Back to Journals » International Medical Case Reports Journal » Volume 17
Glucocorticoid-Induced Side Effects Cause Oral Lesions in Systemic Lupus Erythematosus: A Case Report
Authors Pranadwista ZF ![]() , Hasanah NT
, Hasanah NT ![]() , Dewi TS
, Dewi TS ![]() , Hidayat W
, Hidayat W ![]()
Received 13 August 2024
Accepted for publication 21 October 2024
Published 4 November 2024 Volume 2024:17 Pages 919—926
DOI https://doi.org/10.2147/IMCRJ.S491296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Zulfa Fidi Pranadwista,1 Novia Tri Hasanah,1 Tenny Setiani Dewi,2 Wahyu Hidayat2
1Oral Medicine Residency Program, Faculty of Dentistry, Padjadjaran University, Bandung, Indonesia; 2Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University, Bandung, Indonesia
Correspondence: Zulfa Fidi Pranadwista, Padjadjaran University, Jalan Sekeloa Selatan, No. I, Lebakgede, Bandung, West Java, 40132, Indonesia, Tel +62 8971557962, Fax +62 22 7794121, Email [email protected]
Background: Systemic Lupus Erythematosus (SLE) is a complex autoimmune disease with various complications, making its management difficult. Glucocorticoid not only plays an essential role in the pathogenic therapy of SLE but also causes side effects such as oral lesions, especially when administered long-term or at high doses.
Purpose: This case report aims to describe the management of glucocorticoid-induced side effects that cause oral lesions in SLE patient.
Case Presentation: A 30-year-old woman complained of a sore mouth and mouth-opening difficulty ten days prior. Previously, the patient complained of swelling in the legs and stomach, joint pain, hair loss, and skin redness on exposure to sunlight. Extra-oral examination revealed multiple red-black erosions and crusts on the zygoma region bilaterally over the nasal bridge, well-demarcated with an irregular shape, while the lips bled easily with hemorrhagic crusts that developed into serosanguineous crusts. Intra-oral examination showed scrapable white plaques on the palate, leaving erythematous areas, pain, and ulcers throughout the oral mucosa. The antinuclear antibody (ANA) examination revealed reactive results, positive anti-HSV-1 IgG, and positive hyphal on KOH examination. Based on the examination results, the diagnosis was SLE with herpes virus-associated oral involvement and acute pseudomembranous candidiasis.
Case Management: Comprehensive therapy, including non-pharmacological and pharmacological therapy, was involved. All oral lesions improved within one month.
Conclusion: Various oral lesions may appear as manifestations of the disease and side effects of glucocorticoid therapy in SLE patients, thus requiring multidisciplinary monitoring and therapy from various fields.
Keywords: autoimmune disease, glucocorticoid, oral lesions, oral infections, systemic lupus erythematosus
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune disease characterized by inflammation and organ damage.1 The incidence and prevalence of SLE vary widely depending on population demographics, socioeconomic factors, and specific ethnic populations. The estimated global incidence of SLE for the overall population is 5.14 per 100.000 individuals, and the annual population of newly diagnosed individuals is 0.40 million. Although SLE varies across all age groups, the disease is more common between 15 and 45 years of age. Gender disparity in SLE is also widely recognized, with a male-to-female patient ratio of 1:9.2,3 SLE can be a serious condition and often requires prolonged intensive immunosuppressive therapy, but most guidelines refer to the “standard care” of a combination of hydroxychloroquine and glucocorticoids.1
Remission and preventing organ damage are the aims of SLE management. An essential part of managing SLE is providing emotional support, physical and lifestyle assessments, and patient education. Patients with SLE are entitled to comprehensive education regarding the disease, its possible organ involvement, and the importance of drug adherence and monitoring.4 Glucocorticoids play an essential role in SLE therapy but also cause a series of side effects, especially for short- and long-term administration.5 Glucocorticoids have the potential to impact both innate and adaptive immunity, elevate the risk of disease, reactivate chronic infections, and affect recommendations on vaccination requirements.6 The prevalence of mucosal involvement occurs in approximately 9–45% of cases and is accompanied by systemic forms of disease. More than 40% of patients suffering from this condition have ulceration of the oral mucosa.7
Various oral lesions related to viral, bacterial, fungal, and other pathogen infections may increase as a consequence of glucocorticoid administration, also increasing mortality and morbidity in SLE patients.6 Infections caused by herpes simplex virus type 1 (HSV-1) should be considered in patients with SLE who exhibit atypical symptoms.8 Also, fungal infections such as candidiasis may occur and are the third most common in SLE patients after bacterial and viral infections. Although infection in the oral cavity is not life-threatening, it has been demonstrated that it is the primary site of spread-resistant candida infections.9 Life-threatening circumstances may arise from improper or delayed treatment of various infectious diseases.8
Understanding the characteristic signs and symptoms of oral lesions supports early diagnosis and management, which improves the prognosis and patients’ quality of life. A thorough oral examination to record the oral lesion findings and its management is recommended in SLE patients, especially those with active disease, proteinuria, high white blood cell count, and glucocorticoid consumption or immunosuppressive agents.10,11 This report aims to describe the management of glucocorticoid-induced oral lesions in SLE patients.
