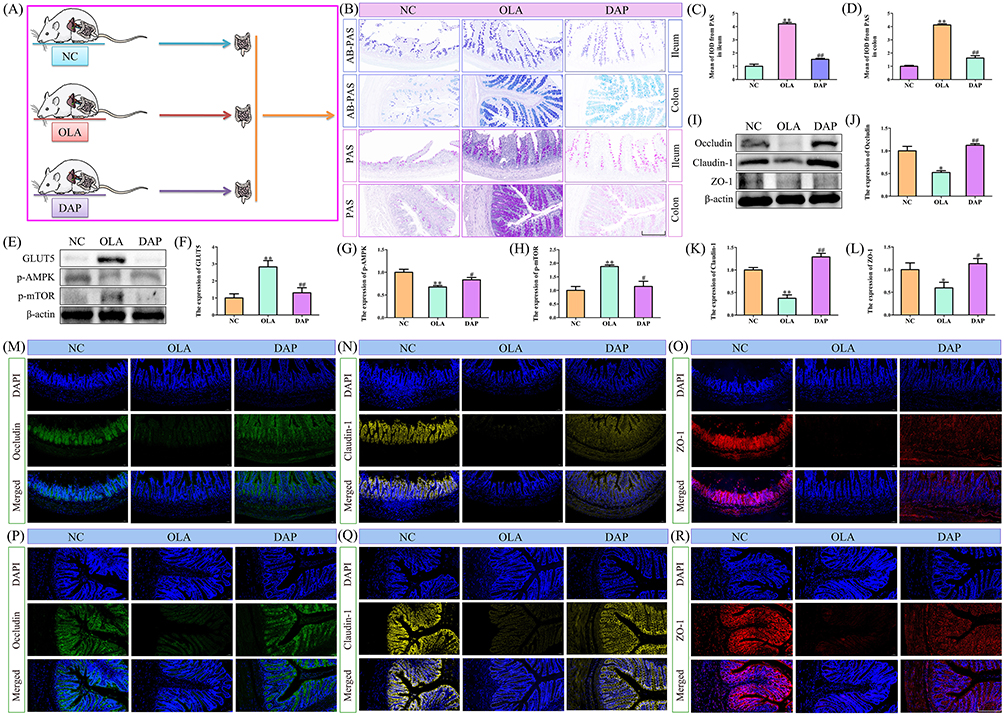 |
Figure 5 Dapagliflozin reversed GLUT5/AMPK/mTOR to improve intestinal barrier injury. (A) Flow chart. (B) AB-PAS/PAS staining in ileum and colon. (C) Corresponding statistical analysis of PAS staining in ileum. (D) Corresponding statistical analysis of PAS staining in colon. (E) Western blotting of GLUT5, p-AMPK, p-mTOR in intestinal tract. (F) Corresponding statistical analysis of GLUT5 from Western blotting in intestinal tract. (G) Corresponding statistical analysis of p-AMPK from Western blotting in intestinal tract. (H) Corresponding statistical analysis of p-mTOR from Western blotting in intestinal tract. (I) Western blotting of occludin, claudin-1, ZO-1. (J) Corresponding statistical analysis of occludin from Western blotting. (K) Corresponding statistical analysis of claudin-1 from Western blotting. (L) Corresponding statistical analysis of ZO-1 from Western blotting. (M) Immunofluorescent staining of occludin in ileum. (N) Immunofluorescent staining of claudin-1 in ileum. (O) Immunofluorescent staining of ZO-1 in ileum. (P) Immunofluorescent staining of occludin in colon. (Q) Immunofluorescent staining of claudin-1 in colon. (R) Immunofluorescent staining of ZO-1 in colon. *P < 0.05, **P < 0.01 vs NC. #P < 0.05, ##P < 0.01 vs OLA. Scale bar was 200 µm. Abbreviations: NC, control group; OLA, olanzapine group; DAP, dapagliflozin intervention group. |
Dapagliflozin Reversed GLUT5/AMPK/mTOR to Improve Liver Injury
Figure 6A was flow chart. Figure 6B and C were ALT and AST, where compared with NC group, ALT and AST were increased in OLA group (P < 0.05 or P < 0.01), and compared with OLA group, ALT and AST were reduced in DAP group (P < 0.05 or P < 0.01). Figure 6D was oil red staining, masson staining, sirius red staining of liver. Figure 6E–G were corresponding statistical analysis of oil red staining, masson staining, sirius red staining in liver, in which compared with NC group, the results of oil red staining, masson staining, sirius red staining in liver were deteriorative in OLA group (P < 0.01), compared with OLA group, the results of oil red staining, masson staining, sirius red staining in liver were ameliorative in DAP group (P < 0.01). Figure 6H–K were Western blotting of GLUT5, p-AMPK, p-mTOR and corresponding statistical analysis of GLUT5, p-AMPK, p-mTOR from Western blotting in liver, where compared with NC group, the expression of GLUT5, p-mTOR in liver from Western blotting were increased in OLA group (P < 0.01), on the other hand the expression of p-AMPK in liver from Western blotting was reduced in OLA group (P < 0.05). Compared with OLA group, the expression of GLUT5, p-mTOR in liver from Western blotting were reduced in DAP group (P < 0.05), on the other hand the