Back to Journals » Clinical Ophthalmology » Volume 19
GLP-1R Agonists Improve Ocular Surface Parameters in Type 2 Diabetes Mellitus
Authors Ottonelli G, Gaeta A ![]() , Montericcio N
, Montericcio N ![]() , Tredici C, Ortfeldt V, Birtolo MF
, Tredici C, Ortfeldt V, Birtolo MF ![]() , Jaafar S
, Jaafar S ![]() , Mirani M
, Mirani M ![]() , Di Maria A
, Di Maria A ![]()
Received 17 June 2025
Accepted for publication 14 September 2025
Published 15 October 2025 Volume 2025:19 Pages 3829—3836
DOI https://doi.org/10.2147/OPTH.S547776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Giovanni Ottonelli,1 Alessandro Gaeta,2 Novella Montericcio,3 Costanza Tredici,1 Vittoria Ortfeldt,4 Maria Francesca Birtolo,4,5 Simona Jaafar,4,5 Marco Mirani,5 Alessandra Di Maria1
1Department of Ophthalmology, IRCCS Humanitas Research Hospital, Milan, 20089, Italy; 2Department of Internal Medicine and Medical Specialties (DIMI), Università Di Genova, Genova, 16132, Italy; 3Biomedicine, Neuroscience and Advance Diagnostic (BIND) Department, University of Palermo, Palermo, 90133, Italy; 4Department of Biomedical Sciences, Humanitas University, Milan, 20072, Italy; 5Endocrinology, Diabetology and Medical Andrology Unit, IRCCS, Humanitas Research Hospital, Milan, 20089, Italy
Correspondence: Alessandra Di Maria, Department of Ophthalmology, IRCCS Humanitas Research Hospital, Rozzano, Milan, 20089, Italy, Tel +39 02 8224 2555, Email [email protected]
Purpose: Dry eye disease (DED) is a prevalent ocular surface disorder frequently associated with type 2 diabetes mellitus (T2DM). While glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have demonstrated systemic anti-inflammatory and vascular benefits beyond glycemic control, their potential impact on tear film parameters remains largely unexplored. This study aimed to evaluate the effects of GLP-1 RAs on ocular surface health in patients with T2DM.
Materials and Methods: In this single-center case-control study, 35 patients with T2DM receiving glucose-lowering therapies were enrolled. Participants were divided into two groups: 21 patients treated with GLP-1 RAs (alone or in combination with other agents) and 14 patients treated with non-GLP-1 RA glucose-lowering medications. Ocular surface parameters—including Schirmer I test and tear breakup time (TBUT)—were assessed and compared between groups.
Results: Patients receiving GLP-1 RAs demonstrated significantly higher Schirmer I test values (median 15 mm, range 1– 33) compared to non-GLP-1 RA users (median 7.5 mm, range 0– 40; p = 0.016). TBUT was also significantly longer in the GLP-1 RA group (median 10 sec, range 6.7– 17) versus controls (median 5.85 sec, range 1– 11; p < 0.01). A subgroup analysis revealed significant differences in tear production across patients treated with GLP-1 RAs alone, SGLT2 inhibitors alone, or both (p = 0.016).
Conclusion: GLP-1 receptor agonist therapy is associated with improved tear production and tear film stability in patients with type 2 diabetes, suggesting a potential protective effect on the ocular surface. These findings highlight an emerging link between antidiabetic therapies and ocular surface health. Prospective, larger-scale studies are warranted to validate these preliminary results and investigate underlying mechanisms.