Case Presentation
A 30-year-old female hospitalized patient was referred from the Internal Medicine clinic with chief complaints of multiple oral ulcers, a sore palate, and difficulty opening her mouth ten days prior. Initially, the ulcers appeared on the buccal mucosa and palate, progressing rapidly throughout the oral cavity. Doctors from the hospital beforehand have prescribed medication to relieve the pain complaints, but there has been no improvement. Since being hospitalized, the patient has had difficulty cleaning her mouth and can only consume milk through a straw. The patient has a habit of peeling off the scabs on the lips.
The patient experienced a body fever three days before being hospitalized. There were no complaints of coughing, runny noses, or altered taste. The patient has also complained of swollen legs and abdomen, pain in all joints, hair loss, and reddish skin once exposed to sunlight three months prior. Following a previous hospital diagnosis of nephrotic syndrome, the patient was prescribed furosemide 80 mg, albumin, and methylprednisolone 32 mg. The patient stopped the drugs after taking them for two weeks without consulting a doctor because she felt her condition was improving.
Extra-oral examination at the first visit showed multiple hemorrhagic crusts and erosions in the bilateral frontal and zygoma regions passed through the bridge of the nose, an irregular shape with distinct borders, and hemorrhagic crusts on the upper and lower lips that bleed easily. Intra-oral examination revealed erythema throughout oral mucosa and multiple irregular white plaques with diffuse borders that vary in size, which can be partially scraped off to reveal patches of erythema on the palate (Figure 1). Based on the history and clinical findings, the suspected diagnosis in the first visit was oral lesions associated with SLE and acute pseudomembranous candidiasis, with the differential diagnoses were pemphigus vulgaris (PV), erythema major and Steven Johnson syndrome (SJS).
 |
Figure 1 Clinical features in the first visit. Crusts on the frontal region, bilateral zygoma, and nasal bridge (A); hemorrhagic crusts on the lips (B); ulcers and erythema on the buccal mucosa (C and D); and white plaques on the palate (E). |
The internal medicine specialist made a provisional diagnosis of suspected SLE with mucocutaneous, musculoskeletal, renal, and serositis involvement. Suspected chronic cutaneous lupus erythematosus (CCLE) and suspected toxic epidermal necrolysis-like acute cutaneous lupus erythematosus (TEN-like ACLE) were established as differential diagnoses. An antinuclear-antibodies (ANA) test was performed in the second visit (third day) and showed reactive results with a homogeneous pattern (titer 1:3200). Complete blood cell count and other parameters in laboratory examination were performed to assess the patient’s general health status (Table 1).