expression of p-AMPK in liver from Western blotting was increased in DAP group (P < 0.05). Figure 6L–N were immunofluorescent staining of COLI, COLIII, fibronectin in liver. Figure 6O–Q were corresponding statistical analysis of COLI, COLIII, fibronectin in liver, in which compared with NC group, the expression of COLI, COLIII, fibronectin in liver were increased in OLA group (P < 0.01), compared with OLA group, the expression of COLI, COLIII, fibronectin in liver were reduced in DAP group (P < 0.01). Figure 6R–T were Western blotting of E-cadherin/α-SMA and corresponding statistical analysis of E-cadherin/α-SMA from Western blotting in liver, where compared with NC group, the expression of E-cadherin in liver from Western blotting was reduced in OLA group (P < 0.05), on the other hand the expression of α-SMA in liver from Western blotting was increased in OLA group (P < 0.05). Compared with OLA group, the expression of E-cadherin in liver from Western blotting was increased in DAP group (P < 0.01), on the other hand the expression of α-SMA in liver from Western blotting was reduced in DAP group (P < 0.01). Figure 6U–W were immunofluorescent staining of E-cadherin/α-SMA and corresponding statistical analysis of E-cadherin/α-SMA from immunofluorescent staining in liver, where compared with NC group, the expression of E-cadherin in liver from immunofluorescent staining was reduced in OLA group (P < 0.01), on the other hand the expression of α-SMA in liver from immunofluorescent staining was increased in OLA group (P < 0.01). Compared with OLA group, the expression of E-cadherin in liver from immunofluorescent staining was increased in DAP group (P < 0.01), on the other hand the expression of α-SMA in liver from immunofluorescent staining was reduced in DAP group (P < 0.05). These results suggested that dapagliflozin reversed GLUT5/AMPK/mTOR to improve liver injury.
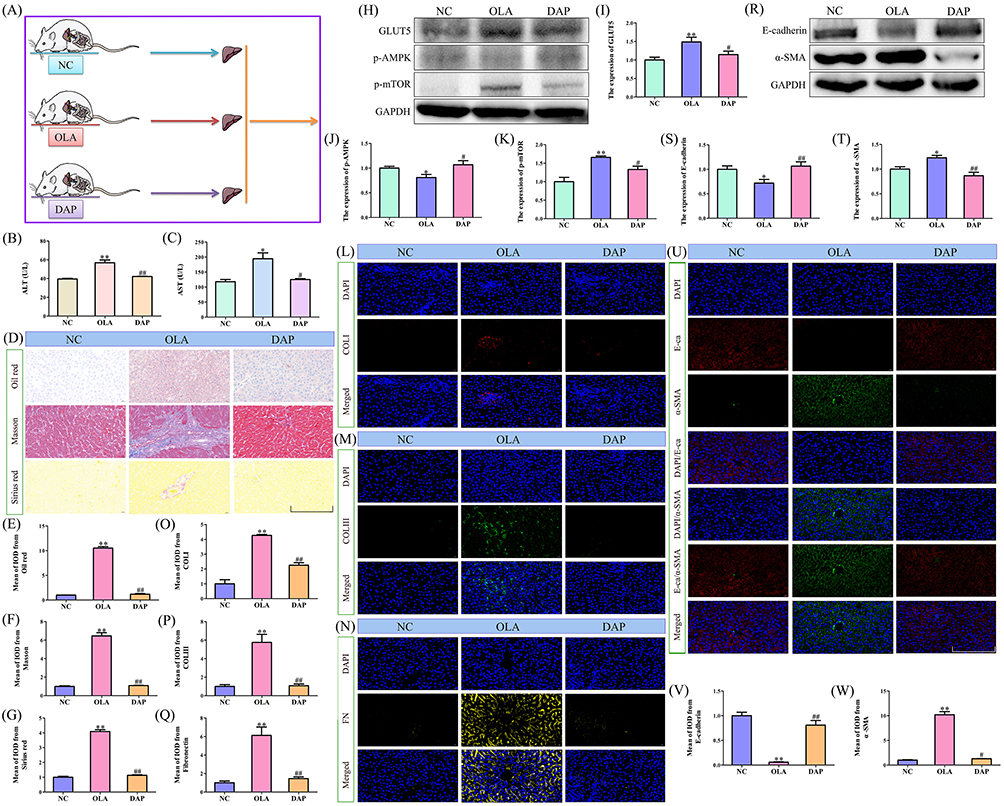 |
Figure 6 Dapagliflozin reversed GLUT5/AMPK/mTOR to improve liver injury. (A) Flow chart. (B) ALT. (C) AST. (D) Oil red staining, masson staining, sirius red staining of liver. (E) Corresponding statistical analysis of oil red staining in liver. (F) Corresponding statistical analysis of masson staining in liver. (G) Corresponding statistical analysis of sirius red staining in liver. (H) Western blotting of GLUT5, p-AMPK, p-mTOR in liver. (I) Corresponding statistical analysis of GLUT5 from Western blotting in liver. (J) Corresponding statistical analysis of p-AMPK from Western blotting in liver. (K) Corresponding statistical analysis of p-mTOR from Western blotting in liver. (L) Immunofluorescent staining of COLI in liver. (M) Immunofluorescent staining of COLIII in liver. (N) Immunofluorescent staining of fibronectin in