Back to Journals » International Medical Case Reports Journal » Volume 19
Giant Parathyroid Adenoma Masked by Severe Vitamin D Deficiency with Hypocalcemic Presentation: A Case Report
Authors Khalil B ![]() , Chiha A, Kousa A
, Chiha A, Kousa A ![]() , Alrez A, Alayyoubi A, Alhamid AAH, Glore A
, Alrez A, Alayyoubi A, Alhamid AAH, Glore A
Received 7 January 2026
Accepted for publication 24 March 2026
Published 30 March 2026 Volume 2026:19 594398
DOI https://doi.org/10.2147/IMCRJ.S594398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Thomas E Hutson
Bana Khalil,1,* Ali Chiha,2,* Alyamama Kousa,3 Anass Alrez,4 Aya Alayyoubi,5 Ahmad Abdul Hakim Alhamid,6 Areen Glore7
1Faculty of Medicine, Tishreen University, Latakia, Syria; 2School of Medicine, St. George’s University, St. George’s, Grenada; 3Department of Cardiology, Syrian Arab Red Crescent Hospital, Damascus, Syria; 4Faculty of Medicine, Al-Sham Private University, Damascus, Syria; 5Department of General Surgery, Al- Razi Hospital, Aleppo, Syria; 6Department of Orthopedic Surgery, Al-Razi Hospital, Aleppo, Syria; 7Faculty of Medicine, Aleppo University, Aleppo, Syria
*These authors contributed equally to this work
Correspondence: Bana Khalil, Faculty of Medicine, Tishreen University, Latakia, Syria, Email [email protected]
Introduction: Giant parathyroid adenomas, defined as lesions weighing at least 3.5 grams, are rare and typically present with hypercalcemia due to excessive parathyroid hormone secretion. Severe vitamin D deficiency can alter this pattern by lowering serum calcium, which may obscure the diagnosis of primary hyperparathyroidism, especially in younger patients. This case is notable because a large parathyroid adenoma presented with hypocalcemia rather than hypercalcemia, creating an atypical biochemical profile that initially mimicked secondary hyperparathyroidism.
Case Presentation: A 30-year-old Syrian woman presented with a nine-month history of progressive fatigue, generalized bone pain, intermittent paresthesia in her fingertips, and cervical discomfort. Physical examination was unremarkable, with no palpable cervical or thyroid mass. Laboratory evaluation demonstrated severe vitamin D deficiency, hypocalcemia with low total and ionized calcium, and markedly elevated parathyroid hormone levels. She was started on calcium and vitamin D supplementation, which normalized calcium levels; however, parathyroid hormone levels remained inappropriately elevated, thereby unmasking underlying autonomous primary hyperparathyroidism. Two ultrasound examinations were non-diagnostic, whereas 99mTc-sestamibi scintigraphy showed persistent radiotracer uptake consistent with a hyperfunctioning left inferior parathyroid gland. The patient underwent focused parathyroidectomy, and a 3.5-gram adenoma was excised. Histopathological examination confirmed a benign giant adenoma without capsular or vascular invasion. Postoperatively, serum calcium remained stable and parathyroid hormone levels were appropriately suppressed. The patient experienced no symptoms of hypocalcemia and did not develop hungry bone syndrome. She was discharged the same day and had an uneventful recovery with normal biochemical findings on follow-up.
Conclusion: This case demonstrates how severe vitamin D deficiency can mask the expected biochemical features of primary hyperparathyroidism and delay recognition of a giant parathyroid adenoma. It highlights the limitations of ultrasound in detecting deep or inferior parathyroid glands and emphasizes the importance of functional imaging when anatomic studies are inconclusive. Recognition of this atypical presentation is essential to avoid diagnostic delays and guide appropriate imaging and timely surgical management.
Plain Language Summary: People with an overactive parathyroid gland usually have high levels of calcium in their blood. However, some individuals with severe vitamin D deficiency may show the opposite pattern, with low calcium levels that hide the true problem. This makes the condition harder for doctors to recognize.
In this report, we describe the experience of a 30-year-old woman who had long-lasting bone pain and vitamin D deficiency. Even though her parathyroid hormone (a hormone that controls calcium levels) was high, her blood calcium was low. After she received vitamin D and calcium supplements, her calcium returned to normal, but her parathyroid hormone remained much too high. This finding helped reveal that she had an overactive parathyroid gland.