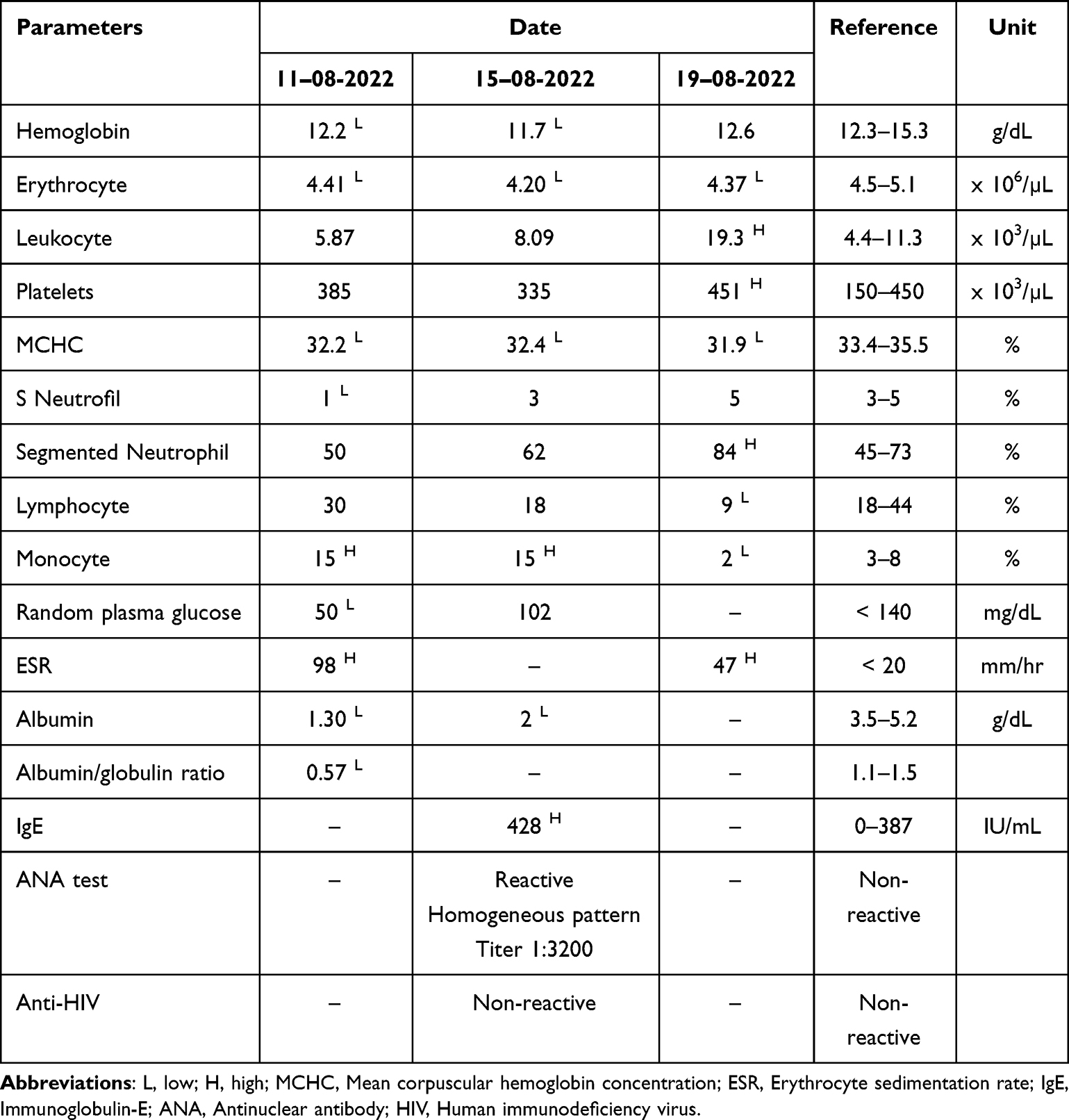 |
Table 1 Results of the Laboratory Examination |
Disease activity assessment was performed using the Mexican-Systemic Lupus Erythematosus Disease Activity Index (Mex-SLEDAI) and revealed a score of 7. Based on these examination results, the internal medicine specialist diagnosed SLE, and the oral medicine specialist diagnosed lupus cheilitis and palatal erythematous ulcer. Evaluation from the oral medicine department at the second visit showed no improvement in the oral lesions.