liver. (O) Corresponding statistical analysis of COLI from immunofluorescent staining in liver. (P) Corresponding statistical analysis of COLIII from immunofluorescent staining in liver. (Q) Corresponding statistical analysis of fibronectin from immunofluorescent staining in liver. (R) Western blotting of E-cadherin/α-SMA in liver. (S) Corresponding statistical analysis of E-cadherin from Western blotting in liver. (T) Corresponding statistical analysis of α-SMA from Western blotting in liver. (U) Immunofluorescent staining of E-cadherin/α-SMA in liver. (V) Corresponding statistical analysis of E-cadherin from immunofluorescent staining in liver. (W) Corresponding statistical analysis of α-SMA from immunofluorescent staining in liver. *P < 0.05, **P < 0.01 vs NC. #P < 0.05, ##P < 0.01 vs OLA. Scale bar was 200 µm. Abbreviations: NC, control group; OLA, olanzapine group; DAP, dapagliflozin intervention group; FN, fibronectin; E-ca, E-cadherin. |
Mechanism Diagram of Olanzapine Activated GLUT5/AMPK/mTOR Driving Gut-Liver Axis Injury and Dapagliflozin Intervention
Olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury. Dapagliflozin reversed GLUT5/AMPK/mTOR, and ameliorated the gut-liver axis injury to improve NAFLD, which was shown in Figure 7.
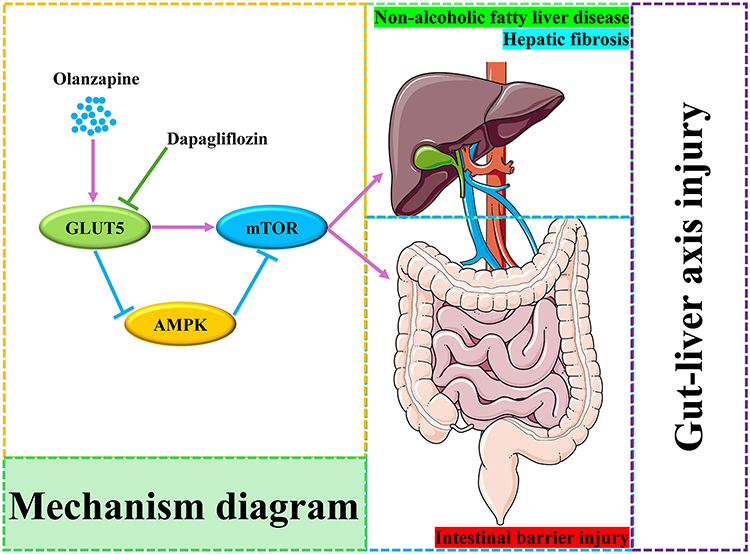 |
Figure 7 Mechanism diagram of olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury and dapagliflozin intervention. |
Discussion
NAFLD refers to a type of metabolic stress-induced liver injury characterized by diffuse fatty changes in liver cells, provided that long-term excessive alcohol consumption, hepatitis B virus infection, etc. are excluded. NAFLD is the main cause of chronic liver diseases and liver transplantation worldwide, seriously endangering human life and health safety, and also imposing a huge economic burden on public healthcare and social security.45,46 The progression of NAFLD is related to various factors such as obesity, insulin resistance, genetics, metabolic stress, systemic chronic low-grade inflammation, intestinal flora disorder, and unreasonable dietary structure.47,48
The gut-liver axis is a highly generalized term for the bidirectional relationship between the gut and its microbiota and the liver. On one hand, the liver and the gut both develop from the anterior hindgut of the endoderm and share the same embryonic origin.49 On the other hand, the metabolic products of the liver and intestinal flora interact through the bile duct and portal vein, influencing the physiological metabolic functions of the body.50 The liver and the intestine also have complex interactions in terms of immunity, metabolism and endocrinology. The intestinal barrier is composed of four layers: biological, mechanical, chemical and immune barriers.