A specialized imaging test, called a Sestamibi scan, showed a large parathyroid growth that ultrasound could not detect. Surgeons removed a 3.5-gram parathyroid adenoma, which is unusually large. After surgery, her hormone levels returned to normal, and she recovered without complications.
This case shows that very low vitamin D levels can hide important signs of parathyroid disease, leading to delays in diagnosis. It also highlights the value of combining different tests, like blood work, vitamin D correction, and specialized imaging, to identify the true cause of symptoms. Recognizing this pattern can help doctors make earlier diagnoses and provide more effective care.
Keywords: parathyroid adenoma, primary hyperparathyroidism, vitamin D deficiency
Introduction
Primary Hyperparathyroidism (PHPT) is the leading cause of hypercalcemia in outpatient settings and results from autonomous overproduction of parathyroid hormone (PTH) by one or more parathyroid glands. It typically presents with elevated serum calcium and inappropriately normal or elevated PTH levels.1 PHPT is most commonly diagnosed in adults between 50 and 70 years of age and is three times more prevalent in women. Most cases are caused by a single parathyroid adenoma (PTA), whereas multiglandular disease is less common, and parathyroid carcinoma accounts for fewer than 1% of cases.2 PTAs typically weigh less than 1 g, and adenomas that weigh at least 3.5 g are classified as giant parathyroid adenomas (GPTA), a rare subgroup representing no more than 1.5% of all parathyroid adenomas.3,4
The diagnosis of parathyroid lesions may present significant challenges within endocrine and head and neck pathology, particularly when biochemical findings are atypical. Distinguishing between benign and malignant parathyroid neoplasms based solely on macroscopic or radiologic features can be unreliable, as large adenomas may mimic carcinoma in both clinical and imaging presentations.5,6 Accordingly, accurate diagnosis relies on a multimodal approach incorporating laboratory findings, targeted imaging, and definitive histopathological evaluation, with ancillary testing playing a critical role in preventing misclassification and guiding appropriate management. This lines with current international consensus guidelines that emphasize a structured, criteria-based approach to the evaluation and management of PHPT.7
Vitamin D deficiency is frequently observed in individuals with PHPT and can alter the classical biochemical presentation of the disease.8 Reduced vitamin D levels decrease intestinal calcium absorption, which may maintain normal or even low serum calcium levels despite elevated PTH secretion.3 As a result, severe vitamin D deficiency can mask the hypercalcemia typically associated with PHPT, delay recognition of the underlying disorder, and complicate the diagnostic evaluation.9
We present a case of PHPT in a 30-year-old Syrian woman in whom severe vitamin D deficiency produced hypocalcemia, obscured the classical biochemical profile, and delayed the diagnosis of a giant parathyroid adenoma. This case highlights the importance of considering PHPT in patients with elevated PTH levels even when hypercalcemia is not present.
Case Presentation
A 30-year-old Syrian woman presented to the endocrinology department with a nine-month history of progressive fatigue, generalized bone pain, and cervical discomfort. She reported intermittent paresthesia in the fingertips and denied nephrolithiasis, pathological fractures, gastrointestinal symptoms, or psychiatric manifestations. The patient had no history of chronic medical conditions and was not taking any medications known to affect calcium metabolism. There was no reported family history suggesting a hereditary endocrine syndrome. On physical examination, no lymphadenopathy or palpable cervical or thyroid mass was detected. Chvostek’s and Trousseau’s signs were absent, and the remainder of the examination was unremarkable.
Initial laboratory evaluation demonstrated severe vitamin D deficiency (25-hydroxyvitamin D: 25 nmol/L) and hypocalcemia (serum calcium: 1.89 mmol/L; ionized calcium: 1.05 mmol/L) with markedly elevated intact parathyroid hormone levels (PTH: 247 ng/L). Serum albumin was within the normal range (38.2 g/L), indicating that the low calcium level was not attributable to hypoalbuminemia. Serum phosphorus was mildly decreased at 0.71 mmol/L, while renal function remained normal (creatinine: 62.8 µmol/L). Alkaline phosphatase was mildly elevated at 168 U/L. Routine laboratory studies, including complete blood count, were within normal limits. The pattern of hypocalcemia with elevated PTH prompted initiation of calcium and vitamin D supplementation. After six weeks of treatment, vitamin D improved to 75.25 nmol/L and serum calcium normalized to 2.27 mmol/L (ionized calcium: 1.28 mmol/L). However, PTH remained inappropriately elevated at 151 ng/L (Table 1).