The patient complained of increasing crusts on her lips at her follow-up on the third visit (sixth day), while the pain in the oral cavity remained. Extra-oral examination reveals an improvement in the crust of the frontal region, bilateral zygomas, and nose bridge, but the hemorrhagic crust on the lips develops into the serosanguinolenta crust. Intra-oral examination showed multiple ulcers surrounded by diffusely bounded erythema areas on the buccal mucosa and palate (Figure 2). An anti-HSV-1 IgG examination was carried out, and positive results were obtained at a ratio of 1.57 times. Diagnosis of lupus cheilitis associated with HSV-1 infection, oral discoid lupus erythematosus (DLE), and palatal erythematous ulcer was established.
 |
Figure 2 Clinical features on the sixth day. Improvement of crusts on the frontal region, bilateral zygoma, and nasal bridge (A); hemorrhagic crust developed into serosanguinolenta crusts (B); ulcers on the buccal mucosa (C and D) and palate (E). |
The patient felt that the complaints in the oral cavity had begun to improve on the fourth visit (thirteenth day), but there was still a slight stinging sensation on the lips, buccal mucosa, and palate. Extra-oral examination showed that the crusts on the lips had improved but still bled easily. Intra-oral examination revealed improvement, as indicated by a decrease in lesion size (Figure 3).
 |
Figure 3 Clinical presentation on the thirteenth day, the lesions started to improve (A-E). |
On the fifth visit (40th day), the patient no longer felt sore in the oral cavity, and all lesions had disappeared (Figure 4). The patient has been able to eat normally for the last 10 days, following a three-meal-A-day diet accompanied by routine consumption of vegetables and fruits. The patient was instructed to continue maintaining oral hygiene.
 |
Figure 4 Clinical presentation on the fortieth day, all lesions disappeared (A-E). |
Case Management
Comprehensive management, including pharmacological and non-pharmacological therapy, was given to the patient with a multidisciplinary approach from various fields, such as internal medicine, dermatology venereology, and oral medicine. Figure 5 presents a chart summarizing the therapeutic flow from multiple departments, including pharmacologic and non-pharmacologic therapies.
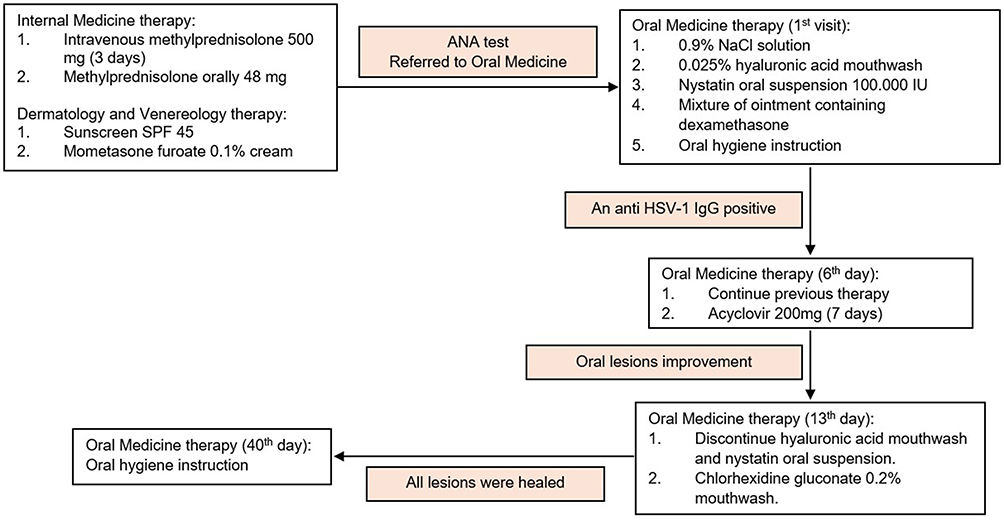 |
Figure 5 Case management chart. |
Pharmacological therapy from internal medicine was methylprednisolone 500 mg intravenously administered for three days and continued orally at a dose of 48 mg per day, while dermatology and venereology prescribed SPF 45 sunscreen and mometasone furoate 0.1% cream. These drugs were continued alongside therapy from the oral medicine clinic, such as 0.9% NaCl solution, 0.025% hyaluronic acid mouthwash, nystatin oral suspension 100.000 IU/mL, and a mixture of ointments containing dexamethasone. Acyclovir 200 mg as an antiviral agent was added on the sixth day after the anti-HSV-1 IgG test showed a positive result. Chlorhexidine gluconate 0.2% mouthwash was given on the thirteenth day to replace hyaluronic acid mouthwash, and nystatin oral suspension was stopped.
Non-pharmacological therapy includes instructions for applying moist gauze moistened with 0.9% NaCl solution to compress lips at least three times daily. Education is given to the patient to stop the habit of peeling scabs on the lips, encouraging a healthy lifestyle and adequate hydration at least two liters per day. All lesions healed within 40 days, and the patient was still educated on maintaining oral hygiene.
