Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Giant Nevus Lipomatosus Cutaneous Superficialis with Cerebriform Surfaces on the Back and Sacral Region: A Case Report
Authors Li S, Xiao Y, Wang H, Liu Z
Received 18 March 2022
Accepted for publication 8 May 2022
Published 30 May 2022 Volume 2022:15 Pages 981—985
DOI https://doi.org/10.2147/CCID.S366432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Shuo Li,1,* Yiding Xiao,1,* He Wang,2 Zhifei Liu1
1Department of Plastic Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Department of Neurological Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhifei Liu, Email [email protected]
Abstract: Nevus lipomatosus cutaneous superficialis (NLCS) is a rare hamartoma of adipose tissue characterized by the ectopic build-up of adipose tissue among collagen bundles and proliferation of ectopic adipocytes in the dermis, which leads to an absence of connection to the subcutaneous tissue. Giant NLCS (over 15 × 15 cm) is even rarer. So far, the largest NLCS mass in the literature was a giant lesion measuring 50 × 50 cm on the sacral area reported in 2014. Herein, we report a case of an even larger NLCS lesion with a size of 106 × 30 cm on the back and sacral regions. These lesions had been left untreated and had grown from small yellowish papules and nodules to giant multilocular pedunculated masses with cerebriform surfaces over 24 years. To the best of our knowledge, the NLCS lesion presented here is the largest reported. The report aimed to increase clinicians’ awareness of this rare and easily misdiagnosed disease. Furthermore, physicians should be mindful that early recognition and appropriate treatment are essential for NLCS patients, and lesions of NLCS can coalesce into unimaginable huge masses if left untreated resulting in more significant therapeutic challenges.
Keywords: nevus lipomatosus cutaneous superficialis, giant mass, early recognition, ectopic adipocytes, surgical resection and skin graft
Introduction
Nevus lipomatosus cutaneous superficialis (NLCS) is a rare benign malformation of ectopic mature adipocytes proliferating within the reticular dermis, generally classified into two clinical types, the classic and the solitary form.1 Giant NLCS (over 15 × 15 cm) is even rarer, and the largest NLCS mass so far was reported by Tas et al in 2014,2 a massive lesion of classic type measuring 50 × 50 cm on the sacral area associated with diffuse intramuscular lipomatosis. Herein, we encounter a giant pedunculated NLCS mass with cerebriform surfaces measuring 106 × 30 cm on the back and buttock successfully removed by staged excisions and skin graft, which is considered the largest ever reported.
Case Report
In 2019, a 39-year-old male who presented with multiple, asymptomatic, skin-colored, cerebriform masses widely distributed on the dorsal, sacral, left facial, and the nuchal area was admitted to our institution (Figure 1A). These lesions were initially noticed 24 years ago as hyperkeratotic yellowish papules clustered around the lower back, buttock, and neck. The nodules then progressively and insidiously increased in size and coalesced into tender, multilocular and pedunculated plaques with non-ulcerated and cerebriform surfaces measuring 106 × 30 cm on the dorsal region and 25 × 21.5 cm on the left nuchal region. The lesions intermittently discharged purulent exudates without any pain or itching feelings. Magnetic resonance imaging and computed tomography showed huge, subcutaneous, predominantly fatty, space-occupying lesions on the posterior and lateral walls of the abdominopelvic region. No regional lymphadenopathy was found, and no routine laboratory examinations showed remarkable abnormalities. No family members were found to manifest similar symptoms. The patient was referred to our plastic surgery department for surgical excision as the giant masses severely influenced his quality of life physically and mentally. The largest portion of the total pedunculated mass on the back measuring 36 × 28 × 5.5 cm was completely removed during the first surgical resection and split-thickness skin graft under general anesthesia. Histopathological examination found ectopic mature adipocytes intermingled with collagen bundles and proliferating in the dermis around the blood vessels and periadnexal structures (Figure 2). Thus, combined with manifestations and pathological characteristics, the patient was diagnosed with nevus lipomatosus cutaneous superficialis (NLCS). As the masses were huge and widely distributed, the patient underwent five staged surgical resections in total at about a 6-month distance between each operation. The postoperative skin graft area survived well without tenderness or ulceration. No recurrence of NLCS was observed in the 3-year follow-up, which dramatically improved the patient’s basic self-care abilities and psychological health (Figure 1B and C).