Keywords: dry eye disease, type 2 diabetes mellitus, GLP-1 receptor agonists, semaglutide, antidiabetic therapy, ocular surface, tear film, T-BUT, schirmer test, real-world evidence
Introduction
Dry eye disease (DED) is a multifactorial disorder of the ocular surface characterized by a loss of tear film homeostasis, resulting in ocular discomfort, visual disturbance, and tear film instability.1 DED is one of the most common ocular conditions worldwide, though its prevalence varies widely from 5% in younger and healthy populations to over 30–50% in high-risk conditions (ie, older age, postmenopausal, arid climates, systemic diseases, etc).2 The pathophysiology of DED involves a complex interplay of inflammation, hyperosmolarity, and neurosensory abnormalities, making this condition challenging to manage.3
Among systemic diseases, diabetes mellitus (DM) has been strongly associated with an increased risk of DED.4,5 Chronic hyperglycemia in DM leads to microvascular damage, including corneal neuropathy and reduced tear production, which can impair ocular surface health.6 Additionally, diabetes-associated inflammation and oxidative stress may further exacerbate DED by disrupting the homeostasis of the tear film and ocular surface.7
In recent years, the role of systemic medications in the development or exacerbation of DED has garnered significant attention, with antihistamines, antidepressants, and antihypertensives have been shown to be implicated in altering tear production or stability.8 However, the impact of newer classes of DM medications, including Glucagon like peptide −1 Receptor agonists (GLP-1 RAs), Dypeptyl-peptidase-4 Inhibitors (DPP4-I), and sodium-glucose cotransporter-2 inhibitors (iSGLT2), on ocular surface health remains poorly understood. In particular GLP-1 RAs, such as dulaglutide and semaglutide, are widely used for the management of type 2 diabetes mellitus (T2DM) due to their efficacy in improving glycemic control, promoting weight loss, and reducing cardiovascular risk.9,10 Specifically, GLP-1 receptors have been identified in lacrimal gland tissue,11 suggesting a potential role of GLP-1 RAs in modulating tear production and inflammatory pathways relevant to DED.12,13 Recent data suggests that GLP-1 RAs could have anti-inflammatory properties that may benefit ocular surface homeostasis.14 However, some findings highlight concerns regarding their potential disruptions to tear film composition and lacrimal gland function. In the specific setting of DM, the potential role of GLP-1 RAs in the development or exacerbation of DED remains unexplored.
Beyond their established role in improving glycemic control and reducing cardiovascular and renal risk, GLP-1 receptor agonists have demonstrated anti-inflammatory, anti-oxidative, and endothelial-protective effects across multiple organ systems. These systemic actions are particularly relevant in the context of diabetic microvascular complications, including ocular involvement. Chronic low-grade inflammation and vascular dysfunction are key contributors to ocular surface damage and tear film instability in patients with diabetes. Therefore, it is biologically plausible that the pleiotropic effects of GLP-1 RAs may extend to ocular tissues, providing protective benefits that could influence the pathophysiology of dry eye disease. This hypothesis supports the rationale for investigating the ocular surface profile in patients treated with GLP-1 RAs.
Thus, the aim of the present study is to evaluate the impact of GLP-1 RAs on DED in patients with T2DM, through the assessment of ocular surface parameters such as tear breakup time (TBUT) and Schirmer test results.
Materials and Methods
Study Population
This single-center, retrospective, case-control study included 35 consecutive patients with a diagnosis of type 2 diabetes mellitus followed-up at the Ophthalmology Departments and Endocrinology and Diabetology Unit of IRCCS Humanitas Research Hospital, Rozzano - Milan (Italy). Patients were divided into two groups: cases (n=21) including those receiving a GLP-1 RAs, alone or in association with other anti-diabetic medication, and controls (n=14) including those receiving other glucose lowering agents but not a GLP-1 RAs.
Inclusion criteria were 1) age > 18 years old, 2) type 2 diabetes mellitus diagnosis, 3) GLP-1 RA therapy for at least a year (cases group). Patients with corneal diseases, glaucoma or concomitant rheumatic diseases that can cause dry eye, epiphora due to obstructions in lacrimal ducts, were excluded.
Clinical and biochemical data - including age, gender, glycated hemoglobin, medications, comorbidities - were collected from electronic medical records. Data collection was finalized in March 2025 and data analysis was completed by 30 April 2025.
As this was a retrospective observational study utilizing all eligible patient records from a fixed timeframe, no formal a priori sample size calculation was feasible. Nevertheless, the final cohort of 35 patients was deemed adequate for exploratory analysis based on clinical relevance, statistical stability, and consistency with previous studies on ocular surface changes in diabetic populations. This approach aligns with standard practice in retrospective real-world investigations.