Discussion
SLE is a chronic autoimmune disease that can affect various organs and shows a diverse spectrum of clinical manifestations.12 The patient in this case showed symptoms such as swollen legs and abdomen, pain in all joints, hair loss, and reddish skin in exposure to sunlight three months before being diagnosed with SLE. SLE manifestations are associated with multiple autoantibodies, leading to the formation and deposition of immune complexes and other immune processes. Constitutional, mucocutaneous, and musculoskeletal signs are the earliest and most common complaints reported by most SLE patients.13
Immunosuppressive agents and glucocorticoids, frequently used in the early stages of SLE, aim to prevent or minimize major organ damage. Still, these drugs also have potential side effects such as infection.9 The risk of infection caused by systemic glucocorticoids related to the daily dose of therapy or duration of treatment is still unknown and debated; nonetheless, a meta-analysis revealed that the risk of infection was highest during the initial days or weeks of medication in contrast to more prolonged exposure.14
Glucocorticoid therapy leads to a decrease in the ability of neutrophils to adhere to the vascular endothelium and out of circulation, resulting in neutrophilia. Glucocorticoids also suppress dendritic cell maturation, which causes lymphopenia characterized by inhibiting T cell activation. Another critical effect of glucocorticoid therapy is the apoptosis of eosinophils. Altogether, these cellular and molecular effects increase the risk of bacterial, viral (especially herpes virus), and fungal (especially Candida species) infections as soon as the first dose of glucocorticoids is given and increases over time.6,15
Various organs, including the skin, hematologic system, kidney, neuropsychiatric, cardiovascular, and respiratory, may be affected by SLE. These manifestations may not all appear concomitantly, and there may be a gap of months or years between the appearance of various symptoms.13 More than 40% of patients suffering from this condition have ulceration of the oral mucosa. Oral lesions related to infection in patients with SLE can rapidly develop due to its disease or therapy-related immunosuppression.7 Abrupt discontinuation of exogenous steroids, as the patient did in the case three months before being admitted, can result in symptoms similar to adrenal insufficiency. Adrenal insufficiency conditions have an increased risk of infection due to altered innate cellular immunity characterized by significantly decreased cytotoxic natural killer (NK) cells.16
Immunosuppressive therapy in some diseases, such as autoimmune diseases, often leads to the reactivation of opportunistic agents and increases disease severity when the virus replicates. Viral reactivation of HSV-1, in this case, was demonstrated by the development of hemorrhagic crusts into serosanguinolenta on the lips after high-dose glucocorticoid therapy. An anti-HSV-1 IgG serology test revealed a positive result with a 1.57-fold ratio, so systemic antiviral drugs were added on the sixth day. Infections caused by herpes simplex virus type 1 (HSV-1), although rare, should be considered in patients with SLE who present with atypical symptoms.8
Indications for treatment with systemic antiviral drugs include healthy individuals experiencing conditions such as primary oral herpes simplex infection episodes; recurrent herpes labialis; severe, frequent, or persistent lesions; and/or recurrent gingivostomatitis depending on clinical judgment. The use of systemic antiviral drugs should be based on a thorough clinical assessment in immunocompromised individuals with primary or recurrent episodes of oral herpes simplex infection. Systemic therapy recommendations in the form of acyclovir 200 mg, five times a day can be given in conditions with moderate symptoms such as complaints of swallowing pain or clinical findings in the form of multiple lesions on the buccal or pharyngeal mucosa.17
Oral candidiasis is the most common opportunistic infection in the oral cavity, often known as the “disease of the diseased”. Management of oral candidiasis involves topical and systemic antifungal agents. The first-line treatment for non-invasive cases of oral candidiasis is topical antifungal agents such as nystatin, miconazole, amphotericin B, and clotrimazole. The World Health Organization (WHO) has recommended topical therapy with nystatin, either in suspension or pastilles form as it is considered to be a good substitute for orally administered fluconazole for treating oral and oropharyngeal candidiasis, even in patients with HIV-positive.18
Nystatin oral suspension 100.000 IU in this case was given as a topical antifungal because the patient had a history of nephrotic syndrome. Nystatin oral suspension 100.000 IU was administered four times a day, 2 mL each for 13 days. The duration of antifungal treatment plays an essential role in its efficacy. Nystatin administered at a concentration of 0.25 to 1 time with minimum inhibitory concentration value for half an hour was reported to produce a better antifungal effect for up to 6 hours on Candida isolates.18 Response to antifungal therapy was evidenced by the disappearance of white plaque lesions on the palate, so the administration of nystatin oral suspension was stopped, and chlorhexidine gluconate mouthwash was continued. Chlorhexidine gluconate is an antiseptic agent with antimicrobial effects against bacteria, fungi, and viruses that cause various diseases in the oral cavity.19
Various specific oral lesions as manifestations of SLE include palatal erythematous ulcer, oral discoid lupus erythematosus, honeycomb plaques, and verrucous lupus erythematous.7 Palatal erythematous ulcer and oral discoid lupus erythematosus were found in this case as specific oral lesions related to SLE, so symptomatic therapy was given in the form of 0.025% hyaluronic acid mouthwash, 0.9% NaCl solution, and dexamethasone-containing ointment for the lips.