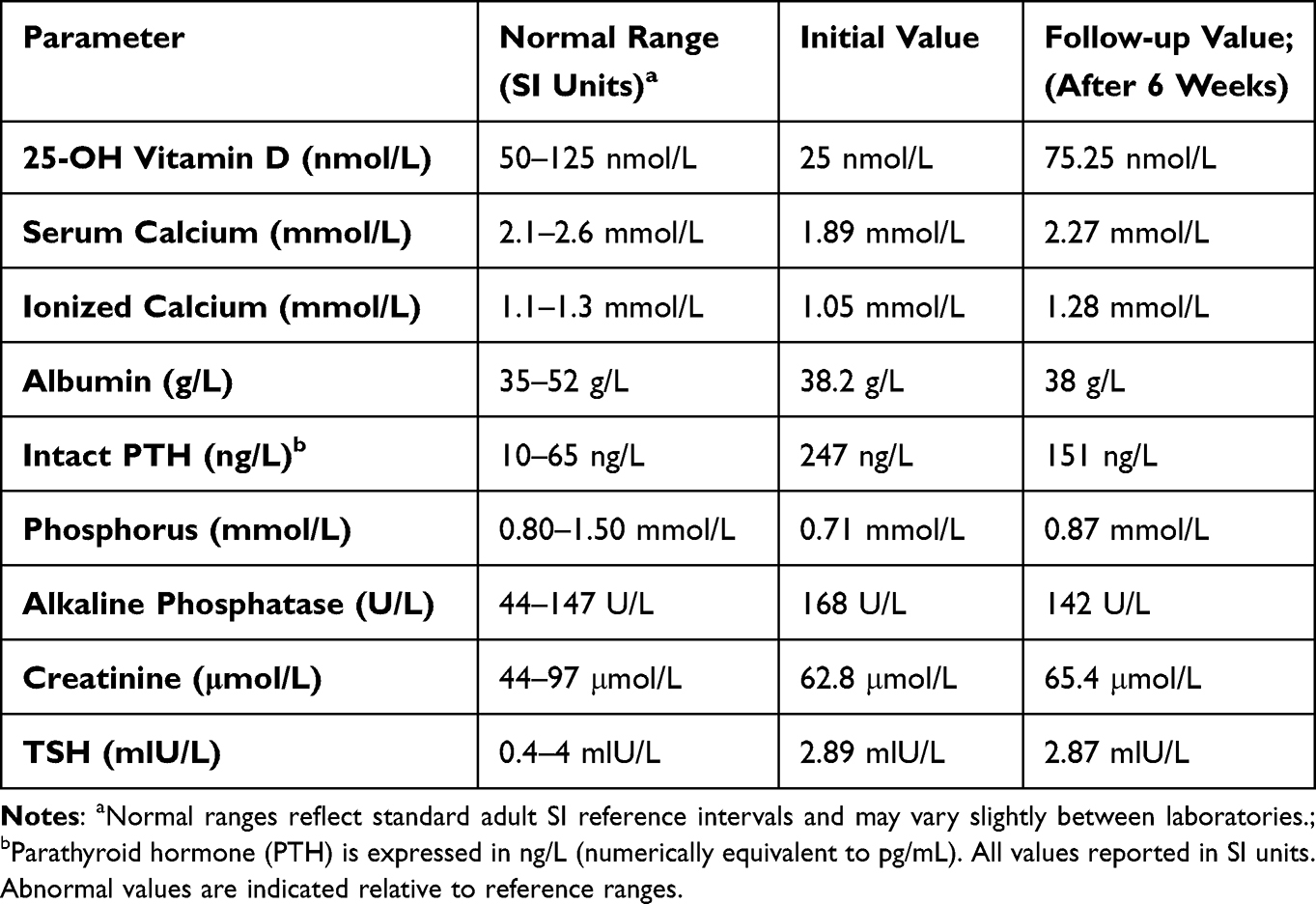 |
Table 1 Laboratory Values at Presentation and After Six weeks of Supplementation |
Persistent elevation of PTH despite correction of vitamin D deficiency raised suspicion for primary hyperparathyroidism and prompted further imaging to localize a potential parathyroid source.