Given the retrospective design, potential confounders were addressed through careful data extraction and stratification. Baseline variables such as age, gender, HbA1c, and treatment type were compared between groups to ensure balance and detect any systematic differences. While these variables were not included in a multivariate regression due to the small sample size, their similar distribution between groups minimizes the risk of major confounding. No formal matching was applied.
Regarding bias control, ocular surface assessments were conducted using standardized instrumentation (SCHWIND MS-39 OCT) and protocols. However, due to the retrospective nature of data collection, observer masking (blinding) was not feasible. We acknowledge this as a limitation that may have introduced information bias, although objective testing methods and anonymized charts may have mitigated this effect.
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Ethics Committee of IRCCS Humanitas Research Hospital. Due to the retrospective nature of the study, the requirement for informed consent was waived by the Ethics Committee. The patient consent to review their medical records was not required by the Ethics Committee of IRCCS Humanitas Research Hospital. This is because, at our institution, all patients routinely sign a general consent for the processing of personal data, which includes authorization to use anonymized clinical data for scientific and research purposes.
Furthermore, the procedures the patients underwent are part of standard clinical practice and reflect good clinical care, with no additional interventions or experimental protocols beyond routine care. All data used in the study were fully anonymized, and patient confidentiality was rigorously protected throughout the entire process.
The primary objective was to evaluate the impact of GLP-1 RAs on DED in patients with T2DM, comparing ocular parameters between cases and controls groups. As secondary endpoint we compared the ocular parameters between patients treated with GLP-1 RAs alone, SGLT2 inhibitors alone or both GLP-1 RAs and SGLT2 inhibitors.
All procedures in the present study that involved human participants were performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Ocular Surface Parameters Assessment
To assess the quality and quantity of tears, we performed Schirmer I test values and break up time calculated by the tear film analysis assessed by the SCHWIND MS-39 OCT (Schwind eye-tech-solutions, Kleinostheim, Germany). The Schirmer I test measures the amount of tear production over a period of time (usually 5 minutes) and is used to assess the presence of dry eye.15 The TBUT measures the stability of the tear film, ie, the time before the ocular surface becomes dry. It is expressed in seconds, and lower values indicate greater instability of the tear film.16 The results of the Schirmer I test were reported in millimeters (mm), while those of TBUT were reported in seconds (sec).
In addition to objective ocular surface parameters, symptoms of dry eye disease were assessed using the Ocular Surface Disease Index (OSDI) questionnaire. The OSDI is a validated 12-item tool that evaluates ocular discomfort, visual disturbance, and the impact of dry eye on daily activities. Scores range from 0 to 100, with higher values indicating greater symptom severity. Categories were defined as normal (0–12), mild (13–22), moderate (23–32), and severe (≥33). The OSDI was administered at baseline (pre-treatment) and during follow-up at 1 week, 1 month, and 3 months. Data were collected from patient records where available and included in the analysis as exploratory outcomes.
Statistical Analysis
Normally distributed continuous data were presented as mean and ± standard deviation, whereas non-normally distributed data were presented as median and range. Shapiro–Wilk test was used to assess normality. Categorical data were presented as number and percentage. Chi- square test or Fisher’s exact test were used to compare categorical variables. Student’s t-test and Wilcoxon’s test or Kruskal–Wallis test were used to compare continuous variables. A p value < 0.05 was considered as significant. Statistical analysis was performed using R software version 4.3.3.17
Results
Cohort Presentation
Thirty-five consecutive patients with T2DM were included: 21 receiving a GLP-1 RAs, alone or in association with other anti-diabetic medication (cases) and 14 receiving other glucose lowering agents but not a GLP-1 RAs (controls). The median duration of T2DM was 4.05 years (range 2–9 years). Clinical, biochemical, and therapeutic features of included patients are summarized in Table 1.