Normal gut-liver axis function requires the support of the intestinal mucosal barrier. Among them, occludin, claudins, and zonula occludens (ZOs) are the main proteins that constitute the intestinal tight junctions. They form the structural basis of intestinal barrier function at the top of the apical surface of the intestinal epithelial cells. The intestinal tight junction proteins are an important component of intestinal barrier function. Under the influence of intestinal-related diseases and drug toxicity and other damaging factors, the integrity of intestinal tight junction proteins is impaired, which in turn leads to intestinal barrier dysfunction and promotes the entry of harmful metabolites into the gut-liver axis circulation.
At present, many studies have found that the injury of the gut-liver axis is closely related to NAFLD. Intervening in the injury of the gut-liver axis can improve NAFLD. Ma et al reported H. rhamnoides L. seed oil effectively mitigated NAFLD by reducing hepatic lipid expression via regulating intestinal microbiota, its SCFA secretion and intestinal barrier.51 Xu et al reported qushi huayu decoction alleviated NAFLD in mice by regulating gut microbiota homeostasis in the gut-liver axis via the pregnane X receptor.52 Yang et al reported ginsenoside Rh4 improved hepatic lipid metabolism and inflammation in a model of NAFLD by targeting the gut-liver axis and modulating the FXR signaling pathway.53 Xiao et al reported tetrastigma hemsleyanum leaf extracts ameliorated NAFLD in mice with low-grade colitis via the gut-liver axis.54 Wang et al reported akebia trifoliata extracts attenuated liver injury via gut-liver axis in a murine model of NAFLD with low-grade colitis.55 Luo et al reported BefA protein alleviated progression of NAFLD by modulating the AMPK signaling pathway through the gut-liver axis.56 Sun et al reported bacteroides ovatus alleviated high-fat and high-cholesterol-induced NAFLD via gut-liver axis.57 Xu et al reported zhuyu pill alleviated NAFLD by regulating bile acid metabolism through the gut-liver axis.58 Kuang et al reported hyodeoxycholic acid alleviated NAFLD through modulating the gut-liver axis.59 Therefore, the gut-liver axis is a key link in the development of NAFLD, and at the same time, it is also a crucial factor for its treatment.
Olanzapine’s prolonged use has been associated with an increased risk of NAFLD,8,9,11–14 however, the underlying mechanism remains unclear. In this study, we focused on the injury of the gut-liver axis induced by olanzapine in rats with NAFLD. Firstly, we found that olanzapine caused intestinal barrier injury and NAFLD and hepatic fibrosis. The transcriptome studies of the intestine and liver further revealed the high expression of GLUT5 in both tissues. GLUT5, as a fructose transporter, plays a significant role in the occurrence and development of various diseases. Studies have shown that GLUT5 regulates fructose metabolism in human bile duct cancer cells, and its overexpression is associated with the progression of bile duct cancer; while GLUT5 is highly expressed in breast cancer, and its expression is not found in normal breast tissue; at the same time, in the case of glucose deficiency, GLUT5-mediated fructose uptake and utilization contribute to the progression of pancreatic cancer, and the fructose-regulated AMPK-mTOR signaling pathway inhibits autophagy-induced cell death, making pancreatic cancer cells more conducive to growth and progression; in lung cancer, GLUT5 is highly expressed in tumor tissues of lung cancer metastasis patients, and promotes the malignant growth of lung cancer cells through the AMPK-mTOR signaling pathway.60,61 In summary, GLUT5 is highly expressed in various diseases and further regulates the AMPK-mTOR signaling pathway to induce disease progression.
Furthermore, we found that in olanzapine-induced rat NAFLD models, olanzapine activated GLUT5/AMPK/mTOR driving gut-liver axis injury. It was mainly manifested in the intestinal aspect by down-regulating intestinal tight junction proteins occludin, claudin-1 and ZO-1, and in the liver aspect by inducing fat accumulation and liver fibrosis. After dapagliflozin intervention, the expression of GLUT5/AMPK/mTOR in the intestine was reversed, and the expression of intestinal barrier proteins increased, thereby improving intestinal barrier injury. In the liver, dapagliflozin reversed the expression of GLUT5/AMPK/mTOR in the liver, improving NAFLD and hepatic fibrosis.