Neck ultrasonography performed at two separate centers identified a well-circumscribed, hypoechoic, oval-shaped nodule in the lower pole of the left thyroid lobe measuring approximately 18×18 × 13 mm. However, due to its posterior location and overlapping sonographic characteristics with thyroid tissue, ultrasound could not reliably distinguish whether the lesion originated from thyroid or parathyroid tissue. Given these inconclusive findings, further localization with functional imaging was indicated. A 99mTc-sestamibi scintigraphy demonstrated a distinct focus of radiotracer uptake inferior to the left thyroid lobe on early images, with persistent tracer retention on delayed imaging, a pattern characteristic of a hyperfunctioning parathyroid adenoma (Figure 1).
 |
Figure 1 99mTc-sestamibi Parathyroid Scintigraphy Demonstrating Left Inferior Parathyroid Adenoma. 99mTc-sestamibi parathyroid scintigraphy demonstrating a left inferior hyperfunctioning parathyroid adenoma. Early-phase imaging (left) shows radiotracer uptake in the thyroid gland with a focal area of increased activity in the left inferior neck. Delayed-phase imaging (right) demonstrates persistent radiotracer retention in the same region, consistent with a parathyroid adenoma. Red arrows indicate the site of abnormal uptake. |
Subsequently, the patient was referred for surgical management. A focused parathyroidectomy was performed under general anesthesia targeting the left inferior parathyroid gland. The procedure lasted approximately one hour. Intraoperatively, a markedly enlarged left inferior parathyroid gland was identified and excised without complication. A Rodivac drain was placed at the surgical site. The surgical specimen was sent for histopathological analysis. Gross examination revealed a well-circumscribed, tan parathyroid nodule measuring 2×2 × 1 cm and weighing 3.5 g, meeting the weight threshold for a giant parathyroid adenoma. Microscopic evaluation showed proliferation of uniform chief cells arranged in solid and trabecular patterns with a thin rim of compressed normal parathyroid tissue. Malignant features such as capsular invasion, vascular invasion, necrosis, or atypical mitotic activity were absent.
Postoperative laboratory studies obtained four hours after surgery demonstrated biochemical cure, with serum calcium stable at 2.09 mmol/L and PTH suppressed to 7 ng/L (reference range: 10–65 ng/L). The postoperative course was uncomplicated. The patient remained hemodynamically stable, reported no symptoms of hypocalcemia, and showed no evidence of recurrent laryngeal nerve injury. Routine postoperative monitoring was sufficient, and no aggressive calcium or calcitriol supplementation was required. She met criteria for same-day discharge and was released with instructions for close biochemical follow-up. The drain was removed on postoperative day three.
Discussion
Primary hyperparathyroidism is most commonly caused by a solitary adenoma under one gram and typically arises in individuals between fifty and seventy years of age.1,2 Cases in patients younger than forty are uncommon, making this presentation at age thirty atypical.2 Giant parathyroid adenomas are particularly rare and are generally defined as lesions weighing at least 3.5 g.4 Several analyses have reported that adenomas of this size can be associated with more pronounced symptoms, including bone pain, musculoskeletal weakness, nephrolithiasis, and neurocognitive complaints although presentations remain variable, and some patients may present with mild or atypical features despite large tumor size.3 Although young age can raise concern for hereditary causes such as MEN1 (Multiple endocrine neoplasia type 1), MEN2A (Multiple endocrine neoplasia type 2A), or CDC73 (Cell division cycle 73 gene)-related syndromes, the solitary nature of the adenoma confirmed on pathology, coupled with the absence of familial history or other syndromic features, makes a sporadic etiology most likely.10
Severe vitamin D deficiency (25 nmol/L) played a central role in this patient’s atypical biochemical profile. Vitamin D is required for intestinal calcium absorption, renal calcium reabsorption, and normal bone mineralization.2,3 When levels are low, calcium availability falls, resulting in hypocalcemia despite markedly elevated PTH. This interaction can mask the hypercalcemia of PHPT and produce a biochemical pattern that mimics secondary hyperparathyroidism, a phenomenon frequently reported in regions with high rates of vitamin D deficiency, including the Middle East.3,8 Emerging evidence also suggests that long-standing vitamin D deficiency may contribute to the development of larger adenomas. Chronic hypocalcemia drives sustained PTH stimulation, and prolonged parathyroid activation may promote cellular hyperplasia and adenoma growth, a mechanism proposed in studies examining giant parathyroid adenomas.3 This hypothesis may help explain the unusually large 3.5 g adenoma identified in this patient.