Hyaluronic acid has advantages over topical steroids due to its safe use in all patients, including infants, pregnant women, and medically compromised patients. Hyaluronic acid plays an essential role in various biological processes, such as cell signaling, morphogenesis, wound healing, regulation of gene expression, and cell proliferation.20 The use of hyaluronic acid mouthwash by the patient showed a good response as indicated by improvement in ulcer lesions in the oral cavity after regular use.
NaCl 0.9% solution is an isotonic solution that is considered ideal as a wound cleanser because it does not interfere with the normal healing process, does not damage tissues or cause sensitization or allergies, and does not alter normal flora.21 Topical corticosteroids are available in several formulations, including ointments (petroleum-based), creams, lotions, gels, and solutions.22 The patient in this case was prescribed a mixture of ointment containing dexamethasone, lanoline, and petroleum jelly-based for the crusted lesions. Before applying the ointment, the patient was educated to compress the lips with a moist gauze soaked in 0.9% NaCl to clean the wound and prevent secondary infection so that the wound healing process can occur more quickly and effectively.
SLE therapy using glucocorticoids or immunosuppressive agents can be challenging for clinicians. Hence, the dose administration and dose adjustment, depending on the clinical-biological status of the patient reduces disease activity and minimizes side effects.5 Monitoring SLE patients avoids adverse manifestations of the disease by compromising the manifestations of SLE and the immunological status of the patient to the use of immunosuppressive agents. Decreasing SLE manifestations and enabling immunologic responses may reduce the risk of infection and further decrease the risk of mortality and morbidity.8
Conclusion
Oral lesions that occur in SLE patients may appear as the manifestations of its disease or the side effects of glucocorticoid therapy. The risk of infection after high-dose glucocorticoid administration is difficult to establish, but in those SLE patients treated with multiple immunosuppressive agents, an increased risk of infection may be present. Comprehensive management, including a multidisciplinary team approach, is required to maximize therapeutic outcomes, improve quality of life, and prevent morbidity and mortality.
Consent Statements
The patient has approved and written informed consent for the publication of this case report, including the images. The institution has also approved the publication of this article.
Acknowledgments
The authors would like to thank the patient who generously participated in this study, the staff of Dr. Hasan Sadikin Central General Hospital, and the Oral Medicine Department, Faculty of Dentistry, Padjadjaran University, for funding the publication.
Funding
Padjadjaran University funded this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Porta S, Danza A, Saavedra MA, et al. Glucocorticoids in systemic lupus erythematosus. Ten questions and some issues. J Clin Med. 2020;9(9):1–13. doi:10.3390/jcm9092709
2. Fatoye F, Gebrye T, Mbada C. Global and regional prevalence and incidence of systemic lupus erythematosus in low-and-middle income countries: a systematic review and meta-analysis. Rheumatol Int. 2022;42(12):2097–2107. doi:10.1007/s00296-022-05183-4
3. Tian J, Zhang D, Yao X, Huang Y, Lu Q. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheum Dis. 2023;82(3):351–356. doi:10.1136/ard-2022-223035
4. Justiz Vaillant AA, Goyal A, Varacallo M. Systemic Lupus Erythematosus. Treasure Island: StatPearls. 2023.
5. Popa R, Lautaru LA, Lucretiu R, et al. Therapy side effects in systemic lupus erythematosus. Curr Heal Sci J. 2018;44(3):316.