Of course, this study had certain limitations. This study lacked some parameters related to overall metabolism. This would be further explored in our future in-depth research on the mechanism and clinical studies.
Conclusion
In this study, we discovered for the first time that GLUT5/AMPK/mTOR was associated with gut-liver axis injury mediating olanzapine-induced NAFLD and dapagliflozin intervention could reverse GLUT5/AMPK/mTOR-driven gut-liver axis injury ameliorating olanzapine-induced NAFLD. This provides a new understanding of the occurrence of olanzapine-induced NAFLD and offers a reference plan for its clinical intervention.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Dong-Dong Wang) on reasonable request.
Funding
This work was supported by The Basic Science (Natural Science) Project of Higher Education Institutions in Jiangsu Province (No. 25KJD310004), The Natural Science Foundation of Jiangsu Province (No. BK20241046), The Science and Technology Program of Xuzhou (No. KC25105), The Medical Research Project of Jiangsu Provincial Health Commission (No. Z2023010), The Suzhou Applied Basic Research Science and Technology Innovation Project (No. SYWD2024258).
Disclosure
Xiao Chen, Yue Zhang, and Jie Wang are co-first authors. The authors report no conflicts of interest.
References
1. Ciarolla A, Bobilev AM, Dybowski F, et al. The hippocampal-cortical system cerebral blood flow in schizophrenia: primary disease versus antipsychotic medication effects. Schizophr Res. 2025;287:3–15. doi:10.1016/j.schres.2025.11.003
2. Park JS, Kim S, Jeong D, et al. Dementia in older adults with schizophrenia: a 12-year analysis of prevalence, incidence, and treatment patterns in South Korea. Schizophrenia. 2025;11(1):134. doi:10.1038/s41537-025-00680-4
3. Qin X, Hou W, Mao Z, et al. Peripheral NMDAR subunits as predictors of working memory improvement in schizophrenia. Schizophrenia. 2025;11(1):133. doi:10.1038/s41537-025-00679-x
4. Smyrnis A, Smyrnis G, Smyrnis N. Add-on pharmacotherapy in Schizophrenia: does it improve long-term outcomes? A systematic review. J Clin Med. 2025;14(21):7847. doi:10.3390/jcm14217847
5. Xie Y, Ouyang A, Zhang T, et al. Mapping the landscape of fMRI research in schizophrenia: a bibliometric and meta-analytic study. Asian J Psychiatr. 2025;114:104768. doi:10.1016/j.ajp.2025.104768
6. Schulze AT, Schurr T, Post F, et al. Subjective well-being in early-phase schizophrenia patients using long-acting injectable versus oral antipsychotic drugs: data from the European Long-acting Antipsychotics in Schizophrenia Trial (EULAST). Eur Psychiatry. 2025;68(1):e116. doi:10.1192/j.eurpsy.2025.10086
7. Zhao G, Sun Y, Zhang Y, et al. Efficacy and tolerability of seven antipsychotic drugs in acutely ill patients with schizophrenia: a randomized, multicenter, assessor-blinded trial. Am J Psychiatry. 2025:appiajp20250111.
