Back to Journals » International Journal of Women's Health » Volume 18
Giant Vulvar Mesonephric Duct Cysts Mimicking Malignancy: A Case Report and Diagnostic Challenge
Authors Sembiring RH ![]() , Suardi D, Salima S
, Suardi D, Salima S ![]() , Siddiq A
, Siddiq A
Received 3 May 2026
Accepted for publication 1 July 2026
Published 10 July 2026 Volume 2026:18 621675
DOI https://doi.org/10.2147/IJWH.S621675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Rico Henando Sembiring, Dodi Suardi, Siti Salima, Amillia Siddiq
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Rico Henando Sembiring, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, Tel +6282295948911, Email [email protected]
Background: Vulvar masses present a diagnostic challenge due to their wide spectrum from benign lesions to malignancy. Mesonephric duct cysts are rare benign lesions derived from Wolffian duct remnants that may clinically mimic vulvar cancer, particularly when large or symptomatic.
Case Presentation: A 49-year-old multiparous woman presented with a painful vulvar mass that had progressively enlarged over one year. The patient reported that a similar lesion had been present for approximately 10 years. The lesion ruptured spontaneously several years earlier with purulent discharge and subsequently decreased in size. However, the patient did not seek medical attention or receive any treatment at that time. Progressive enlargement and pain developed during the preceding year, prompting medical consultation. Physical examination revealed multiple bilateral vulvar masses and uterine enlargement. Imaging suggested uterine leiomyoma. Due to high suspicion of malignancy, surgical excision of vulvar masses combined with total hysterectomy and bilateral salpingo-oophorectomy was performed. Histopathological examination revealed multiple mesonephric duct cysts without atypia or invasion and confirmed uterine leiomyoma.
Conclusion: Mesonephric duct cysts can closely mimic vulvar malignancy, especially when presenting as large and symptomatic masses. Histopathological evaluation remains the gold standard for diagnosis, and surgical excision is essential in cases with diagnostic uncertainty.
Keywords: mesonephric duct cyst, vulvar mass, benign lesion, vulvar tumor, diagnostic challenge
Introduction
Vulvar lesions encompass a broad spectrum of conditions, ranging from benign cystic lesions to malignant tumors. Differentiating between these entities is critical, as delayed diagnosis of vulvar malignancy is associated with worse clinical outcomes.1,2
Mesonephric duct cysts arise from remnants of the Wolffian (mesonephric) duct. Gartner duct cysts represent a specific subtype occurring within the vaginal wall, whereas mesonephric remnants may occur at other sites of the female genital tract, originate from embryological remnants of the Wolffian duct. Although typically small and asymptomatic, these cysts may enlarge due to chronic inflammation, obstruction, or infection, leading to atypical presentations that mimic malignancy.3,4
This case highlights the diagnostic challenges and clinical decision-making involved in managing a large vulvar mass initially suspected as malignancy but ultimately confirmed as a benign mesonephric duct cyst.
Case Presentation
A 49-year-old multiparous woman presented with a painful vulvar mass that had progressively enlarged over one year. The patient reported that a similar lesion had been present for approximately 10 years. The lesion ruptured spontaneously several years earlier with purulent discharge and subsequently decreased in size. However, the patient did not seek medical attention or receive any treatment at that time. Progressive enlargement and pain developed during the preceding year, prompting medical consultation.
Physical examination revealed multiple bilateral vulvar masses involving both labia majora (Figure 1). The masses were irregular in contour, predominantly cystic-to-firm in consistency, mildly tender on palpation, and partially mobile relative to the underlying tissue. The largest mass measured approximately 6×5 cm on clinical examination. The patient reported a similar lesion that had been present for approximately 10 years and had ruptured spontaneously several years earlier with purulent discharge, after which partial regression occurred. However, progressive enlargement and pain developed during the preceding year. Because of the irregular surface, progressive growth, bilateral involvement, and associated pain, vulvar malignancy could not be excluded clinically.
 |
Figure 1 Clinical appearance of vulvar masses. Multiple bilateral vulvar masses with irregular surface and varying sizes observed on physical examination. |
Pelvic ultrasonography demonstrated a markedly enlarged uterus corresponding to a 20–24-week gestational size and containing a large leiomyoma (Figure 2). Considering the patient’s age, completed parity, symptomatic uterine enlargement, and the need for definitive surgical management of a vulvar lesion highly suspicious for malignancy, total hysterectomy with bilateral salpingo-oophorectomy was performed concurrently with excision of the vulvar masses.