Localization of the adenoma presented diagnostic challenges in this case. Although ultrasonography is the standard initial imaging modality, its sensitivity is operator dependent and notably reduced for posterior or inferior parathyroid glands.9 In contrast, 99mTc-sestamibi scintigraphy demonstrates higher sensitivity for hyperfunctioning parathyroid adenomas and is recommended as an optimal modality for their detection.9 In this patient, two separate ultrasound examinations were inconclusive, whereas 99mTc-sestamibi imaging clearly localized the left inferior adenoma through persistent radiotracer retention on delayed images, consistent with the characteristic appearance of a solitary hyperfunctioning parathyroid gland.
Current international guidelines from the Fifth International Workshop on Primary Hyperparathyroidism recommend parathyroidectomy as the definitive treatment when specific clinical criteria are met.7 Indications for surgery include symptomatic disease, evidence of skeletal or renal involvement, serum calcium levels significantly above the upper limit of normal, or age younger than 50 years, which alone is considered sufficient justification for surgical management. Importantly, patients are required to meet only one of these criteria to be considered appropriate candidates for surgery. High cure rates have been reported following surgical excision of solitary lesions, including giant adenomas.7,11
In the present case, surgical intervention was justified because the patient fulfilled this guideline criterion by virtue of her age of 30 years.7 In addition, she presented with symptoms including bone pain and paresthesia and demonstrated persistently elevated parathyroid hormone levels despite correction of severe vitamin D deficiency. Functional imaging further localized a solitary hyperfunctioning parathyroid lesion consistent with an adenoma, therefore, observation alone was not considered an optimal management strategy.7 Additionally, long term surveillance in young patients with primary hyperparathyroidism may expose them to decades of ongoing parathyroid hormone excess and the potential development of progressive skeletal and renal complications.7
Large parathyroid adenomas may clinically or radiologically mimic parathyroid carcinoma, making histopathologic evaluation essential.12 In this case, the presence of uniform chief cells, preserved lobular architecture, and the absence of capsular or vascular invasion supported the diagnosis of a benign adenoma rather than carcinoma.12
Although Hungry Bone Syndrome (HBS) remains a significant postoperative concern in primary hyperparathyroidism, our patient did not meet high-risk criteria. As outlined in recent literature, HBS is most strongly associated with markedly elevated PTH levels (>1000 ng/L), ALP values exceeding 3–4 times the upper limit of normal, and metabolic profiles seen in secondary hyperparathyroidism or dialysis patients.13 Our patient’s ALP was corrected pre-operatively, PTH elevation was modest rather than severe, and both calcium and 25-hydroxyvitamin D levels were stable prior to surgery, placing her within the low-risk group.13 Rather than aggressive prophylactic therapy, close postoperative monitoring was clinically appropriate and consistent with recommendations reserving high-dose calcium and calcitriol protocols for patients with severe biochemical or skeletal risk factors.14
This report has several limitations inherent to a single-case design. The findings are not generalizable to all patients with primary hyperparathyroidism, particularly given the rarity of giant parathyroid adenomas and the atypical biochemical presentation observed in this case. In addition, the duration of follow-up was limited, precluding assessment of long-term outcomes such as recurrence or persistent metabolic complications. Finally, while severe vitamin D deficiency appeared to mask the underlying disorder, a causal relationship between vitamin D status and the development, size, or progression of the adenoma cannot be established.
Conclusion
This case highlights the importance of maintaining a high index of suspicion for primary hyperparathyroidism in patients presenting with discordant calcium–PTH patterns, particularly in the setting of severe vitamin D deficiency. It emphasizes the need for reassessment of biochemical parameters following vitamin D and calcium repletion to avoid misclassification as secondary hyperparathyroidism. Additionally, when first line imaging such as ultrasonography is non-diagnostic, functional imaging with 99mTc-sestamibi scintigraphy plays a critical role in accurate localization and surgical planning. From a broader policy and healthcare systems perspective, this case supports the need for increased awareness of atypical presentations of endocrine disorders, especially in regions with a high prevalence of vitamin D deficiency, and highlights the importance of ensuring access to appropriate diagnostic imaging and timely surgical management. Early recognition and intervention remain essential to prevent complications and achieve optimal patient outcomes.