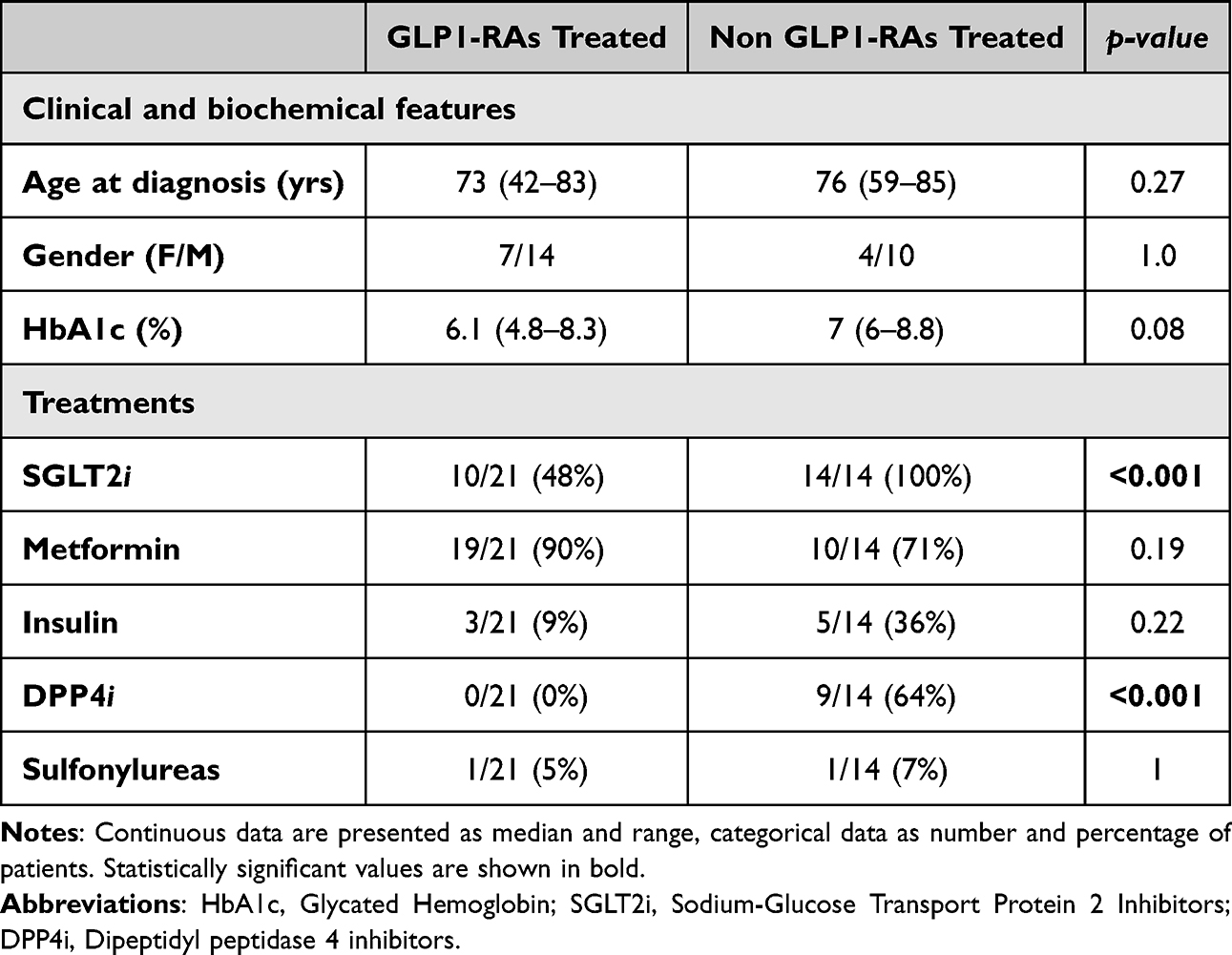 |
Table 1 Clinical, biochemical, and treatment characteristics of patients with type 2 diabetes mellitus treated with GLP-1 receptor agonists versus non-GLP-1 receptor agonist therapies |
The median age of whole cohort was 73 years (range 42–85 years), with a male predominance (2.18 to 1). The entire cohort median of the glycated hemoglobin was 6.6% (range 4.8–8.8%). Specifically, no differences were detected between cases and controls groups in terms of age (p-value = 0.27), sex (p-value = 1) and median glycated hemoglobin (p-value = 0.08).
Concomitant Treatments
Significant differences were observed in concomitant antidiabetic therapies between groups (Table 1). SGLT2 inhibitors and DPP4 inhibitors were more frequently prescribed in the control group (100% and 64%, respectively) compared with the GLP-1 RA group (48% and 0%; both p < 0.001). In contrast, metformin use was high in both groups (90% vs 71%, p = 0.19). Insulin and sulfonylureas were prescribed less frequently, without significant differences between groups. These differences may reflect distinct therapeutic strategies and could have influenced ocular surface outcomes.