8. Ebrahimian Z, Razavi BM, Mousavi Shaegh SA, Hosseinzadeh H. Exploring the therapeutic potential of chlorogenic acid in alleviating olanzapine-induced metabolic syndrome in rats: a key role of hypothalamic satiety proteins. Nutr Neurosci. 2025;28(9):1055–1074. doi:10.1080/1028415X.2025.2460385
9. Huang P, Ran J, Zhu W, et al. PCSK9 dysregulates cholesterol homeostasis and triglyceride metabolism in olanzapine-induced hepatic steatosis via both receptor-dependent and receptor-independent pathways. FASEB J. 2024;38(4):e23464. doi:10.1096/fj.202301748R
10. Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939–951. doi:10.1016/S0140-6736(19)31135-3
11. Li R, Zhu W, Huang P, et al. Olanzapine causes non-alcoholic fatty liver disease via inhibiting the secretion of apolipoprotein A5. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022;47(6):730–738. doi:10.11817/j.issn.1672-7347.2022.210269
12. Li R, Zhu W, Huang P, et al. Olanzapine leads to nonalcoholic fatty liver disease through the apolipoprotein A5 pathway. Biomed Pharmacother. 2021;141:111803. doi:10.1016/j.biopha.2021.111803
13. Zhu W, Ding C, Huang P, et al. Metformin Ameliorates Hepatic Steatosis induced by olanzapine through inhibiting LXRalpha/PCSK9 pathway. Sci Rep. 2022;12(1):5639. doi:10.1038/s41598-022-09610-1
14. Zhu Z, Cao T, Chen H, Zhang B, Lin C, Cai H. Olanzapine-induced nonalcoholic fatty liver disease: the effects of differential food pattern and the involvement of PGRMC1 signaling. Food Chem Toxicol. 2023;176:113757. doi:10.1016/j.fct.2023.113757
15. Ghaseminejad-Raeini A, Yaseri M, Younesian M, et al. The impact of air pollution on non-alcoholic fatty liver disease: a global ecological analysis of incidence and mortality trends by human development index (1990–2019). J Diabetes Metab Disord. 2025;24(2):242. doi:10.1007/s40200-025-01751-0
16. Alhabahbeh RH, Obeidat AN, Jaber DS, et al. Screening for the prevalence of Nonalcoholic Fatty Liver Disease (NAFLD) among patients with prediabetes and type 2 diabetes: a comparison of three screening systems. Int J Endocrinol. 2025;2025:6676114. doi:10.1155/ije/6676114
17. Arellano-Garcia LI, Portillo MP, Martinez JA, Courtois A, Milton-Laskibar I. Postbiotics for the management of obesity, insulin resistance/type 2 diabetes and NAFLD. Beyond microbial viability. Crit Rev Food Sci Nutr. 2025;65(29):6209–6232. doi:10.1080/10408398.2024.2437143
18. Chen K, Zhong C, Zhou L, et al. Randomized controlled trial of effects of metformin in NAFLD patients with newly diagnosed type 2 diabetes treated with an intensive lifestyle: a study protocol. Trials. 2025;26(1):462. doi:10.1186/s13063-025-09191-0
19. Gong W, Lu X, Weng S. Jiangtang Decoction for Type 2 Diabetes and NAFLD: integrative Analysis via Network Pharmacology, Mendelian Randomization, Molecular Docking, and In Vitro Validation. Endocr Metab Immune Disord Drug Targets. 2025. doi:10.2174/0118715303424915250818045151
20. Hou C, Yuan X, Peng M, et al. The role of insulin resistance in the longitudinal progression from NAFLD to cardiovascular-kidney-metabolic disease. Cardiovasc Diabetol. 2025;24(1):398. doi:10.1186/s12933-025-02953-9
21. Ji B, Gao G, Zhao H, et al. The Log(e) GDR was strongly associated with NAFLD as a predictor in normoalbuminuric patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2025;18:115–124. doi:10.2147/DMSO.S500739
22. Khadija T, Rizwan Z, Joel P, et al. The effect of statin therapy on liver enzymes and fibrosis progression in patients with coexisting cardiovascular disease and Non-alcoholic Fatty Liver Disease (NAFLD). Cureus. 2025;17(8):e91301. doi:10.7759/cureus.91301
23. Nevola R, Costabile G, Della Pepa G. Editorial: NAFLD treatment in diabetes: from current dietary interventions to novel treatment. Front Endocrinol. 2025;16:1572770. doi:10.3389/fendo.2025.1572770
24. Petroni ML, Brodosi L, Bugianesi E, Marchesini G. Management of non-alcoholic fatty liver disease. BMJ. 2021;372:m4747. doi:10.1136/bmj.m4747