6. Caplan A, Fett N, Rosenbach M, Werth VP, Micheletti RG. Prevention and management of glucocorticoid-induced side effects: a comprehensive review: infectious complications and vaccination recommendations. J Am Acad Dermatol. 2017;76(2):191–198. doi:10.1016/j.jaad.2016.02.1240
7. Munthe EKM, Sufiawati I. Oral lesions as a clinical sign of systemic lupus erythematosus. Dent J. 2018;51(3):147–152. doi:10.20473/j.djmkg.v51.i3.p147-152
8. Reis AD, Mudinutti C, De Freitas Peigo M, et al. Erratum: active human herpesvirus infections in adults with systemic lupus erythematosus and correlation with the SLEDAI score. Adv Rheumatol. 2020;60(1):42. doi:10.1186/s42358-020-00144-6
9. Damara I, Winston K, Maulida F, Ariane A. factors associated with candidiasis in systemic lupus erythematosus patients in cipto mangunkusumo national general hospital: a single-center case-control study. Cureus. 2022;14(7).
10. Fangtham M, Magder LS, Petri MA. Oral candidiasis in systemic lupus erythematosus. Lupus. 2014;23(7):684–690. doi:10.1177/0961203314525247
11. García-Ríos P, Pecci-Lloret MP, Oñate-Sánchez RE. Oral manifestations of systemic lupus erythematosus: a systematic review. Int J Environ Res Public Health. 2022;19(11910):1–12. doi:10.3390/ijerph191911910
12. Esposito S, Bosis S, Semino M, Rigante D. Infections and systemic lupus erythematosus. In: Shoenfeld Y, Agmon-Levin N, Rose NR, editors. Infection and Autoimmunity.
13. Basta F, Fasola F, Triantafyllias K, Schwarting A. Systemic Lupus Erythematosus (SLE) therapy: the old and the new. Rheumatol Ther. 2020;7(3):433–446. doi:10.1007/s40744-020-00212-9
14. Fardet L, Petersen I, Nazareth I. Common infections in patients prescribed systemic glucocorticoids in primary care: a population-based cohort study. PLoS Med. 2016;13(5):1–20. doi:10.1371/journal.pmed.1002024
15. Noetzlin S, Breville G, Seebach JD, Gastaldi G. Short-term glucocorticoid-related side effects and adverse reactions: a narrative review and practical approach. Swiss Med Wkly. 2022;152(1–2):1–10. doi:10.4414/SMW.2022.w30088
16. Wahab F, Rahman RA, Yaacob LH, Noor NM, Draman N. A case report of steroid withdrawal syndrome. Korean J Family Med Korea. 2020;41(5):359–362. doi:10.4082/kjfm.18.0181
17. Vaghela D, Davies E, Murray G, Convery C, Walker L. Guideline for the management herpes simplex 1 and cosmetic interventions. J Clin Aesthet Dermatol. 2021;14(6 Suppl 1):S11–4.
18. Rai A, Misra SR, Panda S, et al. Nystatin effectiveness in oral candidiasis treatment: a systematic review & meta-analysis of clinical trials. Life. 2022;12(11):1677. doi:10.3390/life12111677
19. Brookes ZLS, Bescos R, Belfield LA, Ali K, Roberts A. Current uses of chlorhexidine for management of oral disease: a narrative review. J Dent. 2020;103:103497. doi:10.1016/j.jdent.2020.103497
20. Waingade M, Medikeri RS, Gaikwad S. Effectiveness of hyaluronic acid in the management of oral lichen planus: a systematic review and meta-analysis. J Dent Anesth Pain Med. 2022;22(6):405. doi:10.17245/jdapm.2022.22.6.405
21. Santos E, Queirós P, Cardoso D, Cunha M, Apóstolo J. The effectiveness of cleansing solutions for wound treatment: a systematic review. Rev Enferm Ref. 2016;4(9):133–143.
22. Stacey SK, McEleney M. Topical corticosteroids: choice and application. Am Fam Physician. 2021;103(6):337–343.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.