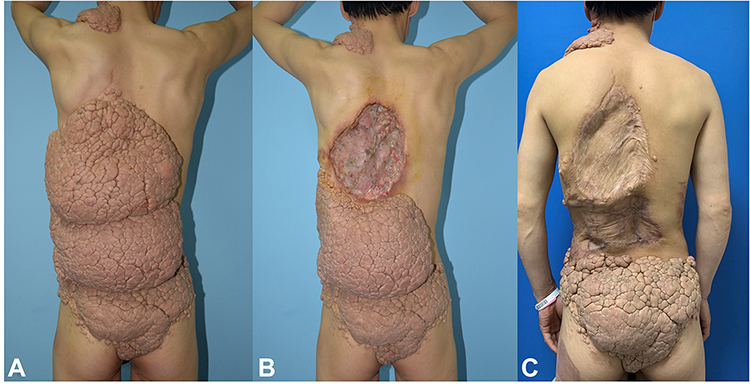 |
Figure 1 Multiple, giant, skin-colored NLCS masses with cerebriform surfaces distributed on the back, buttock, and nuchal area before (A). 7 months after the first operation (B), the patient underwent the second surgical excision. 6 months after the second surgical excision (C). |
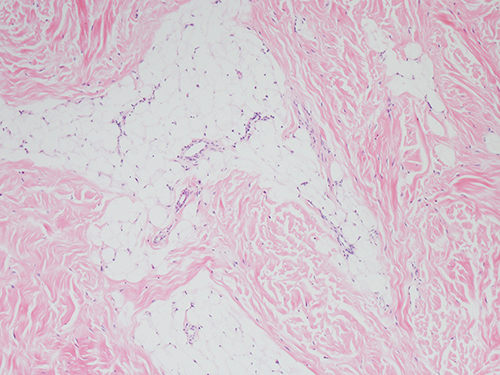 |
Figure 2 Histopathological biopsy revealed ectopic mature adipocytes interspersed with collagen bundles and proliferating in the dermis (Hematoxylin and eosin; ×40). |
Discussion
NLCS is an uncommon and unique hamartoma of lipoma without gender predilection or familial occurrence.1 The two clinical types, the classic and the solitary variant, differ in predilection locations, gross findings, and therapeutic modalities. The classic form of NLCS is generally characterized by multiple skin-colored or yellowish fleshy nodules fusing into larger plaques in a zonal or zosteriform pattern. The classic variants are usually inborn or occur in young people under the age of twenty. The predilection regions of the classic form include the upper part of the thighs, lumbar and pelvic area.3 The lesions in the presented patient were classic variants of NLCS, although this patient was not in the predilection age group. The solitary form usually manifests in isolated papules, mainly affecting adults between thirty and fifty. The solitary variant commonly has no predilection sites, but its occurrence across the clitoris has rarely been reported.4
The diagnosis of NLCS is confirmed by its histopathological characteristics, the deposition of ectopic adipose tissue among the collagen bundles, and the proliferation of mature adipocytes within the reticular and papillary dermis resulting in the absence of connection between the dermis and subcutaneous adipose tissue.5,6 Some other abnormalities have also been reported in NLCS lesions, including the thickening of collagen bundles, the presence of spindle cells standing for immature adipocytes, and the increasing amount of elastic tissue.7 The pathogenesis of NLCS has not been elucidated thoroughly, although several hypotheses have been postulated.8,9 Clinically and pathologically, dermatologic diseases easily confused with NLCS include skin tags, focal dermal hypoplasia, nevus sebaceous, lipofibromas, plexiform neurofibroma, giant acrochordons with fat herniation, segmental neurofibromatosis, and lymphangioma.10,11 A giant skin tag should be differentiated from the solitary form of NLCS. Pathologically, there is a lack of adipocytes in the dermis of skin tags. For lipofibromas, adipocytes can be observed with the absence of dermal appendages. For focal dermal hypoplasia, also called Goltz syndrome, adipocytes completely replace the atrophic dermis with a lack of skin appendages and collagen bundles.12
NLCS has rarely been reported to be associated with malignant transformation and systemic involvement, so surgical interventions are curative mainly for aesthetic improvements.10 The necessity and importance of timely therapeutic correction for patients with NLCS cannot be underestimated, as the nodules or papules can coalesce into large plaques leading to serious health issues and profound psychosocial dysfunction if not treated.13 Since the involved lesions in classic variant NLCS can be extensive, surgical resection is theoretically more appropriate for the solitary type. However, for the giant masses like this current patient with a classic type of NLCS, staged surgical excision combined with a split-thickness skin graft is the best option.