25. Teimouri A, Ebrahimpour Z, Feizi A, et al. Pre-diabetes and cardiovascular risk factors in NAFLD patients: a retrospective comparative analysis. Front Endocrinol. 2025;16:1416407. doi:10.3389/fendo.2025.1416407
26. Varra FN, Varras M, Varra VK, Theodosis-Nobelos P. Mechanisms linking obesity with Non-Alcoholic Fatty Liver Disease (NAFLD) and Cardiovascular Diseases (CVDs)-the role of oxidative stress. Curr Issues Mol Biol. 2025;47(9). doi:10.3390/cimb47090766
27. Bai X, Wang Z, Guo K, Zhou P, Shi L. Gut-liver axis dysregulation and microbial dysbiosis in invasive liver abscess: a narrative review. Front Immunol. 2025;16:1646893. doi:10.3389/fimmu.2025.1646893
28. Chen Z, Liao S, Wu S, et al. The gut‒liver axis in liver disease: molecular mechanisms and therapeutic targets. MedComm. 2025;6(11):e70458. doi:10.1002/mco2.70458
29. Ramos-da-Silva LA, Souza-Tavares H, Medeiros GR, et al. Gut-liver axis: an emerging target for exercise in obesity management. Clin Res Hepatol Gastroenterol. 2025;49(9):102687. doi:10.1016/j.clinre.2025.102687
30. Xing Y, Ou Y, Wang Y, Hou L, Zhu J. New insights into gut-liver axis in advanced liver diseases: a promising therapeutic target. Biochem Pharmacol. 2025;242(Pt 2):117284. doi:10.1016/j.bcp.2025.117284
31. Kobayashi T, Iwaki M, Nakajima A, Nogami A, Yoneda M. Current research on the pathogenesis of NAFLD/NASH and the gut-liver axis: gut microbiota, dysbiosis, and leaky-gut syndrome. Int J Mol Sci. 2022;23(19):11689. doi:10.3390/ijms231911689
32. Paolella G, Mandato C, Pierri L, Poeta M, Di Stasi M, Vajro P. Gut-liver axis and probiotics: their role in non-alcoholic fatty liver disease. World J Gastroenterol. 2014;20(42):15518–15531. doi:10.3748/wjg.v20.i42.15518
33. Pezzino S, Sofia M, Faletra G, et al. Gut-Liver Axis and Non-Alcoholic Fatty Liver Disease: a Vicious Circle of Dysfunctions Orchestrated by the Gut Microbiome. Biology. 2022;11(11):1622. doi:10.3390/biology11111622
34. Zhou W, Shi W, Du X, et al. Assessment of nonalcoholic fatty liver disease symptoms and gut-liver axis status in Zebrafish after exposure to polystyrene microplastics and oxytetracycline, alone and in combination. Environ Health Perspect. 2023;131(4):47006. doi:10.1289/EHP11600
35. Baumann A, Rajcic D, Brandt A, et al. Alterations of nitric oxide homeostasis as trigger of intestinal barrier dysfunction in non-alcoholic fatty liver disease. J Cell Mol Med. 2022;26(4):1206–1218. doi:10.1111/jcmm.17175
36. Forlano R, Mullish BH, Roberts LA, Thursz MR, Manousou P. The intestinal barrier and its dysfunction in patients with metabolic diseases and non-alcoholic fatty liver disease. Int J Mol Sci. 2022;23(2):662. doi:10.3390/ijms23020662
37. Mohamad Nor MH, Ayob N, Mokhtar NM, et al. The effect of probiotics (MCP((R)) BCMC((R)) Strains) on hepatic steatosis, small intestinal mucosal immune function, and intestinal barrier in patients with non-alcoholic fatty liver disease. Nutrients. 2021;13(9):3192. doi:10.3390/nu13093192
38. Nian F, Chen Y, Xia Q, Zhu C, Wu L, Lu X. Gut microbiota metabolite trimethylamine N-oxide promoted NAFLD progression by exacerbating intestinal barrier disruption and intrahepatic cellular imbalance. Int Immunopharmacol. 2024;142(Pt B):113173. doi:10.1016/j.intimp.2024.113173
39. Wang H, Guo Y, Han W, et al. Tauroursodeoxycholic acid improves nonalcoholic fatty liver disease by regulating gut microbiota and bile acid metabolism. J Agric Food Chem. 2024;72(36):20194–20210. doi:10.1021/acs.jafc.4c04630
40. Wang DD, Zhang C, Yang Y, He SM, Zhu P, Chen X. Effects of sodium-glucose cotransporter-2 inhibitors on urine albumin to creatinine ratio in type 2 diabetes mellitus patients and medication care. J Diabetes Res. 2022;2022:5854200. doi:10.1155/2022/5854200
41. Wang DD, He SM, Han Y, Wang TY, Wang YM. Quantifying the relationship between dapagliflozin and loss of weight in type 1 diabetes mellitus patients. J Clin Pharm Ther. 2022;47(2):237–242. doi:10.1111/jcpt.13572
42. Wang DD, Zhang C, Zhu P, He SM, Chen X. Quantitative effects of sodium-glucose cotransporter-2 inhibitors dapagliflozin and empagliflozin on quality of life in heart failure patients. Front Pharmacol. 2022;13:910858. doi:10.3389/fphar.2022.910858