These therapeutic imbalances represent potential confounders, as SGLT2 inhibitors and DPP4 inhibitors may influence hydration status or inflammatory pathways, indirectly affecting ocular surface health. Although our sample size did not allow multivariate adjustment, we acknowledge this as a limitation and emphasize the need for future controlled studies to disentangle the effects of GLP-1 RAs from those of concomitant treatments.
Clinical Characteristics Ad Treatment Profiles
The clinical and biochemical characteristics of the study population are summarized in Table 1. Patients in the GLP-1 RA group had a median age of 73 years (range: 42–83), compared to 76 years (range: 59–85) in the control group (p = 0.27). The gender distribution was similar between groups (7 females / 14 males in the GLP-1 RA group vs 4 females / 10 males in the control group, p = 1.0). Median HbA1c was 6.1% (range: 4.8–8.3) in the GLP-1 RA group and 7.0% (range: 6.0–8.8) in controls, with a trend toward lower values in the GLP-1 RA group (p = 0.08).
Regarding concomitant treatments, SGLT2 inhibitors were significantly more frequent in the control group (100% vs 48%, p < 0.001), as were DPP4 inhibitors (64% vs 0%, p < 0.001). Metformin was used in both groups with high prevalence (90% vs 71%, p = 0.19), while insulin and sulfonylureas were less common and not significantly different.
Ocular Surface Parameters in Cases vs Controls (Figure 1)
Both Schirmer I test and TBUT resulted significantly different between cases and controls. Specifically, cases showed higher Schirmer I test values (median 15 mm, range 1–33, 95% CI: 13.7–18.3) compared to controls (median 7.5 mm, range 0–40; 95% CI: 8.5–19.0; p-value 0.016). A significant difference was found also in TBUT between the two groups (median 10 sec, range 6.7–17, 95% CI: 10.2–11.7 vs median 5.85 sec, range 1–11, 95% CI: 4.6–7.2 respectively; p-value <0.01). Moreover, a significant difference was found in the Schirmer I test between patients treated with GLP-1 RAs alone (median 15 mm, range 1–25), SGLT2 inhibitors alone (median 7.5 mm, range 0–40) or both GLP-1 RAs and SGLT2 inhibitors (median 13 mm, range 2–33; Kruskal–Wallis test, p-value=0.016).
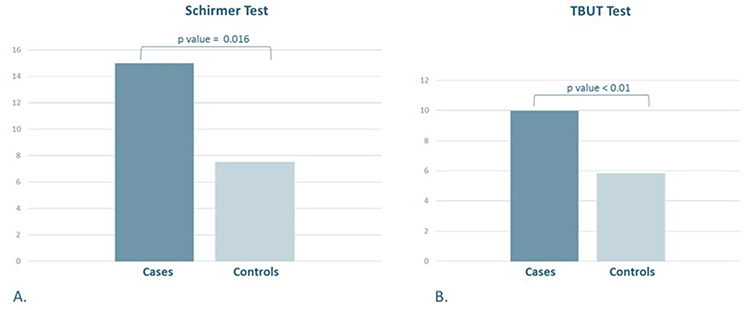 |
Figure 1 Ocular surface parameters in patients receiving GLP-1 RAs (Cases) and not receiving GLP-1 RAs (Controls). (A) Schirmer I test; (B) TBUT (Tear film breakup time) test. |
Patient-Reported Outcomes (Table 2)
Ocular Surface Disease Index (OSDI) scores were evaluated at baseline (pre-treatment) and at 1 week, 1 month, and 3 months after treatment initiation. At baseline, OSDI scores were comparable between groups (median 30 in both, p = 0.88). Over follow-up, patients treated with GLP-1 RAs showed a trend toward lower OSDI values compared with controls, although differences were not statistically significant at any timepoint (Table 2). At 3 months, the GLP-1 RA group reported a median OSDI of 24 (95% CI: 17–28) versus 28 (95% CI: 25–45) in controls (p = 0.39).