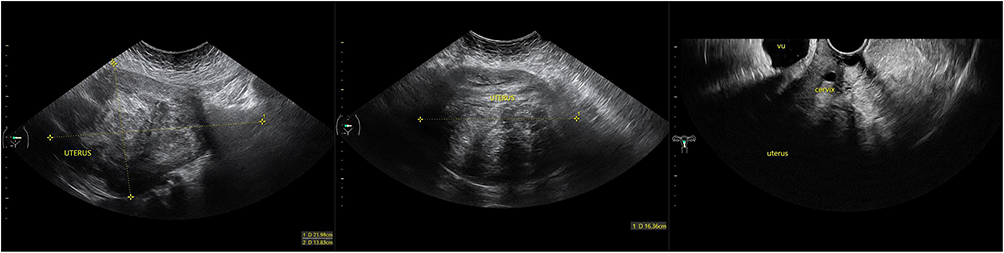 |
Figure 2 Ultrasonographic findings. Pelvic ultrasonography demonstrating an enlarged uterus with a large solid mass consistent with leiomyoma. |
Intraoperatively, bilateral vulvar masses measuring up to 10×13 cm were identified. Preoperative and postoperative findings are presented in Figure 3. Gross surgical specimens obtained during surgery are shown in Figure 4 Histopathological examination confirmed multiple mesonephric duct cysts with fibrotic stroma and lymphocytic infiltration, without cellular atypia or invasion (Figure 5). The uterine mass was confirmed as leiomyoma.
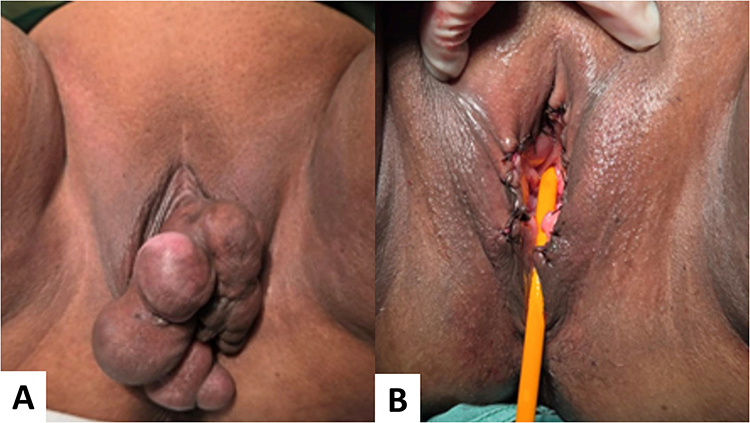 |
Figure 3 Preoperative and postoperative findings. (A) Preoperative appearance of vulvar masses. (B) Postoperative condition following surgical excision. |
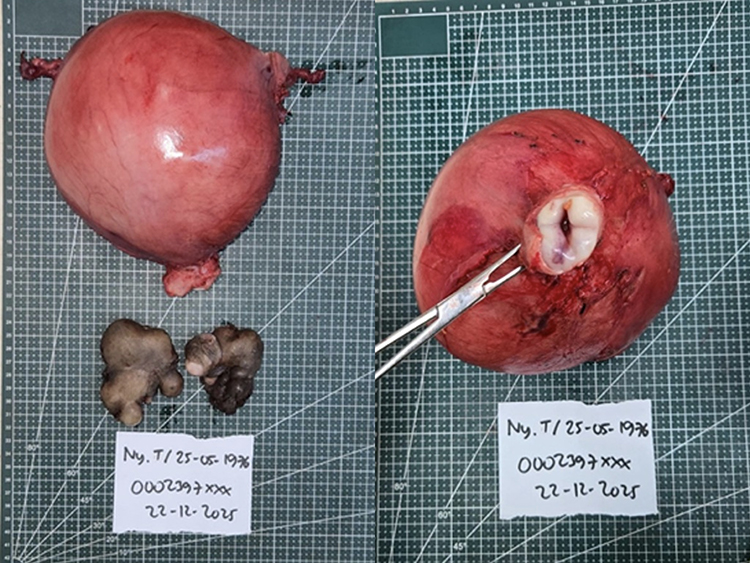 |
Figure 4 Surgical specimen. Gross specimen showing enlarged uterus and excised vulvar masses. |
 |
Figure 5 Histopathological findings. Microscopic examination demonstrating Vulvar mass section lined by keratinized stratified squamous epithelium with nuclei within normal limits. The subepithelial layer consists of edematous fibrocollagenous connective tissue stroma with lymphocytic infiltration. Cutaneous adnexal structures are present, including eccrine (sudoriferous) glands within normal limits. Interspersed are multiple cystic structures lined by ciliated columnar epithelium with nuclei within normal limits. Some lumina contain eosinophilic material. No evidence of malignancy is identified. (H&E stain). |
Discussion
Mesonephric duct cysts arise from remnants of the Wolffian duct that persist in the female genital tract. These remnants retain the ability to undergo epithelial differentiation and cystic dilation.3–6
Large or complicated cysts may mimic malignancy due to progressive enlargement, chronic inflammation, fibrosis, and atypical anatomical location such as the vulva.3,4,7
Clinical examination and imaging alone are often insufficient to reliably distinguish benign from malignant lesions. Therefore, histopathological evaluation remains the gold standard for diagnosis.1,8
In cases where malignancy cannot be excluded clinically, an oncologic approach is justified. Surgical excision provides both definitive diagnosis and therapeutic management, particularly in symptomatic or large lesions.1,9
Several benign vulvar lesions may clinically mimic malignancy. Bartholin gland cysts may present as large unilateral masses with rapid enlargement. Epidermal inclusion cysts may demonstrate irregular contours and chronic inflammation. Aggressive angiomyxoma frequently presents as a large infiltrative vulvar mass and may be mistaken for a soft tissue sarcoma. Vulvar endometriosis may manifest as painful nodular lesions with irregular borders, whereas hidradenitis suppurativa may produce chronic ulcerative lesions and fibrosis that simulate invasive vulvar carcinoma. Consequently, histopathological examination remains essential for definitive diagnosis.10–12