43. Chen X, Xu C, Hu K, et al. Quantitative effects of sodium-glucose cotransporter-2 inhibitors on liver functions in patients with nonalcoholic fatty liver disease. Expert Rev Clin Pharmacol. 2023;16(10):991–998. doi:10.1080/17512433.2023.2256224
44. Wang DD, Zhang C, Hu K, He SM, Zhu P, Chen X. Therapeutic effect and rebound evaluation of dapagliflozin on glycated hemoglobin (HbA1c) in type 1 diabetes mellitus patients. Front Pharmacol. 2022;13:972878. doi:10.3389/fphar.2022.972878
45. Ferguson D, Finck BN. Emerging therapeutic approaches for the treatment of NAFLD and type 2 diabetes mellitus. Nat Rev Endocrinol. 2021;17(8):484–495. doi:10.1038/s41574-021-00507-z
46. Rinella ME. Nonalcoholic fatty liver disease: a systematic review. JAMA. 2015;313(22):2263–2273. doi:10.1001/jama.2015.5370
47. Makri E, Goulas A, Polyzos SA. Epidemiology, pathogenesis, diagnosis and emerging treatment of nonalcoholic fatty liver disease. Arch Med Res. 2021;52(1):25–37. doi:10.1016/j.arcmed.2020.11.010
48. Tilg H, Adolph TE, Moschen AR. Multiple parallel hits hypothesis in nonalcoholic fatty liver disease: revisited after a decade. Hepatology. 2021;73(2):833–842. doi:10.1002/hep.31518
49. Li LC, Wang X, Xu ZR, et al. Single-cell patterning and axis characterization in the murine and human definitive endoderm. Cell Res. 2021;31(3):326–344. doi:10.1038/s41422-020-00426-0
50. Tilg H, Adolph TE, Trauner M. Gut-liver axis: pathophysiological concepts and clinical implications. Cell Metab. 2022;34(11):1700–1718. doi:10.1016/j.cmet.2022.09.017
51. Ma J, Li Y, Yang Y, et al. Gut-liver axis mechanisms of Hippophae rhamnoides L. in non-alcoholic fatty liver disease prevention. Phytomedicine. 2025;149:157517. doi:10.1016/j.phymed.2025.157517
52. Xu Y, Ni Y, Zhou M, Gou X. Qushi Huayu decoction alleviates NAFLD in mice by regulating gut microbiota homeostasis in the gut-liver axis via the pregnane X receptor. Eur J Pharmacol. 2025;1008:178366. doi:10.1016/j.ejphar.2025.178366
53. Yang S, Duan Z, Zhang S, et al. Ginsenoside Rh4 improves hepatic lipid metabolism and inflammation in a model of NAFLD by targeting the gut liver axis and modulating the FXR signaling pathway. Foods. 2023;12(13).
54. Xiao L, Xiong H, Deng Z, et al. Tetrastigma hemsleyanum leaf extracts ameliorate NAFLD in mice with low-grade colitis via the gut-liver axis. Food Funct. 2023;14(1):500–515. doi:10.1039/D2FO03028D
55. Wang X, Chen H, Zhu W, et al. Akebia trifoliata extracts attenuate liver injury via gut-liver axis in a murine model of nonalcoholic fatty liver disease with low-grade colitis. Food Res Int. 2025;208:116202. doi:10.1016/j.foodres.2025.116202
56. Luo J, Cai Y, Jia C, et al. BefA protein alleviates progression of non-alcoholic fatty liver disease by modulating the AMPK signaling pathway through the gut-liver axis. Int J Biol Macromol. 2025;294:139446. doi:10.1016/j.ijbiomac.2024.139446
57. Sun C, Xiong X, Liu M, et al. Bacteroides ovatus alleviates high-fat and high-cholesterol -induced nonalcoholic fatty liver disease via gut-liver axis. Biomed Pharmacother. 2024;178:117156. doi:10.1016/j.biopha.2024.117156
58. Xu L, Xu K, Xiong P, et al. Zhuyu pill alleviates nonalcoholic fatty liver disease by regulating bile acid metabolism through the gut-liver axis. ACS Omega. 2023;8(32):29033–29045. doi:10.1021/acsomega.3c01955
59. Kuang J, Wang J, Li Y, et al. Hyodeoxycholic acid alleviates non-alcoholic fatty liver disease through modulating the gut-liver axis. Cell Metab. 2023;35(10):1752–66e8. doi:10.1016/j.cmet.2023.07.011
60. Chen WL, Jin X, Wang M, et al. GLUT5-mediated fructose utilization drives lung cancer growth by stimulating fatty acid synthesis and AMPK/mTORC1 signaling. JCI Insight. 2020;5(3):e131596. doi:10.1172/jci.insight.131596
61. Hadzi-Petrushev N, Stojchevski R, Jakimovska A, et al. GLUT5-overexpression-related tumorigenic implications. Mol Med. 2024;30(1):114. doi:10.1186/s10020-024-00879-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.