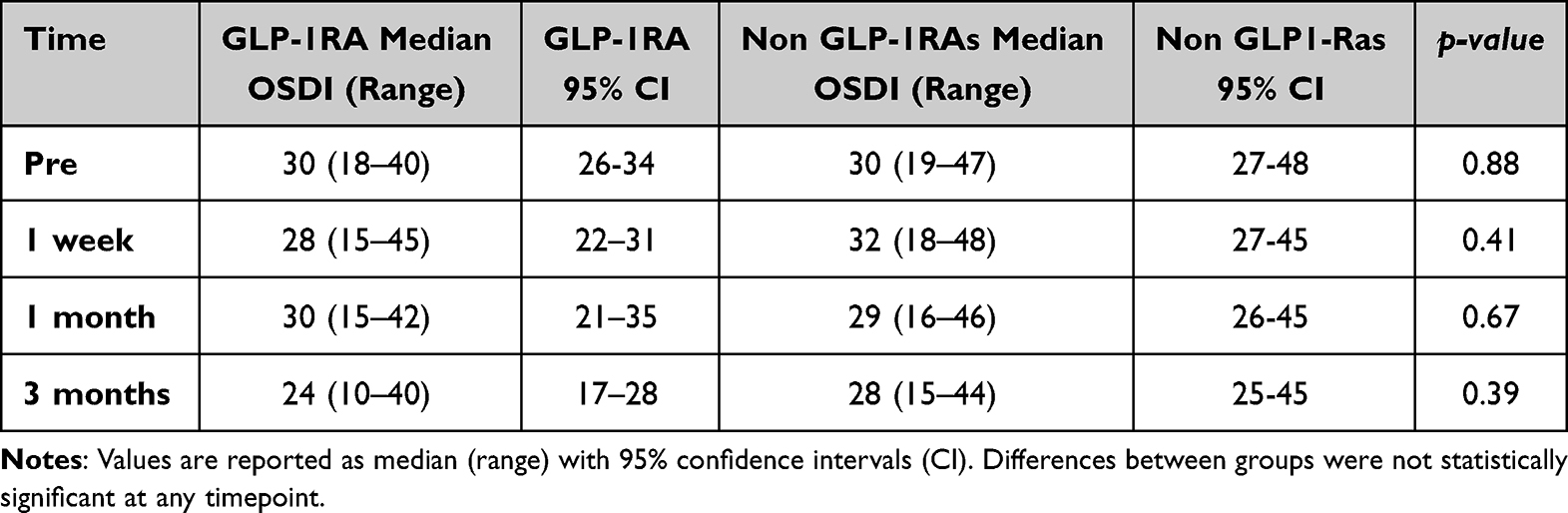 |
Table 2 Ocular Surface Disease Index (OSDI) scores at baseline and during follow-up in patients with type 2 diabetes treated with GLP-1 receptor agonists compared with non-GLP-1 receptor agonist therapies |
Discussion
This retrospective study demonstrated that treatment with GLP-1 RAs has a beneficial impact on tear production and stability in patients with T2DM, potentially reducing the risk of developing dry eye disease. Numerous studies have already highlighted an association between T2DM and DED,18–20 attributing this relationship to factors such as microvascular damage, corneal neuropathy, and chronic inflammation. Diabetes is known to alter meibomian gland function, reduce goblet cell density, and impair corneal sensitivity, all of which contribute to tear film dysfunction.21 However, evidence regarding the specific effects of different antidiabetic drugs on the ocular surface is still limited, with most available data at the preclinical stage.
In addition to ocular surface outcomes, clinical and biochemical characteristics were considered to contextualize our findings. Age and gender distributions were balanced between groups (median age 73 vs 76 years; female proportion 33% vs 29%), minimizing their potential as confounders. Glycemic control, assessed by HbA1c, showed a trend toward lower values in the GLP-1 RA group (6.1% vs 7.0%, p = 0.08), which may have contributed to improved tear film stability and production, although this difference was not statistically significant and cannot solely explain the ocular surface differences. Importantly, significant imbalances in concomitant therapies were observed: SGLT2 inhibitors and DPP4 inhibitors were more prevalent in the control group (100% and 64%, respectively) compared with the GLP-1 RA group (48% and 0%; both p < 0.001), while metformin use was high in both groups (90% vs 71%, p = 0.19). These therapeutic differences may reflect distinct metabolic profiles and could act as confounders, as some antidiabetic agents might indirectly affect ocular surface homeostasis through hydration status or inflammatory pathways. Although our sample size precluded multivariate adjustment, we acknowledge these differences as a study limitation.