Magnetic resonance imaging (MRI) may provide additional diagnostic value in selected patients with large or atypical vulvar masses. MRI offers superior soft-tissue characterization and may better define lesion extent, cystic components, and potential invasion of adjacent structures. However, in many low-resource settings, MRI availability may be limited, and definitive diagnosis ultimately relies on histopathological examination following excision.
This case highlights the importance of considering benign mimickers in the differential diagnosis of vulvar malignancy, particularly in large and atypical lesions.
Conclusion
Mesonephric duct cysts are rare benign lesions that may clinically mimic vulvar malignancy, particularly when presenting with atypical features. A systematic approach with histopathological confirmation is essential.3,4
Abbreviations
ACR, American College of Radiology; ESGO, European Society of Gynaecological Oncology; H&E, Hematoxylin and Eosin; NCCN, National Comprehensive Cancer Network; RCOG, Royal College of Obstetricians and Gynaecologists.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was not required for this case report in accordance with institutional policies. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aul S, Van der Velden J, Oonk M. et al. ESGO guidelines for the management of vulvar cancer. Int J Gynecol Cancer. 2023;33(1):1–6. doi:10.1136/ijgc-2022-004337
2. Royal College of Obstetricians and Gynaecologists (RCOG). Management of Vulval cancer. Green-Top Guideline No 58. 2014.
3. Young RH. Mesonephric lesions of the female genital tract. Mod Pathol. 2016;29(S1):S81–S92. doi:10.1038/modpathol.2015.139
4. McCluggage WG. Mesonephric lesions of the female genital tract. Int J Gynecol Pathol. 2019;38(Suppl 1):S34–S42. doi:10.1097/PGP.0000000000000495
5. Nucci MR, Oliva E. Gynecologic Pathology.
6. Roma AA, Masand RP. Ovarian and extraovarian mesonephric lesions. Adv Anat Pathol. 2015;22(5):290–302. doi:10.1097/PAP.0000000000000079
7. Li X, Zhang Y, Zhao C. et al. Clinical and pathological characteristics of mesonephric lesions. J Obstet Gynaecol Res. 2020;46(6):897–904. doi:10.1111/jog.14242
8. American College of Radiology. ACR Appropriateness Criteria® Staging and Follow-up of Vulvar Cancer; 2022.
9. Berek JS, Hacker NF. Berek & Hacker’s Gynecologic Oncology.
10. Woelber L, Trillsch F, Mahner S.et al. Management of vulvar cancer: ESGO guidelines update. Int J Gynecol Cancer. 2023;33(1):1–25. doi:10.1136/ijgc-2022-004337
11. National Comprehensive Cancer Network (NCCN). NCCN clinical practice guidelines in oncology: vulvar cancer. Version 2024.
12. Köhler C, Buderath P, Hillemanns P. et al. Diagnostic challenges in vulvar lesions: benign mimickers of malignancy. Gynecol Oncol. 2022;166(2):285–292. doi:10.1016/j.ygyno.2022.05.015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.