The intervention procedures in the previously reported giant NLCS (over 15 × 15 cm) were all wide surgical excision combined with flap transposition or skin graft.2,13,14 There have been no reported articles on the application of tissue expansion to repair the defects left after giant NLCS resection. Tissue expansion is a method of implanting expanders under the subcutaneous or muscular layers to enlarge the area of overlying skin and provide additional skin to replace the adjacent skin defect deformities. Compared with skin grafting, the advantages of tissue expansion include minor damage to the donor site with less scar left and no significant pigmentation. Additionally, the color, texture, sensation, and function between the repaired defect area and the surrounding normal skin are identical. However, tissue expansion requires a more extended treatment duration, and the prerequisite for applying tissue expansion is that there should be enough area of normal skin around the defect. Thus, tissue expansion is more appropriate for wounds with a smaller surface, while skin grafting can achieve more satisfying interventional effects on more significant skin defects. This is why the giant NLCS (106 × 30 cm) in the current study applied a split-thickness skin graft on the defect area after staged surgical resection, as the normal skin tissue left around the huge lesion was minimal. Tissue expansion can also be considered an effective therapeutic option in addition to skin graft, especially for smaller NLCS. Postoperative recurrence in NLCS patients has been reported to be very rare.14 Conservative therapeutic interventions include CO2 ablative laser, sodium deoxycholate, phosphatidylcholine, and cryotherapy for NLCS patients in whom surgical treatment cannot achieve satisfactory results.3,15
Searching “Nevus lipomatosus cutaneous superficialis” within PubMed and Web of Science, as NLCS is a unique and rare hamartoma of adipose tissue, we found sporadic case reports on this disease. However, there were even fewer reports of giant NLCS (over 15 × 15 cm) and a classic NLCS lesion with a size of 50 × 50 cm on the thigh and buttock, causing compression of the sciatic nerve, which was also combined with diffuse intramuscular lipomatosis, which has been reported to be the largest.2 In addition, giant NLCS masses with the size of 50 × 40 cm, 40 × 28 cm, and 30 × 20 cm have also been reported, respectively.1,4,13 To the best of our knowledge, the vast, multilocular, asymptomatic, and pedunculated plaque in a cerebriform pattern measuring 106 × 30 cm presented here is the largest reported. There has been no literature documenting that lesions of NLCS can grow up to this size if left untreated for many years. We share our experience to increase awareness and deepen the understanding of this rare and easily misdiagnosed disease among medical personnel. The lesions of NLCS can coalesce into unimaginable huge masses if untreated, which can escalate into significant therapeutic challenges for physicians. Thus, early recognition and appropriate therapeutic interventions are essential for improving NLCS patients’ cosmetic deformities, psychological health, and quality of life.