From a clinical perspective, patient-reported outcomes add important context. The OSDI questionnaire revealed a consistent, though non-significant, trend toward lower symptom burden in GLP-1 RA users. At baseline, OSDI scores were comparable between groups (median 30 in both, p = 0.88). Over follow-up, the GLP-1 RA group reported slightly lower scores at all timepoints, with the largest difference at 3 months (median 24 [95% CI: 17–28]) compared with controls (median 28 [95% CI: 25–45], p = 0.39). The parallel between subjective OSDI improvement and objective ocular surface parameters strengthens the plausibility of a protective effect of GLP-1 RAs. Incorporating patient-reported outcomes in future prospective trials will be crucial to capture the full clinical impact of antidiabetic therapies on ocular surface health.
Mechanistically, GLP-1 RAs such as dulaglutide and semaglutide are known for their anti-inflammatory effects and their modulatory role in tear secretion.22 Preclinical studies have demonstrated the presence of GLP-1 receptors in the lacrimal glands,13 supporting a direct biological mechanism that may explain the better outcomes observed in our GLP-1 RA group. In contrast, SGLT2 inhibitors, although effective for glycemic and cardiovascular risk reduction,23 promote renal excretion of glucose and sodium, potentially leading to mild systemic dehydration and reduced tear production.24,25 Our data support this hypothesis, showing higher Schirmer values in patients treated with GLP-1 RAs alone, intermediate values in those treated with both GLP-1 RAs and SGLT2 inhibitors, and the lowest values in patients treated with SGLT2 inhibitors alone. These findings suggest that the detrimental ocular effects of SGLT2 inhibitors may be mitigated by the protective influence of GLP-1 RAs.
This study has some limitations that must be acknowledged. The retrospective design and small sample size limit generalizability and precluded formal power calculation or multivariate analysis. Differences in concomitant treatments represent another potential confounder, as discussed above. Furthermore, OSDI data were not available for all patients. These factors highlight the need for larger, prospective studies with standardized collection of both objective and patient-reported outcomes to confirm and expand our findings.
Despite these limitations, this is, to our knowledge, the first study to suggest an association between GLP-1 RA therapy and improved tear production and stability in patients with T2DM. If confirmed in larger trials, these results could have relevant implications for personalized diabetes management, offering not only metabolic and cardiovascular benefits but also potential protective effects on ocular surface health.
Conclusion
In this retrospective case-control study, the use of GLP-1 receptor agonists in patients with type 2 diabetes mellitus was associated with improved ocular surface parameters, including increased tear film stability and tear production, compared to patients on other antidiabetic agents. These findings suggest that GLP-1 RAs may exert protective effects on the ocular surface, potentially through anti-inflammatory or neurovascular mechanisms.
While these results are preliminary and hypothesis-generating, they open a new avenue for evaluating antidiabetic therapies not only for systemic metabolic control but also for their ocular effects. Prospective studies with larger samples and mechanistic insights are warranted to validate these findings and explore their clinical translation in the management of diabetes-associated dry eye disease.