Abbreviations
25-OH Vitamin D, 25-hydroxyvitamin D; 99mTc-sestamibi, Technetium-99m sesta-methoxyisobutylisonitrile; ALP, Alkaline phosphatase; CBC, Complete blood count; CDC73, Cell division cycle 73 gene; CT, Computed tomography; GPTA, Giant parathyroid adenoma; HBS, Hungry bone syndrome; MEN1, Multiple endocrine neoplasia type 1; MEN2A, Multiple endocrine neoplasia type 2A; MRI, Magnetic resonance imaging; PHPT, Primary hyperparathyroidism; PTH, Parathyroid hormone; PTA, Parathyroid adenoma; SPECT, Single-photon emission computed tomography; TSH, Thyroid-stimulating hormone; US, Ultrasound.
Data Sharing Statement
The data and materials in this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Formal ethics approval was not required because this case report describes a retrospective analysis of routinely collected clinical information without any experimental intervention.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
The authors gratefully acknowledge Mohammed Sibai for coordinating the research team and for his support in facilitating the completion of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No public or commercial fundings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bestepe N, Cuhaci FN, Polat B, et al. Serum calcium/phosphorus ratio in biochemical screening of primary hyperparathyroidism. Rev Assoc Med Bras. 2022;68(12):1668–7. doi:10.1590/1806-9282.20220645
2. Wolfe SA, Sandeep, Affiliations S. Parathyroid Adenoma (Archived). Available from: https://www.ncbi.nlm.nih.gov/books/NBK507870/?report=printable.
3. Bhan A, Athimulam S, Kumari P, et al. Large parathyroid adenomas: potential mechanisms to reconcile adenoma size and disease phenotype. Front Endocrinol. 2023;14. doi:10.3389/fendo.2023.1009516
4. Algargaz W, Abushukair HM, Odat H, Hamouri S, Abuashour R. Giant versus regular parathyroid adenoma: a retrospective comparative study. Ann Med Surg. 2021;66. doi:10.1016/j.amsu.2021.102454
5. Lenci N, Francesco P, Scarciglia E, et al. Metanephric adenoma with BRAF V600K mutation and a doubtful radiological imaging: pitfalls in the diagnostic process. Med Mol Morphol. 2021;54(2):187–191. doi:10.1007/s00795-020-00269-z
6. Rossi E, Cardisciani L, Policardo F, Tralongo P, Fiorentino V, Rossi ED. What psammoma bodies can represent in the thyroid. What we recently learnt from a story of lack of evidence. Pathologica. 2022;114(5):373–375. doi:10.32074/1591-951X-815
7. Bilezikian JP, Khan AA, Silverberg SJ, et al. Evaluation and management of primary hyperparathyroidism: summary statement and guidelines from the Fifth International Workshop. J Bone Miner Res. 2022;37(11):2293–2314. doi:10.1002/jbmr.4677
8. Elsherbiny TM. Hypovitaminosis D masking hypercalcemia in primary hyperparathyroidism: case report. Ther Adv Endocrinol Metab. 2023;14. doi:10.1177/20420188231213208
9. Kowalski GJ, Buła G, Żądło D, Gawrychowska A, Gawrychowski J. Primary hyperparathyroidism. Endokrynol Pol. 2020;71(3):260–270. doi:10.5603/EP.a2020.0028
10. Ghemigian A, Trandafir A, Petrova E, et al. Primary hyperparathyroidism-related giant parathyroid adenoma (Review). Exp Ther Med. 2021;23(1). doi:10.3892/etm.2021.11011
11. Grover M, Sharma M, Bhandari S, Sharma B, Bhargva S, Samdhani S. Giant parathyroid adenoma: are they different? Indian J Otolaryngol Head Neck Surg. 2022;74(S2):1929–1932. doi:10.1007/s12070-020-01898-7
12. Aziz H, Hussein Z. Giant parathyroid adenoma versus parathyroid carcinoma: differentiating two entities. J ASEAN Fed Endocr Soc. 2021;36(1):104–107. doi:10.15605/JAFES.036.01.11
13. Coman A, Tarta C, Marian M, et al. Hungry bone syndrome after parathyroidectomy for secondary hyperparathyroidism: pathogenesis and contemporary clinical considerations. J Clin Med. 2025;14(19). doi:10.3390/jcm14197104
14. Salman MAA, Rabiee A, Salman AA, et al. Role of vitamin D supplements in prevention of hungry bone syndrome after successful parathyroidectomy for primary hyperparathyroidism: a prospective study. Scand J Surg. 2021;110(3):329–334. doi:10.1177/1457496920962601
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.