Conclusion
NLCS is a rare idiopathic anomaly of fatty tissue, and the current NLCS lesion presented here is the largest ever reported. The experience we share aims to remind health care providers of NLCS diagnosis when facing similar dermatologic masses. Patients with NLCS should perform complementary treatment even if the masses have not manifested with any symptoms temporarily to prevent the lesions from coalescing into larger plaques. Further investigations in a larger cohort are still needed to summarize the epidemiological and clinical features of NLCS, elucidate the etiology and pathogenesis of NLCS, and provide better-personalized treatment methods for NLCS patients.
Ethics Statement
Informed consent for publication of the case report and associated images was obtained from the patient. Institutional approval has been obtained to publish the case details.
Funding
There is no funding to report.
Disclosure
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
References
1. Jung UT, Park HW, Yun S-J, et al. Giant nevus lipomatosus cutaneous superficialis with intramuscular lipomatosis. J Am Acad Dermatol. 2012;67:e168–e170. doi:10.1016/j.jaad.2012.01.025
2. Taş S, Top H. Giant nevus lipomatosus cutaneous superficialis with intramuscular lipomatosis caused sciatic nerve compression. J Cutaneous Med Surg. 2014;18(4):1–2.
3. Castagna RD, Benvegnú AM, Dallazem LN, Brutti CS. Topical corticosteroid therapy: a treatment option for nevus lipomatosus cutaneous superficialis? Anais Brasileiros de Dermatologia. 2018;93(1):158–159.
4. Khandpur S, Nagpal SA, Chandra S, Sharma VK, Kaushal S, Safaya R. Giant nevus lipomatosus cutaneous superficialis. Ind J Dermatol Venereol Leprol. 2009;75:407–408.
5. Chopra R, Al Marzooq YM, Siddiqui FA, Aldawsari S, Al Ameer A. Nevus lipomatosus cutaneous superficialis with focal lipocytic pagetoid epidermal spread and secondary calcinosis cutis: a case report. Am J Dermatopathol. 2015;37(4):326–328.
6. Sato Y, Nobeyama Y, Omori Y, Nakagawa H. Female case of nevus lipomatosus cutaneous superficialis growing depending on the occurrence site. J Dermatol. 2016;1(44):107–108.
7. Joon Y, Choi JH, Kim H, Nam SH, Choi YW. Recurrence of nevus lipomatosus cutaneous superficialis after CO(2) laser treatment. Arch Plastic Surg. 2012;39(6):671.
8. Shinde GB, Viswanath V, Torsekar RG. Multiple yellowish plaques in cerebriform pattern on the right elbow. Int J Dermatol. 2012;51(6):662–664.
9. Gutiérrez‐González E, Montero I, Sánchez‐Aguilar D, Ginarte M, Toribio J. Adult-onset verrucous nevus lipomatosus cutaneous superficialis. Int J Dermatol. 2013;53(1):e69–e71.
10. Lozano‐Masdemont B, Pinedo-Moraleda F, Rodríguez-Lomba E, et al. Clustered yellow papules in the posterior axilla of a middle‐aged woman. Clin Exp Dermatol. 2022;47(1):213–215. doi:10.1111/ced.14868
11. Kumaran MS, Narang T, Dogra S, Saikia UN, Kanwar AJ. Nevus lipomatosus superficialis unseen or unrecognized: a report of eight cases. J Cutaneous Med Surg. 2013;17(5):335–339.
12. Aleena J. Nevus lipomatosus cutaneous superficialis: a rare hamartoma. Ind J Surg Oncol. 2019;11(3):147–149.
13. Knuttel R, Silver EA. A cerebriform mass on the right buttock. Dermatol Surg. 2003;29(7):780–781. doi:10.1046/j.1524-4725.2003.29197.x
14. Takegawa M, Kakudo N, Morimoto N, et al. Giant nevus lipomatosus cutaneous superficialis on the buttock. Plastic Reconstruct Surg. 2018;6(11):e1918. doi:10.1097/GOX.0000000000001918
15. Fatah S, Ellis R, Seukeran DC, et al. Successful CO2 laser treatment of naevus lipomatosus cutaneous superficialis. Clin Exp Dermatol. 2010;35(5):559–560. doi:10.1111/j.1365-2230.2010.03794.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.