AI Declaration
AI tools were not used in the writing process of the present article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/J.JTOS.2017.05.008
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/J.JTOS.2017.05.003
3. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/J.JTOS.2017.05.011
4. Zhang X, Zhao L, Deng S, Sun X, Wang N. Dry eye syndrome in patients with diabetes mellitus: prevalence, etiology, and clinical characteristics. J Ophthalmol. 2016;2016:1–7. doi:10.1155/2016/8201053
5. Kaiserman I, Kaiserman N, Nakar S, Vinker S. Dry eye in diabetic patients. Am J Ophthalmol. 2005;139(3):498–503. doi:10.1016/J.AJO.2004.10.022
6. Misra SL, Patel DV, McGhee CNJ, et al. Peripheral neuropathy and tear film dysfunction in type 1 diabetes mellitus. J Diabetes Res. 2014;2014:1–6. doi:10.1155/2014/848659
7. Kuo YK, Shao SC, Lin ET, Pan LY, Yeung L, Sun CC. Tear function in patients with diabetes mellitus: a systematic review and meta-analysis. Frontiers Media S A. 2022;21. doi:10.3389/fendo.2022.1036002
8. Fraunfelder FT, Sciubba JJ, Mathers WD. The role of medications in causing dry eye. J Ophthalmol. 2012;2012:1–8. doi:10.1155/2012/285851
9. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMOA1607141
10. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMOA2032183
11. Sun Y, Zhang Y, Shi F, et al. Characterization and role of glucagon-like peptide 1 receptor in the lacrimal gland. Am J Pathol. 2024;195(4):797–810. doi:10.1016/j.ajpath.2024.12.003
12. Hebsgaard JB, Pyke C, Yildirim E, Knudsen LB, Heegaard S, Kvist PH. Glucagon-like peptide-1 receptor expression in the human eye. Diabetes Obes Metab. 2018;20(9):2304–2308. doi:10.1111/DOM.13339
13. Sun Y, Zhang Y, Shi F, et al. Characterization and role of glucagon-like peptide 1 receptor in the lacrimal gland: novel insights into diabetic dry eye pathogenesis. Am J Pathol. 2025;195(4):797–810. doi:10.1016/J.AJPATH.2024.12.003
14. Fan YC, Peng SY, Chang CK, et al. The utilization of glucagon-like peptide 1 agonists and risk of following external eye diseases in type 2 diabetes mellitus individuals: a population-based study. Healthcare. 2023;11(20). doi:10.3390/healthcare11202749
15. NR B, M Z, Y R. Schirmer Test. Encyclopedia Ophthalmol. 2025;1–2. doi:10.1007/978-3-642-35951-4_946-1
16. Yokoi N, Georgiev GA. Tear-film-oriented diagnosis for dry eye. Jpn J Ophthalmol. 2019;63(2):127–136. doi:10.1007/S10384-018-00645-4
17. R: the R project for statistical computing. Available from: https://www.r-project.org/.
18. Qian L, Wei W. Identified risk factors for dry eye syndrome: a systematic review and meta-analysis. PLoS One. 2022;17(8):e0271267. doi:10.1371/JOURNAL.PONE.0271267
19. De Freitas GR, Ferraz GAM, Gehlen M, Skare TL. Dry eyes in patients with diabetes mellitus. Prim Care Diabetes. 2021;15(1):184–186. doi:10.1016/J.PCD.2020.01.011
20. Najafi L, Malek M, Valojerdi AE, et al. Dry eye and its correlation to diabetes microvascular complications in people with type 2 diabetes mellitus. J Diabetes Complications. 2013;27(5):459–462. doi:10.1016/j.jdiacomp.2013.04.006
21. Abu EK, O Ofori A, B Boadi-Kusi S, et al. Dry eye disease and meibomian gland dysfunction among a clinical sample of type 2 diabetes patients in Ghana. Afr Health Sci. 2022;22(1):293–302. doi:10.4314/AHS.V22I1.36
22. Vergès B, Charbonnel B. After the LEADER trial and SUSTAIN-6, how do we explain the cardiovascular benefits of some GLP-1 receptor agonists? Diabetes Metab. 2017;43:2S3–2S12. doi:10.1016/S1262-3636(17)30067-8
23. Preda A, Montecucco F, Carbone F, et al. SGLT2 inhibitors: from glucose-lowering to cardiovascular benefits. Cardiovasc Res. 2024;120(5):443–460. doi:10.1093/CVR/CVAE047
24. Schwartz SS, Ahmed I. Sodium-glucose cotransporter 2 inhibitors: an evidence-based practice approach to their use in the natural history of type 2 diabetes. Curr Med Res Opin. 2016;32(5):907–919. doi:10.1185/03007995.2016.1151774
25. Dartt DA, Willcox MDP. Complexity of the tear film: importance in homeostasis and dysfunction during disease. Exp Eye Res. 2013;117:1–3. doi:10.1016/J.EXER.2013.10.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.